Association between the Dietary Inflammatory Index and Risk for Cancer Recurrence and Mortality among Patients with Breast Cancer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Data Collection
2.3. DII
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Patients with and without Breast Cancer Recurrence
3.2. Food and Nutrient Intake of Patients with Breast Cancer According to the DII Score
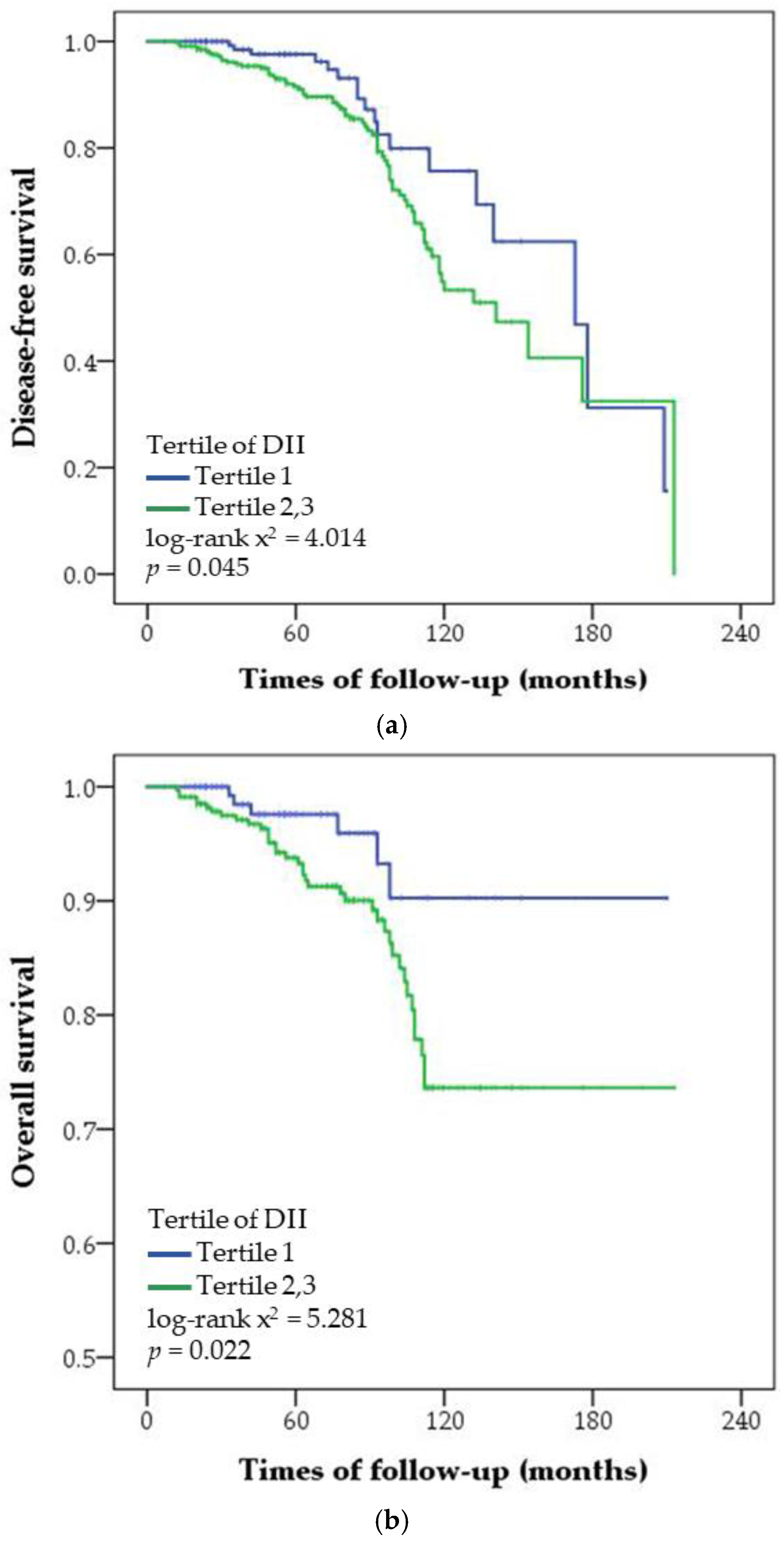
3.3. Association between the DII Score and the Risk for Cancer Recurrence and Overall Mortality in Patients with Breast Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Oh, C.M.; Kong, H.J.; Lee, D.H.; Lee, K.H. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2014. Cancer Res. Treat. 2017, 49, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, C.; Stearns, V.; Hayes, D.F. New prognostic factors for breast cancer recurrence. Semin. Oncol. 2001, 28, 53–67. [Google Scholar] [CrossRef]
- Sunil, S.B.; Shikha, B.; David, R.B.; Vivien, W.C.; James, L.C.; Basak, D.; Carl, J.D.; Stephen, B.E.; Armando, G.; Gabriel, N.H.; et al. AJCC Cancer Staging Manual, 8th ed.; The American College of Surgeons (ACS): Chicago, IL, USA, 2018; pp. 589–636. [Google Scholar]
- Ma, Y.; Ren, Y.; Dai, Z.J.; Wu, C.J.; Ji, Y.H.; Xu, J. IL-6, IL-8 and TNF-alpha levels correlate with disease stage in breast cancer patients. Adv. Clin. Exp. Med. 2017, 26, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L. Diet and breast cancer: Can dietary factors influence survival? J. Mammary Gland Biol. 2003, 8, 119–132. [Google Scholar] [CrossRef]
- Rock, C.L.; Demark-Wahnefried, W. Nutrition and survival after the diagnosis of breast cancer: A review of the evidence. J. Clin. Oncol. 2002, 20, 3302–3316. [Google Scholar] [CrossRef] [PubMed]
- Makarem, N.; Chandran, U.; Bandera, E.V.; Parekh, N. Dietary fat in breast cancer survival. Annu. Rev. Nutr. 2013, 33, 319–348. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nothlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Neale, E.P.; Batterham, M.J.; Tapsell, L.C. Consumption of a healthy dietary pattern results in significant reductions in C-reactive protein levels in adults: A meta-analysis. Nutr. Res. 2016, 36, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Vrieling, A.; Buck, K.; Seibold, P.; Heinz, J.; Obi, N.; Flesch-Janys, D.; Chang-Claude, J. Dietary patterns and survival in German postmenopausal breast cancer survivors. Br. J. Cancer 2013, 108, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systemiatic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Q.; Mo, X.F.; Ye, Y.B.; Shivappa, N.; Lin, F.Y.; Huang, J.; Hebert, J.R.; Yan, B.; Zhang, C.X. A higher dietary inflammatory index score is associated with a higher risk of breast cancer among Chinese women: A case-control study. Br. J. Nutr. 2017, 117, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Rosato, V.; Montella, M.; Serraino, D.; Vecchia, C.L. Association between the dietary inflammatory index and breast cancer in a large Italian case-control study. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R.; Hebert, J.R. Prospective study of the dietary inflammatory index and risk of breast cancer in postmenopausal women. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Sandin, S.; Lof, M.; Hebert, J.R.; Adami, H.O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of breast cancer in Swedish women. Br. J. Cancer 2015, 113, 1099–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabung, F.K.; Steck, S.E.; Liese, A.D.; Zhang, J.; Ma, Y.; Caan, B.; Chlebowski, R.T.; Freudenheim, J.L.; Hou, L.; Mossavar-Rahmani, Y.; et al. Association between dietary inflammatory potential and breast cancer incidence and death: Results from the Women’s Health Initiative. Br. J. Cancer 2016, 114, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; WHO: Geneva, Switzerland, 2000; p. 18. [Google Scholar]
- Zucchetto, A.; Serraino, D.; Shivappa, N.; Hebert, J.R.; Stocco, C.; Puppo, A.; Falcini, F.; Panato, C.; Dal Maso, L.; Polesel, J. Dietary inflammatory index before diagnosis and survival in an Italian cohort of women with breast cancer. Br. J. Nutr. 2017, 117, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the seasonal variation of blood cholesterol study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Dethlefsen, C.; Højfeldt, G.; Hojman, P. The role of intratumoral and systemic IL-6 in breast cancer. Breast Cancer Res. Treat. 2013, 138, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Ge, I.; Rudolph, A.; Shivappa, N.; Flesch-Janys, D.; Hebert, J.R.; Chang-Claude, J. Dietary inflammation potential and postmenopausal breast cancer risk in a German case-control study. Breast 2015, 24, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Eliassen, A.H.; Missmer, S.A.; Tworoger, S.S.; Spiegelman, D.; Barbieri, R.L.; Dowsett, M.; Hankinson, S.E. Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women. J. Natl. Cancer Inst. 2006, 98, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: Collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet 1997, 350, 1047–1059. [Google Scholar] [CrossRef]
- Honma, S.; Shimodaira, K.; Shimizu, Y.; Tsuchiya, N.; Saito, H.; Yanaihara, T.; Okai, T. The influence of inflammatory cytokines on estrogen production and cell proliferation in human breast cancer cells. Endocr. J. 2002, 49, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Newman, S.P.; Reed, M.J. The role of cytokines in regulating estrogen synthesis: Implications for the etiology of breast cancer. Breast Cancer Res. 2002, 4, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnoli, C.; Grioni, S.; Pala, V.; Allione, A.; Matullo, G.; Gaetano, C.D.; Tagliabue, G.; Sieri, S.; Krogh, V. Biomarkers of inflammation and breast cancer risk: A case-control study nested in the EPIC-Varese cohort. Sci. Rep. 2017, 7, 12708. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, A. Obesity as a risk factor for development and poor prognosis of breast cancer. Int. J. Obstet. Gynaecol. 2006, 113, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Jiralerspong, S.; Goodwin, P.J. Obesity and breast cancer prognosis: Evidence, challenges, and opportunities. J. Clin. Oncol 2016, 34, 4203–4216. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Strickler, H.D.; Fine, E.; Sparano, J.A. Clinical studies examining the impact of obesity on breast cancer risk and prognosis. J. Mammary Gland Biol. 2013, 18, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.G.; Hudis, C.A.; Giri, D.; Morrow, M.; Falcone, D.J.; Zhou, X.K.; Du, B.; Brogi, E.; Crawford, C.B.; Kopelovich, L.; et al. Inflammation and increased aromatase expression occur in the breast tissue of obese women with breast cancer. Cancer Prev. Res. 2011, 4, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, S.C.; Frasor, J. Minireview: Inflammation: An instigator of more aggressive estrogen receptor (ER) positive breast cancers. Mol. Endocrinol. 2012, 26, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual hazard rates of recurrence for breast cancer during 24 years of follow-up: Results from the international breast cancer study group trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.P.; Shen, Z.Z.; Liu, T.J.; Agarwal, G.; Tajima, T.; Paik, N.S.; Sandelin, K.; Derossis, A.; Cody, H.; Foulkes, W.D. Is breast cancer the same disease in Asian and Western countries? World J. Surg. 2010, 34, 2308–2324. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Ren, Z.; Pae, M.; Han, S.N.; Meydani, S.N. Diet-induced obesity has a differential effect on adipose tissue and macrophage inflammatory responses of young and old mice. Biofactors 2013, 39, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Korea Health Statistics 2016: Korea National Health and Nutrition Examination Survey (KNHANES VI-VII). Available online: http://knhanes.cdc.go.kr/knhance/eng/index.do (accessed on 10 December 2016).
- Wakimoto, P.; Block, G. Dietary intake, dietary patterns, and changes with age: An epidemiological perspective. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Sheen-Chen, S.M.; Chen, W.J.; Eng, H.L.; Chou, F.F. Serum concentration of tumor necrosis factor in patients with breast cancer. Breast Cancer Res. Treat. 1997, 43, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Ravishankaran, P.; Karunanithi, R. Clinical significance of preoperative serum interleukin-6 and C-reactive protein level in breast cancer patients. World J. Surg. Oncol. 2011, 9, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, W.; Jiang, Y.; Shen, Z.; Shao, Z.; Lu, J. Trastuzumab in the adjuvant treatment of HER2-positive early breast cancer patients: A meta-analysis of published randomized controlled trials. PLoS ONE 2011, 6, e21030. [Google Scholar] [CrossRef] [PubMed]
- Pinto, B.M.; Eakin, E.; Maruyama, N.C. Health behavior changes after a cancer diagnosis: What do we know and where do we go from here? Ann. Behav. Med. 2000, 22, 38–52. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| With Cancer Recurrence (n = 88) | Without Cancer Recurrence (n = 423) | p-Value 2 | |
|---|---|---|---|
| Age (years) | 49.57 ± 11.35 | 52.40 ± 10.50 | 0.024 |
| Postmenopausal status | 38 (43.2) | 215 (50.8) | 0.192 |
| Body mass index (kg/m2) | 23.63 ± 3.32 | 23.03 ± 2.76 | 0.115 |
| Body mass index (kg/m2) | |||
| <25 | 58 (65.9) | 327 (77.3) | 0.024 |
| ≥25 | 30 (34.1) | 96 (22.7) | |
| ER expression | |||
| Positive | 55 (63.2) | 302 (71.7) | 0.114 |
| Negative | 32 (36.8) | 119 (28.3) | |
| PR expression | |||
| Positive | 48 (55.2) | 292 (69.4) | 0.010 |
| Negative | 39 (44.8) | 129 (30.6) | |
| HER2 amplification | |||
| Amplified | 25 (28.7) | 113 (26.8) | 0.718 |
| Not amplified | 62 (71.3) | 308 (73.2) | |
| Subtype | |||
| HR+/HER2- | 45 (51.7) | 256 (60.8) | 0.176 |
| HR+/HER2+ | 18 (20.7) | 69 (16.4) | |
| HR−/HER2+ | 7 (8.0) | 44 (10.5) | |
| HR−/HER2- | 17 (19.5) | 52 (12.4) | |
| Histologic grade | |||
| Grade 1 | 16 (19.3) | 122 (29.9) | 0.048 |
| Grade 2 | 31 (37.3) | 160 (39.2) | |
| Grade 3 | 36 (43.4) | 126 (30.9) | |
| Tumor size (cm) 3 | |||
| ≤2 | 31 (36.0) | 251 (59.9) | <0.001 |
| >2 | 55 (64.0) | 168 (40.1) | |
| Lymph node metastasis | |||
| Absence | 48 (54.5) | 307 (72.6) | 0.001 |
| Presence | 40 (45.5) | 116 (27.4) | |
| AJCC stage | |||
| Stages 0–2 | 68 (78.2) | 372 (88.6) | 0.009 |
| Stage 3 | 19 (21.8) | 48 (11.4) | |
| Treatment | |||
| Chemotherapy | 62 (70.5) | 238 (56.3) | 0.014 |
| Hormonal therapy | 59 (67.0) | 318 (75.2) | 0.115 |
| Radiotherapy | 39 (44.3) | 232 (54.8) | 0.072 |
| DII score | 0.61 ± 1.93 | −0.14 ± 2.16 | 0.003 |
| Death | 41 (46.6) | 3 (0.7) | <0.001 |
| Tertiles of the DII | p for Trend 1 | |||
|---|---|---|---|---|
| T1 (n = 170) −2.37 (−5.87–(−1.07)) | T2 (n = 170) −0.10 (−1.08–0.97) | T3 (n = 171) 2.40 (0.98–5.48) | ||
| Risk for cancer recurrence | ||||
| No. of patients with/without recurrence | 18/152 | 29/141 | 41/130 | |
| Adjusted HR (95% CI) 2 | 1.0 (ref.) | 1.832 (0.94–3.57) | 2.347 (1.17–4.71) | 0.019 |
| Overall mortality | ||||
| No. of deaths/survivors | 6/164 | 17/153 | 21/150 | |
| Adjusted HR (95% CI) 2 | 1.0 (ref.) | 2.403 (0.87–6.65) | 3.049 (1.08–8.83) | 0.041 |
| No. of Patientswith/withoutRecurrence | Tertiles of the DII (HR, 95% CI)2 | p for Trend 1 | |||
|---|---|---|---|---|---|
| T1 (n = 170) −2.37 (−5.87–(−1.07)) | T2 (n = 170) −0.10 (−1.08–0.97) | T3 (n = 171) 2.40 (0.98–5.48) | |||
| Age (years) | |||||
| <50 | 48/189 | 1.0 (ref.) | 3.541 (1.22–10.25) | 4.718 (1.63–13.64) | 0.006 |
| ≥50 | 40/234 | 1.0 (ref.) | 0.919 (0.35–2.39) | 1.636 (0.57–4.74) | 0.335 |
| Menopausal status | |||||
| Premenopause | 50/208 | 1.0 (ref.) | 2.101 (0.73–6.04) | 3.288 (1.25–8.67) | 0.014 |
| Postmenopause | 38/215 | 1.0 (ref.) | 1.226 (0.48–3.11) | 1.281 (0.41–3.99) | 0.669 |
| BMI (kg/m2) | |||||
| <25 | 58/327 | 1.0 (ref.) | 1.621 (0.73–3.60) | 1.980 (0.87–4.51) | 0.109 |
| ≥25 | 30/96 | 1.0 (ref.) | 3.427 (0.66–17.94) | 8.460 (1.42–50.24) | 0.015 |
| Hormone receptor status | |||||
| HR+ | 63/325 | 1.0 (ref.) | 1.966 (0.89–4.34) | 2.374 (1.05–5.37) | 0.045 |
| HR− | 24/96 | 1.0 (ref.) | 2.189 (0.54–8.91) | 4.260 (0.91–19.87) | 0.064 |
| Tumor size (cm) | |||||
| ≤2 | 31/251 | 1.0 (ref.) | 1.053 (0.38–2.91) | 0.843 (0.27–2.61) | 0.743 |
| >2 | 55/168 | 1.0 (ref.) | 1.839 (0.74–4.55) | 3.603 (1.47–8.86) | 0.004 |
| Lymph node metastasis | |||||
| Absence | 48/307 | 1.0 (ref.) | 0.895 (0.37–2.16) | 0.983 (0.38–2.56) | 0.998 |
| Presence | 40/116 | 1.0 (ref.) | 4.245 (1.37–13.19) | 5.287 (1.69–16.54) | 0.006 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.; Chung, M.S.; Kang, S.S.; Park, Y. Association between the Dietary Inflammatory Index and Risk for Cancer Recurrence and Mortality among Patients with Breast Cancer. Nutrients 2018, 10, 1095. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081095
Jang H, Chung MS, Kang SS, Park Y. Association between the Dietary Inflammatory Index and Risk for Cancer Recurrence and Mortality among Patients with Breast Cancer. Nutrients. 2018; 10(8):1095. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081095
Chicago/Turabian StyleJang, Hyeonjeong, Min Sung Chung, Shin Sook Kang, and Yongsoon Park. 2018. "Association between the Dietary Inflammatory Index and Risk for Cancer Recurrence and Mortality among Patients with Breast Cancer" Nutrients 10, no. 8: 1095. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081095