The Effect of a Pilot Dietary Intervention on Pain Outcomes in Patients Attending a Tertiary Pain Service

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Consent and Ethics
2.3. Recruitment and Screening
2.4. Intervention Inclusions and Delivery
2.4.1. Personalized Dietary Consultations
2.4.2. Dietary Supplement (Active Fruit Juice)
2.4.3. Control Group Conditions
2.5. Measurements
2.5.1. Pain
2.5.2. Quality of Life
2.5.3. Dietary Intake
2.5.4. Process Evaluation
2.6. Data Analysis
3. Results
3.1. Number of Study Participants
3.2. Participant Demographics
3.3. Participants’ Description of Their Pain
3.4. Intervention Compliance
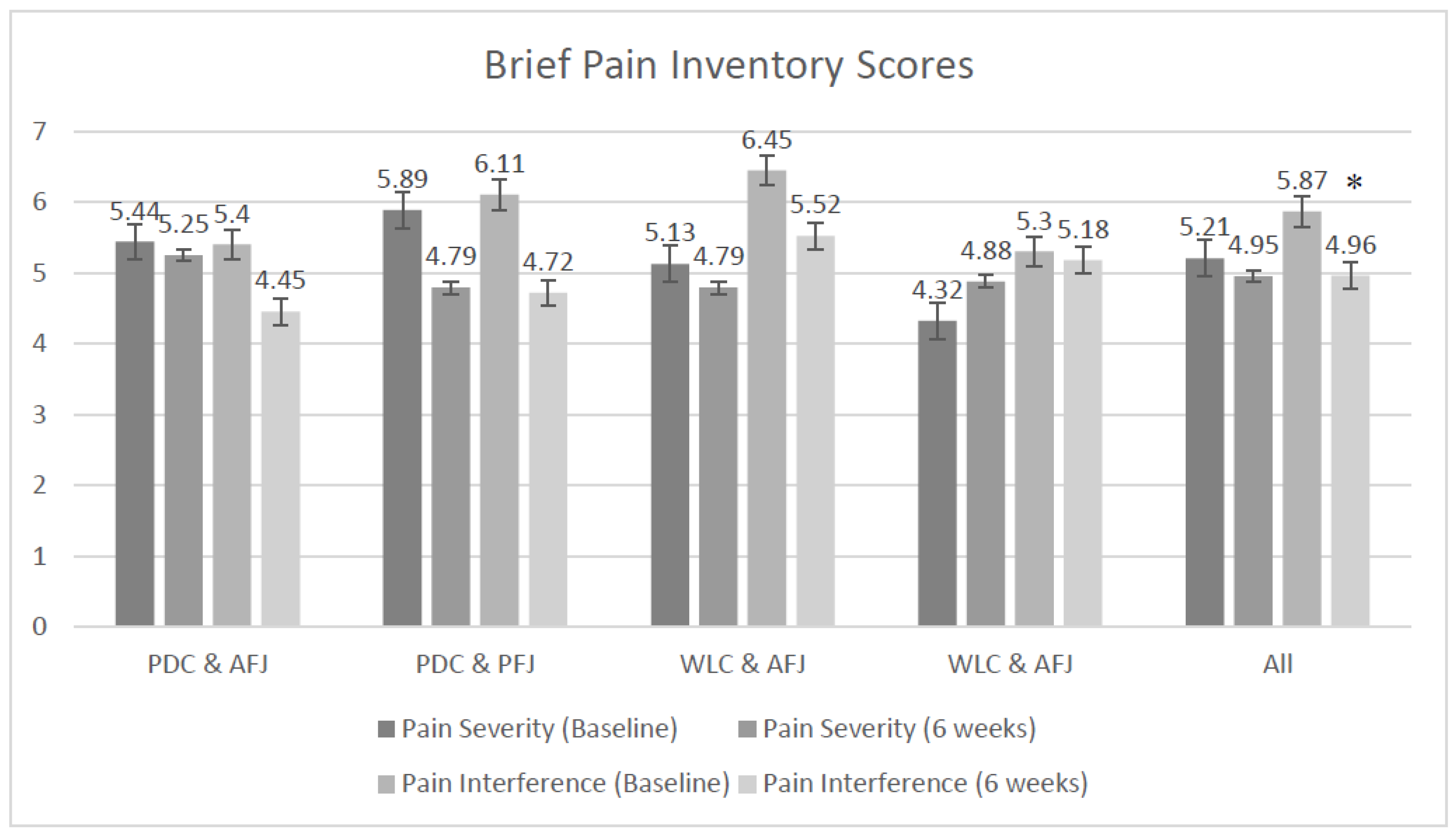
3.5. Pain Outcomes
3.6. Quality-of-Life Outcomes
3.7. Dietary Outcomes
3.8. Process Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Association for the Study of Pain. Descriptions of chronic pain syndromes and definitions of pain terms. Pain Suppl. 1986, 3, S1–S226. [Google Scholar]
- MBF Foundation; University of Sydney Pain Management Research Institute. The High Price of Pain: The Economic Impact of Persistent Pain in Australia; MBF Foundation: Sydney, Australia, 2007. [Google Scholar]
- Moseley, G.L.; Butler, D.S. Fifteen years of explaining pain: The past, present, and future. J. Pain 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. What is this thing called pain? J. Clin. Investig. 2010, 120, 3742–3744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashburn, M.A.; Staats, P.S. Management of chronic pain. Lancet 1999, 353, 1865–1869. [Google Scholar] [CrossRef]
- Brain, K.; Collins, C.; Burrows, L.T.; Hayes, C. Topical Concurrent Session 1G: The why, what and how of diet and nutrition for people experiencing chronic pain. In Proceedings of the Australian Pain Society 38th and New Zealand Pain Society Conjoint Annual Scientific Meeting, Sydney, Australia, 9 April 2018. [Google Scholar]
- Meleger, A.L.; Froude, C.K.; Walker, J., 3rd. Nutrition and eating behavior in patients with chronic pain receiving long-term opioid therapy. PM R 2014, 6, 7–12. [Google Scholar] [CrossRef] [PubMed]
- VanDenKerkhof, E.G.; Macdonald, H.M.; Jones, G.T.; Power, C.; Macfarlane, G.J. Diet, lifestyle and chronic widespread pain: Results from the 1958 British Birth Cohort Study. Pain Res. Manag. 2011, 16, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Amy Janke, E.; Kozak, A.T. “The more pain I have, the more I want to eat”: Obesity in the context of chronic pain. Obesity (Silver Spring) 2012, 20, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.; Naylor, R.; Egger, G. Understanding chronic pain in a lifestyle context: The emergence of the whole-person approach. Am. J. Lifestyle Med. 2012, 6, 421–428. [Google Scholar] [CrossRef]
- Seaman, D.R. The diet-induced proinflammatory state: A cause of chronic pain and other degenerative diseases? J. Manip. Physiol. 2002, 25, 168–179. [Google Scholar] [CrossRef]
- Brain, K.; Burrows, T.L.; Rollo, M.E.; Chai, L.K.; Clarke, E.D.; Hayes, C.; Hodson, F.J.; Collins, C.E. A systematic review and meta-analysis of nutrition interventions for chronic noncancer pain. J. Hum. Nutr. Diet. 2018. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliot, D.L.; Kuehl, K.S.; Jones, K.D.; Dulacki, K. Using an eccentric exercise-testing protocol to assess the beneficial effects of tart cherry juice in fibromyalgia patients. Integr. Med. 2010, 9, 24–29. [Google Scholar]
- Schumacher, H.; Pullman-Mooar, S.; Gupta, S.; Dinnella, J.; Kim, R. Randomized double-blind crossover study of the efficacy of a tart cherry juice blend in treatment of osteoarthritis (OA) of the knee. Osteoarthr. Cartil. 2013, 21, 1035–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed]
- Mazza, G.; Miniati, E. Anthocyanins in Fruits, Vegetables, and Grains; CRC Press: Boca Raton, FL, USA, 1993. [Google Scholar]
- Mulabagal, V.; Lang, G.A.; DeWitt, D.L.; Dalavoy, S.S.; Nair, M.G. Anthocyanin content, lipid peroxidation and cyclooxygenase enzyme inhibitory activities of sweet and sour cherries. J. Agric. Food Chem. 2009, 57, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Ou, B.; Bosak, K.N.; Brickner, P.R.; Iezzoni, D.G.; Seymour, E.M. Processed tart cherry products—Comparative phytochemical content, in vitro antioxidant capacity and in vitro anti-inflammatory activity. J. Food Sci. 2012, 77, H105–H112. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Nair, M.G.; Strasburg, G.M.; Chang, Y.C.; Booren, A.M.; Gray, J.I.; DeWitt, D.L. Antioxidant and antiinflammatory activities of anthocyanins and their aglycon, cyanidin, from tart cherries. J. Nat. Prod. 1999, 62, 294–296. [Google Scholar] [CrossRef]
- Ducharme, N.G.; Fortier, L.A.; Kraus, M.S.; Hobo, S.; Mohammed, H.O.; McHugh, M.P.; Hackett, R.P.; Soderholm, L.V.; Mitchell, L.M. Effect of a tart cherry juice blend on exercise-induced muscle damage in horses. Am. J. Vet. Res. 2009, 70, 758–763. [Google Scholar] [CrossRef]
- He, Y.H.; Zhou, J.; Wang, Y.S.; Xiao, C.; Tong, Y.; Tang, J.C.; Chan, A.S.; Lu, A.P. Anti-inflammatory and anti-oxidative effects of cherries on Freund’s adjuvant-induced arthritis in rats. Scand. J. Rheumatol. 2006, 35, 356–358. [Google Scholar] [CrossRef]
- Tall, J.M.; Seeram, N.P.; Zhao, C.; Nair, M.G.; Meyer, R.A.; Raja, S.N. Tart cherry anthocyanins suppress inflammation-induced pain behavior in rat. Behav. Brain Res. 2004, 153, 181–188. [Google Scholar] [CrossRef]
- Kelley, D.S.; Adkins, Y.; Laugero, K.D. A Review of the Health Benefits of Cherries. Nutrients 2018, 10, 368. [Google Scholar] [CrossRef] [PubMed]
- Schell, J.; Scofield, R.H.; Barrett, J.R.; Kurien, B.T.; Betts, N.; Lyons, T.J.; Zhao, Y.D.; Basu, A. Strawberries Improve Pain and Inflammation in Obese Adults with Radiographic Evidence of Knee Osteoarthritis. Nutrients 2017, 9, 949. [Google Scholar] [CrossRef] [PubMed]
- Igwe, E.O.; Charlton, K.E.; Roodenrys, S.; Kent, K.; Fanning, K.; Netzel, M.E. Anthocyanin-rich plum juice reduces ambulatory blood pressure but not acute cognitive function in younger and older adults: A pilot crossover dose-timing study. Nutr. Res. 2017, 47, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Norberto, S.; Silva, S.; Meireles, M.; Faria, A.; Pintado, M.; Calhau, C. Blueberry anthocyanins in health promotion: A metabolic overview. J. Funct. Foods 2013, 5, 1518–1528. [Google Scholar] [CrossRef]
- Seeram, N.P.; Momin, R.A.; Nair, M.G.; Bourquin, L.D. Cyclooxygenase inhibitory and antioxidant cyanidin glycosides in cherries and berries. Phytomedicine 2001, 8, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.; Charlton, K.; Roodenrys, S.; Batterham, M.; Potter, J.; Traynor, V.; Gilbert, H.; Morgan, O.; Richards, R. Consumption of anthocyanin-rich cherry juice for 12 weeks improves memory and cognition in older adults with mild-to-moderate dementia. Eur. J. Nutr. 2017, 56, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Neveu, V.; Perez-Jiménez, J.; Vos, F.; Crespy, V.; du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef]
- Kelly, J.T.; Reidlinger, D.P.; Hoffmann, T.C.; Campbell, K.L. Telehealth methods to deliver dietary interventions in adults with chronic disease: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 104, 1693–1702. [Google Scholar] [CrossRef]
- Rollo, M.E.; Hutchesson, M.J.; Burrows, T.L.; Krukowski, R.A.; Harvey, J.R.; Hoggle, L.B.; Collins, C.E. Video Consultations and Virtual Nutrition Care for Weight Management. J. Acad. Nutr. Diet. 2015, 115, 1213–1225. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. 2018. Nutrition Care Process. Available online: https://www.andeal.org/ncp (accessed on 29 August 2018).
- Lacey, K.; Pritchett, E. Nutrition Care Process and Model: ADA adopts road map to quality care and outcomes management. J. Am. Diet. Assoc. 2003, 103, 1061–1072. [Google Scholar] [CrossRef]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Page, P. Beyond statistical significance: Clinical interpretation of rehabilitation research literature. Int. J. Sports Phys. 2014, 9, 726–736. [Google Scholar]
- Dworkin, R.H.; Turk, D.C.; McDermott, M.P.; Peirce-Sandner, S.; Burke, L.B.; Cowan, P.; Farrar, J.T.; Hertz, S.; Raja, S.N.; Rappaport, B.A.; et al. Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations. Pain 2009, 146, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Inc, A. Scopia ®; Avaya Inc.: Santa Clara, CA, USA, 2018. [Google Scholar]
- Collins, C.E.; Burrows, T.L.; Rollo, M.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Hutchesson, M.J. The comparative validity and reproducibility of a diet quality index for adults: The Australian Recommended Food Score. Nutrients 2015, 7, 785–798. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council; Australian Government Department of Health and Ageing; New Zealand Ministry Health. Nutrient Reference Values. 2018. Available online: https://www.nrv.gov.au/ (accessed on 6 November 2018).
- Boyer, J.; Liu, R.H. Apple phytochemicals and their health benefits. Nutr. J. 2004, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Hobba, G. (Borenore) Apple Juice for Pain Study. Personal Communication, 2018. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Keller, S.; Bann, C.M.; Dodd, S.L.; Schein, J.; Mendoza, T.R.; Cleeland, C.S. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin. J. Pain 2004, 20, 309–318. [Google Scholar] [CrossRef]
- Tardif, H.; Arnold, C.; Hayes, C.; Eagar, K. Establishment of the Australasian Electronic Persistent Pain Outcomes Collaboration. Pain Med. 2016, 18, 1007–1018. [Google Scholar] [CrossRef]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Hobden, E.; Stiell, I.G.; Wells, G.A. Clinically important change in the visual analog scale after adequate pain control. Acad. Emerg. Med. 2003, 10, 1128–1130. [Google Scholar] [CrossRef]
- National Health and Medical Research Council; Australian Government Department of Health and Ageing; New Zealand Ministry Health. Recommendations to Reduce Chronic Disease Risk: Summary. 2017. Available online: https://www.nrv.gov.au/chronic-disease/summary (accessed on 6 November 2018).
- National Health and Medical Research Council; Australian Government Department of Health and Ageing; New Zealand Ministry Health. Macronutrient Balance. 2014. Available online: https://www.nrv.gov.au/chronic-disease/macronutrient-balance (accessed on 6 November 2018).
- Electronic Persistent Pain Outcomes Collaboration Annual Data Report 2016. Available online: https://ahsri.uow.edu.au/content/groups/public/@web/@chsd/@aroc/documents/doc/uow240735.pdf (accessed on 6 November 2018).
- Williams, R.L.; Rollo, M.E.; Schumacher, T.; Collins, C.E. Diet Quality Scores of Australian Adults Who Have Completed the Healthy Eating Quiz. Nutrients 2017, 9, 880. [Google Scholar] [CrossRef] [PubMed]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef]
- Brain, K.; Burrows, T.; Rollo, M.E.; Hayes, C.; Hodson, F.J.; Collins, C.E. Population Characteristics in a Tertiary Pain Service Cohort Experiencing Chronic Non-Cancer Pain: Weight Status, Comorbidities, and Patient Goals. Healthcare 2017, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Food and Nutrients, 2011–2012; Australian Bureau of Statistics: Canberra, Australia, 2014.
- Neil, C.; Keast, D.; Fulgoni, V.; Nicklas, T. Food Sources of Energy and Nutrients among Adults in the US: NHANES 2003–2006. Nutrients 2012, 4, 2097. [Google Scholar] [CrossRef]
- Ocké, M.C.; Larrañaga, N.; Grioni, S.; van den Berg, S.W.; Ferrari, P.; Salvini, S.; Benetou, V.; Linseisen, J.; Wirfält, E.; Rinaldi, S.; et al. Energy intake and sources of energy intake in the European Prospective Investigation into Cancer and Nutrition. Eur. J. Clin. Nutr. 2009, 63, S3. [Google Scholar] [CrossRef]
- Hrobjartsson, A.; Gotzsche, P.C. Placebo interventions for all clinical conditions. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef] [PubMed]
- Jubb, J.; Bensing, J.M. The sweetest pill to swallow: How patient neurobiology can be harnessed to maximise placebo effects. Neurosci. Biobehav. Rev. 2013, 37, 2709–2720. [Google Scholar] [CrossRef]
- Carvalho, C.; Caetano, J.M.; Cunha, L.; Rebouta, P.; Kaptchuk, T.J.; Kirsch, I. Open-label placebo treatment in chronic low back pain: A randomized controlled trial. Pain 2016, 157, 2766–2772. [Google Scholar] [CrossRef] [PubMed]
- Vase, L.; Skyt, I.; Hall, K.T. Placebo, nocebo, and neuropathic pain. Pain 2016, 157 (Suppl. 1), S98–S105. [Google Scholar] [CrossRef]
- Cardenas, D.D.; Warms, C.A.; Turner, J.A.; Marshall, H.; Brooke, M.M.; Loeser, J.D. Efficacy of amitriptyline for relief of pain in spinal cord injury: Results of a randomized controlled trial. Pain 2002, 96, 365–373. [Google Scholar] [CrossRef]
- Robinson, L.R.; Czerniecki, J.M.; Ehde, D.M.; Edwards, W.T.; Judish, D.A.; Goldberg, M.L.; Campbell, K.M.; Smith, D.G.; Jensen, M.P. Trial of amitriptyline for relief of pain in amputees: Results of a randomized controlled study. Arch. Phys. Med. Rehabil. 2004, 85, 1–6. [Google Scholar] [PubMed]
- Hanley, M.A.; Jensen, M.P.; Ehde, D.M.; Robinson, L.R.; Cardenas, D.D.; Turner, J.A.; Smith, D.G. Clinically significant change in pain intensity ratings in persons with spinal cord injury or amputation. Clin. J. Pain 2006, 22, 25–31. [Google Scholar] [CrossRef]
- Trompetter, H.R.; Bohlmeijer, E.T.; Veehof, M.M.; Schreurs, K.M. Internet-based guided self-help intervention for chronic pain based on Acceptance and Commitment Therapy: A randomized controlled trial. J. Behav. Med. 2015, 38, 66–80. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PDC + AFJ (n = 17) | PDC + PFJ (n = 14) | WLC + AFJ (n = 15) | WLC + PFJ (n = 14) | Total (n = 60) | p-Value | |
|---|---|---|---|---|---|---|
| Female n (%) | 12 (70.6) | 10 (71.4) | 9 (60) | 10 (71.4) | 41 (68.3) | 0.896 |
| Male n (%) | 5 (29.4) | 4 (28.6) | 6 (40) | 4 (28.6) | 19 (31.7) | |
| Age | 48.24 ± 14.60 | 47.00 ± 15.66 | 49.27 ± 16.72 | 50.93 ± 13.85 | 48.83 ± 14.92 | 0.930 |
| BMI | 33.14 ± 8.31 | 32.83 ± 8.15 | 33.43 ± 5.82 | 30.78 ± 8.74 | 32.59 ± 7.70 | 0.561 |
| Employment n (%) | 0.088 | |||||
| - Unemployed (due to pain) | 7 (41.2) | 4 (28.6) | 5 (33.3) | 0 (0) | 16 (26.7) | |
| - Retired | 3 (17.6) | 2 (14.3) | 4 (26.7) | 3 (21.4) | 12 (20) | |
| - Part-time paid work | 0 (0) | 3 (21.4) | 3 (20.0) | 4 (28.6) | 10 (16.7) | |
| - Unemployed (not due to pain) | 0 (0) | 2 (14.3) | 0 (0) | 3 (21.4) | 5 (8.3) | |
| - Home duties | 1 (5.9) | 2 (14.3) | 0 (0) | 1 (7.1) | 4 (6.7) | |
| - Full-time paid work | 2 (11.8) | 1 (7.1) | 0 (0) | 1 (7.1) | 4 (6.7) | |
| - Studying | 2 (11.8) | 0 (0) | 2 (13.3) | 0 (0) | 4 (6.7) | |
| - At work (limited hours/duties) | 1 (5.9) | 0 (0) | 1 (6.7) | 1 (7.1) | 3 (5.0) | |
| - On leave from work due to pain | 1 (5.9) | 0 (0) | 0 (0) | 1 (7.1) | 2 (3.3) | |
| Outcome Variable (mean ± SE *) | Time Point | PDC + AFJ | PDC + PFJ | WLC + AFJ | WLC + PFJ | Total | Time F Stat (p-Value) | Group F Stat (p-Value) | Group × Time F Stat (p-Value) |
|---|---|---|---|---|---|---|---|---|---|
| Number of participants | Baseline | 17 | 14 | 15 | 14 | 60 | |||
| 6 weeks | 11 | 8 | 13 | 10 | 42 | ||||
| Number of juice bottles consumed (Maximum 42) | 6 weeks | 39.64 ± 1.89 | 41.00 ± 0.76 | 41.46 ± 0.31 | 41.90 ± 0.10 | 41.00 ± 3.39 | |||
| Telehealth attendance | N/A | 12 | 7 | N/A | N/A | N/A | |||
| Pain | |||||||||
| VAS † | Baseline | 48.24 ± 5.31 | 52.00 ± 5.85 | 45.40 ± 5.65 | 47.64 ± 5.85 | 48.27 ± 2.75 | 1.16 (0.254) | 0.102 (0.959) | 0.113 (0.952) |
| 6 weeks | 43.87 ± 6.39 | 44.99 ± 7.43 | 43.61 ± 6.00 | 45.68 ± 6.74 | 44.57 ± 3.20 | ||||
| ∆6 week − baseline | −4.37 ± 6.71 | −7.02 ± 7.77 | −1.78 ± 6.39 | −1.96 ± 7.11 | −3.69 ± 3.37 | ||||
| PSEQ ^ | Baseline | 26.82 ± 3.07 | 21.29 ± 3.38 | 26.87 ± 3.27 | 25.21 ± 3.38 | 25.17 ± 1.62 | 8.835 (0.004) | 0.606 (0.613) | 1.181 (0.321) |
| 6 weeks | 35.21 ± 3.74 | 33.61 ± 4.37 | 30.75 ± 3.48 | 26.41 ± 3.94 | 31.37 ± 1.91 | ||||
| ∆6 week − baseline | 8.38 ± 4.15 | 12.32 ± 4.79 | 3.89 ± 3.67 | 1.19 ± 4.40 | 6.21 ± 2.16 | ||||
| PCS # | Baseline | 21.24 ± 3.27 | 27.43 ± 3.60 | 21.60 ± 3.48 | 24.93 ± 3.60 | 23.63 ± 1.72 | 4.074 (0.046) | 0.831 (0.480) | 0.073 (0.974) |
| 6 weeks | 18.23 ± 3.80 | 24.70 ± 4.37 | 17.63 ± 3.64 | 19.96 ± 4.03 | 19.86 ± 1.93 | ||||
| ∆6 week − baseline | −3.02 ± 3.49 | −2.73 ± 4.05 | −3.97 ± 3.28 | −4.97 ± 3.68 | −3.78 ± 1.75 | ||||
| Quality of life | |||||||||
| Physical function | Baseline | 45.59 ± 6.91 | 42.86 ± 7.62 | 36.67 ± 7.36 | 38.57 ± 7.62 | 41.08 ± 3.63 | 6.040 (0.016) | 0.689 (0.561) | 0.293 (0.830) |
| 6 weeks | 55.86 ± 7.87 | 56.22 ± 9.04 | 42.25 ± 7.66 | 43.79 ± 8.41 | 49.13 ± 4.02 | ||||
| ∆6 week − baseline | 10.28 ± 6.72 | 13.37 ± 7.83 | 5.58 ± 6.30 | 5.22 ± 7.09 | 8.05 ± 3.38 | ||||
| Role limitation (physical limits) | Baseline | 23.53 ± 7.97 | 12.50 ± 8.78 | 1.67 ± 8.48 | 10.71 ± 8.78 | 12.50 ± 4.28 | 14.133 (<0.001) | 2.053 (0.112) | 0.238 (0.870) |
| 6 weeks | 43.78 ± 9.76 | 34.78 ± 11.40 | 17.23 ± 9.06 | 39.48 ± 10.26 | 33.13 ± 5.03 | ||||
| ∆6 week − baseline | 20.25 ± 11.04 | 22.28 ± 12.74 | 15.57 ± 10.59 | 28.77 ± 11.73 | 20.63 ± 5.62 | ||||
| Role limitation (emotional issues) | Baseline | 50.98 ± 9.78 | 23.81 ± 10.77 | 26.67 ± 10.41 | 19.05 ± 10.77 | 31.11 ± 5.23 | 16.526 (<0.001) | 0.369 (0.776) | 1.838 (0.146) |
| 6 weeks | 53.41 ± 11.93 | 60.98 ± 13.94 | 55.10 ± 11.10 | 64.24 ± 12.56 | 58.25 ± 6.17 | ||||
| ∆6 week − baseline | 2.43 ± 13.31 | 37.17 ± 15.37 | 28.44 ± 12.75 | 45.19 ± 14.14 | 27.14 ± 7.02 | ||||
| Energy & fatigue | Baseline | 35.29 ± 4.84 | 33.21 ± 5.34 | 22.67 ± 5.16 | 30.71 ± 5.34 | 30.58 ± 2.62 | 4.650 (0.34) | 2.409 (0.072) | 0.639 (0.592) |
| 6 weeks | 48.56 ± 5.75 | 35.67 ± 6.67 | 26.95 ± 5.45 | 26.63 ± 6.09 | 39.92 ± 3.00 | ||||
| ∆6 week − baseline | 13.26 ± 5.75 | 2.46 ± 6.68 | 4.28 ± 5.45 | 5.92 ± 6.09 | 6.33 ± 2.97 | ||||
| Emotional wellbeing | Baseline | 60.71 ± 4.79 | 49.43 ± 5.28 | 54.40 ± 5.10 | 50.29 ± 5.28 | 54.07 ± 2.53 | 9.348 (0.003) | 0.488 (0.692) | 0.485 (0.693) |
| 6 weeks | 63.81 ± 5.67 | 61.86 ± 6.57 | 64.25 ± 5.38 | 60.76 ±6.00 | 62.80 ± 2.89 | ||||
| ∆6 week − baseline | 3.12 ± 5.62 | 12.43 ± 6.52 | 9.85 ± 5.32 | 10.48 ± 5.94 | 8.73 ± 2.83 | ||||
| Social functioning | Baseline | 27.94 ± 3.24 | 25.89 ± 3.58 | 16.67 ± 3.45 | 15.18 ± 3.58 | 21.67 ± 1.84 | 11.342 (0.001) | 5.285 (0.002) | 0.401 (0.753) |
| 6 weeks | 37.15 ± 3.98 | 33.36 ± 4.66 | 20.98 ± 3.69 | 26.30 ± 4.19 | 29.07 ± 2.16 | ||||
| ∆6 week − baseline | 9.21 ± 4.55 | 7.46 ± 5.25 | 4.32 ± 4.38 | 11.12 ± 4.84 | 7.40 ± 2.36 | ||||
| Pain | Baseline | 37.21 ± 4.83 | 48.39 ± 5.33 | 36.00 ± 5.15 | 36.96 ± 5.33 | 39.46 ± 2.57 | 0.345 (0.559) | 1.107 (0.350) | 0.768 (0.515) |
| 6 weeks | 44.91 ± 5.95 | 44.02 ± 6.96 | 33.65 ± 5.51 | 44.49 ± 6.25 | 41.27 ± 3.05 | ||||
| ∆6 week − baseline | 7.71 ± 6.92 | −4.38 ± 7.97 | −2.35 ± 6.66 | 7.52 ± 7.36 | 1.82 ± 3.59 | ||||
| General health | Baseline | 43.82 ± 4.82 | 38.93 ± 5.31 | 39.67 ± 5.13 | 27.86 ± 5.31 | 37.92 ± 2.65 | 15.839 (<0.001) | 2.567 (0.059) | 0.958 (0.416) |
| 6 weeks | 54.10 ± 5.40 | 53.59 ± 6.17 | 44.30 ± 5.31 | 33.98 ± 5.78 | 46.17 ± 2.89 | ||||
| ∆6 week − baseline | 10.27 ± 4.30 | 14.66 ± 5.02 | 4.63 ± 4.02 | 6.12 ± 4.54 | 8.25 ± 2.19 | ||||
| Outcome Variable (mean ± SE *) | Time Point | PDC + AFJ | PDC + PFJ | WLC + AFJ | WLC + PFJ | Total | Time F Stat (p-Value) | Group F Stat (p-Value) | Group × Time F Stat (p-Value) |
|---|---|---|---|---|---|---|---|---|---|
| Energy (kJ) (recommended intake) | Baseline | 9247.00 ± 932.65 | 9051.39 ± 1034.68 | 9046.07 ± 963.23 | 8138.00 ± 1034.98 | 8870.61 ± 496.16 | 4.210 (0.043) | 0.032 (0.992) | 1.263 (0.292) |
| 6 weeks | 7708.05 ± 1059.79 | 8399.67 ± 1149.39 | 7736.72 ± 1007.31 | 8487.45 ± 1094.25 | 8082.97 ± 239.08 | ||||
| ∆6 week − baseline | −1539.92 ± 785.52 | −651.72 ± 835.58 | −1309.35 ± 689.08 | 349.45 ± 753.60 | −787.64 ± 363.89 | ||||
| Carbohydrates (% of total energy (E)) 45–65% [51] | Baseline | 43.06 ± 2.32 | 46.31 ± 2.58 | 42.87 ± 2.40 | 45.31 ± 2.58 | 44.39 ± 1.24 | 1.703 (0.195) | 1.530 (0.212) | 0.440 (0.725) |
| 6 weeks | 40.33 ± 3.01 | 46.06 ± 3.21 | 38.04 ± 2.65 | 44.61 ± 2.90 | 42.26 ± 1.47 | ||||
| ∆6 week − baseline | −2.74 ± 2.29 | −0.25 ± 3.52 | −4.82 ± 2.97 | −0.70 ± 3.24 | −2.13 ± 1.63 | ||||
| Protein (% total E) 15–25% [51] | Baseline | 19.81 ± 1.08 | 18.23 ± 1.20 | 21.00 ± 1.12 | 17.08 ± 1.20 | 19.03 ± 0.58 | 0.128 (0.721) | 2.920 (0.038) | 0.769 (0.515) |
| 6 weeks | 18.50 ± 1.35 | 18.38 ± 1.44 | 22.22 ± 1.21 | 17.95 ± 1.32 | 19.26 ± 0.67 | ||||
| ∆6 week − baseline | −1.31 ± 1.32 | 0.15 ± 1.41 | 1.21 ± 1.18 | 0.88 ± 1.28 | 0.23 ± 0.65 | ||||
| Fat (% total E) 20–35% [51] | Baseline | 35.81 ± 1.61 | 33.69 ± 1.79 | 35.20 ± 1.66 | 33.08 ± 1.79 | 34.45 ± 0.86 | 0.633 (0.428) | 2.156 (0.099) | 3.290 (0.024) |
| 6 weeks | 30.09 ± 2.10 | 32.07 ± 2.23 | 39.13 ± 1.84 | 32.87 ± 2.01 | 33.54 ± 1.02 | ||||
| ∆6 week − baseline | −5.73 ± 2.30 ** | −1.62 ± 2.47 | 3.93 ± 2.09 | −0.21 ± 2.27 | −0.91 ± 1.14 | ||||
| Saturated fat (% total E) <10% [52] | Baseline | 14.63 ± 0.83 | 14.46 ± 0.92 | 15.33 ± 0.86 | 14.85 ± 0.92 | 14.82 ± 0.44 | 1.624 (0.206) | 2.259 (0.087) | 2.029 (0.116) |
| 6 weeks | 11.88 ± 1.08 | 13.70 ± 1.15 | 16.50 ± 0.95 | 14.21 ± 1.03 | 14.07 ± 0.53 | ||||
| ∆6 week − baseline | −2.75 ± 1.18 | −0.77 ± 1.26 | 1.17 ± 10.7 | −0.63 ± 1.16 | −0.75 ± 0.59 | ||||
| Alcohol (% total E) <5% [52] | Baseline | 2.00 ± 1.26 | 2.39 ± 1.39 | 1.47 ± 1.30 | 5.23 ± 1.39 | 2.77 ± 0.67 | 0.034 (0.854) | 2.485 (0.066) | 1.541 (0.209) |
| 6 weeks | 0.04 ± 1.46 | 4.03 ± 1.58 | 1.06 ± 1.37 | 5.52 ± 1.49 | 2.66 ± 0.74 | ||||
| ∆6 week − baseline | -1.96 ± 1.18 | 1.65 ± 1.26 | −0.40 ± 1.04 | 0.29 ± 1.14 | −0.12 ± 0.18 | ||||
| Saturated fat (% total fat) | Baseline | 44.81 ± 1.60 | 47.31 ± 1.77 | 47.40±1.65 | 48.54 ± 1.77 | 47.02 ± 0.85 | 3.085 (0.083) | 3.840 (0.012) | 1.054 (0.373) |
| 6 weeks | 38.85 ± 2.12 | 46.98 ± 2.25 | 46.20 ± 1.84 | 47.34 ± 2.01 | 44.84 ± 1.03 | ||||
| ∆6 week − baseline | −5.97 ± 2.48 | −0.32 ± 2.66 | −1.20 ± 2.27 | −1.20 ± 2.47 | −2.17 ± 1.24 | ||||
| MUFA (% total fat) | Baseline | 41.56 ± 1.28 | 40.31 ± 1.42 | 40.13 ± 1.32 | 39.54 ± 1.42 | 40.39 ± 0.68 | 0.109 (0.742) | 0.208 (0.891) | 1.444 (0.236) |
| 6 weeks | 37.80 ± 1.69 | 40.41 ± 1.80 | 41.55 ± 1.47 | 40.47 ± 1.61 | 40.06 ± 0.82 | ||||
| ∆6 week − baseline | −3.76 ± 1.99 | 0.10 ± 2.14 | 1.42 ± 1.83 | 0.94 ± 1.99 | −0.33 ± 0.99 | ||||
| PUFA (% total fat) | Baseline | 41.56 ± 1.28 | 40.31 ± 1.42 | 40.13 ± 1.32 | 39.54 ± 1.42 | 40.39 ± 0.68 | 0.109 (0.742) | 0.208 (0.891) | 1.444 (0.236) |
| 6 weeks | 37.80 ± 1.69 | 40.41 ± 1.80 | 41.55 ± 1.47 | 40.47 ± 1.61 | 40.06 ± 0.82 | ||||
| ∆6 week − baseline | −3.76 ± 1.99 | 0.10 ± 2.14 | 1.42 ± 1.83 | 0.94 ± 1.99 | −0.33 ± 0.99 | ||||
| Fiber (g) 25–30 g/day [51] | Baseline | 25.79 ± 2.41 | 25.17 ± 2.67 | 22.79 ± 2.49 | 19.71 ± 2.67 | 23.39 ± 1.28 | 2.365 (0.128) | 0.901 (0.444) | 0.593 (0.621) |
| 6 weeks | 23.54 ± 2.86 | 23.19 ± 3.08 | 19.15 ± 2.65 | 20.24 ± 2.88 | 21.53 ± 1.44 | ||||
| ∆6 week − baseline | −2.25 ± 2.47 | −1.98 ± 2.67 | −3.74 ± 2.18 | 0.54 ± 2.38 | −1.86 ± 1.21 | ||||
| Thiamin (mg) | Baseline | 1.53 ± 0.18 | 1.60 ± 0.20 | 1.47 ± 0.19 | 1.36 ± 0.20 | 1.49 ± 0.10 | 1.288 (0.260) | 0.398 (0.755) | 0.432 (0.730) |
| 6 weeks | 1.43 ± 0.21 | 1.57 ± 0.23 | 1.21 ± 0.20 | 1.34 ± 0.22 | 1.39 ± 0.12 | ||||
| ∆6 week − baseline | -0.10 ± 0.18 | −0.03 ± 0.20 | −0.26 ± 0.16 | −0.02 ± 0.18 | −0.10 ± 0.09 | ||||
| Riboflavin (mg) | Baseline | 2.19 ± 0.35 | 2.40 ± 0.38 | 2.56 ± 0.36 | 1.80 ± 0.38 | 2.24 ± 0.18 | 0.247 (0.620) | 0.602 (0.615) | 0.341 (0.796) |
| 6 weeks | 2.18 ± 0.37 | 2.38 ± 0.41 | 2.34 ± 0.37 | 1.84 ± 0.40 | 2.18 ± 0.19 | ||||
| ∆6 week − baseline | −0.02 ± 0.23 | −0.01 ± 0.24 | −0.23 ± 0.20 | 0.04 ± 0.22 | −0.06 ± 0.11 | ||||
| Niacin (mg) | Baseline | 26.99 ± 2.60 | 23.693 ± 2.88 | 24.16 ± 2.68 | 20.70 ± 2.88 | 23.87 ± 1.38 | 0.703 (0.404) | 0.358 (0.783) | 0.948 (0.421) |
| 6 weeks | 23.62 ± 3.05 | 23.73 ± 3.29 | 21.53 ± 2.84 | 22.44 ± 3.09 | 22.83 ± 1.54 | ||||
| ∆6 week − baseline | −3.37 ± 2.53 | 0.10 ± 2.69 | −2.63 ± 2.23 | 1.75 ± 2.44 | −1.04 ± 1.24 | ||||
| Calcium (mg) | Baseline | 971.25 ± 226.83 | 1160.92 ± 251.65 | 1483.19 ± 234.27 | 827.11 ± 251.65 | 1110.62 ± 120.63 | 0.340 (0.562) | 1.307 (0.277) | 0.256 (0.857) |
| 6 weeks | 972.89 ± 238.22 | 1051.28 ± 261.85 | 1445.13 ± 238.12 | 847.12 ± 256.59 | 1079.10 ± 124.46 | ||||
| ∆6 week − baseline | 1.63 ± 111.10 | −109.64 ± 117.95 | −38.06 ± 96.61 | 20.01 ± 105.78 | −31.51 ± 54.07 | ||||
| Iron (mg) | Baseline | 13.47 ± 1.46 | 13.06 ± 1.62 | 12.75 ± 1.51 | 11.22 ± 1.62 | 12.63 ± 0.78 | 1.545 (0.217) | 0.156 (0.925) | 1.978 (0.123) |
| 6 weeks | 11.40 ± 1.62 | 13.16 ± 1.77 | 11.04 ± 1.56 | 12.26 ± 1.69 | 11.96 ± 0.83 | ||||
| ∆6 week − baseline | −2.08 ± 1.09 | 0.10 ± 1.16 | −1.71 ± 0.96 | 1.04 ± 1.04 | −0.66 ± 0.53 | ||||
| Zinc (mg) | Baseline | 13.69 ± 1.56 | 12.65 ± 1.73 | 14.48 ± 1.61 | 11.02 ± 1.73 | 12.96 ± 0.83 | 1.410 (0.238) | 0.344 (0.793) | 1.506 (0.219) |
| 6 weeks | 11.68 ± 1.74 | 11.72 ± 1.89 | 13.27 ± 1.67 | 12.36 ± 1.81 | 12.26 ± 0.89 | ||||
| ∆6 week − baseline | −2.01 ± 1.21 | −0.93 ± 1.29 | −1.20 ± 1.06 | 1.34 ± 1.16 | 0.70 ± 0.59 | ||||
| Core (%E) | Baseline | 57.77 ± 3.31 | 57.77 ± 3.78 | 67.20 ± 3.52 | 47.92 ± 3.78 | 57.66 ± 1.80 | 13.286 (<0.001) | 6.186 (0.001) | 0.633 (0.596) |
| 6 weeks | 61.88 ± 3.94 | 61.67 ± 4.20 | 75.52 ± 3.68 | 52.34 ± 3.99 | 52.85 ± 1.98 | ||||
| ∆6 week − baseline | 4.11 ± 3.03 | 3.90 ± 3.05 | 8.32 ± 2.52 | 4.42 ± 2.75 | 5.19 ± 1.42 | ||||
| Energy-dense, nutrient-poor (%E) | Baseline | 42.24 ± 3.21 | 42.23 ± 3.78 | 32.80 ± 3.52 | 52.08 ± 3.78 | 42.34 ± 1.80 | 13.286 (<0.001) | 6.186 (0.001) | 0.633 (0.596) |
| 6 weeks | 38.12 ± 3.94 | 38.33 ± 4.20 | 24.48 ± 3.68 | 47.66 ± 3.99 | 37.15 ± 1.98 | ||||
| ∆6 week − baseline | −4.11 ± 3.03 | −3.90 ± 3.05 | −8.23 ± 2.52 | −4.42 ± 2.75 | −5.19 ± 1.42 | ||||
| ARFS †: Total (73 points) | Baseline | 30.69 ± 2.65 | 32.54 ± 2.94 | 27.60 ± 2.74 | 25.69 ± 2.94 | 29.13 ± 1.41 | 0.028 (0.868) | 1.080 (0.362) | 0.211 (0.888) |
| 6 weeks | 31.49 ± 3.06 | 31.95 ± 3.23 | 26.64 ± 2.85 | 26.82 ± 3.08 | 29.30 ± 1.53 | ||||
| ∆6 week − baseline | 0.81 ± 2.21 | −0.59 ± 2.22 | −0.66 ± 1.83 | 1.13 ± 2.00 | 0.17 ± 1.04 | ||||
| ARFS: Vegetables (21 points) | Baseline | 13.31 ± 1.33 | 11.77 ± 1.48 | 10.20 ± 1.37 | 10.92 ± 1.48 | 11.55 ± 0.71 | 0.400 (0.529) | 0.819 (0.487) | 0.259 (0.855) |
| 6 weeks | 12.77 ± 1.67 | 13.10 ± 1.72 | 10.64 ± 1.47 | 11.49 ± 1.60 | 12.00 ± 0.81 | ||||
| ∆6 week − baseline | −0.54 ± 1.50 | 1.33 ± 1.52 | 0.44 ± 1.26 | 0.56±1.38 | 0.45 ± 0.71 | ||||
| ARFS: Fruit (12 points) | Baseline | 3.44 ± 0.77 | 6.08 ± 0.85 | 4.73 ± 0.79 | 2.77±0.85 | 4.25 ± 0.41 | 0.569 (0.453) | 2.153 (0.099) | 0.863 (0.464) |
| 6 weeks | 3.70 ± 0.90 | 4.92 ± 0.94 | 4.62 ± 0.83 | 2.82±0.90 | 4.01 ± 0.45 | ||||
| ∆6 week − baseline | 0.26 ± 0.68 | −1.15 ± 0.68 | −0.11 ± 0.56 | 0.05±0.62 | −0.24 ± 0.32 | ||||
| ARFS: Meat, chicken & fish (7 points) | Baseline | 2.81 ± 0.35 | 3.15 ± 0.39 | 2.40 ± 0.36 | 2.31±0.39 | 2.67 ± 0.19 | 0.064 (0.801) | 1.090 (0.358) | 0.107 (0.956) |
| 6 weeks | 3.03 ± 0.46 | 3.01 ± 0.47 | 2.45 ± 0.39 | 2.40±0.43 | 2.72 ± 0.22 | ||||
| ∆6 week − baseline | 0.22 ± 0.45 | −0.14 ± 0.46 | 0.05 ± 0.39 | 0.10±0.42 | 0.06 ± 0.22 | ||||
| ARFS: Vegetarian choices (6 or 12 points) | Baseline | 2.13 ± 0.31 | 1.85 ± 0.34 | 1.47 ± 0.32 | 1.54±0.34 | 1.74 ± 0.17 | 1.663 (0.201) | 0.940 (0.425) | 0.160 (0.923) |
| 6 weeks | 1.72 ± 0.42 | 1.74 ± 0.42 | 1.33 ± 0.35 | 1.13±0.38 | 1.48 ± 0.20 | ||||
| ∆6 week − baseline | −0.41 ± 0.43 | −0.11 ± 0.44 | −0.14 ± 0.37 | −0.41 ± 0.40 | −0.27 ± 0.21 | ||||
| ARFS: Grains (13 points) | Baseline | 3.94 ± 0.47 | 3.92 ± 0.52 | 4.07 ± 0.48 | 3.54 ± 0.52 | 3.87 ± 0.25 | 1.189 (0.279) | 0.182 (0.908) | 1.350 (0.264) |
| 6 weeks | 4.41 ± 0.61 | 4.44 ± 0.62 | 3.50 ± 0.52 | 4.32 ± 0.57 | 4.17 ± 0.29 | ||||
| ∆6 week − baseline | 0.47 ± 0.58 | 0.52 ± 0.59 | −0.57 ± 0.49 | 0.78 ± 0.54 | 0.30 ± 0.28 | ||||
| ARFS: Dairy (11 points) | Baseline | 3.38 ± 0.46 | 4.62 ± 0.51 | 3.27 ± 0.47 | 3.54 ± 0.51 | 3.70 ± 0.24 | 0.363 (0.548) | 0.782 (0.507) | 0.959 (0.416) |
| 6 weeks | 3.67 ± 0.57 | 3.79 ± 0.59 | 3.15 ± 0.50 | 3.63 ± 0.55 | 3.56 ± 0.28 | ||||
| ∆6 week − baseline | 0.29 ± 0.50 | −0.83 ± 0.50 | −0.12 ± 0.42 | 0.09 ± 0.46 | −0.14 ± 0.23 | ||||
| ARFS: Condiments (2 points) | Baseline | 1.19 ± 0.18 | 0.62 ± 0.20 | 0.73 ± 0.19 | 0.62 ± 0.20 | 0.79 ± 0.10 | 1.460 (0.230) | 3.374 (0.022) | 1.115 (0.347) |
| 6 weeks | 1.46 ± 0.24 | 0.86 ± 0.24 | 0.53 ± 0.20 | 0.86 ± 0.22 | 0.93 ± 0.11 | ||||
| ∆6 week − baseline | 0.27 ± 0.24 | 0.25 ± 0.25 | 0.20 ± 0.21 | 0.25 ± 0.23 | 0.14 ± 0.12 | ||||
| ARFS: Water (1 point) | Baseline | 0.50 ± 0.12 | 0.54 ± 0.14 | 0.73 ± 0.13 | 0.46 ± 0.14 | 0.56 ± 0.07 | 1.138 (0.254) | 1.867 (0.141) | 1.911 (0.134) |
| 6 weeks | 0.75 ± 0.15 | 0.61 ± 0.16 | 0.85 ± 0.13 | 0.30 ± 0.15 | 0.63 ± 0.07 | ||||
| ∆6 week − baseline | 0.25 ± 0.13 | 0.08 ± 0.13 | 0.11 ± 0.11 | −0.16 ± 0.12 | 0.07 ± 0.06 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brain, K.; Burrows, T.L.; Rollo, M.E.; Hayes, C.; Hodson, F.J.; Collins, C.E. The Effect of a Pilot Dietary Intervention on Pain Outcomes in Patients Attending a Tertiary Pain Service. Nutrients 2019, 11, 181. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010181
Brain K, Burrows TL, Rollo ME, Hayes C, Hodson FJ, Collins CE. The Effect of a Pilot Dietary Intervention on Pain Outcomes in Patients Attending a Tertiary Pain Service. Nutrients. 2019; 11(1):181. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010181
Chicago/Turabian StyleBrain, Katherine, Tracy L. Burrows, Megan E. Rollo, Chris Hayes, Fiona J. Hodson, and Clare E. Collins. 2019. "The Effect of a Pilot Dietary Intervention on Pain Outcomes in Patients Attending a Tertiary Pain Service" Nutrients 11, no. 1: 181. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010181