Plasma 25-Hydroxy Vitamin D Is Not Associated with Either Cognitive Function or Academic Performance in Adolescents

Abstract
:1. Introduction
2. Methods
2.1. Cognitive Function Tests and Students’ Academic Performance
2.2. Blood Collection and Biochemical Analyses
2.3. Statistical Methods
3. Results
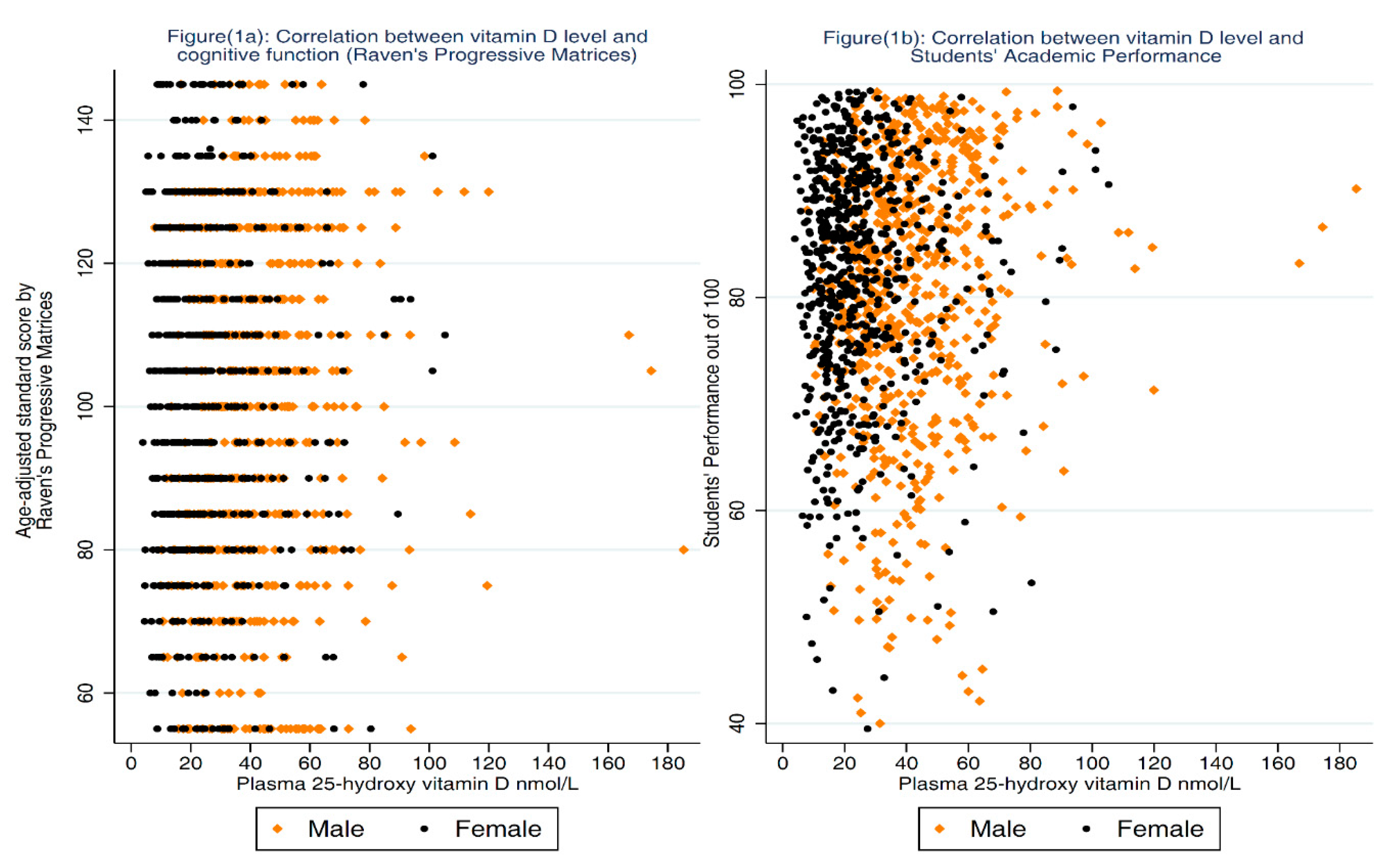
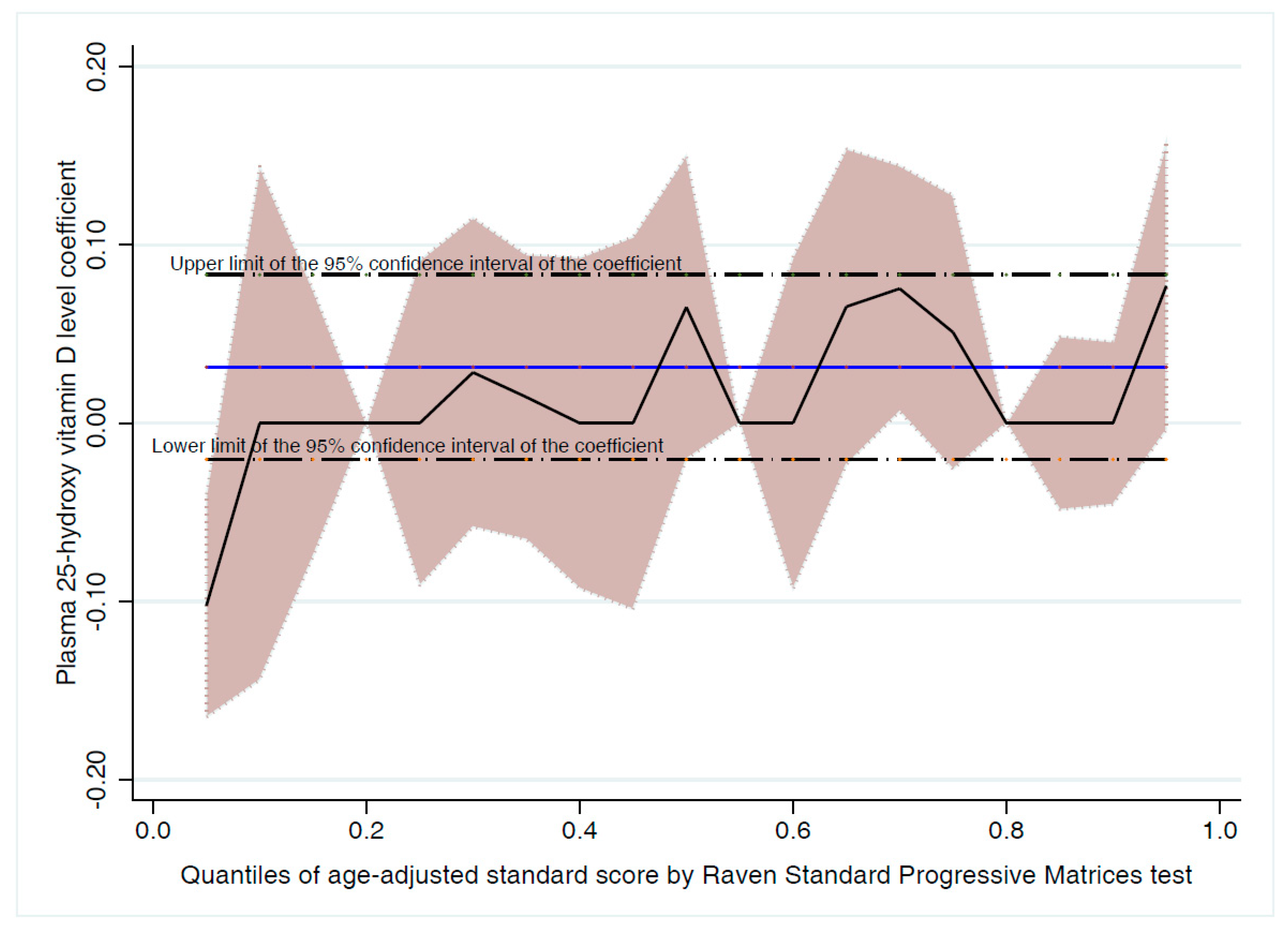
3.1. Association between 25-OH-D and Cognitive Function
3.2. Association between 25-OH-D and Academic Performance
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| 25-OH-D | 25-hydroxy vitamin D |
| ASC | age-adjusted standard score |
| CAP | College of American Pathologists |
| LC-MS/MS | liquid chromatography tandem mass spectrometry |
| PTH | parathyroid hormone |
| RCT | randomized control trials |
| SP | school performance |
| SPM | Standard Progressive Matrices |
| VD | vitamin D |
| VDR | vitamin D receptors |
References
- Van Schoor, N.; Lips, P. Global overview of vitamin D status. Endocrinol. Metab. Clin. N. Am. 2017, 46, 845–870. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Brannon, P.M.; Rosen, C.J.; Taylor, C.L. Vitamin D deficiency—Is there really a pandemic? N. Engl. J. Med. 2016, 375, 1817–1820. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.; Gupta, P. Vitamin D deficiency: Is the pandemic for real? Indian J. Community Med. 2015, 40, 215–217. [Google Scholar] [PubMed]
- Stokes, C.S.; Lammert, F. Vitamin D supplementation: Less controversy, more guidance needed. F1000Res 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Boil. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Al-Taiar, A.; Rahman, A.; Al-Sabah, R.; Shaban, L.; Al-Harbi, A. Vitamin D status among adolescents in kuwait: A cross-sectional study. BMJ Open 2018, 8, e021401. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R. Extra-skeletal effects of vitamin D. Front. Horm. Res. 2018, 50, 72–88. [Google Scholar] [PubMed]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2014, CD007470. [Google Scholar] [CrossRef] [PubMed]
- Straube, S.; Derry, S.; Straube, C.; Moore, R.A. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst. Rev. 2015, CD007771. [Google Scholar] [CrossRef] [PubMed]
- Beveridge, L.A.; Khan, F.; Struthers, A.D.; Armitage, J.; Barchetta, I.; Bressendorff, I.; Cavallo, M.G.; Clarke, R.; Dalan, R.; Dreyer, G.; et al. Effect of vitamin D supplementation on markers of vascular function: A systematic review and individual participant meta-analysis. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Das, R.R.; Singh, M.; Naik, S.S. Vitamin D as an adjunct to antibiotics for the treatment of acute childhood pneumonia. Cochrane Database Syst. Rev. 2018, 7, CD011597. [Google Scholar] [CrossRef] [PubMed]
- Lardner, A.L. Vitamin D and hippocampal development-the story so far. Front. Mol. Neurosci. 2015, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the vitamin D receptor and 1 alpha-hydroxylase in human brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Prufer, K.; Veenstra, T.D.; Jirikowski, G.F.; Kumar, R. Distribution of 1,25-dihydroxyvitamin D3 receptor immunoreactivity in the rat brain and spinal cord. J. Chem. Neuroanat. 1999, 16, 135–145. [Google Scholar] [CrossRef]
- Miller, W.L.; Portale, A.A. Vitamin d 1 alpha-hydroxylase. Trends Endocrinol. Metab. TEM 2000, 11, 315–319. [Google Scholar] [CrossRef]
- Garcion, E.; Sindji, L.; Leblondel, G.; Brachet, P.; Darcy, F. 1,25-dihydroxyvitamin D3 regulates the synthesis of gamma-glutamyl transpeptidase and glutathione levels in rat primary astrocytes. J. Neurochem. 1999, 73, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Gooch, H.; Petty, A.; McGrath, J.J.; Eyles, D. Vitamin D and the brain: Genomic and non-genomic actions. Mol. Cell. Endocrinol. 2017, 453, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Di Somma, C.; Scarano, E.; Barrea, L.; Zhukouskaya, V.V.; Savastano, S.; Mele, C.; Scacchi, M.; Aimaretti, G.; Colao, A.; Marzullo, P. Vitamin D and neurological diseases: An endocrine view. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Dursun, E.; Feron, F.; Gezen-Ak, D.; Kalueff, A.V.; Littlejohns, T.; Llewellyn, D.J.; Millet, P.; Scott, T.; Tucker, K.L.; et al. ‘Vitamin D and cognition in older adults’: Updated international recommendations. J. Intern. Med. 2015, 277, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Goodwill, A.M.; Szoeke, C. A systematic review and meta-analysis of the effect of low vitamin D on cognition. J. Am. Geriatr. Soc. 2017, 65, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- Tolppanen, A.M.; Williams, D.; Lawlor, D.A. The association of circulating 25-hydroxyvitamin D and calcium with cognitive performance in adolescents: Cross-sectional study using data from the third national health and nutrition examination survey. Paediatr. Périnat. Epidemiol. 2011, 25, 67–74. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.; Scragg, R.; Chant, D.; Eyles, D.; Burne, T.; Obradovic, D. No association between serum 25-hydroxyvitamin D3 level and performance on psychometric tests in NHANES III. Neuroepidemiology 2007, 29, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Cukic, I.; Brett, C.E.; Calvin, C.M.; Batty, G.D.; Deary, I.J. Childhood IQ and survival to 79: Follow-up of 94% of the Scottish mental survey 1947. Intelligence 2017, 63, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Batty, G.D.; Clark, H.; McIntyre, S.; Leon, D.A. Association of childhood intelligence with risk of coronary heart disease and stroke: Findings from the Aberdeen Children of the 1950s cohort study. Eur. J. Epidemiol. 2008, 23, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Yaroch, A.L.; Dancel, M.; Saraiya, M.; Crane, L.A.; Buller, D.B.; Manne, S.; O’Riordan, D.L.; Heckman, C.J.; Hay, J.; et al. Measures of sun exposure and sun protection practices for behavioral and epidemiologic research. Arch. Dermatol. 2008, 144, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Lamparello, B.; Kruczek, K.; Anderson, E.J.; Hubbard, J.; Misra, M. Validation of a food frequency questionnaire for determining calcium and vitamin D intake by adolescent girls with anorexia nervosa. J. Am. Diet. Assoc. 2009, 109, 479–485, 485.e1–485.e3. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Rachaniotis, N.; Lari, M.; Al Mussabi, W. Validation of a food frequency questionnaire for vitamin D and calcium intake in healthy female college students. Food Nutr. Sci. 2014, 5, 2048–2052. [Google Scholar] [CrossRef]
- UEA. Youth Physical Activity Questionnaire. Available online: http://epi-meta.medschl.cam.ac.uk/includes/speedy/pdf/PhysicalActivity%20V4%20SPEEDY-3.pdf (accessed on 28 August 2015).
- Al-Hazzaa, H.M.; Al-Sobayel, H.I.; Musaiger, A.O. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int. J. Environ. Res. Public Health 2011, 8, 3810–3820. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Khalek, A.M. Reliability and factorial validity of the standard progressive matrices among Kuwaiti children ages 8 to 15 years. Percept. Mot. Skills 2005, 101, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Raven, J. Manual for Raven’s Progressive Matrices and Vocabullary Scale; Pearson Education: London, UK, 2000. [Google Scholar]
- Al-Harbi, A.N.; Khan, K.M.; Rahman, A. Developmental vitamin D deficiency affects spatial learning in wistar rats. J. Nutr. 2017, 147, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, W. Robust locally weighted fitting and smoothing scatterplots. J. Am. Stat. Assoc. 1979, 74, 829–836. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Society for Adolescent Health and Medicine. Recommended vitamin D intake and management of low vitamin D status in adolescents: A position statement of the society for adolescent health and medicine. J. Adolesc. Health 2013, 52, 801–803. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.F.; Amin, D.A.; Hamed, A.I.; Nassar, J.F.; Abou-Zeid, A.E.; Attaby, M.A. Vitamin D status and scholastic achievement in middle age childhood. J. Egypt. Soc. Parasitol. 2012, 42, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Ballester-Plane, J.; Laporta-Hoyos, O.; Macaya, A.; Poo, P.; Melendez-Plumed, M.; Vazquez, E.; Delgado, I.; Zubiaurre-Elorza, L.; Narberhaus, A.; Toro-Tamargo, E.; et al. Measuring intellectual ability in cerebral palsy: The comparison of three tests and their neuroimaging correlates. Res. Dev. Disabil. 2016, 56, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Tolppanen, A.M.; Sayers, A.; Fraser, W.D.; Lawlor, D.A. Association of serum 25-hydroxyvitamin D3 and D2 with academic performance in childhood: Findings from a prospective birth cohort. J. Epidemiol. Community Health 2012, 66, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Usdin, T.B.; Gruber, C.; Bonner, T.I. Identification and functional expression of a receptor selectively recognizing parathyroid hormone, the PTH2 receptor. J. Boil. Chem. 1995, 270, 15455–15458. [Google Scholar] [CrossRef]
- Joborn, C.; Hetta, J.; Niklasson, F.; Rastad, J.; Wide, L.; Agren, H.; Akerstrom, G.; Ljunghall, S. Cerebrospinal fluid calcium, parathyroid hormone, and monoamine and purine metabolites and the blood-brain barrier function in primary hyperparathyroidism. Psychoneuroendocrinology 1991, 16, 311–322. [Google Scholar] [CrossRef]
- Henderson, V.H.; Velleman, F.P. Building multiple regression models interactively. Biometrics 1981, 37, 391–411. [Google Scholar] [CrossRef]
- Jorde, R.; Waterloo, K.; Saleh, F.; Haug, E.; Svartberg, J. Neuropsychological function in relation to serum parathyroid hormone and serum 25-hydroxyvitamin D levels. The tromsø study. J. Neurol. 2006, 253, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Bjorkman, M.P.; Sorva, A.J.; Tilvis, R.S. Does elevated parathyroid hormone concentration predict cognitive decline in older people? Aging Clin. Exp. Res. 2010, 22, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Feart, C.; Helmer, C.; Merle, B.; Herrmann, F.R.; Annweiler, C.; Dartigues, J.F.; Delcourt, C.; Samieri, C. Associations of lower vitamin D concentrations with cognitive decline and long-term risk of dementia and alzheimer’s disease in older adults. Alzheimers Dement. 2017, 13, 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Matchar, D.B.; Chei, C.L.; Yin, Z.X.; Koh, V.; Chakraborty, B.; Shi, X.M.; Zeng, Y. Vitamin D levels and the risk of cognitive decline in Chinese elderly people: The Chinese longitudinal healthy longevity survey. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2016, 71, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, C.; Bi, W.G.; Leduc, L.; Tabatabaei, N.; Jantchou, P.; Luo, Z.C.; Audibert, F.; Nuyt, A.M.; Wei, S.Q. Prenatal vitamin D status and offspring’s growth, adiposity and metabolic health: A systematic review and meta-analysis. Br. J. Nutr. 2018, 119, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Pet, M.A.; Brouwer-Brolsma, E.M. The impact of maternal vitamin D status on offspring brain development and function: A systematic review. Adv. Nutr. 2016, 7, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Rose, G. Sick individuals and sick populations. Int. J. Epidemiol. 2001, 30, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogeser, M. Quantification of circulating 25-hydroxyvitamin D by liquid chromatography-tandem mass spectrometry. J. Steroid Biochem. Mol. Boil. 2010, 121, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Ali, M.; Al-Elq, A.H.; Al-Shaikh, I.H.; Al-Turki, H.A.; Al-Ali, A.K.; Al-Othman, A.A. Assessment of low vitamin D among Saudi Arabians. Did we overshoot the runway? Saudi Med. J. 2014, 35, 1243–1249. [Google Scholar] [PubMed]
- Lai, J.K.; Lucas, R.M.; Banks, E.; Ponsonby, A.L. Variability in vitamin D assays impairs clinical assessment of vitamin D status. Intern. Med. J. 2012, 42, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||
|---|---|---|
| Age in years, Mean (SD) years | 12.4 | (0.9) |
| n | (%) | |
| Gender | ||
| Male | 674 | (49.2) |
| Nationality | ||
| Kuwaiti | 1047 | (76.4) |
| Non-Kuwait | 323 | (23.6) |
| Father’s Education 1 | ||
| No formal education | 15 | (1.11) |
| Primary/Intermediate | 215 | (16.1) |
| Secondary (high school) | 330 | (24.7) |
| Diploma | 251 | (18.8) |
| University & above | 526 | (39.3) |
| Mother’s Education 2 | ||
| No formal education | 31 | (2.3) |
| Primary/Intermediate | 145 | (10.7) |
| Secondary (high school) | 294 | (21.9) |
| Diploma | 293 | (21.7) |
| University & above | 587 | (43.5) |
| Father’s Income 3 (Kuwaiti Dinars) | ||
| Less than 500 | 89 | (6.7) |
| 500 to 1000 | 291 | (22.0) |
| 1001 to 1500 | 414 | (31.3) |
| 1501 to 2000 | 213 | (16.1) |
| More than 2000 | 164 | (12.4) |
| Do not wish to tell | 153 | (11.6) |
| Mother’s Employment Status 4 | ||
| Housewife | 466 | (34.7) |
| Paid employment | 664 | (49.5) |
| Others | 212 | (15.8) |
| Housing 5 | ||
| Rented flat | 499 | (36.9) |
| Rented house | 159 | (11.8) |
| Owned flat | 55 | (4.1) |
| Owned house | 638 | (47.2) |
| Vitamin D Status | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
|---|---|---|---|---|---|
| β [95%CI] | β [95%CI] | β [95%CI] | β [95%CI] | β [95%CI] | |
| 25-OH-D levels nmol/L | 0.03 | 0.01 | 0.00 | 0.00 | −0.01 |
| [−0.02, 0.08] | [−0.04, 0.07] | [−0.05, 0.06] | [−0.05, 0.06] | [−0.07, 0.05] | |
| p-value | 0.23 | 0.70 | 0.95 | 0.85 | 0.73 |
| Q1 (25-OH-D < 19.2 nmol/L) (n = 337) | [Reference] | [Reference] | [Reference] | [Reference] | [Reference] |
| Q2 (25-OH-D ≥ 19.2 to <29.7 nmol/L) (n = 346) | 0.86 | 1.12 | −0.39 | 1.15 | 0.82 |
| [−2.65, 4.38] | [−2.32, 4.58] | [−4.28, 3.49] | [−2.29, 4.59] | [−2.82, 4.46] | |
| Q3 (25-OH-D from 29.7 to <44.1 nmol/L) (n = 344) | 2.67 | 2.29 | −0.26 | 2.69 | 0.84 |
| [−0.86, 6.19] | [−1.43, 6.02] | [−6.25−5.72] | [−1.03, 6.41] | [−3.24, 4.92] | |
| Q4 (25-OH-D ≥ 44.1 nmol/L) (n = 343) | 2.91 | 0.95 | −0.70 | 0.50 | −0.42 |
| [−0.62, 6.43] | [−3.00, 4.90] | [−7.92, 6.53] | [−3.47, 4.47] | [−4.82, 4.01] | |
| p-value | 0.30 | 0.67 | 1.00 | 0.45 | 0.88 |
| Severe deficiency (25-OH-D < 25 nmol/L) (n = 544) | [Reference] | [Reference] | [Reference] | [Reference] | [Reference] |
| Deficiency (25-OH-D ≥ 25 to <50 nmol/L) (n = 572) | 2.28 | 2.52 | 2.70 | 2.71 | 1.36 |
| [−0.46, 5.04] | [−0.39, 5.44] | [0.22, 5.63] | [−0.22, 5.63] | [−1.86, 4.59] | |
| Insufficiency (25-OH-D ≥ 50 to <75 nmol/L) (n = 205) | 1.40 | −0.66 | −0.93 | −0.94 | −1.53 |
| [−2.36, 5.16] | [−4.66, 3.34] | [−4.94, 3.09] | [−4.97, 3.08] | [−6.01, 2.94] | |
| Sufficiency (25-OH-D ≥ 75 nmol/L) (n = 49) | 5.46 | 4.98 | 2.79 | 3.02 | 1.47 |
| [−1.39, 12.31] | [−1.96, 11.92] | [−4.16, 9.74] | [−3.93, 9.98] | [−5.96, 8.91] | |
| p-value | 0.24 | 0.11 | 0.11 | 0.10 | 0.48 |
| Vitamin D Status | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
|---|---|---|---|---|---|
| β [95%CI] | β [95%CI] | β [95%CI] | β [95%CI] | β [95%CI] | |
| 25-OH-D levels nmol/L | 0.02 | −0.00 | −0.00 | −0.01 | −0.01 |
| [−0.01, 0.06] | [−0.03, 0.03] | [−0.04, 0.03] | [−0.04, 0.03] | [−0.04, 0.03] | |
| p-value | 0.22 | 0.94 | 0.77 | 0.67 | 0.69 |
| Q1 (25-OH-D < 19.2 nmol/L) (n = 337) | [Reference] | [Reference] | [Reference] | [Reference] | [Reference] |
| Q2 (25-OH-D ≥19.2 to <29.7 nmol/L) (n = 346) | 1.10 | 1.61 | 2.01 | 1.66 | 1.74 |
| [−1.54, 3.74] | [−0.34, 3.57] | [0.01, 4.01] | [−0.42, 3.75] | [−0.33, 3.80] | |
| Q3 (25-OH-D from 29.7 to <44.1 nmol/L) (n = 344) | 0.40 | 0.70 | 0.98 | 0.90 | 0.94 |
| [−2.15, 2.95] | [−1.58, 2.99] | [−1.26, 3.21] | [−1.39, 3.20] | [−1.41, 3.30] | |
| Q4 (25-OH-D ≥ 44.1 nmol/L) (n = 343) | 2.60 | 0.82 | 1.00 | 1.40 | 1.67 |
| [0.06, 5.25] | [−1.51, 3.14] | [−1.38, 3.38] | [−1.03, 3.83] | [−0.86, 4.19] | |
| p-value | 0.17 | 0.43 | 0.27 | 0.45 | 0.36 |
| Severe deficiency (25-OH-D < 25 nmol/L) (n = 544) | [Reference] | [Reference] | [Reference] | [Reference] | [Reference] |
| Deficiency (25-OH-D ≥ 25 to <50 nmol/L) (n = 572) | −0.30 | −1.36 | −0.84 | −0.99 | −0.94 |
| [−2.35, 1.75] | [−3.04, 0.32] | [−2.65, 0.96] | [−2.73, 0.73] | [−2.88, 0.99] | |
| Insufficiency (25-OH-D ≥ 50 to <75 nmol/L) (n = 205) | 2.30 | −0.34 | 0.31 | 0.28 | 0.38 |
| [−0.33, 4.93] | [−2.46, 1.77] | [−2.51, 1.88] | [−1.89, 2.47] | [−1.97, 2.73] | |
| Sufficiency (25-OH-D ≥ 75 nmol/L) (n = 49) | 3.10 | −1.71 | −1.27 | −2.12 | −1.99 |
| [−0.83, 7.03] | [−5.15, 1.73] | [−5.39, 2.84] | [−5.99, 1.74] | [−5.86, 1.89] | |
| p-value | 0.08 | 0.38 | 0.78 | 0.35 | 0.45 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, A.; Al-Taiar, A.; Shaban, L.; Al-Sabah, R.; Al-Harbi, A.; Mojiminiyi, O. Plasma 25-Hydroxy Vitamin D Is Not Associated with Either Cognitive Function or Academic Performance in Adolescents. Nutrients 2018, 10, 1197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10091197
Rahman A, Al-Taiar A, Shaban L, Al-Sabah R, Al-Harbi A, Mojiminiyi O. Plasma 25-Hydroxy Vitamin D Is Not Associated with Either Cognitive Function or Academic Performance in Adolescents. Nutrients. 2018; 10(9):1197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10091197
Chicago/Turabian StyleRahman, Abdur, Abdullah Al-Taiar, Lemia Shaban, Reem Al-Sabah, Anwar Al-Harbi, and Olusegun Mojiminiyi. 2018. "Plasma 25-Hydroxy Vitamin D Is Not Associated with Either Cognitive Function or Academic Performance in Adolescents" Nutrients 10, no. 9: 1197. https://0-doi-org.brum.beds.ac.uk/10.3390/nu10091197