Approaches to Assess Vitamin A Status in Settings of Inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project

 , , and
, , and
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Participant Characteristics
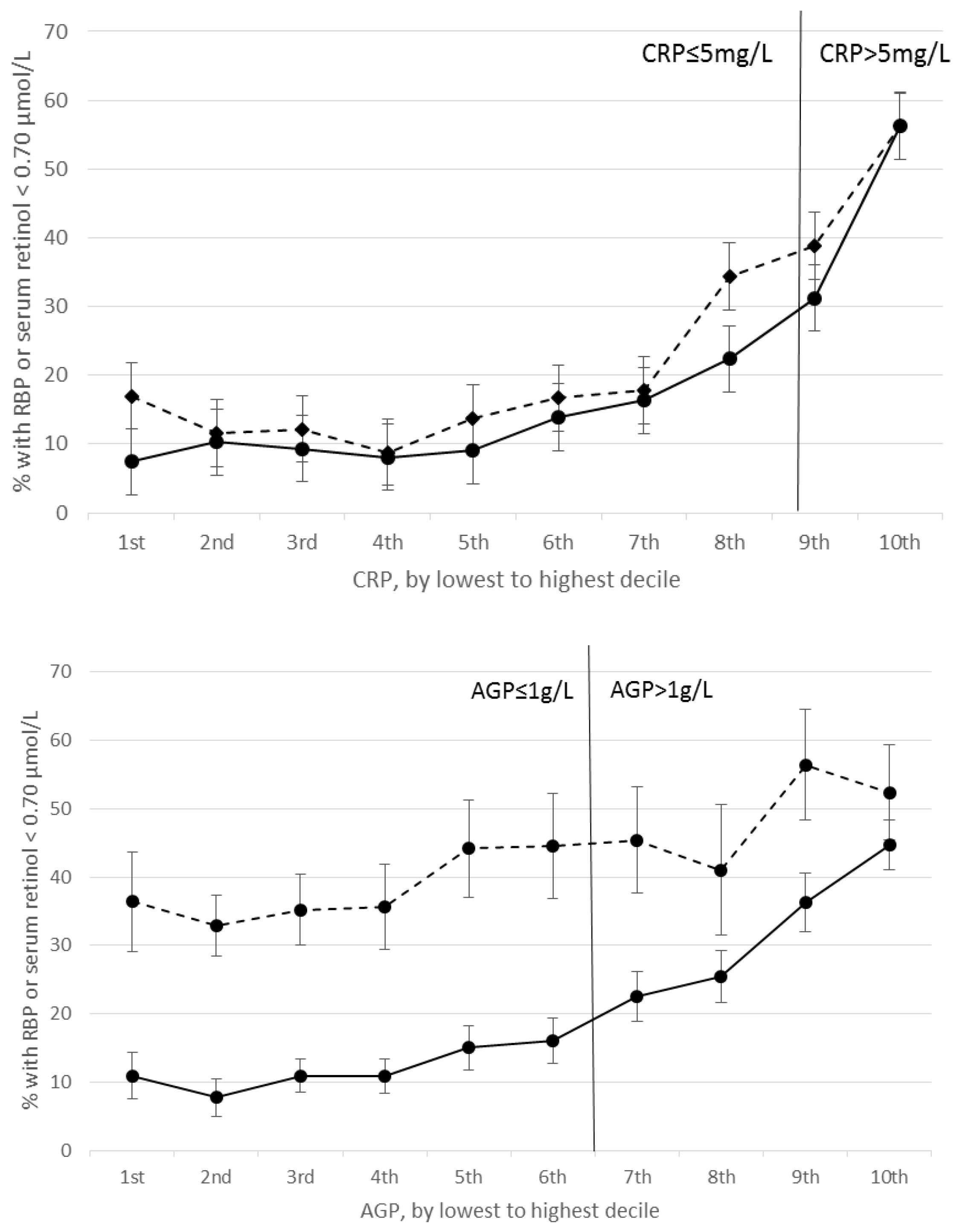
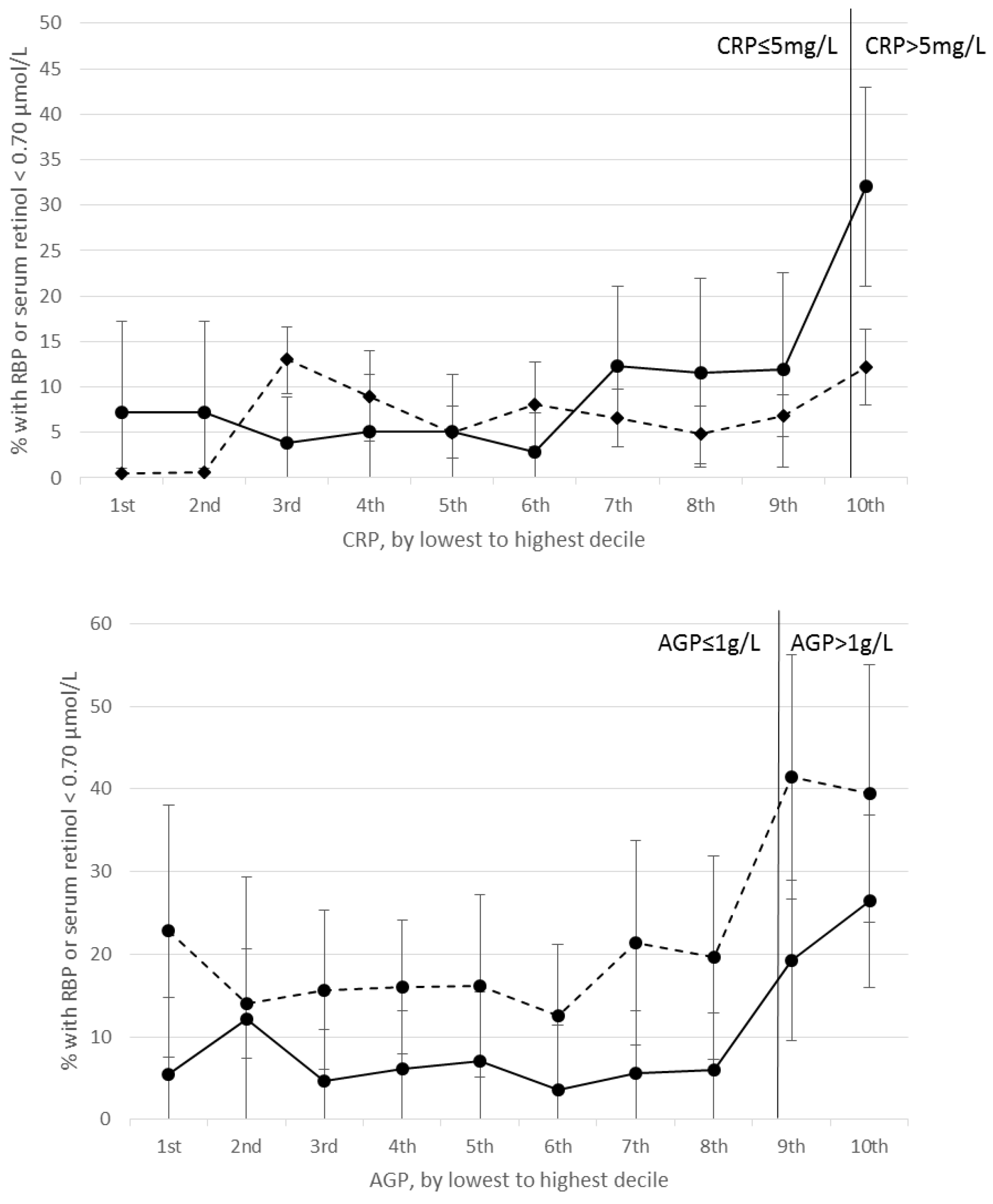
3.2. Relation between RBP, Retinol, and Inflammation
3.3. Unadjusted prevalence of VAD in PSC, SAC, and WRA
3.4. Estimated prevalence of VAD in PSC and SAC adjusting for inflammation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- West, K.P., Jr. Vitamin A deficiency disorders in children and women. Food Nutr. Bull. 2003, 24, S78–S90. [Google Scholar] [CrossRef] [PubMed]
- Tanumihardjo, S.A. Biomarkers of vitamin A status: What do they mean? Panama City, Panama, 15–17 September 2010. World Health Organization: Geneva, Switzerland. 2012. Available online: http://www.who.int/nutrition/publications/micronutrients/background_paper2_report_assessment_vitAandIron_status.pdf (accessed on 15 May 2017).
- WHO. Indicators for assessing vitamin A deficiency and their application in monitoring and evaluation intervention programmes. Available online: http://www.who.int/nutrition/publications/micronutrients/vitamin_a_deficiency/WHONUT96.10.pdf (accessed on 18 April 2015).
- WHO. Serum retinol concentrations for determining the prevalence of vitamin A deficiency in populations. Available online: http://www.who.int/vmnis/indicators/retinol.pdf (accessed on 16 January 2015).
- Rosales, F.J.; Ritter, S.J.; Zolfaghari, R.; Smith, J.E.; Ross, A.C. Effects of acute inflammation on plasma retinol, retinol-binding protein, and its mRNA in the liver and kidneys of vitamin A-sufficient rats. J. Lipid Res. 1996, 37, 962–971. [Google Scholar] [PubMed]
- Keusch, G. Infection, fever and nutrition. Encyclopaedia of Food Science, Food Technology and Nutrition; Academic Press: Cambridge, MA, USA, 1993; pp. 2522–2526. [Google Scholar]
- Baumann, H.; Gauldie, J. The acute phase response. Immunol. Today 1994, 15, 74–80. [Google Scholar] [CrossRef]
- Fleck, A.; Myers, M. Diagnostic and prognostic significance of the acute phase proteins. The Acute Phase Response to Injury and Infection; Elsevier: New York, NY, USA, 1985; pp. 249–271. [Google Scholar]
- Feelders, R.; Vreugdenhil, G.; Eggermont, A.; Kuiper-Kramer, P.; Van Eijk, H.; Swaak, A. Regulation of iron metabolism in the acute-phase response: Interferon-g and tumor necrosis factor-A induce hypoferraemia, ferritin production and a decrease in circulating transferrin receptors in cancer patients. Eur. J. Clin. Investig. 1998, 28, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A.K.; Alvarez, J.O.; Guay-Woodford, L.; Fuchs, G.J.; Wahed, M.; Stephensen, C.B. Urinary retinol excretion and kidney function in children with shigellosis. Am. J. Clin. Nutr. 1998, 68, 1095–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, J.A.; Werbeck, A.; Louw, M.E.; Kotze, T.J.; Cooper, R.; Labadarios, D. Blood vitamin concentrations during the acute-phase response. Crit. Care. Med. 1992, 20, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Suchdev, P.S.; Namaste, S.M.; Aaron, G.J.; Raiten, D.J.; Brown, K.H.; Flores-Ayala, R. Overview of the biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Adv. Nutr. 2016, 7, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Larson, L.M.; Namaste, S.M.; Williams, A.M.; Engle-Stone, R.; Addo, O.Y.; Suchdev, P.S.; Wirth, J.P.; Temple, V.; Serdula, M.; Northrop-Clewes, C.A. Adjusting retinol-binding protein concentrations for inflammation: Biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 390s–401s. [Google Scholar] [PubMed]
- Namaste, S.M.; Aaron, G.J.; Varadhan, R.; Peerson, J.M.; Suchdev, P.S. Methodologic approach for the biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 333s–347s. [Google Scholar] [PubMed]
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined measurement of ferritin, soluble transferrin receptor, retinol binding protein, and C-reactive protein by an inexpensive, sensitive, and simple sandwich enzyme-linked immunosorbent assay technique. J. Nutr. 2004, 134, 3127–3132. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.A. Principles of Nutritional Assessment; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Thurnham, D.I.; McCabe, G.P.; Northrop-Clewes, C.A.; Nestel, P. Effects of subclinical infection on plasma retinol concentrations and assessment of prevalence of vitamin A deficiency: Meta-analysis. Lancet 2003, 362, 2052–2058. [Google Scholar] [CrossRef]
- Mills, J.P.; Furr, H.C.; Tanumihardjo, S.A. Retinol to retinol-binding protein (RBP) is low in obese adults due to elevated apo-RBP. Exp. Biol. Med. 2008, 233, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Benn, C.S.; Aaby, P.; Arts, R.J.; Jensen, K.J.; Netea, M.G.; Fisker, A.B. An enigma: Why vitamin A supplementation does not always reduce mortality even though vitamin A deficiency is associated with increased mortality. Int. J. Epidemiol. 2015, 44, 906–918. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.B.; Ramirez, M.A.; Fernandez, C.M.; Pedro, R.; Lloren, T.; Saldanha, L.; Deitchler, M.; Eisele, T. Effects on vitamin A deficiency in children of periodic high-dose supplements and of fortified oil promotion in a deficient area of the philippines. Int. J. Vitam. Nutr. Res. 2011, 81, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.; Greiner, T.; Shrimpton, R.; Sanders, D.; Yukich, J. Vitamin A policies need rethinking. Int. J. Epidemiol. 2014, 44, 283–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurnham, D.I. Correcting nutritional biomarkers for the influence of inflammation. Br. J. Nutr. 2017, 118, 761–762. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, R.D. Inclusion of the modified relative dose response test in population-based surveys in Guatemala, Uganda, Mozambique, and Nepal: Implications for cut-offs and prevalence of vitamin A deficiency. In Proceedings of the Micronutrient Forum, Cancun, Mexico, 23–28 October 2016. [Google Scholar]
- National Statistics Office; Community Health Services Unit of the Ministry of Health; Centers for Disease Control & Prevention; Emory University. Malawi Micronutrient Survey Key Indicators Report 2015–2016; Atlanta, GA, USA. Available online: https://dhsprogram.com/pubs/pdf/FR319/FR319m.pdf (accessed on 4 April 2018).
- Wieringa, F.T.; Dijkhuizen, M.A.; West, C.E.; Northrop-Clewes, C.A.; Muhilal. Estimation of the effect of the acute phase response on indicators of micronutrient status in Indonesian infants. J. Nutr. 2002, 132, 3061–3066. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country, year | n | Age (Months) Mean (Min, Max) | RBP (μmol/L) Median (95% CI) | Serum Retinol (μmol/L) Median (95% CI) | CRP > 5mg/L Percent (95% CI) | AGP > 1g/L Percent (95% CI) | CRP > 5mg/L or AGP > 1g/L Percent (95% CI) |
|---|---|---|---|---|---|---|---|
| Preschool Age Children | |||||||
| Afghanistan, 2013 | 657 | 29.1 (6, 58) | 0.70 (0.67, 0.73) | 10.1 (6.9, 13.4) | 23.6 (19.3, 27.9) | 25.7 (20.8, 30.5) | |
| Azerbaijan, 2013 | 1053 | 35.6 (6, 59) | 1.01 (0.98, 1.03) | 8.1 (6.0, 10.1) | 29.9 (26.2, 33.5) | 30.9 (27.1, 34.6) | |
| Bangladesh, 2010 | 1493 | 8.3 (6, 11) | 0.88 (0.87, 0.90) | 14.3 (11.8, 16.7) | 33.4 (29.9, 36.9) | 35.8 (32.2, 39.5) | |
| Bangladesh, 2012 | 458 | 36.5 (6, 59) | 0.85 (0.81, 0.89) | 7.3 (3.2, 11.5) | 28.5 (22.6, 34.4) | 29.0 (23.1, 34.9) | |
| Cambodia, 2014 | 665 | 35.9 (6, 60) | 1.32 (1.23, 1.40) | 10.0 (7.3, 12.8) | 36.2 (29.5, 42.9) | 38.3 (30.6, 46.0) | |
| Cameroon, 20091 | 774 | 31 (12, 60) | 0.84 (0.82, 0.87) | 0.70 (0.62, 0.77) | 37.5 (32.7, 42.3) | 39.3 (33.7, 45.0) | 48.3 (43.1, 53.5) |
| Colombia, 2010 | 3794 | 37.6 (12, 59) | 0.85 (0.83, 0.87) | 18.8 (17.1, 20.6) | |||
| Côte d’Ivoire, 2007 | 733 | 31.7 (6, 59) | 0.89 (0.86, 0.92) | 40.4 (36.5, 44.3) | 64.5 (60.3, 68.6) | 67.5 (63.8, 71.3) | |
| Ecuador, 2012 | 2017 | 30.8 (6, 59) | 0.88 (0.86, 0.90) | 12.5 (10.1, 14.9) | |||
| Kenya, 2007 | 888 | 19.9 (6, 36) | 0.87 (0.85, 0.90) | 27.8 (23.9, 31.7) | 64.2 (60.2, 68.2) | 66.0 (61.9, 70.1) | |
| Kenya, 2010 | 843 | 21.4 (6, 35) | 0.84 (0.81, 0.87) | 34.2 (29.6, 38.7) | 60.7 (56.0, 65.4) | 61.9 (57.2, 66.6) | |
| Liberia, 2011 | 1434 | 19.9 (6, 36) | 0.85 (0.82, 0.88) | 29.5 (26.5, 32.5) | 56.2 (52.5, 60.0) | 59.1 (55.6, 62.7) | |
| Mongolia, 2006 2 | 202 | 20 (7, 36) | 0.79 (0.74, 0.83) | 26.2 (20.2, 32.3) | |||
| Malawi, 2016 1 | 1084 | 32.5 (6, 59) | 0.86 (0.82, 0.90) | 1.00 (0.82, 1.19) | 23.7 (18.6, 28.7) | 55.9 (50.3, 61.5) | 57.0 (51.2, 62.7) |
| Mexico, 2012 | 2512 | 39.1 (12, 60) | 0.93 (0.91, 0.96) | 11.6 (9.3, 14.0) | |||
| Nigeria, 2005 | 1420 | 33.4 (6, 60) | 1.22 (1.17, 1.26) | 24.0 (20.5, 27.5) | |||
| Pakistan, 2011 | 7318 | 27.3 (6, 59) | 0.67 (0.65, 0.69) | 35.3 (33.8, 36.8) | |||
| Papua New Guinea, 2005 | 871 | 31.4 (6, 60) | 0.87 (0.84, 0.90) | 31.6 (27.2, 36.0) | 54.1 (49.4, 58.9) | 57.0 (52.6, 61.5) | |
| Philippines, 2011 | 1767 | 15 (6, 24) | 1.03 (1.01, 1.05) | 13.9 (11.6, 16.2) | 21.2 (17.7, 24.6) | 26.0 (22.4, 29.5) | |
| Vietnam, 2010 | 360 | 37.3 (10, 60) | 1.16 (1.11, 1.21) | 12.8 (9.7, 15.8) | |||
| School Age Children | |||||||
| Bangladesh, 2010 | 1271 | 9.4 (6, 14) | 0.86 (0.83, 0.88) | 4.3 (2.0, 6.6) | 15.4 (12.1, 18.7) | 16.0 (12.6, 19.4) | |
| Ecuador, 2012 | 3281 | 7.6 (5, 15) | 0.92 (0.90, 0.94) | 7.7 (5.7, 9.7) | |||
| Malawi, 2016 1 | 750 | 9.5 (5, 15) | 0.98 (0.94, 1.01) | 1.11 (1.02, 1.19) | 16.2 (12.3, 20.2) | 32.9 (28.6, 37.3) | 35.0 (30.2, 39.8) |
| Mexico, 2012 | 3144 | 8.6 (5, 12) | 1.17 (1.15, 1.18) | 7.7 (6.4, 9.0) | |||
| United Kingdom, 2014 | 556 | 9.9 (5, 14) | 1.16 (1.12, 1.19) | 4.6 (2.2, 6.9) | |||
| United States, 2006 | 3089 | 10.8 (6, 15) | 1.33 (1.32, 1.35) | 6.6 (5.2, 8.1) | |||
| Women of Reproductive Age | |||||||
| Afghanistan, 2013 | 1046 | 30.9 (15, 49) | 1.13 (1.07, 1.19) | 12.8 (10.4, 15.2) | 11.6 (8.8, 14.4) | 19.3 (15.8, 22.8) | |
| Azerbaijan, 2013 | 2656 | 32.1 (15, 50) | 1.46 (1.44, 1.49) | 13.2 (11.3, 15.1) | 31.3 (29, 33.6) | 34.5 (32.0, 36.9) | |
| Bangladesh, 2012 | 897 | 29.7 (15, 49) | 1.12 (1.07, 1.16) | 5.7 (3.2, 8.2) | 12.8 (8.9, 16.6) | 16.7 (12.4, 20.9) | |
| Cambodia, 2014 | 705 | 30.2 (16, 49) | 1.96 (1.74, 2.18) | 9.5 (7.1, 11.8) | 33.5 (24.9, 42.2) | 36.7 (27.3, 46.0) | |
| Cameroon, 2009 1 | 751 | 27.2 (15, 48) | 1.44 (1.40, 1.48) | 1.24 (1.16, 1.32) | 17.8 (14.8, 20.7) | 7.2 (5.1, 9.3) | 19.7 (16.6, 22.9) |
| Côte d’Ivoire, 2007 | 816 | 27.6 (15, 48) | 1.49 (1.44, 1.54) | 19.7 (16.5, 22.8) | 26.9 (23.5, 30.4) | 33.7 (29.6, 37.9) | |
| Ecuador, 2012 | 5979 | 33.2 (19, 49) | 1.27 (1.25, 1.28) | 19.0 (17.1, 21.0) | |||
| Liberia, 2011 | 1875 | 28.6 (15, 50) | 1.33 (1.30, 1.36) | 14.3 (12.1, 16.4) | 10.4 (8.7, 12.2) | 18.5 (16.2, 20.8) | |
| Malawi, 2016 1 | 753 | 28.1 (15, 49) | 1.39 (1.34, 1.44) | 1.39 (1.26, 1.53) | 7.5 (5.1, 9.9) | 10.7 (7.5, 13.8) | 13.0 (9.6, 16.4) |
| Pakistan, 2011 | 5929 | 30.8 (16, 49) | 0.84 (0.81, 0.88) | 12.0 (11.0, 13.0) | 24.1 (22.7, 25.6) | 31.6 (30.0, 33.1) | |
| Papua New Guinea, 2005 | 749 | 29.1 (15, 49) | 1.61 (1.57, 1.66) | 10.0 (7.5, 12.5) | 21.8 (18.1, 25.6) | 24.8 (21.0, 28.7) | |
| United Kingdom, 2014 | 875 | 34.6 (15, 49) | 1.61 (1.55, 1.68) | 15.8 (12.5, 19.1) | |||
| United States, 2006 | 3145 | 33.5 (15, 50) | 1.74 (1.72, 1.77) | 25.7 (23.5, 27.8) | |||
| Vietnam, 2010 | 1434 | 32.3 (15, 49) | 1.62 (1.59, 1.65) | 6.7 (5.5, 7.9) | |||
| Approach | Absolute Median (Range) Percentage Point (pp) Difference for Surveys That Measured both CRP and AGP | Absolute Median (Range) Percentage Point (pp) Difference for Surveys That Measured either CRP or AGP | ||
|---|---|---|---|---|
| RBP 1 | Retinol | RBP 1 | Retinol | |
| Preschool Children | ||||
| Sample size (No. of surveys) | 10 | 2 | - | 6 |
| Exclusion | −12.0 pp (−18.0 pp, −5.5 pp) | −6.6 pp (−8.3 pp, −4.9 pp) | - | −3.4 pp (−7.2 pp, −0.2 pp) |
| ICF | −10.1 pp (−13.6 pp, −5.1 pp) | −4.5 pp (−6.1 pp, −2.8 pp) | - | −3.6 pp (−4.9 pp, −0.5 pp) |
| IRC | −16.4 pp (−22.1 pp, −6.0 pp) | −13.1 pp (−15.9 pp, −10.2 pp) | - | −6.4 pp (−9.9 pp, −1.1 pp) |
| School-Aged children | ||||
| Sample size (No. of surveys) | 1 | 1 | - | 4 |
| Exclusion | −6.6 pp | −4.0 pp | - | −0.5 pp (−2.0 pp, −0.3 pp) |
| ICF | −7.1 pp | −3.0 pp | - | −0.5 pp (−1.6 pp, −0.1 pp) |
| IRC | −8.8 pp | −6.9 pp | - | −0.8 pp (−3.9 pp, −0.2 pp) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larson, L.M.; Guo, J.; Williams, A.M.; Young, M.F.; Ismaily, S.; Addo, O.Y.; Thurnham, D.; Tanumihardjo, S.A.; Suchdev, P.S.; Northrop-Clewes, C.A. Approaches to Assess Vitamin A Status in Settings of Inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project. Nutrients 2018, 10, 1100. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081100
Larson LM, Guo J, Williams AM, Young MF, Ismaily S, Addo OY, Thurnham D, Tanumihardjo SA, Suchdev PS, Northrop-Clewes CA. Approaches to Assess Vitamin A Status in Settings of Inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project. Nutrients. 2018; 10(8):1100. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081100
Chicago/Turabian StyleLarson, Leila M., Junjie Guo, Anne M. Williams, Melissa F. Young, Sanober Ismaily, O Yaw Addo, David Thurnham, Sherry A. Tanumihardjo, Parminder S. Suchdev, and Christine A. Northrop-Clewes. 2018. "Approaches to Assess Vitamin A Status in Settings of Inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project" Nutrients 10, no. 8: 1100. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10081100