Evaluation of the Effect of a Growing up Milk Lite vs. Cow’s Milk on Diet Quality and Dietary Intakes in Early Childhood: The Growing up Milk Lite (GUMLi) Randomised Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Intakes
2.3. Assessment of Nutrient Intakes with Nutrient Reference Values
2.4. Assessment of Diet Quality Using the PANDiet Score
2.5. Statistical Analysis
3. Results
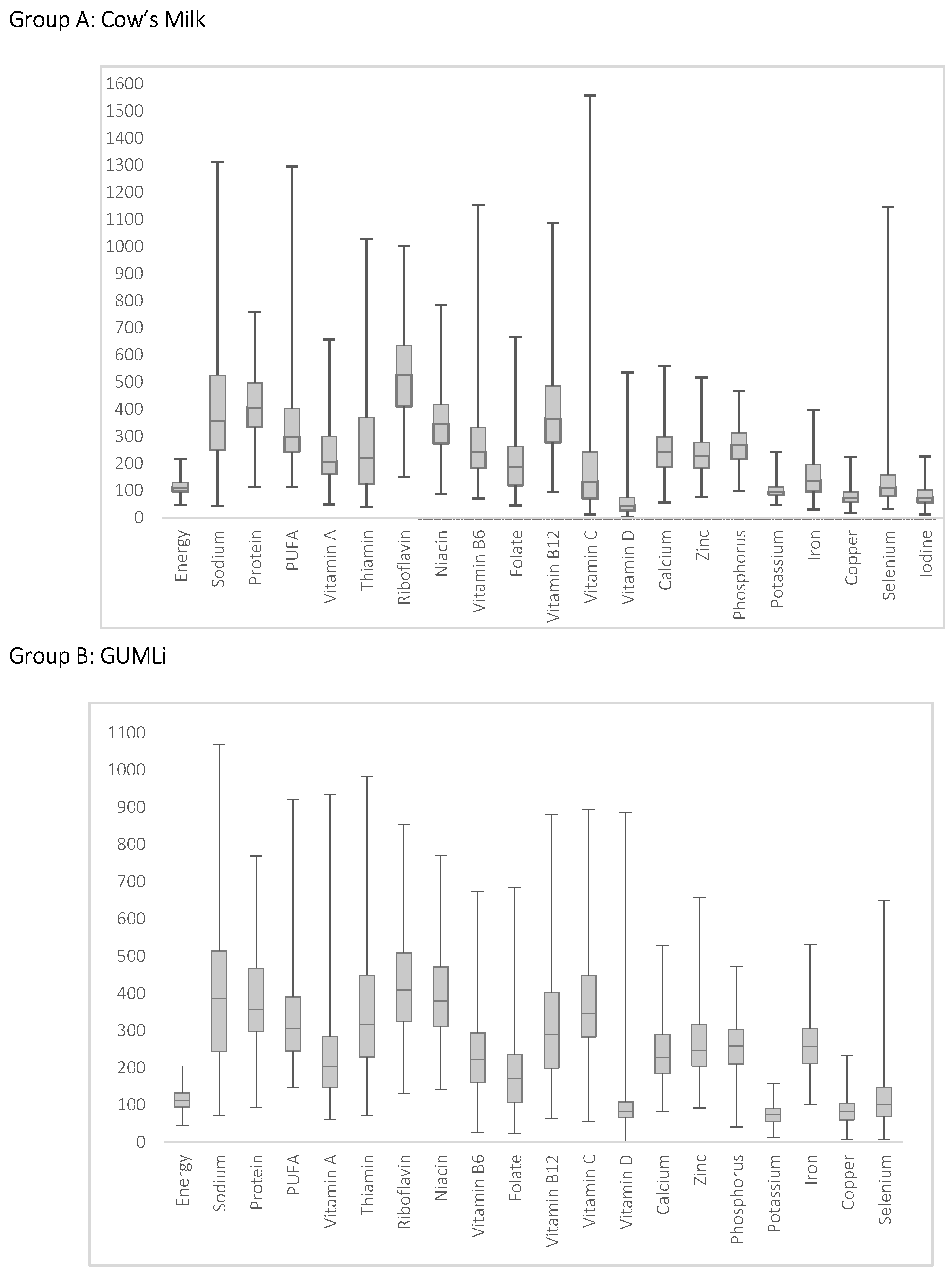
3.1. Evaluation of Nutrient Intakes
3.2. PANDiet Scores According to Intake of GUMLi or CM
4. Discussion
4.1. Diet Quality and PANDiet Scores According to GUMLi or CM Allocation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J. Nutrition for toddlers: The foundation for good health—2. Current problems and ways to overcome them. J. Fam. Health Care 2005, 15, 85–88. [Google Scholar] [PubMed]
- Golley, R.K.; Hendrie, G.A.; McNaughton, S.A. Scores on the Dietary Guideline Index for Children and Adolescents Are Associated with Nutrient Intake and Socio-Economic Position but Not Adiposity—3. J. Nutr. 2011, 141, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.T.; Menon, P. Child feeding practices are associated with child nutritional status in Latin America: Innovative uses of the demographic and health surveys. J. Nutr. 2002, 132, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Indexes of overall diet quality: A review. J. Am. Diet. Assoc. 1996, 96, 785–791. [Google Scholar] [CrossRef]
- Marshall, S.; Burrows, T.; Collins, C.E. Systematic review of diet quality indices and their associations with health-related outcomes in children and adolescents. J. Hum. Nutr. Diet. 2014, 27, 577–598. [Google Scholar] [CrossRef]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef]
- Waijers, P.M.; Feskens, E.J.; Ocké, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Lazarou, C.; Newby, P.K. Use of dietary indexes among children in developed countries. Adv. Nutr. 2011, 2, 295–303. [Google Scholar] [CrossRef]
- Smithers, L.G.; Golley, R.K.; Brazionis, L.; Emmett, P.; Northstone, K.; Lynch, J.W. Dietary patterns of infants and toddlers are associated with nutrient intakes. Nutrients 2012, 4, 935–948. [Google Scholar] [CrossRef] [PubMed]
- Verger, E.O.; Mariotti, F.; Holmes, B.A.; Paineau, D.; Huneau, J. Evaluation of a diet quality index based on the probability of adequate nutrient intake (PANDiet) using national French and US dietary surveys. PLoS ONE 2012, 7, e42155. [Google Scholar] [CrossRef] [PubMed]
- Schoen, S.; Jergens, S.; Barbaresko, J.; Nöthlings, U.; Kersting, M.; Remer, T.; Stelmach-Mardas, M.; Ziegler, A.G.; Hummel, S. Diet quality during infancy and early childhood in children with and without risk of type 1 diabetes: A DEDIPAC study. Nutrients 2017, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Ghisolfi, J.; Fantino, M.; Turck, D.; de Courcy, G.P.; Vidailhet, M. Nutrient intakes of children aged 1–2 years as a function of milk consumption, cows’ milk or growing-up milk. Public Health Nutr. 2013, 16, 524–534. [Google Scholar] [CrossRef]
- Walton, J.; Flynn, A. Nutritional adequacy of diets containing growing up milks or unfortified cow’s milk in Irish children (aged 12–24 months). Food Nutr. Res. 2013, 57, 21836. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.; Magarey, A.; Daniels, L. Food and beverage intake in Australian children aged 12–16 months participating in the NOURISH and SAIDI studies. Aust. N. Z. J. Public Health 2014, 38, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; De Ronne, N.; Van De Sompel, A.; Huysentruyt, K.; Robert, M.; Rigo, J.; Scheers, I.; Brasseur, D.; Goyens, P. A Belgian consensus-statement on growing-up milks for children 12–36 months old. Eur. J. Pediatr. 2014, 173, 1365–1371. [Google Scholar] [CrossRef]
- Eussen, S.R.; Pean, J.; Olivier, L.; Delaere, F.; Lluch, A. Theoretical impact of replacing whole cow’s milk by young-child formula on nutrient intakes of UK young children: Results of a simulation study. Ann. Nutr. Metab. 2015, 67, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.R.; Hill, R.J.; Lovell, A.L.; Matsuyama, M.; Milne, T.; Grant, C.C. A Multi-Centre, Double Blind, Randomised, Placebo Controlled Trial to Evaluate the Effect of Consuming Growing Up Milk. ‘Lite’ on Body Composition in Children Aged 12–23 Months. Available online: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=366785 (accessed on 29 December 2018).
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA Automated Multiple-Pass Method accurately estimates group total energy and nutrient intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [CrossRef]
- Watson, P. Development & Pretesting of Methodologies for the Children’s Nutrition Survey: Validation Report: A Report to the Ministry of Health. Report Three; Institute of Food, Nutrition and Human Health, Massey University: Palmerston North, NZ, USA, 2003. [Google Scholar]
- Coblac, L.; Bowen, J.; Burnett, J.; Syrette, J.; Dempsey, J.; Balle, S.; Wilson, C.; Flight, I.; Good, N.; Saunders, I. Australian National Children’s Nutrition and Physical Activity Survey: Main Findings; Australian Bureau of Statistics: Canberra, Australia, 2008.
- User Guide. Australian National Children’s Nutrition and Physical Activity Survey; Commonwealth Scientific Industrial Research Organisation: Canberra, Australia, 2010. [Google Scholar]
- Briefel, R.R.; Reidy, K.; Karwe, V.; Devaney, B. Feeding infants and toddlers study: Improvements needed in meeting infant feeding recommendations. J. Am. Diet. Assoc. 2004, 104 (Suppl. 1), 31. [Google Scholar] [CrossRef]
- Devaney, B.; Kalb, L.; Briefel, R.; Zavitsky-Novak, T.; Clusen, N.; Ziegler, P. Feeding infants and toddlers study: Overview of the study design. J. Am. Diet. Assoc. 2004, 104 (Suppl. 1), 8. [Google Scholar] [CrossRef] [PubMed]
- Emmett, P.; North, K.; Noble, S. Types of drinks consumed by infants at 4 and 8 months of age: A descriptive study. Public Health Nutr. 2000, 3, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Lennox, A.; Sommerville, J.; Ong, K.; Henderson, H.; Allen, R. Diet and Nutrition Survey of Infants and Young Children; Department of Health and Food Standards Agency: London, UK, 2013.
- Institute for Plant & Food Research Limited, Ministry of Health. New Zealand Food composition Database: New Zealand FOODfiles; Institute for Plant & Food Research Limited, Ministry of Health: Wellington, New Zealand, 2016. [Google Scholar]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; National Health and Medical Research Council: Canberra, Australia, 2006.
- Carriquiry, A.L. Assessing the prevalence of nutrient inadequacy. Public Health Nutr. 1999, 2, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Itakes for Calcium and Vitamin, D; Institute of Medicine: Washington, DC, USA, 2011. [Google Scholar]
- Verger, E.O.; Eussen, S.; Holmes, B.A. Evaluation of a nutrient-based diet quality index in UK young children and investigation into the diet quality of consumers of formula and infant foods. Public Health Nutr. 2016, 19, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Verger, E.O.; Eussen, S.; Holmes, B.A. Diet quality and nutritional adequacy of young children in the UK according to their consumption of young child formula and commercial infant food. Proc. Nutr. Soc. 2015, 74, E250. [Google Scholar] [CrossRef]
- Agostoni, C.V.; Berni Canani, R.; Fairweather Tait, S.; Heinonen, M.; Korhonen, H.; La Vieille, S.; Marchelli, R.; Martin, A.; Naska, A.; Neuhäuser Berthold, M.; et al. Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union: EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2013, 11, 1–103. [Google Scholar]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012: Integrating Nutrition and Physical Activity; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Institute of Medicine (US); Panel on Macronutrients, Institute of Medicine (US). Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; Institute of Medicine: Washington, DC, USA, 2005. [Google Scholar]
- Hilbig, A.; Drossard, C.; Kersting, M.; Alexy, U. Nutrient adequacy and associated factors in a nationwide sample of German toddlers. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom: Report of the Panel on Dietary Reference Values of the committee On Medical Aspects of Food Policy; HM Stationery Office: Richmond, UK, 1991. [Google Scholar]
- Butte, N.F.; Fox, M.K.; Briefel, R.R.; Siega-Riz, A.M.; Dwyer, J.T.; Deming, D.M.; Reidy, K.C. Nutrient intakes of US infants, toddlers, and preschoolers meet or exceed dietary reference intakes. J. Am. Diet. Assoc. 2010, 110, S37. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.; Kehoe, L.; McNulty, B.A.; Nugent, A.P.; Flynn, A. Nutrient intakes and compliance with nutrient recommendations in children aged 1–4 years in Ireland. J. Hum. Nutr. Diet. 2017, 30, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Hojsak, I.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hulst, J.; Indrio, F.; Lapillonne, A.; Mølgaard, C.; et al. Young Child Formula: A Position Paper by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 177–185. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline Demographics | Study Group | p-Value * | |
|---|---|---|---|
| Intervention (N = 41) n (%) | Control (N = 42) n (%) | ||
| Child’s sex | 0.062 | ||
| Boy | 19 (46) | 28 (67) | |
| Girl | 22 (54) | 14 (33) | |
| Other children in the family | 0.222 | ||
| No | 16 (39) | 22 (52) | |
| Yes | 25 (61) | 20 (48) | |
| Day care attendance | 0.893 | ||
| No | 25 (61) | 25 (60) | |
| Yes | 16 (39) | 17 (40) | |
| Breastfed at baseline | 0.415 | ||
| No | 27 (66) | 24 (57) | |
| Yes | 14 (34) | 18 (43) | |
| Mother’s Ethnicity | 0.903 | ||
| Māori | 8 (20) | 6 (14) | |
| Pacific | 0 (0) | 1 (2) | |
| Asian | 3 (7) | 2 (5) | |
| European | 23 (56) | 26 (62) | |
| Other | 7 (17) | 7 (17) | |
| Mother’s Age, years (mean ± SD) | 32 ± 5 | 32 ± 4 | 0.874 |
| Mother’s BMI, kgm2 (mean ± SD) | 26 ± 5 | 27 ± 6 | 0.916 |
| Mother’s Highest Level of Education | 0.589 | ||
| No school qualifications | 0(0) | 0(0) | |
| Primary | 2 (5) | 0 (0) | |
| Secondary | 5 (12) | 7 (17) | |
| Tertiary | 33 (80) | 33 (79) | |
| Other | 1 (2) | 2 (5) | |
| Mother’s Employment Status | 0.082 | ||
| Full-time caregiver | 14 (34) | 15 (36) | |
| Full-time paid employment | 5 (12) | 13 (31) | |
| Part-time paid employment | 14 (34) | 13 (31) | |
| Receiving a benefit | 1 (2) | 0 (0) | |
| Unemployed, no benefit | 3 (7) | 0 (0) | |
| Other | 4 (10) | 1 (2) | |
| Smoking | |||
| Current smoking | 1 (2) | 1 (2) | 1.000 |
| Smoking before pregnancy | 5 (12) | 2 (5) | 0.432 |
| Smoking during pregnancy | 1 (2) | 0 (0) | 0.494 |
| Usual Intake Values | Adjusted Difference (95%CI) | p * | ||
|---|---|---|---|---|
| Nutrients | Intervention (N = 41) Mean (SD) | Control (N = 42) Mean (SD) | ||
| Energy (kcal) | ||||
| Month 07 | 1135.92 (294.19) | 1122.34 (187.51) | 36.61 (−93.18, 166.41) | 0.579 |
| Month 08 | 1114.07 (277.52) | 1246.07 (378.83) | −108.96 (−238.76, 20.84) | 0.100 |
| Month 10 | 1128.31 (383.78) | 1068.61 (291.44) | 82.74 (−47.05, 212.54) | 0.210 |
| Month 11 | 1190.24 (288.14) | 1118.93 (283.21) | 94.34 (−35.45, 224.14) | 0.154 |
| Carbohydrate (g) | ||||
| Month 07 | 142.45 (40.53) | 127.44 (36.36) | 18.26 (−0.25, 36.76) | 0.053 |
| Month 08 | 138.50 (38.12) | 144.65 (56.59) | −2.90 (−21.41, 15.61) | 0.758 |
| Month 10 | 138.25 (45.72) | 123.41 (41.01) | 18.09 (−0.42, 36.59) | 0.055 |
| Month 11 | 145.81 (41.01) | 126.61 (43.06) | 22.45 (3.94, 40.96) | 0.018 * |
| Total fat (g) | ||||
| Month 07 | 38.49 (13.70) | 43.91 (11.34) | −4.69 (−11.04, 1.65) | 0.146 |
| Month 08 | 37.76 (14.79) | 46.21 (16.22) | −7.72 (−14.07, −1.37) | 0.017 * |
| Month 10 | 39.53 (17.61) | 40.34 (13.50) | −0.08 (−6.42, 6.27) | 0.981 |
| Month 11 | 43.99 (15.81) | 43.75 (13.59) | 0.97 (−5.38, 7.32) | 0.764 |
| Saturated fat (g) | ||||
| Month 07 | 18.98 (7.37) | 21.16 (5.98) | −1.96 (−5.27, 1.34) | 0.243 |
| Month 08 | 18.11 (7.41) | 22.16 (8.16) | −3.83 (−7.14, −0.53) | 0.023 * |
| Month 10 | 19.46 (8.88) | 19.73 (7.77) | −0.05 (−3.35, 3.26) | 0.977 |
| Month 11 | 20.93 (8.11) | 21.00 (6.84) | 0.15 (−3.16, 3.45) | 0.930 |
| NMES (g) | ||||
| Month 07 | 45.46 (18.22) | 42.02 (17.88) | 4.33 (−5.27, 13.93) | 0.375 |
| Month 08 | 45.90 (19.00) | 49.01 (30.16) | −2.22 (−11.83, 7.38) | 0.649 |
| Month 10 | 40.13 (23.17) | 39.00 (19.24) | 2.03 (−7.58, 11.63) | 0.678 |
| Month 11 | 48.53 (25.02) | 39.29 (21.47) | 10.14 (0.54, 19.74) | 0.039 * |
| Protein (g) | ||||
| Month 07 | 46.07 (17.15) | 50.13 (10.13) | −3.26 (−9.65, 3.13) | 0.316 |
| Month 08 | 46.09 (14.01) | 56.47 (17.08) | −9.58 (−15.97, −3.19) | 0.004 * |
| Month 10 | 46.45 (18.34) | 44.33 (12.51) | 2.92 (−3.47, 9.31) | 0.369 |
| Month 11 | 44.59 (14.36) | 47.48 (13.13) | −2.09 (−8.48, 4.30) | 0.520 |
| Thiamin (mg) | ||||
| Month 07 | 1.50 (0.63) | 1.19 (0.84) | 0.34 (0.03, 0.64) | 0.030 * |
| Month 08 | 1.54 (0.56) | 1.29 (0.72) | 0.28 (−0.02, 0.59) | 0.069 |
| Month 10 | 1.35 (0.70) | 1.03 (0.82) | 0.36 (0.05, 0.66) | 0.022 * |
| Month 11 | 1.36 (0.68) | 0.99 (0.64) | 0.40 (0.10, 0.71) | 0.010 * |
| Riboflavin (mg) | ||||
| Month 07 | 1.82 (0.64) | 2.12 (0.64) | −0.29 (−0.56, −0.02) | 0.037 * |
| Month 08 | 1.71 (0.54) | 2.30 (0.77) | −0.58 (−0.85, −0.30) | <0.0001 * |
| Month 10 | 1.66 (0.50) | 2.07 (0.67) | −0.39 (−0.66, −0.11) | 0.006 * |
| Month 11 | 1.63 (0.61) | 2.11 (0.57) | −0.47 (−0.74, −0.20) | 0.001 * |
| Niacin (mg) | ||||
| Month 07 | 19.97 (7.25) | 17.79 (4.64) | 2.49 (−0.12, 5.09) | 0.061 |
| Month 08 | 20.63 (5.18) | 20.09 (7.30) | 0.85 (−1.75, 3.45) | 0.521 |
| Month 10 | 19.34 (6.64) | 15.80 (5.87) | 3.84 (1.24, 6.45) | 0.004 * |
| Month 11 | 19.09 (5.31) | 17.28 (5.39) | 2.11 (−0.49, 4.71) | 0.112 |
| Vitamin B12 (µg) | ||||
| Month 07 | 2.36 (1.12) | 2.78 (1.09) | −0.41 (−0.91, 0.09) | 0.108 |
| Month 08 | 2.25 (1.30) | 3.17 (1.55) | −0.91 (−1.41, −0.41) | 0.0004 * |
| Month 10 | 2.14 (0.94) | 2.57 (0.93) | −0.42 (−0.92, 0.07) | 0.095 |
| Month 11 | 2.03 (0.91) | 2.58 (1.15) | −0.55 (−1.05, −0.05) | 0.031 * |
| Vitamin C (mg) | ||||
| Month 07 | 104.00 (44.39) | 45.38 (37.36) | 57.38 (35.76, 79.01) | <0.0001 * |
| Month 08 | 99.95 (39.44) | 50.22 (54.71) | 48.48 (26.86, 70.11) | <0.0001 * |
| Month 10 | 92.84 (34.62) | 50.54 (65.97) | 41.05 (19.43, 62.68) | 0.0002 * |
| Month 11 | 92.51 (48.54) | 58.80 (61.49) | 32.47 (10.85, 54.10) | 0.003 * |
| Vitamin D (µg) | ||||
| Month 07 | 6.02 (6.57) | 3.23 (3.18) | 2.80 (1.07, 4.53) | 0.002 * |
| Month 08 | 4.73 (2.70) | 3.59 (4.00) | 1.16 (−0.57, 2.89) | 0.188 |
| Month 10 | 5.17 (2.76) | 2.92 (2.49) | 2.27 (0.54, 4.00) | 0.011 * |
| Month 11 | 4.86 (3.44) | 3.73 (4.75) | 1.15 (−0.58, 2.88) | 0.194 |
| Calcium (mg) | ||||
| Month 07 | 901.26 (268.15) | 898.06 (287.37) | 8.15 (−113.76, 130.06) | 0.895 |
| Month 08 | 808.31 (257.94) | 943.49 (314.09) | −130.24 (−252.15, −8.33) | 0.036 * |
| Month 10 | 899.34 (284.54) | 836.03 (251.58) | 68.25 (−53.65, 190.16) | 0.271 |
| Month 11 | 830.41 (284.29) | 891.05 (280.79) | −55.70 (−177.60, 66.21) | 0.369 |
| Zinc (mg) | ||||
| Month 07 | 6.75 (2.76) | 6.11 (1.51) | 0.71 (−0.22, 1.64) | 0.133 |
| Month 08 | 6.64 (2.24) | 6.85 (2.65) | −0.13 (−1.07, 0.80) | 0.776 |
| Month 10 | 6.44 (2.45) | 5.37 (1.74) | 1.14 (0.21, 2.07) | 0.017 * |
| Month 11 | 6.42 (1.77) | 5.45 (1.69) | 1.04 (0.11, 1.97) | 0.029 * |
| Phosphorus (mg) | ||||
| Month 07 | 1023.06 (284.32) | 1004.05 (202.02) | 33.99 (−83.88, 151.87) | 0.571 |
| Month 08 | 966.96 (257.85) | 1106.43 (293.65) | −124.49 (−242.36, −6.62) | 0.039 * |
| Month 10 | 984.67 (335.64) | 930.98 (252.54) | 68.68 (−49.20, 186.55) | 0.252 |
| Month 11 | 989.53 (278.71) | 988.18 (262.19) | 16.33 (−101.54, 134.20) | 0.785 |
| Potassium (mg) | ||||
| Month 07 | 1666.69 (703.04) | 1962.08 (433.28) | −283.10 (−528.37, −37.83) | 0.024 * |
| Month 08 | 1537.51 (481.42) | 2232.75 (761.17) | −682.95 (−928.21, −437.68) | <0.0001 * |
| Month 10 | 1406.79 (493.64) | 1861.05 (503.26) | −441.97 (−687.24, −196.70) | 0.001 * |
| Month 11 | 1512.12 (526.22) | 1987.09 (511.40) | −462.67 (−707.94, −217.40) | 0.000 * |
| Iron (mg) | ||||
| Month 07 | 10.62 (3.36) | 6.23 (2.82) | 4.58 (3.31, 5.85) | <0.0001 * |
| Month 08 | 10.80 (2.96) | 6.90 (2.75) | 4.10 (2.83, 5.37) | <0.0001 * |
| Month 10 | 9.83 (2.89) | 5.64 (3.07) | 4.38 (3.11, 5.65) | <0.0001 * |
| Month 11 | 10.26 (3.24) | 5.24 (2.35) | 5.21 (3.93, 6.48) | <0.0001 * |
| Copper (mg) | ||||
| Month 07 | 0.62 (0.32) | 0.6 (0.24) | 0.04 (−0.08, 0.15) | 0.524 |
| Month 08 | 0.6 (0.26) | 0.68 (0.35) | −0.06 (−0.18, 0.05) | 0.255 |
| Month 10 | 0.63 (0.28) | 0.5 (0.21) | 0.15 (0.04, 0.26) | 0.010 * |
| Month 11 | 0.6 (0.18) | 0.53 (0.18) | 0.09 (−0.02, 0.2) | 0.115 |
| Iodine (µg) | ||||
| Month 07 | 64.08 (23.15) | 52.65 (24.78) | 11.80 (0.49, 23.11) | 0.041 * |
| Month 08 | 63.58 (29.84) | 55.72 (21.88) | 8.22 (−3.09, 19.54) | 0.154 |
| Month 10 | 60.53 (27.92) | 53.13 (26.95) | 7.77 (−3.55, 19.08) | 0.178 |
| Month 11 | 65.92 (30.56) | 53.53 (21.06) | 12.76 (1.45, 24.07) | 0.027 |
| Score | Intervention (N = 41) | Control (N = 42) | Adjusted Difference (95% CI) | p-Value * |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| PANDiet 3 | 52.9 (3.07) | 50.12 (3.97) | 3.11 (1.56, 4.67) | 0.0001 * |
| Moderation sub-score | 29.82 (6.47) | 27.77 (6.58) | 2.06 (−0.87, 4.99) | 0.1660 |
| Protein | 0.41 (0.50) | 0.33 (0.48) | 0.08 (−0.14, 0.30) | 0.4747 |
| Total Fat | 0.10 (0.30) | 0.48 (0.51) | −0.40 (−0.59, −0.22) | <0001 * |
| Total Carbohydrate | 0.85 (0.36) | 0.55 (0.50) | 0.33 (0.14, 0.53) | 0.0011 * |
| SFA | 0.10 (0.16) | 0.06 (0.12) | 0.05 (−0.01, 0.11) | 0.1231 |
| NMES | 0.16 (0.22) | 0.23 (0.28) | −0.08 (−0.19, 0.03) | 0.1699 |
| Sodium | 0.03 (0.14) | 0.02 (0.04) | 0.01 (−0.03, 0.06) | 0.5832 |
| Adequacy sub-score | 75.98 (4.98) | 72.46 (5.88) | 4.17 (1.82, 6.51) | 0.0007 * |
| Protein | 0.99 (0.03) | 1.00 (0.001) | −0.01 (−0.01, 0.002) | 0.1697 |
| Total Carbohydrate | 0.98 (0.16) | 1.00 (0.00) | −0.02 (−0.07, 0.03) | 0.4293 |
| Total Fat | 1.00 (0.00) | 0.86 (0.35) | 0.14 (0.03, 0.26) | 0.0140 * |
| PUFA | 0.15 (0.19) | 0.18 (0.23) | −0.01 (−0.10, 0.08) | 0.7975 |
| Vitamin A | 0.96 (0.08) | 0.98 (0.02) | −0.02 (−0.05, 0.001) | 0.0560 |
| Thiamin | 1.00 (0.005) | 0.94 (0.09) | 0.06 (0.03, 0.09) | 0.0001 * |
| Riboflavin | 1.00 (0.001) | 1.00 (0.0003) | −0.0003 (−0.001, 0.00) | 0.0853 |
| Niacin | 1.00 (0.00001) | 1.00 (0.0005) | 0.0001 (0.00, 0.0002) | 0.1819 |
| Vitamin B6 | 0.00 (0.00) | 0.00 (0.00) | 0.00 (0.00,0.00) | 0.9775 |
| Folate | 0.89 (0.18) | 0.91 (0.21) | −0.01 (−0.10, 0.07) | 0.7717 |
| Vitamin B12 | 0.99 (0.02) | 1.00 (0.01) | −0.01 (−0.02, −0.003) | 0.0081 * |
| Vitamin C | 1.00 (0.01) | 0.71 (0.32) | 0.30 (0.20, 0.40) | <0001 * |
| Vitamin D | 0.43 (0.34) | 0.19 (0.31) | 0.25 (0.10, 0.39) | 0.0011 * |
| Calcium | 0.99 (0.02) | 1.00 (0.02) | −0.002 (−0.01, 0.01) | 0.7227 |
| Magnesium | 0.99 (0.02) | 1.00 (0.004) | −0.005 (−0.01, 0.002) | 0.1826 |
| Zinc | 1.00 (0.003) | 0.99 (0.02) | 0.01 (−0.0002, 0.01) | 0.0585 |
| Phosphorus | 1.00 (0.01) | 1.00 (0.002) | −0.001 (−0.003, 0.0005) | 0.1323 |
| Potassium | 1.00 (0.002) | 1.00 (1E−6) | −0.0003 (−0.001, 0.0002) | 0.1998 |
| Iron | 1.00 (0.01) | 0.78 (0.32) | 0.25 (0.16, 0.35) | <0001 * |
| Copper | 0.34 (0.30) | 0.27 (0.27) | 0.10 (−0.03, 0.23) | 0.1203 |
| Selenium | 0.57 (0.37) | 0.70 (0.28) | −0.09 (−0.23, 0.06) | 0.2314 |
| Iodine | 0.46 (0.28) | 0.29 (0.24) | 0.18 (0.06, 0.30) | 0.0035 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovell, A.L.; Milne, T.; Jiang, Y.; Chen, R.X.; Grant, C.C.; Wall, C.R. Evaluation of the Effect of a Growing up Milk Lite vs. Cow’s Milk on Diet Quality and Dietary Intakes in Early Childhood: The Growing up Milk Lite (GUMLi) Randomised Controlled Trial. Nutrients 2019, 11, 203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010203
Lovell AL, Milne T, Jiang Y, Chen RX, Grant CC, Wall CR. Evaluation of the Effect of a Growing up Milk Lite vs. Cow’s Milk on Diet Quality and Dietary Intakes in Early Childhood: The Growing up Milk Lite (GUMLi) Randomised Controlled Trial. Nutrients. 2019; 11(1):203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010203
Chicago/Turabian StyleLovell, Amy L., Tania Milne, Yannan Jiang, Rachel X. Chen, Cameron C. Grant, and Clare R. Wall. 2019. "Evaluation of the Effect of a Growing up Milk Lite vs. Cow’s Milk on Diet Quality and Dietary Intakes in Early Childhood: The Growing up Milk Lite (GUMLi) Randomised Controlled Trial" Nutrients 11, no. 1: 203. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11010203