1. Introduction
Research suggests that the sedentary lifestyle of today’s Western societies is associated with the development of chronic systemic low-grade inflammation, which is at the root of many typically Western diseases associated with the metabolic syndrome [
1]. Due to the anti-inflammatory capacities of aerobic physical activity, integration of regular activity sessions into everyday life seems to be beneficial regarding improvement of general health and, furthermore, regarding protection of the brain from metabolic stress [
1,
2]. In addition, especially regular aerobic activity has been consistently reported to prevent mental illness (e.g., depression) and alleviate mood problems, as well as to improve cognitive and brain function, but even acute, moderate activity sessions seem to exert similar effects [
2,
3,
4,
5]. In this context, different research studies describe modulators of effect size being the temporal sequencing of cognitive assessment in relation to exercise (e.g., following exercise session or during exercise session), the modality of aerobic training (e.g., cycling or running), and the cognitive parameters measured (e.g., memory or processing speed), as well as age and medical condition [
3,
4,
6].
While supplementation studies suggest that single nutrients (e.g., docosahexaenoic acid) can increase cognitive performance, research on the effects of whole meals and, especially, different meal compositions on cognitive function and mood is limited [
7]. Compared to a meal intake which is in accordance with the Western dietary pattern, a Mediterranean diet provides higher levels of nutrients including essential fatty acids, vitamins, minerals, and antioxidants, which seem to support brain function. Additionally, the Mediterranean dietary pattern contains fewer refined carbohydrates and saturated fatty acids, which have been associated with cognitive deficits [
7,
8]. Therefore, it is likely that a regular choice of food items characteristic for the Mediterranean dietary pattern is beneficial with regard to the prevention of age-related cognitive deficits [
9,
10]. In this context, numerous epidemiological studies suggest that an adherence to plant-based dietary patterns, especially the Mediterranean dietary pattern, is associated with improved cognitive performance, slower age-related cognitive decline and lower risk of cognitive impairment and neurodegenerative disease in older adults [
11,
12,
13,
14].
Current randomized interventions trials evaluating the acute interactive effects of meal composition and physical activity on cognitive performance and emotions are limited [
15,
16] and to the best of our knowledge, no previous human study has investigated the acute effects of postprandial exercise suitable for daily implementation neither on postprandial attention as a complex cognitive function, nor on mood/emotions following the consumption of meals reflecting different dietary patterns, especially in subjects with a risk phenotype for the development of cardiovascular and neurodegenerative diseases (e.g., elevated age; characteristics of metabolic syndrome). Since current research suggests that breakfast as the first meal of the day is most important from a dietary perspective [
17] and is vital for optimal cognitive function and intellectual performance by providing readily available energy to the brain [
18], the test meals in the present study were provided as breakfast challenges after an overnight fast (≥12 h). The study tested two main hypotheses: (i) a Mediterranean-type diet meal (MD) generates higher postprandial satiety, postprandial attention and a better subjective mood than an iso-energetic Western diet high-fat meal (WD); and (ii) Moderate walking in the postprandial period as compared to remaining sedentary, results in increased postprandial attention and a better subjective mood. In addition to these main hypotheses, this study examined the impact of plasma cortisol concentration on postprandial attention, since elevated systemic cortisol concentrations have been associated with detrimental effects on cognition and a long-term contribution to Alzheimer’s disease pathology [
19,
20]. In this context, the present study evaluated if the activity session or the intake of high-energy meals were high enough stressors to trigger cortisol release and if effects of different plasma cortisol concentrations on postprandial attention are relevant even in an acute study design.
The data presented in this manuscript are ancillary examinations (secondary outcome measures) of the intervention study which has initially been designed to investigate the effects of meal composition and postmeal walking on different metabolic, inflammatory, oxidative, and endothelial events in the postprandial period, with postprandial triglycerides as primary outcome measure [
21].
4. Discussion
The purpose of this study was to investigate the acute impact of dietary composition and moderate postmeal walking on postprandial attention (representing one aspect of cognitive function), mood, and the sensations of hunger and satiety in older subjects with a risk phenotype for the development of cardiovascular and neurodegenerative diseases.
Prior research suggests that the consumption of breakfast is vital for optimal cognitive performance, since it provides readily available energy as first meal of the day after an overnight fast [
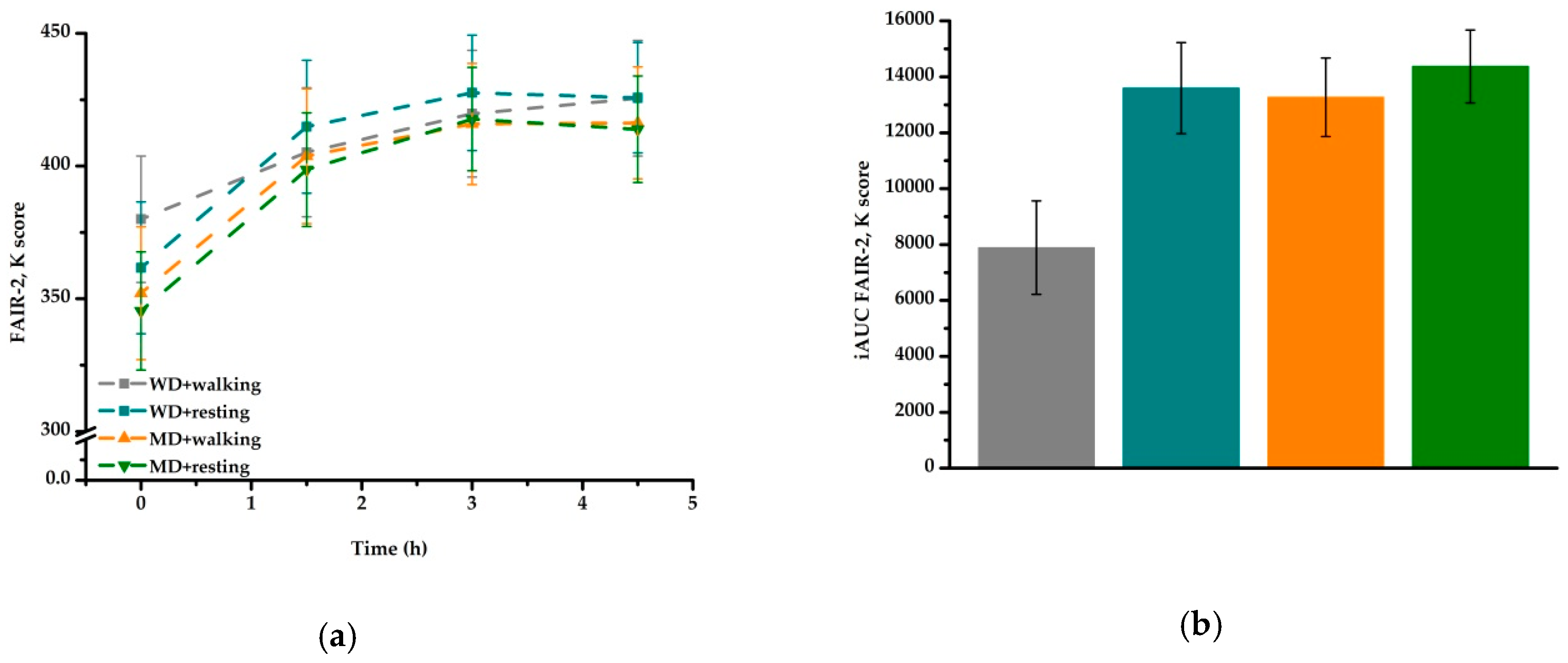
15,
18]. In the present study, the consumption of both test meals (breakfast challenges) yielded a reliable and substantial (10–20%) increase of postprandial attention over time. iAUC data revealed that the increase in postprandial attention was significantly higher after MD than after WD, which is in accordance with our hypothesis that a MD results in higher postprandial attention than a WD. Considering the fact that glucose is the main fuel for brain function and therefore plays an important role in general cognitive performance [
29,
30], the observed meal effect on postprandial attention in the present study might be due to the higher amount of carbohydrate in MD (133.3 g vs. 93.7 g). It remains unclear whether the different nutrient composition of the breakfast challenges (
Table 1) contributed to the observed results. Since an adherence to the Mediterranean dietary pattern is in the long run associated with improved cognitive performance and mental health, future intervention studies in this field of research might consider taking into account the habitual diet/nutritional status of their participants as a further possible influencing factor of acute nutritional effects on cognitive parameters such as postprandial attention.
Furthermore, an activity effect was observed after WD, with lower postprandial attention after walking than after resting. From the perspective of energy availability to the brain, these findings are rather unexpected, since we observed higher plasma glucose concentrations after walking than after resting for both meal types [
21].
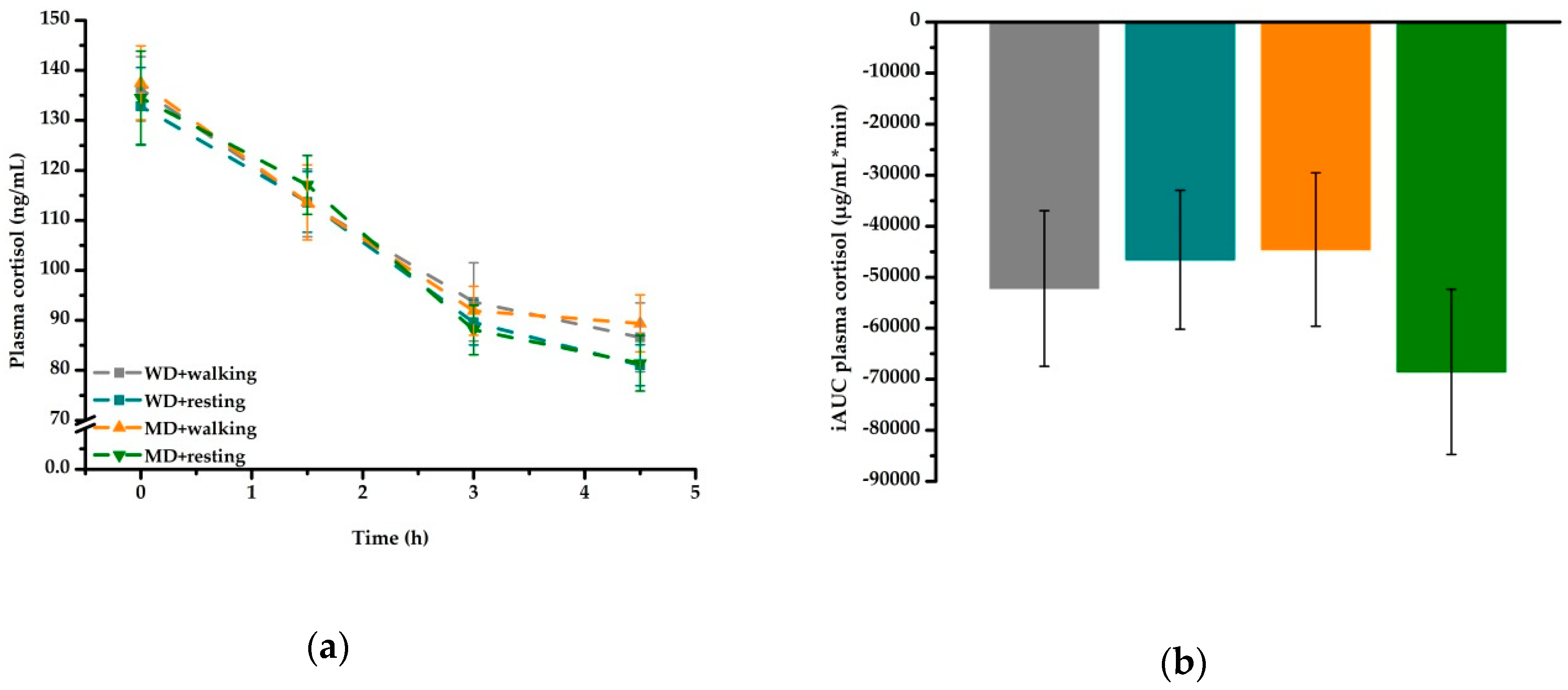
An increase in postprandial cortisol concentrations could further explain the decreased attention values observed after the WD + walking treatment, since elevated plasma cortisol is associated with altered cognitive function [
31]. However, our data showed no activity effect on postprandial plasma cortisol over time for none of the four treatments. Since the walking session in the present study was of moderate intensity and short duration only, the stressor might not have been high enough to trigger an increase in plasma cortisol concentrations [
32]. However, it is possible that an activity effect on postprandial cortisol would have been detectable if blood samples had been taken during and/or directly at the end of the walking session [
32]. In accordance with previous postprandial trials [
33,
34], in the present study, postprandial cortisol significantly decreased from morning to afternoon, similar to its diurnal variation, and the stimulus of meal intake was not strong enough to alter this distinct pattern (
Figure 4a,
Table 6). Since postprandial attention as well as cortisol showed a strong time effect, it is difficult to separate between the extent to which time influenced postprandial attention and the extent to which postprandial cortisol had an influence on this parameter.
The fact that the increase of overall postprandial attention was due to an increase in test speed and not in test accuracy suggests, that the repetition of the same test procedure on each time point on each of the four study days led to a learning effect. This learning effect, however, cannot be quantified but should be taken in to account when evaluating the practical relevance of the statistical results.
In contrast to a previous postprandial exercise trial conducted in healthy, habitually active, middle-aged women, which showed an association between the consumption of breakfast and lower fatigue and higher overall mood and alertness post-exercise [
16], in the present study, no relevant effect of meal intake or postprandial activity behavior on the measured mood dimensions (good vs. bad mood, alertness vs. fatigue, and ease vs. unease) could be observed (
Table 4). Despite statistical significance, for all three dimensions, changes in mean values between all time points were minor. The obtained results showed that the subjects were alert, at ease and in rather good mood during the course of each study day (
Table 4). Since meal or activity effects on subjective parameters like mood are complex to measure, it is possible that the MDMQ was not sensitive enough to determine clinically relevant treatment effects on mood over time [
35].
In comparison to the present study, future intervention studies in this field of research might consider the habitual activity level/physical activity status of their participants as a modulator of effect size. It can be assumed that the intensity of an acute physical activity session is perceived differently depending on the activity status of a person (low or high metabolic stressor), possibly resulting in different effects on postprandial attention and / or postprandial emotional state.
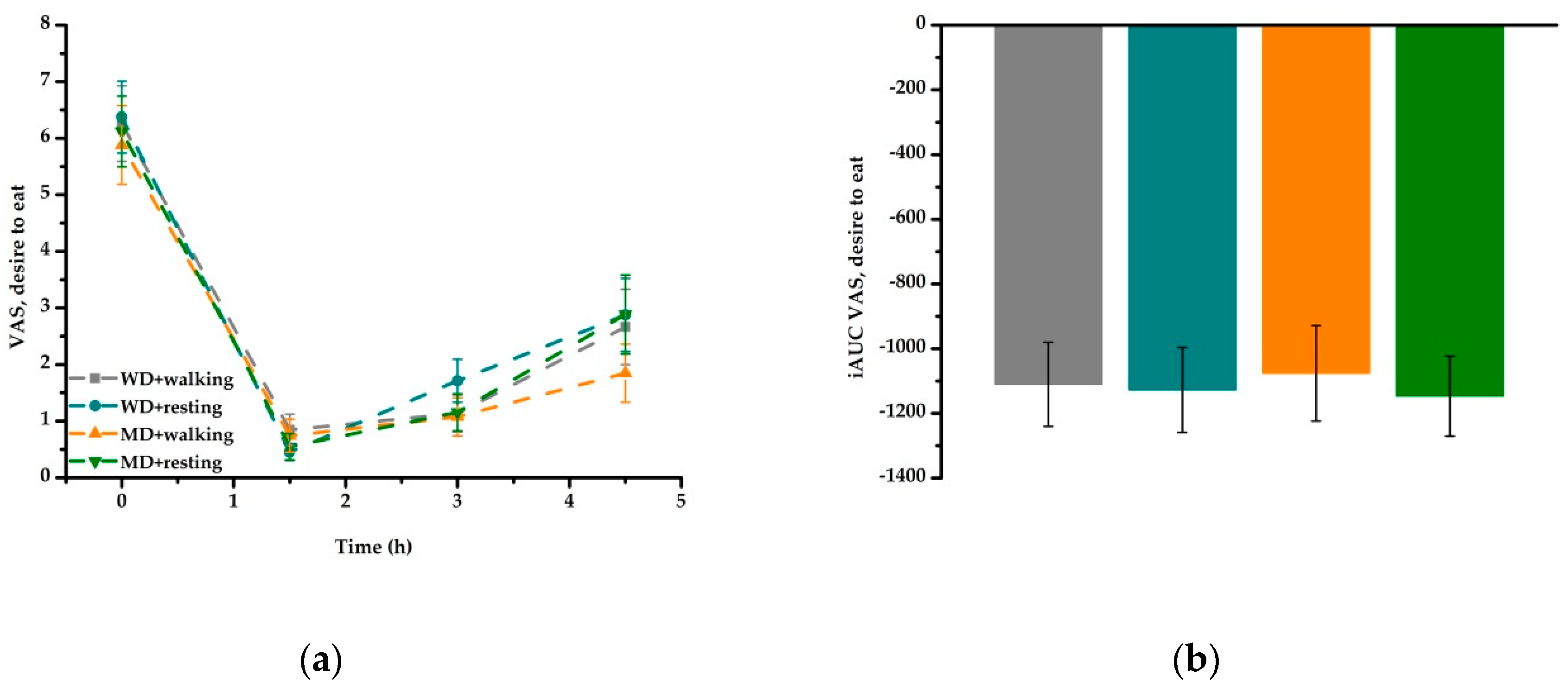
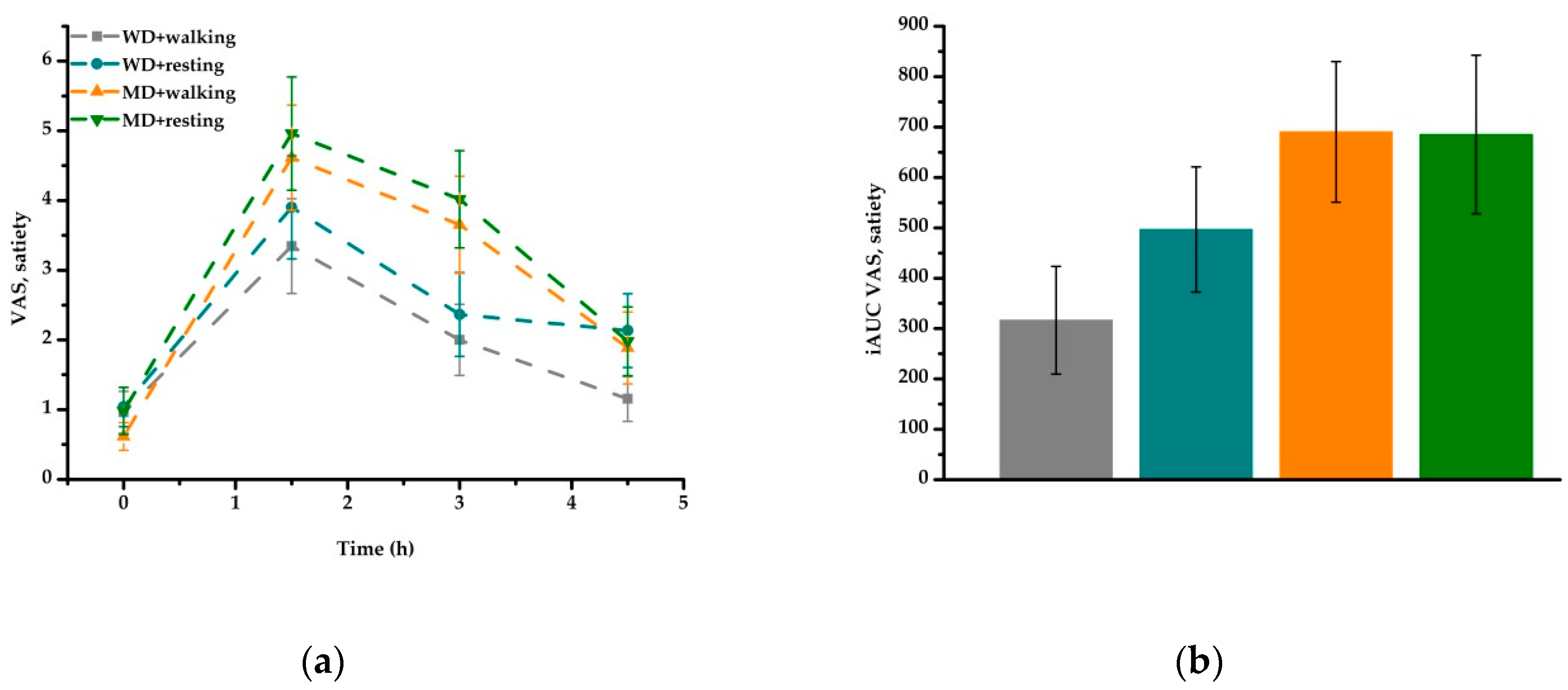
Research suggests that the consumption of food in the early morning leads to control and moderation of total energy intake throughout the whole day, since the complex carbohydrates usually consumed during breakfast affect activity as well as release of hormones (e.g., gastric inhibitory peptide, glucagon-like peptide-1, cholecystokinin), which differently affect postprandial plasma glucose and, consequently, satiety [
18]. In the present study, the higher satiety values over time that were observed after MD treatments compared to WD treatments are mainly due to the higher volume of the MD (781 g/MD meal vs. 390 g/WD meal), as well as the higher dietary fiber content (14.5 g/MD meal vs. 4.2 g/WD meal). It is possible that this marked satiating power led to control and moderation of total energy intake throughout the remaining day.
The major strengths of the present study are the controlled, crossover design, the absence of study dropouts, and the high rate of treatment compliance. In contrast to previous studies in this flied of research, this trial followed a holistic approach and focused on regular meals reflecting different dietary patterns and not on the administration of nutrient solutions (e.g., fat tolerance tests). The 30 min session of moderate postmeal walking was designed to be easily incorporable into daily routines, even by inactive or physically more restricted individuals. One limitation of the present work is that it is an explorative analysis of secondary outcome measures. The study was originally designed to investigate the effects of meal composition and postmeal walking on different metabolic, inflammatory, oxidative, and endothelial outcome measures in the postprandial period and a priori sample size calculation was based on serum triglycerides as primary outcome measure of the postprandial intervention study [
21]. Another potential limitation of the study is the time points selected for the measurement of outcome measures, which may not have been representative of the overall postprandial period. However, for scheduling reasons, further time points and shorter intervals were precluded from the study design. Furthermore, the repeated use of the FAIR-2 type A to examine attention behavior may have led to a learning effect which might have influenced time- and treatment effects. However, alternate use of both test types (A and B) could not be performed as there was a risk of possible bias due to changes in target items and test procedures. Future intervention trials focusing on the evaluation of selective attention as a primary outcome measure might consider including a variety of test procedures focusing on different aspects of cognitive performance (including vigilance) and a chronometric approach might be reasonable in order to evaluate cognitive function more specifically. This might be especially relevant in chronic rather than acute intervention trials.

 and
and 




{kind=link}
{kind=link}
{kind=link}
{kind=link}