Effect of a Very-Low-Calorie Ketogenic Diet on Circulating Myokine Levels Compared with the Effect of Bariatric Surgery or a Low-Calorie Diet in Patients with Obesity

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
2.2.1. VLCK Diet
2.2.2. Low-Calorie Diet
2.2.3. Bariatric Surgery
2.3. Anthropometric and Body Composition Measurements
2.4. Biochemical Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128·9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Apovian, C.M.; Aronne, L.J.; Bessesen, D.H.; McDonnell, M.E.; Murad, M.H.; Pagotto, U.; Ryan, D.H.; Still, C.D. Endocrine Society. Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2015, 100, 342–362. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving Healthy Muscle during Weight Loss. Adv. Nutr. 2017, 8, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verreijen, A.M.; Engberink, M.F.; Memelink, R.G.; van der Plas, S.E.; Visser, M.; Weijs, P.J.M. Effect of a High Protein Diet and/or Resistance Exercise on the Preservation of Fat Free Mass during Weight Loss in Overweight and Obese Older Adults: A Randomized Controlled Trial. Nutr. J. 2017, 16, 10. [Google Scholar] [CrossRef]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Ordoñez-Mayan, L.; Carreira, J.; Galban, C.; Martinez-Olmos, M.A.; Crujeiras, A.B.; Sajoux, I.; Casanueva, F.F. Body Composition Changes after Very Low-Calorie-Ketogenic Diet in Obesity Evaluated by Three Standardized Methods. J. Clin. Endocrinol. Metab. 2016, 102, 2016–2385. [Google Scholar] [CrossRef]
- Frimel, T.N.; Sinacore, D.R.; Villareal, D.T. Exercise Attenuates the Weight-Loss-Induced Reduction in Muscle Mass in Frail Obese Older Adults. Med. Sci. Sports Exerc. 2008, 40, 1213–1219. [Google Scholar] [CrossRef] [Green Version]
- Bonfanti, N.; Fernández, J.M.; Gomez-Delgado, F.; Pérez-Jiménez, F. Effect of two hypocaloric diets and their combination with physical exercise on basal metabolic rate and body composition. Nutr. Hosp. 2014, 29, 635–643. [Google Scholar] [CrossRef]
- Jastrzębska-Mierzyńska, M.; Ostrowska, L.; Hady, H.R.; Dadan, J.; Konarzewska-Duchnowska, E. The Impact of Bariatric Surgery on Nutritional Status of Patients. Wideochir Inn. Tech. Maloinwazyjne 2015, 10, 115–124. [Google Scholar] [CrossRef]
- Merra, G.; Miranda, R.; Barrucco, S.; Gualtieri, P.; Mazza, M.; Moriconi, E.; Marchetti, M.; Chang, T.F.M.; De Lorenzo, A.; Di Renzo, L. Very-Low-Calorie Ketogenic Diet with Aminoacid Supplement versus Very Low Restricted-Calorie Diet for Preserving Muscle Mass during Weight Loss: A Pilot Double-Blind Study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2613–2621. [Google Scholar]
- Ahima, R.S.; Park, H.K. Connecting Myokines and Metabolism. Endocrinol. Metab. 2015, 30, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Jun, H.S. Role of Myokines in Regulating Skeletal Muscle Mass and Function. Front. Physiol. 2019, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscle as an Endocrine Organ: Focus on Muscle-Derived Interleukin-6. Physiol. Rev. 2008, 88, 1379–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.M.; Choo, S. Salivary Leptin Level in Young Adult Males and Its Association with Anthropometric Measurements, Fat Distribution and Muscle Mass. Eur. Endocrinol. 2018, 14, 94–98. [Google Scholar] [CrossRef]
- León, H.H.; Melo, C.A.; Ramírez, J.F. Role of the Myokines Production through the Exercise. J. Sport Health Res. 2012, 4, 157–166. [Google Scholar]
- Leal, L.G.; Lopes, M.A.; Batista, M.L.J. Physical Exercise-Induced Myokines and Muscle-Adipose Tissue Crosstalk: A Review of Current Knowledge and the Implications for Health and Metabolic Diseases. Front. Physiol. 2018, 9, 1307. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Tamaki, H.; Hayao, K.; Yotani, K.; Ogita, F.; Yamamoto, N.; Onishi, H. Electrical Stimulation of Denervated Rat Skeletal Muscle Retards Capillary and Muscle Loss in Early Stages of Disuse Atrophy. Biomed Res. Int. 2017, 2017, 5695217. [Google Scholar] [CrossRef] [PubMed]
- Pratesi, A. Skeletal Muscle: An Endocrine Organ. Clin. Cases Miner. Bone Metab. 2013, 10, 11–14. [Google Scholar] [CrossRef]
- Jaoude, J.; Koh, Y. Matrix Metalloproteinases in Exercise and Obesity. Vasc. Health Risk Manag. 2016, 12, 287–295. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Pardo, M.; Casanueva, F.F. Irisin: ‘Fat’ or Artefact. Clin. Endocrinol. 2015, 82, 467–474. [Google Scholar] [CrossRef]
- De Luis, D.; Domingo, J.C.; Izaola, O.; Casanueva, F.F.; Bellido, D.; Sajoux, I. Effect of DHA Supplementation in a Very Low-Calorie Ketogenic Diet in the Treatment of Obesity: A Randomized Clinical Trial. Endocrine 2016, 54, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Moreno, B.; Bellido, D.; Sajoux, I.; Goday, A.; Saavedra, D.; Crujeiras, A.B.; Casanueva, F.F. Comparison of a Very Low-Calorie-Ketogenic Diet with a Standard Low-Calorie Diet in the Treatment of Obesity. Endocrine 2014, 47, 793–805. [Google Scholar] [CrossRef] [PubMed]
- Moreno, B.; Crujeiras, A.B.; Bellido, D.; Sajoux, I.; Casanueva, F.F. Obesity Treatment by Very Low-Calorie-Ketogenic Diet at Two Years: Reduction in Visceral Fat and on the Burden of Disease. Endocrine 2016, 54, 681–690. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Scientific Opinion on the Essential Composition of Total Diet Replacements for Weight Control. EFSA J. 2015, 13, 3957. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Cabia, B.; Carreira, M.C.; Amil, M.; Cueva, J.; Andrade, S.; Seoane, L.M.; Pardo, M.; Sueiro, A.; Baltar, J.; et al. Secreted Factors Derived from Obese Visceral Adipose Tissue Regulate the Expression of Breast Malignant Transformation Genes. Int. J. Obes. 2016, 40, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Lee, Y.J.; Heo, Y.-S.; Park, H.S.; Lee, S.H.; Lee, S.K.; Jang, Y.J. Serum SPARC and Matrix Metalloproteinase-2 and Metalloproteinase-9 Concentrations after Bariatric Surgery in Obese Adults. Obes. Surg. 2014, 24, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Crujeiras, A.B.; Pardo, M.; Arturo, R.-R.; Navas-Carretero, S.; Zulet, M.A.; Martínez, J.A.; Casanueva, F.F. Longitudinal Variation of Circulating Irisin after an Energy Restriction-Induced Weight Loss and Following Weight Regain in Obese Men and Women. Am. J. Hum. Biol. 2014, 26, 198–207. [Google Scholar] [CrossRef]
- Duzova, H.; Gullu, E.; Cicek, G.; Koksal, B.K.; Kayhan, B.; Gullu, A.; Sahin, I. The Effect of Exercise Induced Weight-Loss on Myokines and Adipokines in Overweight Sedentary Females: Steps-Aerobics vs. Jogging-Walking Exercises. J. Sports Med. Phys. Fit. 2018, 58, 295–308. [Google Scholar] [CrossRef]
- Pedersen, B.K. Muscles and Their Myokines. J. Exp. Biol. 2011, 214, 337–346. [Google Scholar] [CrossRef]
- Kim, J.E.; O’Connor, L.E.; Sands, L.P.; Slebodnik, M.B.; Campbell, W.W. Effects of Dietary Protein Intake on Body Composition Changes after Weight Loss in Older Adults: A Systematic Review and Meta-Analysis. Nutr. Rev. 2016, 74, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arbelaez, D.; Crujeiras, A.B.; Castro, A.I.; Martinez-Olmos, M.A.; Canton, A.; Ordoñez-Mayan, L.; Sajoux, I.; Galban, C.; Bellido, D.; Casanueva, F.F. Resting Metabolic Rate of Obese Patients under Very Low Calorie Ketogenic Diet. Nutr. Metab. 2018, 15, 18. [Google Scholar] [CrossRef] [PubMed]
- Crujeiras, A.B.; Gomez-Arbelaez, D.; Zulet, M.A.; Carreira, M.C.; Sajoux, I.; de Luis, D.; Castro, A.I.; Baltar, J.; Baamonde, I.; Sueiro, A.; et al. Plasma FGF21 Levels in Obese Patients Undergoing Energy-Restricted Diets or Bariatric Surgery: A Marker of Metabolic Stress? Int. J. Obes. 2017, 41, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Arvidsson, E.; Viguerie, N.; Andersson, I.; Verdich, C.; Langin, D.; Arner, P. Effects of Different Hypocaloric Diets on Protein Secretion from Adipose Tissue of Obese Women. Diabetes 2004, 53, 1966–1971. [Google Scholar] [CrossRef] [PubMed]
- Crujeiras, A.B.; Parra, D.; Milagro, F.I.; Goyenechea, E.; Larrarte, E.; Margareto, J.; Martínez, J.A. Differential Expression of Oxidative Stress and Inflammation Related Genes in Peripheral Blood Mononuclear Cells in Response to a Low-Calorie Diet: A Nutrigenomics Study. OMICS A J. Integr. Biol. 2008, 12, 251–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouloumié, A.; Sengenès, C.; Portolan, G.; Galitzky, J.; Lafontan, M. Adipocyte Produces Matrix Metalloproteinases 2 and 9: Involvement in Adipose Differentiation. Diabetes 2001, 50, 2080–2086. [Google Scholar] [CrossRef]
- Chavey, C.; Mari, B.; Monthouel, M.-N.; Bonnafous, S.; Anglard, P.; Van Obberghen, E.; Tartare-Deckert, S. Matrix Metalloproteinases Are Differentially Expressed in Adipose Tissue during Obesity and Modulate Adipocyte Differentiation. J. Biol. Chem. 2003, 278, 11888–11896. [Google Scholar] [CrossRef] [Green Version]
- Hopps, E.; Caimi, G. Matrix Metalloproteinases in Metabolic Syndrome. Eur. J. Intern. Med. 2012, 23, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Ress, C.; Tschoner, A.; Ciardi, C.; Laimer, M.W.; Engl, J.W.; Sturm, W.; Weiss, H.; Tilg, H.; Ebenbichler, C.F.; Patsch, J.R.; et al. Influence of Significant Weight Loss on Serum Matrix Metalloproteinase (MMP)-7 Levels. Eur. Cytokine Netw. 2010, 21, 65–70. [Google Scholar] [CrossRef]
- Scheede-Bergdahl, C.; Bergdahl, A.; Schjerling, P.; Qvortrup, K.; Koskinen, S.O.; Dela, F. Exercise-Induced Regulation of Matrix Metalloproteinases in the Skeletal Muscle of Subjects with Type 2 Diabetes. Diabetes Vasc. Dis. Res. 2014, 11, 324–334. [Google Scholar] [CrossRef]
- Perakakis, N.; Triantafyllou, G.A.; Fernández-Real, J.M.; Huh, J.Y.; Park, K.H.; Seufert, J.; Mantzoros, C.S. Physiology and Role of Irisin in Glucose Homeostasis. Nat. Rev. Endocrinol. 2017, 13, 324–337. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.Y.; Panagiotou, G.; Mougios, V.; Brinkoetter, M.; Vamvini, M.T.; Schneider, B.E.; Mantzoros, C.S. FNDC5 and Irisin in Humans: I. Predictors of Circulating Concentrations in Serum and Plasma and II. MRNA Expression and Circulating Concentrations in Response to Weight Loss and Exercise. Metabolism 2012, 61, 1725–1738. [Google Scholar] [CrossRef] [PubMed]
- Roca-Rivada, A.; Castelao, C.; Senin, L.L.; Landrove, M.O.; Baltar, J.; Belén Crujeiras, A.; Seoane, L.M.; Casanueva, F.F.; Pardo, M. FNDC5/Irisin Is Not Only a Myokine but Also an Adipokine. PLoS ONE 2013, 8, 60563. [Google Scholar] [CrossRef] [PubMed]
- Goday, A.; Bellido, D.; Sajoux, I.; Crujeiras, A.B.; Burguera, B.; García-Luna, P.P.; Oleaga, A.; Moreno, B.; Casanueva, F.F. Short-Term Safety, Tolerability and Efficacy of a Very Low-Calorie-Ketogenic Diet Interventional Weight Loss Program versus Hypocaloric Diet in Patients with Type 2 Diabetes Mellitus. Nutr. Diabetes 2016, 6, 230. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arbelaez, D.; Crujeiras, A.B.; Castro, A.I.; Goday, A.; Mas-Lorenzo, A.; Bellon, A.; Tejera, C.; Bellido, D.; Galban, C.; Sajoux, I.; et al. Acid–Base Safety during the Course of a Very Low-Calorie-Ketogenic Diet. Endocrine 2017, 58, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Huang, Q.; Tominaga, T.; Liu, C.; Suzuki, K. An 8-Week Ketogenic Diet Alternated Interleukin-6, Ketolytic and Lipolytic Gene Expression, and Enhanced Exercise Capacity in Mice. Nutrients 2018, 10, 1696. [Google Scholar] [CrossRef]
- Castro, A.I.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Granero, R.; Aguera, Z.; Jimenez-Murcia, S.; Sajoux, I.; Lopez-Jaramillo, P.; Fernandez-Aranda, F.; Casanueva, F.F. Effect of A Very Low-Calorie Ketogenic Diet on Food and Alcohol Cravings, Physical and Sexual Activity, Sleep Disturbances, and Quality of Life in Obese Patients. Nutrients 2018, 10, 1348. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | VLCKD | LCD | Bariatric Surgery | ANOVA p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (0 Months) | Endpoint (2–3 Months) | Follow-up (4–6 Months) | Baseline (0 Months) | Endpoint (2–3 Months) | Follow-up (4–6 Months) | Baseline (0 Months) | Endpoint (2–3 Months) | Follow-up (4–6 Months) | Time | Study | Time × Study | |
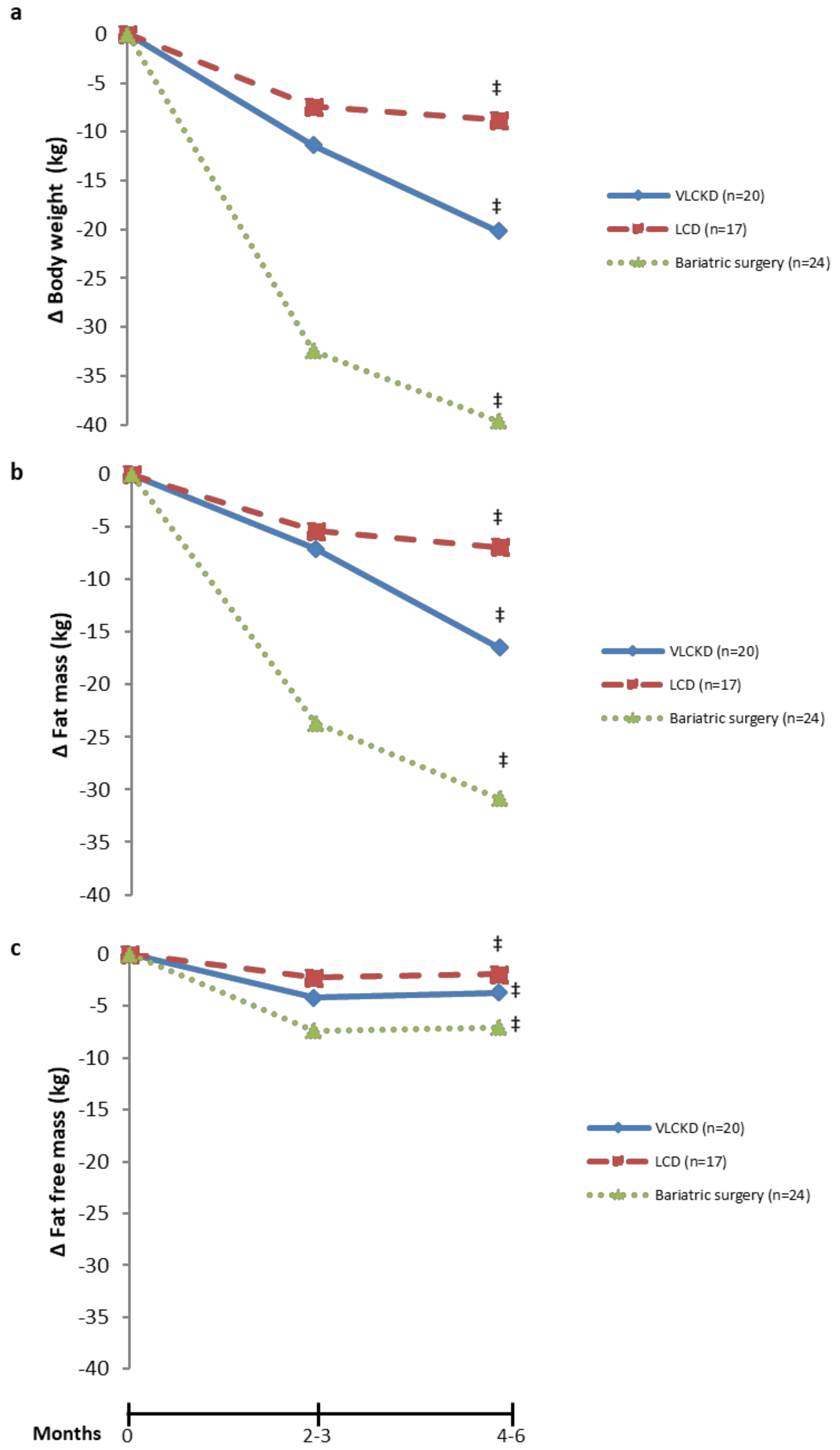
| Body weight (kg) | 96.0 ± 16.3 | 84.2 ± 13.0 ‡ | 76.6 ± 11.1 ‡,†,* | 93.0 ± 13.2 | 89.0 ± 12.5 ‡ | 87.6 ± 12.3 ‡,†,* | 121.3 ± 21.5 | 88.9 ± 13.4 ‡ | 81.7 ± 14.3 ‡,†,* | <0.001 | <0.001 | <0.001 |
| Fat mass (kg) | 42.2 ± 9.2 | 35.0 ± 7.8 ‡ | 25.7 ± 5.8 ‡,†,* | 34.6 ± 8.3 | 31.4 ± 7.6 ‡ | 30.7 ± 7.6 ‡,†,* | 62.57 ± 14.9 | 38.9 ± 7.1 ‡ | 31.7 ± 8.2 ‡,†,* | <0.001 | 0.012 | <0.001 |
| Fat free mass (kg) | 52.8 ± 10.3 | 48.6 ± 9.3 ‡ | 49.1 ± 9.7 ‡,* | 58.3 ± 11.7 | 57.6 ± 11.6 ‡ | 56.9 ± 11.2 ‡,†,* | 56.7 ± 9.9 | 49.3 ± 9.6 ‡ | 49.6 ± 8.5 ‡,* | <0.001 | 0.002 | <0.001 |
| β-OHB (mmol/L) | 0.3 ± 0.02 | 1.34 ± 0.13 ‡ | 0.24 ± 0.18 ‡,†,* | 0.39 ± 0.01 | 0.38 ± 0.02 | 0.38 ± 0.01 | 0.45 ± 0.26 | 0.51 ± 0.29 ‡ | 0.44 ± 0.30 | <0.001 | 0.942 | <0.001 |
| HOMA-IR | 4.43 ± 2.37 | 1.53 ± 0.47 ‡ | 1.71 ± 0.57 ‡,* | 3.28 ± 1.54 | 1.65 ± 0.93 ‡ | 1.98 ± 2.31 ‡,* | 5.21 ± 2.86 | 2.52 ± 1.18 ‡ | 2.10 ± 1.24 ‡,†,* | <0.001 | 0.029 | 0.055 |
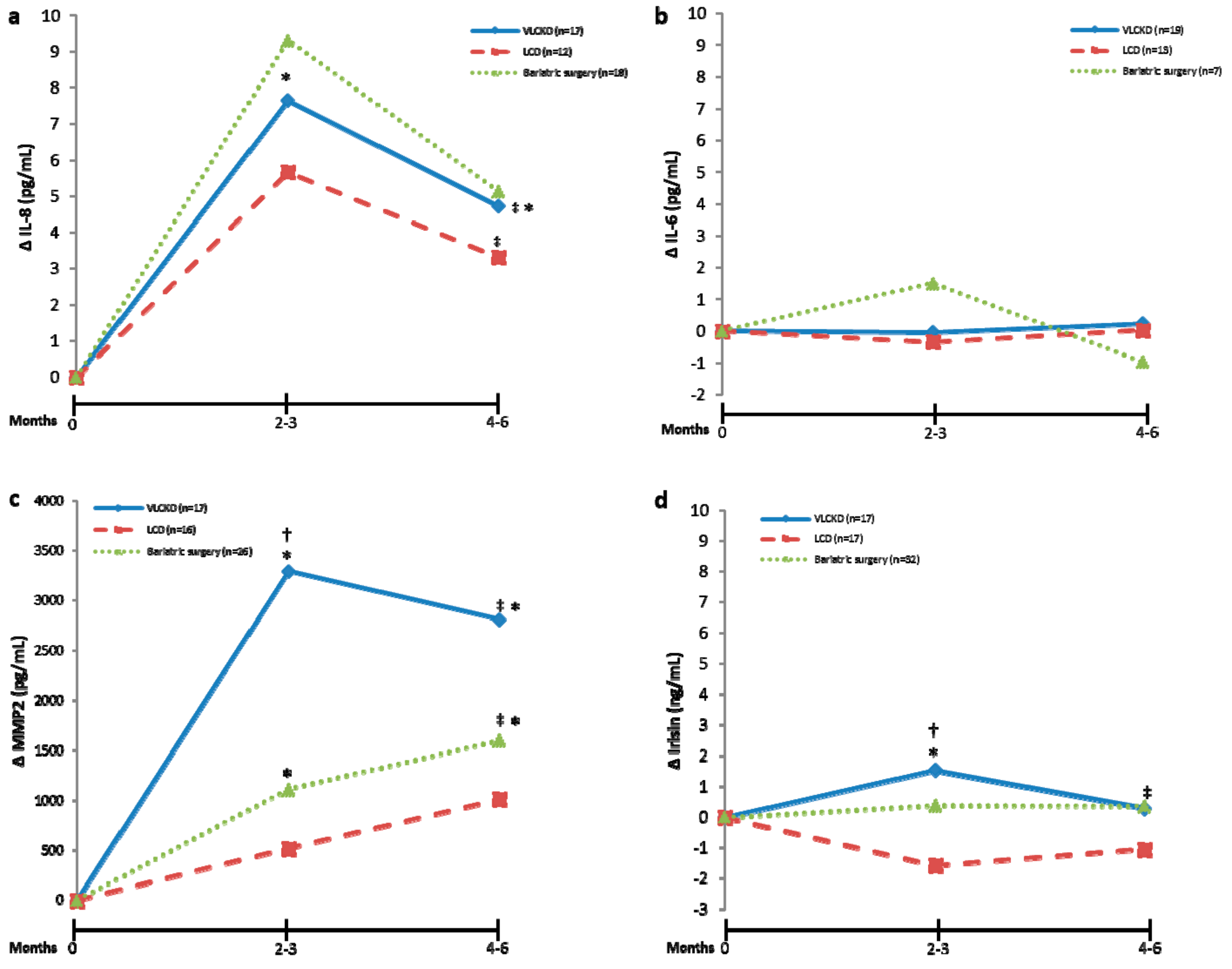
| IL-8 (pg/mL) | 27.5 ± 8.7 | 35.1 ± 12.7 ‡ | 32.2 ± 8.8 ‡,* | 22.0 ± 7.5 | 27.7 ± 7.7 | 25.3 ± 4.4 * | 34.2 ± 17.8 | 44.1 ± 26.6 | 39.8 ± 20.3 | 0.001 | 0.028 | 0.758 |
| MMP2 (pg/mL) | 7782 ± 6637 | 11074 ± 11542 ‡ | 10590 ± 11878 ‡,* | 6782 ± 6524 | 7301 ± 7113 | 7793 ± 7455 | 3700 ± 4077 | 4813 ± 5527 ‡ | 5300 ± 5654 ‡,* | 0.001 | 0.072 | 0.421 |
| IL-6 (pg/mL) | 3.96 ± 3.02 | 3.92 ± 3.24 | 4.19 ± 6.33 | 2.62 ± 1.35 | 2.27 ± 0.83 | 2.65 ± 1.68 | 3.26 ± 1.10 | 4.77 ± 2.52 | 2.30 ± 0.51 | 0.796 | 0.081 | 0.872 |
| Irisin (ng/mL) | 13.4 ± 3.3 | 14.9 ± 2.6 ‡ | 13.7 ± 3.2 * | 11.9 ± 6.6 | 10.4 ± 4.7 | 11.4 ± 7.5 | 10.6 ± 2.8 | 10.9 ± 2.8 | 11.3 ± 2.9 | 0.869 | 0.009 | 0.043 |
| ΔIL-8_Endpoint | ΔIL-8_Follow-Up | ΔMMP2_Endpoint | ΔMMP2_Follow-Up | ΔIL-6_Endpoint | ΔIL-6_Follow-up | ΔIrisin_Endpoint | ΔIrisin_Follow-Up | ||
|---|---|---|---|---|---|---|---|---|---|
| ΔBW_ Endpoint | R | 0.237 | 0.18 | −0.309 | −0.296 | 0.057 | 0.326 | −0.454 | 0.281 |
| p-value | 0.395 | 0.522 | 0.262 | 0.285 | 0.841 | 0.236 | 0.089 | 0.31 | |
| ΔBW_ Follow-up | R | 0.196 | 0.194 | −0.33 | −0.333 | −0.032 | 0.128 | −0.304 | 0.224 |
| p-value | 0.483 | 0.488 | 0.23 | 0.225 | 0.909 | 0.648 | 0.271 | 0.423 | |
| ΔFM_ Endpoint | R | −0.195 | −0.217 | −0.526 | −0.409 | −0.104 | 0.362 | −0.286 | 0.208 |
| p-value | 0.486 | 0.437 | 0.044 | 0.13 | 0.713 | 0.185 | 0.301 | 0.457 | |
| ΔFM_Follow-up | R | −0.082 | −0.052 | −0.415 | −0.389 | −0.03 | 0.088 | −0.161 | 0.125 |
| p-value | 0.772 | 0.854 | 0.124 | 0.152 | 0.915 | 0.755 | 0.566 | 0.656 | |
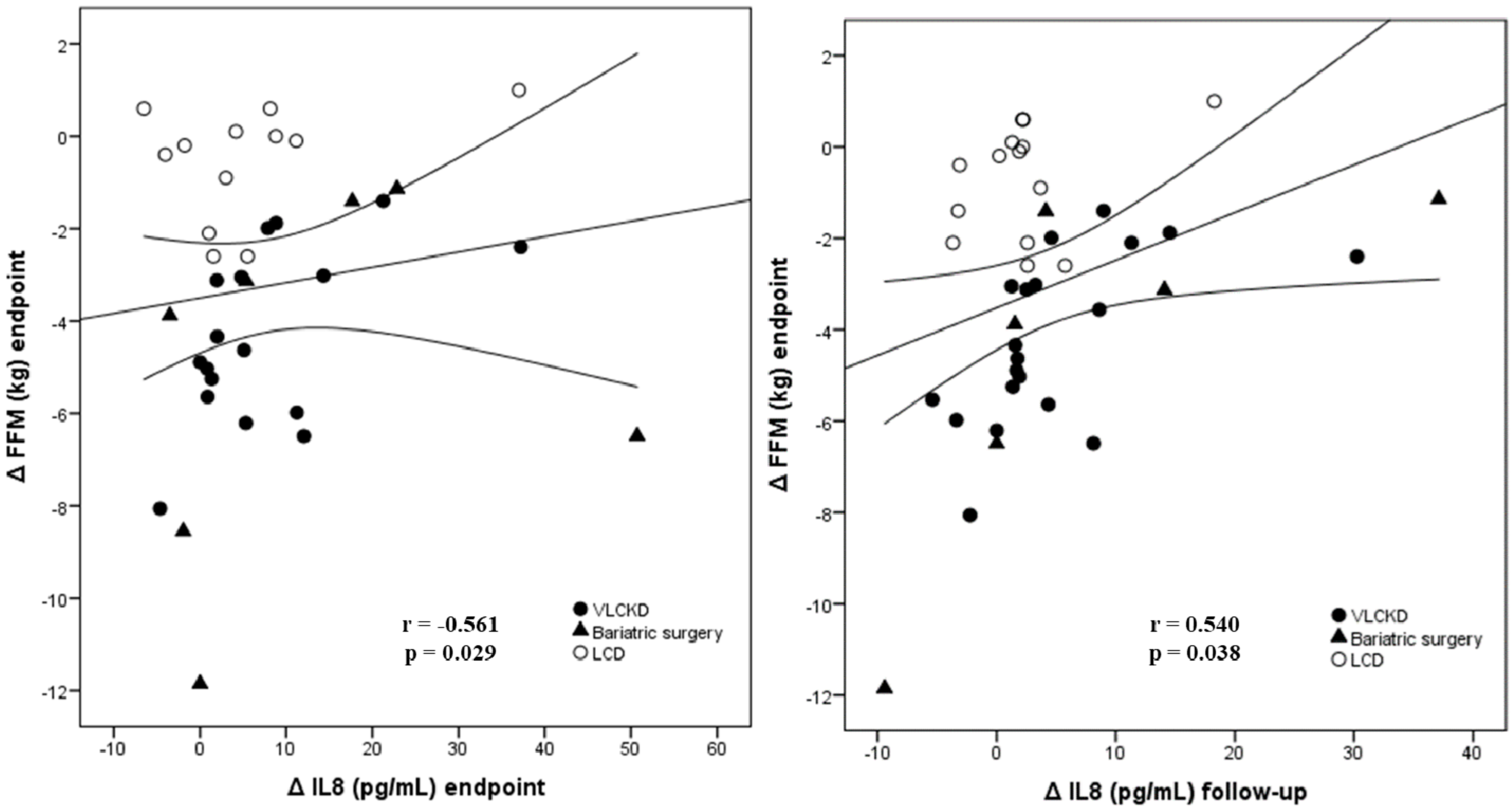
| ΔFFM_ Endpoint | R | 0.561 | 0.54 | −0.073 | −0.172 | 0.228 | 0.161 | −0.324 | 0.362 |
| p-value | 0.029 | 0.038 | 0.797 | 0.539 | 0.413 | 0.566 | 0.239 | 0.185 | |
| ΔFFM_ Follow-up | R | 0.443 | 0.414 | −0.074 | −0.237 | 0.113 | 0.039 | −0.25 | 0.3 |
| p-value | 0.098 | 0.125 | 0.793 | 0.396 | 0.688 | 0.889 | 0.369 | 0.278 | |
| ΔβOHB_ Endpoint | R | −0.105 | 0.05 | −0.249 | −0.084 | −0.151 | −0.024 | −0.103 | −0.458 |
| p-value | 0.71 | 0.86 | 0.371 | 0.766 | 0.591 | 0.933 | 0.714 | 0.086 | |
| ΔβOHB_ Follow-up | R | 0.193 | 0.228 | −0.031 | 0.075 | 0.045 | 0.342 | −0.423 | −0.305 |
| p-value | 0.491 | 0.414 | 0.911 | 0.79 | 0.873 | 0.212 | 0.116 | 0.269 | |
| ΔHOMA-IR_ Endpoint | R | 0.557 | 0.502 | 0.121 | 0.153 | 0.195 | 0.078 | −0.438 | −0.146 |
| p-value | 0.031 | 0.057 | 0.667 | 0.586 | 0.486 | 0.782 | 0.103 | 0.602 | |
| ΔHOMA-IR_ Follow-up | R | 0.573 | 0.586 | 0.152 | 0.184 | 0.247 | −0.039 | −0.378 | −0.295 |
| p-value | 0.026 | 0.022 | 0.589 | 0.511 | 0.376 | 0.889 | 0.165 | 0.285 |
| Standardized Coefficients β (95% CI) | P-Value | |
|---|---|---|
| Model 1 ΔFFM_endpoint | ||
| ΔIL-8 | 0.869 (0.09; 0.28) | 0.001 |
| ΔIL-6 | 0.248 (−0.06; 0.25) | 0.195 |
| ΔMMP2_ | −0.535 (0.00; 0.00) | 0.026 |
| ΔIrisin | 0.001 (−0.28; 0.28) | 0.996 |
| Corrected R2 = 0.507 | 0.008 | |
| Model 2 ΔFFM_endpoint | ||
| ΔIL-8 | 0.868 (0.09; 0.27) | 0.001 |
| ΔIL-6 | 0.248 (−0.05; 0.25) | 0.171 |
| ΔMMP2 | −0.535 (0.00; 0.00) | 0.018 |
| Corrected R2 = 0.540 | 0.003 | |
| Model 3 ΔFFM_follow-up | ||
| ΔIL-8 | 0.337 (−0.04; 0.18) | 0.180 |
| ΔIL-6 | 0.159 (−0.14; 0.25) | 0.575 |
| ΔMMP2_ | −0.081 (0.00; 0.00) | 0.771 |
| ΔIrisin | 0.020 (−0.29; 0.30) | 0.947 |
| Corrected R2 = −0.019 | 0.494 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sajoux, I.; Lorenzo, P.M.; Gomez-Arbelaez, D.; Zulet, M.A.; Abete, I.; Castro, A.I.; Baltar, J.; Portillo, M.P.; Tinahones, F.J.; Martinez, J.A.; et al. Effect of a Very-Low-Calorie Ketogenic Diet on Circulating Myokine Levels Compared with the Effect of Bariatric Surgery or a Low-Calorie Diet in Patients with Obesity. Nutrients 2019, 11, 2368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102368
Sajoux I, Lorenzo PM, Gomez-Arbelaez D, Zulet MA, Abete I, Castro AI, Baltar J, Portillo MP, Tinahones FJ, Martinez JA, et al. Effect of a Very-Low-Calorie Ketogenic Diet on Circulating Myokine Levels Compared with the Effect of Bariatric Surgery or a Low-Calorie Diet in Patients with Obesity. Nutrients. 2019; 11(10):2368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102368
Chicago/Turabian StyleSajoux, Ignacio, Paula M. Lorenzo, Diego Gomez-Arbelaez, M. Angeles Zulet, Itziar Abete, Ana I. Castro, Javier Baltar, María P. Portillo, Francisco J. Tinahones, J. Alfredo Martinez, and et al. 2019. "Effect of a Very-Low-Calorie Ketogenic Diet on Circulating Myokine Levels Compared with the Effect of Bariatric Surgery or a Low-Calorie Diet in Patients with Obesity" Nutrients 11, no. 10: 2368. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102368