Nutritional Status in Spanish Children and Adolescents with Celiac Disease on a Gluten Free Diet Compared to Non-Celiac Disease Controls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Food Habits and Nutrient Intakes
2.3. Anthropometric Measures
2.4. Blood Parameters
2.5. Bone Mineral Density
2.6. Physical Activity
2.7. Statistical Analysis
3. Results
3.1. Food Habits and Nutrient Intake
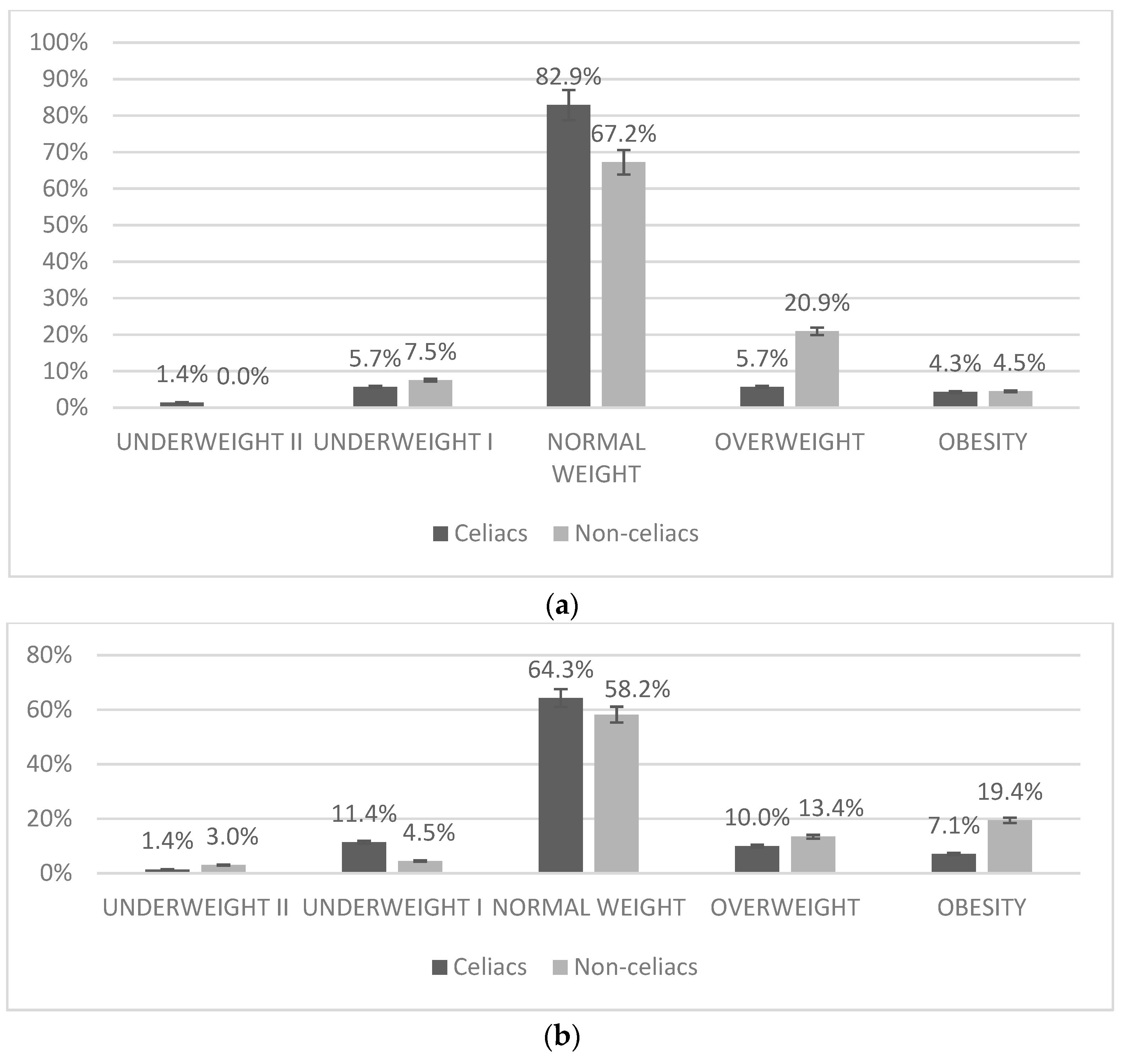
3.2. Anthropometric Measures
3.3. Blood Parameters
3.4. Physical Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Polanco, I. Libro Blanco de la Enfermedad Celiaca; Comunidad de Madrid: Madrid, Spain, 2008. [Google Scholar]
- Dubé, C.; Rostom, A.; Sy, R.; Cranney, A.; Saloojee, N.; Garritty, C.; Sampson, M.; Zhang, L.; Yazdi, F.; Mamaladze, V.; et al. The prevalence of celiac disease in average-risk and at-risk Western European populations: A systematic review. Gastroenterology 2005, 128, S57–S67. [Google Scholar] [CrossRef] [PubMed]
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Gatti, S.; Fasano, A. The New Epidemiology of Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, S7–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra, E. Epidemiología de la enfermedad celíaca. IntraMed 2003, 43, 317–320. [Google Scholar]
- Garrido, M. Estudio Epidemiológico para Determinar la Prevalencia de la Enfermedad Celíaca en la Población Escolar de la Comunidad de Madrid; Consejería de Sanidad: Madrid, Spain, 2009. [Google Scholar]
- Cilleruelo, M.L.; Roman-Riechmann, E.; Sanchez-Valverde, F.; Donat, E.; Manuel-Ramos, J.; Martín-Orte, E.; López, M.J.; García-Novo, D.; García, S.; Pavón, P.; et al. Spanish national registry of celiac disease: Incidence and clinical presentation. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Calvo, M.C. La Dieta Sin Gluten; Ergon: Madrid, Spain, 2013. [Google Scholar]
- Rashid, M.; Cranney, A.; Zarkadas, M.; Graham, I.D.; Switzer, C.; Case, S.; Molloy, M.; Warren, R.E.; Burrows, V.; Butzner, J.D. Celiac Disease: Evaluation of the Diagnosis and Dietary Compliance in Canadian Children. Pediatrics 2005, 116, e754–e759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuccotti, G.; Fabiano, V.; Dilillo, D.; Picca, M.; Cravidi, C.; Brambilla, P. Intakes of nutrients in Italian children with celiac disease and the role of commercially available gluten-free products. J. Hum. Nutr. Diet. 2013, 26, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Penagini, F.; DiLillo, D.; Meneghin, F.; Mameli, C.; Fabiano, V.; Zuccotti, G.V. Gluten-Free Diet in Children: An Approach to a Nutritionally Adequate and Balanced Diet. Nutrients 2013, 5, 4553–4565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wierdsma, N.J.; Berkenpas, M.; Mulder, C.J.J.; Van Bodegraven, A.A. Vitamin and Mineral Deficiencies Are Highly Prevalent in Newly Diagnosed Celiac Disease Patients. Nutrients 2013, 5, 3975–3992. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T.; Dennis, M.; Higgins, L.A.; Lee, A.R.; Sharrett, M.K. Gluten-free diet survey: Are Americans with coeliac disease consuming recommended amounts of fibre, iron, calcium and grain foods? J. Hum. Nutr. Diet. 2005, 18, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Cicala, M.; Tiberi, E.; Spadaccio, C.; Marcella, L.; Gatto, A.; Calzolari, P.; Castellucci, G. High fat consumption in children with celiac disease. Acta Gastro Enterol. Belg. 2009, 72, 296–300. [Google Scholar]
- Mariani, P.; Viti, M.G.; Montouri, M.; La Vecchia, A.; Cipolletta, E.; Calvani, L.; Bonamico, M. The Gluten-Free Diet: A Nutritional Risk Factor for Adolescents with Celiac Disease? J. Pediatr. Gastroenterol. Nutr. 1998, 27, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Hopman, E.G.; Le Cessie, S.; Von Blomberg, B.M.E.; Mearin, M.L. Nutritional Management of the Gluten-free Diet in Young People with Celiac Disease in The Netherlands. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öhlund, K.; Olsson, C.; Hernell, O.; Öhlund, I. Dietary shortcomings in children on a gluten-free diet. J. Hum. Nutr. Diet. 2010, 23, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Kautto, E.; Ivarsson, A.; Norstrom, F.; Hogberg, L.; Carlsson, A.; Hornell, A. Nutrient intake in adolescent girls and boys diagnosed with coeliac disease at an early age is mostly comparable to their non-coeliac contemporaries. J. Hum. Nutr. Diet. 2014, 27, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Salazar Quero, J.C.; Espín Jaime, B.; Rodríguez Martínez, A.; Argüelles Martín, F.; García Jiménez, R.; Rubio Murillo, M.; Martín, A.P. Nutritional assessment of gluten-free diet. Is gluten-free diet deficient in some nutrient? An. Pediatr. 2015, 83, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Balamtekin, N.; Aksoy, Ç.; Baysoy, G.; Uslu, N.; Demir, H.; Köksal, G.; Saltik-Temizel, I.N.; Özen, H.; Gürakan, F.; Yüce, A. Is compliance with gluten-free diet sufficient? Diet composition of celiac patients. Turk. J. Pediatr 2015, 57, 374. [Google Scholar] [PubMed]
- Castillejo, G.; Recasens, M.; Masip, G.; Sánchez, E.; Sánchez, N.B.; Vaqué, C.; Alcázar, M.; Martínez-Cerezo, F.; Gutiérrez-Pensado, V.; Vila-Martí, A.; et al. Patients with Celiac Disease Reported Higher Consumption of Added Sugar and Total Fat Than Healthy Individuals. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 63–69. [Google Scholar]
- Diamanti, A.; Capriati, T.; Basso, M.S.; Panetta, F.; Laurora, V.M.D.C.; Bellucci, F.; Cristofori, F.; Francavilla, R. Celiac Disease and Overweight in Children: An Update. Nutrients 2014, 6, 207–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, C.; Hino, B.; Lerner, A.; Eshach-Adiv, O.; Berkowitz, D.; Shaoul, R.; Pacht, A.; Rozenthal, E.; Tamir, A.; Shamaly, H.; et al. Bone quantitative ultrasound and bone mineral density in children with celiac disease. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 504–510. [Google Scholar] [CrossRef]
- Valitutti, F.; Trovato, C.M.; Montuori, M.; Cucchiara, S. Pediatric Celiac Disease: Follow-Up in the Spotlight12. Adv. Nutr. 2017, 8, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Anania, C.; Pacifico, L.; Olivero, F.; Perla, F.M.; Chiesa, C. Cardiometabolic risk factors in children with celiac disease on a gluten-free diet. World J. Clin. Pediatr. 2017, 6, 143–148. [Google Scholar] [CrossRef]
- European Food Safety Authority. Guidance on the EU Menu methodology. EFSA J. 2014, 12, 3944. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Ingestas diarias recomendadas de energía y nutrients para la población española. In Tablas de Composición de Alimentos, 18th ed.; Ediciones Pirámide (Grupo Anaya, SA): Madrid, Spain, 2016. [Google Scholar]
- Aranceta, J. Objetivos nutricionales para la población española. Consenso de la Sociedad Española de Nutrición Comunitaria (SENC). Rev. Esp. Nutr. Comunitaria 2011, 17, 178–199. [Google Scholar]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Standards for Anthropometric Assesment (ISAK); ISAK: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.; Horswill, C.A.; Stillman, R.J.; Van Loan, M.D.; Bemben, D.A. Skinfold equations for estimation of body fatness in children and youth. Hum. Boil. 1988, 60, 709–723. [Google Scholar]
- WHO Multicentre Growth Reference Study Group; de Onis, M. Assessment of differences in linear growth among populations in the WHO Multicentre Growth Reference Study. Acta Paediatr. 2006, 95, 56–65. [Google Scholar]
- Fernández, C.L.H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de Crecimiento de Bilbao. Curvas y Tablas de Crecimiento. Estudio Transversal; Fundación Faustino Orbegozo: Vizcaya, Spain, 2011. [Google Scholar]
- Díaz, J.A.; Soblechero, B.A.; Caballero, P.B.; Hernández, L.D.; Yepes, M.G.; Castelar, J.L.; Rosa, J.R.; de Espinosa, M.G. Diagnosis de la obesidad: Actualización de criterios y su validez clínica y poblacional. An. Pediatr. 2006, 65, 5–14. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- Manchola-González, J.; Bagur-Calafat, C.; Girabent-Farrés, M. Fiabilidad de la versión española del cuestionario de actividad física PAQ-C/Reliability Spanish Version of Questionnaire of Physical Activity PAQ-C. Rev. Int. de Med. Cienc. de la Act. Física Deporte 2017, 17, 139–152. [Google Scholar] [CrossRef]
- Martinez-Gomez, D.; Martínez-De-Haro, V.; Pozo, T.; Welk, G.J.; Villagra, A.; Calle, M.E.; Marcos, A.; Veiga, O.L. Fiabilidad y validez del cuestionario de actividad física PAQ-A en adolescentes españoles. Rev. Esp. Salud Pública 2009, 83, 427–439. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Actividad Física para la Salud y Reducción del Sedentarismo. Recomendaciones Para la Población; NIBO: Madrid, Spain, 2015. [Google Scholar]
- García-Manzanares, Á.; Lucendo, A.J. Review: Nutritional and Dietary Aspects of Celiac Disease. Nutr. Clin. Pract. 2011, 26, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Segura, M.E.M.; Rosell, C.M. Chemical Composition and Starch Digestibility of Different Gluten-free Breads. Plant Foods Hum. Nutr. 2011, 66, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caponio, F.S.C.; Clodoveo, M.L.; Pasqualone, A. Evaluation of the nutritional quality of the lipid fraction of gluten-free biscuits. Eur. Food Res. Technol. 2008, 227, 135–139. [Google Scholar] [CrossRef]
- Ruiz, E.; Ávila, J.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; et al. Macronutrient Distribution and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española de Seguridad Alimentaria y Nutrición. Encuesta Nacional de Ingesta Dietética Española; Agencia Española de Seguridad Alimentaria y Nutrición: Madrid, Spain, 2011. [Google Scholar]
- Missbach, B.; Schwingshackl, L.; Billmann, A.; Mystek, A.; Hickelsberger, M.; Bauer, G.; König, J. Gluten-free food database: The nutritional quality and cost of packaged gluten-free foods. PeerJ 2015, 3, e1337. [Google Scholar] [CrossRef] [PubMed]
- Raehsler, S.L.; Choung, R.S.; Marietta, E.V.; Murray, J.A. Accumulation of heavy metals in people on a gluten-free diet. Clin. Gastroenterol. Hepatol. 2018, 16, 244–251. [Google Scholar] [CrossRef]
- De Lorenzo, A. Assessment of body composition by bioelectrical impedance in adolescent patients with celiac disease. Am. J. Gastroenterol. 1999, 94, 2951–2955. [Google Scholar] [PubMed]
- Capriati, T.; Francavilla, R.; Ferretti, F.; Castellaneta, S.; Ancinelli, M.; Diamanti, A. The overweight: A rare presentation of celiac disease. Eur. J. Clin. Nutr. 2016, 70, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Valletta, E.; Fornaro, M.; Cipolli, M.; Conte, S.; Bissolo, F.; Danchielli, C. Celiac disease and obesity: Need for nutritional follow-up after diagnosis. Eur. J. Clin. Nutr. 2010, 64, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Norsa, L.; Shamir, R.; Zevit, N.; Verduci, E.; Hartman, C.; Ghisleni, D.; Riva, E.; Giovannini, M. Cardiovascular disease risk factor profiles in children with celiac disease on gluten-free diets. World J. Gastroenterol. 2013, 19, 5658–5664. [Google Scholar] [CrossRef] [PubMed]
- Barera, G.; Mora, S.; Brambilla, P.; Ricotti, A.; Menni, L.; Beccio, S.; Bianchi, C. Body composition in children with celiac disease and the effects of a gluten-free diet: A prospective case-control study. Am. J. Clin. Nutr. 2000, 72, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Brar, P.S.; Lee, A.R.; Green, P.H. Body mass index in celiac disease: Beneficial effect of a gluten-free diet. J. Clin. Gastroenterol. 2010, 44, 267–271. [Google Scholar] [CrossRef]
- Radlović, N.; Mladenović, M.; Leković, Z.; Zivanović, D.; Brdar, R.; Radlović, V.; Ristić, D.; Pavlović, M.; Stojsić, Z.; Vuletić, B.; et al. Effect of gluten-free diet on the growth and nutritional status of children with coeliac disease. Srp. Arh. Celok. Lek. 2009, 137, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Reilly, N.R.; Aguilar, K.; Hassid, B.G.; Cheng, J.; DeFelice, A.R.; Kazlow, P.; Bhagat, G.; Green, P.H. Celiac disease in normal-weight and overweight children: Clinical features and growth outcomes following a gluten-free diet. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Pozzobon, G.; Pietrobelli, A. Physical activity as the main therapeutic tool for metabolic syndrome in childhood. Int. J. Obes. 2011, 35, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Venkatasubramani, N.; Telega, G.; Werlin, S.L. Obesity in Pediatric Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 295–297. [Google Scholar] [CrossRef]
- Aranceta, J.; Pérez-Rodrigo, C.; Ribas, L.; Serra-Majem, L.; Serra-Majem, L. Sociodemographic and lifestyle determinants of food patterns in Spanish children and adolescents: The enKid study. Eur. J. Clin. Nutr. 2003, 57, S40–S44. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Estudio ALADINO 2015: Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España 2015; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2016. [Google Scholar]
- Brambilla, P.; Picca, M.; DiLillo, D.; Meneghin, F.; Cravidi, C.; Tischer, M.; Vivaldo, T.; Bedogni, G.; Zuccotti, G.V. Changes of body mass index in celiac children on a gluten-free diet. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 177–182. [Google Scholar] [CrossRef]
- Van Der Pals, M.; Myléus, A.; Norström, F.; Hammarroth, S.; Högberg, L.; Rosén, A.; Ivarsson, A.; Carlsson, A. Body mass index is not a reliable tool in predicting celiac disease in children. BMC Pediatr. 2014, 14, 165. [Google Scholar] [CrossRef]
- Dufour, D.R.L.J.A.; Nolte, F.S.; Gretch, D.R.; Koff, R.S.; Seeff, L.B. Guías del laboratorio para screening, diagnóstico y monitoreo de la lesión hepática. Acta Bioquím. Clin. Latinoam. 2005, 39, 359–376. [Google Scholar]
- Córdoba, C.G.F. Vitamina D: Una Perspectiva Actual. Sociedad Española de Bioquímica Clínica y Patología Molecular: Barcelona, Spain, 2013. [Google Scholar]
- Motta, M.E.F.A.; De Faria, M.E.N.; Da Silva, G.A.P. Prevalence of low bone mineral density in children and adolescents with celiac disease under treatment. Sao Paulo Med. J. 2009, 127, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, H.; Mazure, R.; Gonzalez, D.; Flores, D.; Pedreira, S.; Niveloni, S.; Smecuol, E.; Mauriño, E.; Bai, J.C. Risk of fractures in celiac disease patients: A cross-sectional, case-control study. Am. J. Gastroenterol. 2000, 95, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.L.; Bardella, M.T. Bone in celiac disease. Osteoporos Int. 2008, 19, 1705–1716. [Google Scholar] [CrossRef] [PubMed]
- Krupa-Kozak, U. Pathologic bone alterations in celiac disease: Etiology, epidemiology, and treatment. Nutrition 2014, 30, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krzesiek, E.; Iwańczak, B. Assessment of bone mineral density in children with celiac disease. Pol. Merkur. Lek. Organ Pol. Tow. Lek. 2008, 24, 219–226. [Google Scholar]
- Kirsaçlioğlu, C.T.; Kuloğlu, Z.; Tanca, A.; Küçük, N.O.; Aycan, Z.; Ocal, G.; Ensari, A.; Kalayci, A.G.; Girgin, N.; Kırsaçlıoğlu, C.T.; et al. Bone mineral density and growth in children with coeliac disease on a gluten free-diet. Turk. J. Med. Sci. 2016, 46, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, J.; Bohdanowicz-Pawlak, A.; Waszczuk, E.; Jakubowska, J. Low bone mineral density in adult patients with coeliac disease. Endokrynol. Polska 2012, 63, 270–276. [Google Scholar]
- Krupa-Kozak, U.; Drabińska, N. Calcium in Gluten-Free Life: Health-Related and Nutritional Implications. Foods 2016, 5, 51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Question | Yes |
|---|---|
| Are you the only one who follows a gluten-free diet at home? | 74.3% |
| Do you have trouble knowing what you can eat and what you cannot? | 20.0% |
| Have you received information on celiac disease and on the labeling of gluten-free products? | 84.3% |
| Would you say that you follow a strict gluten-free diet? | 98.6% |
| Have you noticed improvement in your health since you started on the gluten-free diet? | 82.9% |
| Perceived changes: | |
| I have lost weight | 18.6% |
| I have gained weight | 38.6% |
| I am more active | 42.9% |
| When you eat away from home, do you have any problem because you suffer celiac disease? | 58.6% |
| Is your diet very different from your siblings/cousins/friends? | 25.7% |
| At home, do you usually buy gluten-free industrially manufactured products? | 98.6% |
| Do you find it difficult to build up a gluten-free menu? | 7.1% |
| You don’t eat more gluten-free products… | |
| Because you don’t like them | 31.4% |
| Because they are expensive | 25.7% |
| Because you consider that your diet is already complete | 51.4% |
| Your perception of gluten-free products is: | |
| I find them insipid | 18.6% |
| I find them tasty | 44.3% |
| I like their texture | 28.6% |
| I think they have a similar quality to their gluten-containing counterparts | 34.3% |
| I have never tried products that contain gluten | 31.4% |
| Food Group | Food Frequency Consumption (Number of Portions/Week) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Milk and yogurt | 12.5 (10.0–14.2) | 12.0 (10.0–14.0) | 13.0 (10.0–15.0) | 11.0 (8.5–14.0) | 12.0 (10.0–14.0) | 12.0 (10.0–14.0) | 12.5 (10.0–14.0) | 12.0 (10.0–14.0) | 12.0 (9.7–16.2) | 12.0 (8.0–14.0) |
| Fruit | 10.0 (6.0–14.0) | 8.0 (5.0–12.0) | 10.0 * (7.0–15.0) | 7.0 (4.0–10.5) | 8.0 (6.0–11.0) | 10.0 (6.7–13.0) | 10.0 (6.0–14.0) | 10.0 (6.0–13.0) | 7.5 (6.7–11.0) | 6.0 (4.0–10.0) |
| Vegetables | 8.0 (4.0–8.0) | 8.0 (6.0–8.0) | 8.0 (4.0–8.0) | 8.0 (6.0–8.0) | 7.0 (4.0–8.0) | 8.0 (6.0–8.0) | 8.0 (4.5–8.0) | 8.0 (6.0–8.0) | 6.0 (4.0–8.0) | 8.0 (6.0–8.0) |
| Legumes | 2.0 (2.0–2.0) | 2.0 (2.0–2.0) | 2.0 (2.0–2.0) | 2.0 (2.0–2.0) | 2.0 (2.0–2.0) | 2.0 (2.0–3.0) | 2.0 (2.0–2.0) | 2.0 (2.0–2.0) | 2.0 (2.0–2.2) | 2.0 (2.0–3.0) |
| Meat | 6.0 (4.0–8.0) | 6.0 (4.0–8.0) | 6.0 (4.0–8.0) | 6.0 (4.5–8.0) | 6.0 (4.0–8.0) | 6.0 (4.0–8.0) | 6.0 (4.0–7.7) | 6.0 (4.7–8.0) | 6.0 (3.7–8.0) | 7.0 (4.0–8.0) |
| Fish | 4.0 (3.0–6.0) | 4.0 (3.0–6.0) | 4.0 (3.0–6.0) | 4.0 (3.0–6.0) | 5.0 (3.0–6.0) | 3.0 (3.0–6.0) | 5.0 (3.0–6.0) | 4.0 (3.0–6.0) | 3.0 (2.7–5.2) | 3.0 (3.0–5.0) |
| Bread/pasta/rice | 14.0 * (11.0–20.0) | 18.0 (12.0–22.0) | 16.0 (12.0–21.0) | 18.0 (13.0–22.5) | 14.0 (10.0–19.0) | 17.0 (12.0–20.5) | 14.0 (10.2–21.7) | 18.0 (12.0–22.0) | 14.5 * (11.7–16.7) | 18.0 (16.0–22.5) |
| Pastries | 6.0 (4.0–8.0) | 7.0 (4.0–10.0) | 6.0 (3.0–8.0) | 7.0 (2.5–10.0) | 6.0 (4.0–8.0) | 7.0 (4.0–10.0) | 6.0 (4.0–8.75) | 7.0 (3.5–10.0) | 6.0 (3.7–8.0) | 6.0 (3.5–9.0) |
| Nutrient | Percentage Contribution of Macronutrients Total Energy Intake (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Carbohydrates | 39.9 (35.5–43.5) | 39.9 (35.9–4.3) | 40.6 (37.2–44.4) | 40.1 (35.9–43.7) | 38.1 (34.0–42.4) | 39.1 (35.0–46.4) | 39.8 (35.8–43.7) | 39.6 (35.2–43.5) | 40.1 (34.2–42.8) | 42.4 (37.0–45.6) |
| Proteins | 15.5 * (13.9–16.5) | 16.5 (15.3–18.5) | 15.2 * (14.2–16.4) | 16.4 (15.3–18.7) | 16.0 (13.1–16.6) | 16.7 (15.3–17.1) | 15.3 * (13.9–165–) | 16.8 (15.5–18.0) | 15.8 (14.5–16.4) | 15.7 (14.9–19.9) |
| Lipids | 41.6 (38.1–44.6) | 40.7 (37.5–45.6) | 40.0 (36.7–43.4) | 40.7 (37.8–44.9) | 42.4 (38.3–46.7) | 41.0 (36.0–46.4) | 42.1 (37.3–45.0) | 43.2 (37.7–47.3) | 40.3 (38.7–41.3) | 39.7 (37.0–43.6) |
| Nutrient | Percentage Contribution of Lipids to Total Energy Intake (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| PUFA | 3.9 * (3.4–4.4) | 4.4 (3.8–5.2) | 3.7 * (3.5–4.2) | 4.3 (2.8–5.2) | 4.0 * (3.4–4.5) | 4.6 (3.9–5.6) | 3.9 * (3.3–4.4) | 4.4 (3.7–5.0) | 4.2 * (3.5–4.3) | 4.6 (4.1–5.6) |
| MUFA | 17.5 (13.9–19.8) | 17.9 (14.6–20.7) | 15.5 (13.7–18.6) | 18.1 (14.5–20.0) | 17.9 (14.4–20.1) | 17.3 (15.5–21.3) | 17.6 (13.9–19.8) | 18.7 (15.6–21.3) | 17.1 (14.7–19.3) | 16.2 (14.0–17.9) |
| SFA | 14.2 (12.8–15.5) | 13.8 (12.1–15.6) | 13.9 (12.0–14.7) | 13.8 (12.1–15.6) | 14.5 (12.9–16.0) | 13.8 (12.1–15.6) | 14.3 (12.2–15.5) | 13.9 (12.5–15.9) | 14.0 (13.5–14.7) | 13.8 (11.51–4.9) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Fiber (g/day) | 16.3 (13.1–20.9) | 15.9 (13.6–20.0) | 16.5 (15.0–23.2) | 15.9 (13.1–19.5) | 15.5 (12.4–19.0) | 16.1 (13.9–22.0) | 16.3 (13.5–20.8) | 15.9 (13.7–20.8) | 15.7 (12.4–24.3) | 15.3 (13.4–17.8) |
| Percentage Contribution of Mineral Intakes to Recommended Intakes (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Calcium | 64.1 * (24.1–133.2) | 74.7 (43.6–145.5) | 64.2 * (49.6–70.8) | 75.2 (61.9–94.5) | 64.5 (52.4–82.9) | 74.3 (62.6–93.9) | 66.5 * (56.1–77.0) | 76.9 (66.5–97.1) | 56.9 (45.1–62.4) | 65.1 (58.0–78.3) |
| Phosphorus | 115.0 (46.5–265.6) | 139.5 (65.6–359.8) | 111.9 (97.8–153.9) | 140.2 (104–190.6) | 125.7 (95.9–191.0) | 136.3 (109.2–190.8) | 128.2 * (98.5–177.4) | 161.4 (115.2–207.5) | 101.3 (93.8–112.7) | 120.4 (87.6–139.5) |
| Magnesium | 74.4 * (32.4–180.4) | 82.8 (29.5–179.4) | 62.6 * (54.6–85.8) | 78.9 (65.0–94.1) | 79.3 (54.3–94.8) | 87.6 (72.3–100.7) | 76.0 * (57.4–92.9) | 88.0 (76.1–103.2) | 56.0 (45.2–77.3) | 67.0 (62.0–82.8) |
| Iron | 76.0 * (18.9–212.2) | 103.1 (46.7–223.3) | 76.0 * (64.2–102.5) | 110.3 (85.8–133.9) | 74.7 (43.9–103.3) | 102.2 (59.4–124.4) | 81.7 * (55.4–105.0) | 116.4 (90.7–150.6) | 68.4 (64.2–82.8) | 78.3 (61.7–99.2) |
| Zinc | 65.6 (24.0–137.0) | 67.5 (32.7–142.0) | 66.0 (53.3–82.0) | 64.7 (54.7–87.1) | 65.4 (43.4–81.0) | 69.3 (57.0–89.0) | 66.7 * (47.0–83.0) | 75.7 (59.0–96.5) | 58.7 (46.0–71.1) | 56.7 (47.3–69.3) |
| Iodine | 77.8 (27.2–448.9) | 79.9 (28.9–170.0) | 75.2 (55.9–89.8) | 79.2 (72.1–95.2) | 92.2 (58.3–107.0) | 85.9 (66.3–98.5) | 79.7 (57.8–106.6) | 86.6 (101.4–76.7) | 62.8 (51.5–81.2) | 66.3 (52.3–79.3) |
| Selenium | 159.9 * (38.2–416.7) | 268.3 (75,0–670,0) | 159.9 * (132.4–220.3) | 299.2 (181,0–365,0) | 155.7 * (126.3–205.1) | 234.0 (187.8–313.3) | 170.0 * (136.6–223.6) | 299.2 (199.3–376.3) | 127.6 * (83.3–143.4) | 210.0 (177.4–304.7) |
| Percentage Contribution of Mineral and Vitamin Intakes to Recommended Intakes (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample | Boys | Girls | Children (41–2 Years) | Adolescents (131–8 Years) | ||||||
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Thiamine | 110.0 * (36.7–18.2) | 133.3 (63.0–300) | 110.0 (82.7–45.5) | 120.5 (95.0–65.3) | 106.1 (91.1–57.1) | 149.4 (111.1–77.8) | 110.0 * (87.4–58.6) | 141.6 (105.2–84.7) | 96.4 (82.4–29.7) | 120.0 (92.0–56.4) |
| Riboflavin | 107.1 * (37.1–90.0) | 121.4 (64.7–25.0) | 106.3 (86.9–125.0) | 119.7 (93.5–142.5) | 107.7 (92.9–150.0) | 121.4 (114.3–140.1) | 113.3 (93.1–141.7) | 129.7 (113.3–150.0) | 94.1 (82.0–105.9) | 100.1 (88.4–129.4) |
| Pyridoxine | 118.5 * (35.0–312.8) | 141.9 (50.6–285.7) | 113.4 * (90.5–137.5) | 139.3 (99.3–137.5) | 120.1 (87.5–136.4) | 141.9 (123.8–157.1) | 121.4 * (93.8–142.0) | 143.2 (125.0–159.8) | 95.2 (90.5–102.3) | 109.5 (95.2–150.0) |
| Vitamin B12 | 276.7 (42.0–1826.7) | 295.2 (65.0–1230.0) | 276.7 (205.0–338.9) | 282.5 (214.2–355.0) | 281.7 * (213.3–326.7) | 320.0 (248.5–422.8) | 270.0 (211.7–320.0) | 311.7 (244.3–357.5) | 328.1 (204.8–410.0) | 263.6 (175.0–422.8) |
| Niacin | 177.4 * (68.2–286.9) | 231.4 (76.9–383.9) | 185.2 * (154.6–223.4) | 227.6 (191.8–270.7) | 166.7 (146.2–214.2) | 233.3 (196.9–257.6) | 184.6 * (155.1–222.7) | 237.9 (204.7–276.5) | 158.2 (141.8–200.6) | 216.5 (158.2–248.4) |
| Folates | 67.45 * (23.3–190.5) | 82.0 (32.5–244.5) | 61.5 (49.3–89.3) | 77.9 (54.8–104.0) | 77.5 * (44.8–87.2) | 87.7 (56.7–117.2) | 77.0 * (48.9–95.0) | 89.5 (71.6–117.6) | 58.7 (44.2–62.0) | 55.0 (47.0–70.3) |
| Vitamin C | 167.9 (19.7–484.0) | 151.3 (32.7–447.2) | 196.3 (100.7–246.7) | 130.6 (88.0–212.5) | 153.9 (91.5–232.7) | 178.3 (139.8–271.7) | 161.7 (94.8–226.8) | 169.9 (109.6–245.3) | 225.0 (112.2–263.3) | 129.7 (85.8–186.7) |
| Pantothenic acid | 118.2 (34.0–180.0) | 128.5 (66.0–205.0) | 123.5 (104.4–130) | 116.8 (108.5–146.7) | 119.4 (87.5–152.5) | 132.9 (116.0–147.6) | 125.0 (100.0–140.0) | 135.0 * (115.0–157.5) | 106.0 (92.0–116.0) | 122.0 (100.0–130.0) |
| Biotin | 143.25 (21.6–414.3) | 131.2 (52.5–308.6) | 140.5 (97.0–183.6) | 125.0 (92.1–169.9) | 154.7 (88.4–216.7) | 142.5 (96.1–220.1) | 158.8 (102.5–214.0) | 156.6 (120.3–211.2) | 116.0 (88.4–140.9) | 91.2 (74.4–131.8) |
| Vitamin A | 97.5 (20.7–343.8) | 120.8 (11.7–631.8) | 83.7 (57.3–166.8) | 100.3 (54.9–185.0) | 123.5 (73.1–210.3) | 151.2 (100.1–191.3) | 110.2 62.6–184.8) | 148.5 (95.7–206.4) | 77.8 (63.1–119.3) | 78.0 (55.0–136.1) |
| Vitamin D | 10.0 (1.2–294.7) | 13.2 (0.9–360.0) | 11.0 (4.0–18.7) | 11.3 (7.4–22.5) | 9.0 (6.7–18.0) | 15.6 (7.3–26.7) | 8.7 (4.8–17.9) | 13.6 (6.4–22.4) | 14.0 (8.7–22.0) | 10.7 (8.0–26.7) |
| Vitamin E | 62.2 (31.0–111.3) | 65.0 (20.0–162.5) | 62.8 (50.1–77.5) | 64.6 (41.9–85.0) | 61.0 (40.0–82.0) | 70.0 (55.0–88.0) | 63.0 (48.6–79.8) | 73.1 (58.8–90.0) | 55.8 (40.0–72.6) | 51.7 (40.0–64.8) |
| Vitamin K | 144.6 (34.9–381.7) | 142.8 (30.6–406.7) | 145.6 (86.5–196.4) | 127.7 (94.5–202.1) | 143.0 (74.9–201.8) | 148.4 (100.4–169.9) | 146.8 (87.8–199.1) | 161.5 (105.6–202.1) | 93.7 (69.9–197.0) | 100.6 (60.7–151.8) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Weight (kg) | 34.1 (23.9–46.9) | 35.9 (28.7–51.5) | 35.3 (27.5–52.1) | 34.3 (28.3–54.3) | 33.4 (22.1–45.9) | 38.4 (30.4–49.0) | 31.6 (22.5–38.3) | 31.1 (25.4–37.6) | 55.0 (48.1–59.7) | 56.4 (49.2–72.7) |
| Height (cm) | 139.9 (123.8–155.4) | 141.8 (128.0–159.6) | 139.7 (126.4–156.0) | 141.8 (127.9–161.0) | 140.1 (115.5–155.0) | 142.9 (128.2–158.7) | 137.5 (119.1–145.9) | 134.4 (122.9–142.7) | 163.8 (159.1–173.0) | 161.4 (158.9–170.7) |
| BMI (kg/m2) | 17.0 (15.7–19.2) | 18.5 (15.8–21.2) | 17.1 (16.0–19.7) | 19.1 (16.0–21.9) | 16.9 (15.5–18.7) | 17.6 (15.7–20.8) | 16.7 (15.4–18.3) | 17.1 (15.3–19.8) | 19.4 (18.3–22.9) | 21.6 (19.3–24.8) |
| Body fat (% of total weight) | 16.3 (12.9–22.5) | 17.0 (13.5–23.3) | 15.2 (11.0–23.3) | 14.5 (12.0–22.8) | 17.6 (14.1–22.4) | 19.1 (15.5–24.9) | 16.1 (13.3–22.4) | 15.9 (12.4–22.8) | 18.2 (10.8–23.3) | 21.5 (14.3–24.1) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 70) | Non-Celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| BMD (g/cm2) | 0.522 (0.467–0.593) | 0.517 (0.464–0.576) | 0.540 (0.468–0.565) | 0.520 (0.466–0.568) | 0.515 (0.454–0.575) | 0.505 (0.459–0.614) | 0.517 (0.458–0.579) | 0.514 (0.464–0.552) | 0.602 (0.501–0.720) | 0.517 (0.459–0.633) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 67) | Non-Celiac (n = 66) | Celiac (n = 33) | Non-Celiac (n = 41) | Celiac (n = 34) | Non-Celiac (n = 25) | Celiac (n = 53) | Non-Celiac (n = 45) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Iron (µg/dL) | 98.0 (75.0–123.0) | 102.5 (83.0–123.0) | 90.0 (74.0–109.0) | 101.0 (83.0–116.0) | 108.0 (84.0–132.0) | 109.0 (83.0–123.0) | 98.0 (79.0–123.0) | 104.0 (84.0–124.0) | 95.5 (68.0–122.0) | 101.0 (82.0–110.0) |
| AST (U/L) | 30.0 (26.0–35.5) | 31.0 (26.0–37,0) | 31.0 (27.0–37.0) | 31.0 (27.0–37.0) | 28.5 (24.0–33.0) | 28.0 (25.0–33.0) | 31.0 (27.0–36.0) | 32.0 (28.0–38.0) | 26.0 (19.0–32.0) | 25.0 (21.0–31.0) |
| ALT (U/L) | 27.0 (23.0–31.0) | 29.0 (24.0–32.0) | 28.0 (24.0–32.0) | 30.0 (26.0–32.0) | 26.0 (22.0–31.0) | 27.0 (23.0–30.0) | 27.0 (23.0–31.0) | 29.0 (25.0–33.0) | 29.0 (27.0–40.0) | 27.0 (22.5–30.0) |
| Alkaline Phosphatase (U/L) | 197.0 (161.5–228.5) | 207.0 (171.0–251.0) | 195.0 (162.0–239.0) | 207.0 (182.0–266.0) | 198.0 (161.0–225.0) | 202.0 (142.0–249.0) | 210.0 (188.0–237.0) | 211.0 (193.0–274.0) | 78.5 (54.0–159.0) | 141.0 (89.0–222.0) |
| Phosphorus (mg/dL) | 5.0 (4.7–5.4) | 5.0 (4.7–5.4) | 5.1 (4.7–5.4) | 5.0 (4.7–5.4) | 5.0 (4.7–5.3) | 5.0 (4.6–5.3) | 5.1 (4.9–5.5) | 5.1 (4.9–5.5) | 4.4 (4.2–5.0) | 4.7 (4.2–5.0) |
| Folate (ng/mL) | 6.7 (4.3–9.1) | 6.0 (4.5–8.2) | 7.1 (4.3–9.9) | 6.0 (4.2–8.5) | 6.4 (4.3–8.4) | 6.0 (4.8–7.5) | 7.0 (4.4–9.9) | 6.9 (4.6–10.8) | 5.0 (4.1–7.2) | 4.9 (3.6–6.0) |
| Vitamin D (ng/mL) | 28.0 (22.8–33.9) | 28.9 (23.9–35.8) | 30.6(4.3–36.5) | 26.6 (23.7–33.7) | 25.9 * (21.9–32.6) | 30.7 (25.8–36.5) | 27.9 (22.9–33.6) | 29.8 (24.1–36.5) | 28.8 (22.7–35.8) | 26.1 (23.0–32.3) |
| Calcium (mg/dL) | 9.8 (9.6–10.0) | 9.8 (9.6–9.9) | 9.8(9.7–10.0) | 9.8 (9.5–10.0) | 9.8 (9.7–10.0) | 9.7 (9.5–10.0) | 9.8 (9.6–10.0) | 9.8 (9.6–10.0) | 9.7 (9.6–10.0) | 9.7 (9.5–9.9) |
| Growth hormone (ng/mL) | 0.3 (0.1-3.5) | 0.4 (0.1–1.9) | 0.5 (0.3–1.0) | 0.2 (0.1–0.2) | 1.9 (0.2–5.3) | 0.5 (0.3–2.5) | 0.3 (0.1–3.1) | 0.4 (0.1–1.4) | 1.0 (0.3–7.3) | 0.4 (0.1–2.5) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 46) | Non-Celiac (n = 48) | Celiac (n = 22) | Non-Celiac (n = 34) | Celiac (n = 24) | Non-Celiac (n = 14) | Celiac (n = 36) | Non-Celiac (n = 34) | Celiac (n = 10) | Non-Celiac (n = 14) | |
| Glucose (mg/dL) | 79.5 (76.0–84.0) | 79.5 (76.0–83.5) | 79.5 (76.0–84.0) | 80.0 (76.0–85.0) | 80.0 (77.0–83.5) | 78.5 (73.7–82.0) | 80.5 (76.0–83.5) | 80.0 (76.0–84.0) | 79.0 (69.0–84.0) | 79.0 (78.0–82.0) |
| Cholesterol (mg/dL) | 167.0 (143.0–184.0) | 163.5 (152.0–182.0) | 168.0 (146.0–177.0) | 165.0 (152.0–189.0) | 165.5 (142.5–194.0) | 162.5 (153.0–182.2) | 168.5 (142.5–186.5) | 165.0 (154.0–190.0) | 159.0 (150.0–184.0) | 158.5 (140.0–179.0) |
| Triglyceri-des (mg/dL) | 42.5 (38.0–59.0) | 52.0 (38.0–62.5) | 42.5 (35.0–61.0) | 52.0 (38.0–60.0) | 40.5 (35.7–61.5) | 52.0 (37.2–61.5) | 42.0 (37.5–56.5) | 52.0 (38.0–62.0) | 55.5 (38.0–61.0) | 50.0 (38.0–60.0) |
| HDL-Cholesterol (mg/dL) | 64.5 (54.0–74.0) | 64.5 (59.0–75.5) | 70.5 (54.0–76.0) | 63.0 (59.0–71.0) | 64.0 (55.0–69.5) | 66.5 (60.0–81.0) | 64.0 (55.0–72.0) | 68.5 (59.0–77.0) | 70.5 (54.0–76.0) | 60.0 (59.0–67.0) |
| LDL-Cholesterol (mg/dL) | 92.1 (73.2–100.4) | 88.7 (76.9–101.6) | 86.9 (72.0–98.6) | 89.1 (75.2–18.6) | 94.3 (78.8–117.2) | 86.8 (78.8–92.6) | 94.1 (76.1–100.6) | 89.2 (83.2–99.0) | 80.8 (72.0–97.8) | 78.8 (72.5–109.7) |
| Total Cholesterol/HDL Cholesterol | 2.4 (2.3–2.7) | 2.4 (2.2–2.9) | 2.4 (2.2–2.6) | 2.6 (2.2–3.1) | 2.6 * (2.4–2.9) | 2.3 (2.2–2.7) | 2.5 (2.2–2.9) | 2.4 (2.2–2.9) | 2.5 (2.2–2.6) | 2.5 (2.0–3.0) |
| LDL-Cholesterol /HDL-Cholesterol | 1.3 (1.2–1.6) | 1.3 (1.1–1.8) | 1.4 (1.1–1.8) | 1.3 (1.1–1.4) | 1.4 * (1.3–1.7) | 1.2 (1.1–1.5) | 1.4 (1.2–1.7) | 1.3 (1.1–1.8) | 1.3 (1.0–1.4) | 1.4 (0.9–1.8) |
| Total Sample | Boys | Girls | Children (4–12 Years) | Adolescents (13–18 Years) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Celiac (n = 70) | Non-celiac (n = 67) | Celiac (n = 35) | Non-Celiac (n = 41) | Celiac (n = 35) | Non-Celiac (n = 26) | Celiac (n = 56) | Non-Celiac (n = 46) | Celiac (n = 14) | Non-Celiac (n = 21) | |
| Score | 2.5 (2.0–3.2) | 2.7 (2.2–3.3) | 2.5 (2.0–3.2) | 2.8 (2.2–3.5) | 2.5 (1.9–3.2) | 2.6 (2.3–3.1) | 2.5 * (2.0–3.2) | 3.0 (2.5–3.4) | 2.8 * (2.2–3.1) | 2.2 (1.7–2.7) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández, C.B.; Varela-Moreiras, G.; Úbeda, N.; Alonso-Aperte, E. Nutritional Status in Spanish Children and Adolescents with Celiac Disease on a Gluten Free Diet Compared to Non-Celiac Disease Controls. Nutrients 2019, 11, 2329. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102329
Fernández CB, Varela-Moreiras G, Úbeda N, Alonso-Aperte E. Nutritional Status in Spanish Children and Adolescents with Celiac Disease on a Gluten Free Diet Compared to Non-Celiac Disease Controls. Nutrients. 2019; 11(10):2329. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102329
Chicago/Turabian StyleFernández, Catalina Ballestero, Gregorio Varela-Moreiras, Natalia Úbeda, and Elena Alonso-Aperte. 2019. "Nutritional Status in Spanish Children and Adolescents with Celiac Disease on a Gluten Free Diet Compared to Non-Celiac Disease Controls" Nutrients 11, no. 10: 2329. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102329