Endemic Goiter and Iodine Prophylaxis in Calabria, a Region of Southern Italy: Past and Present

 , , ,
, , ,
Abstract
:1. Introduction
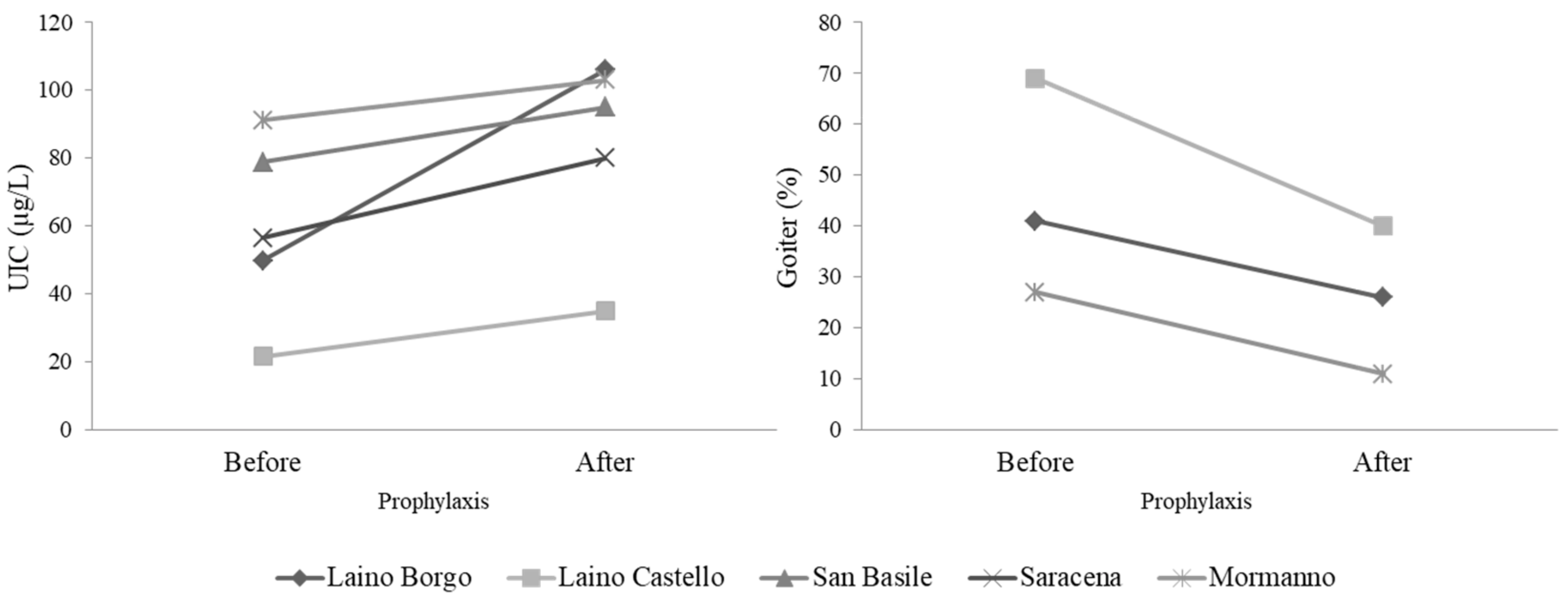
2. History of Goiter and Iodine Deficiency in Calabria: Epidemiological Surveys during the 1980–2000 Period
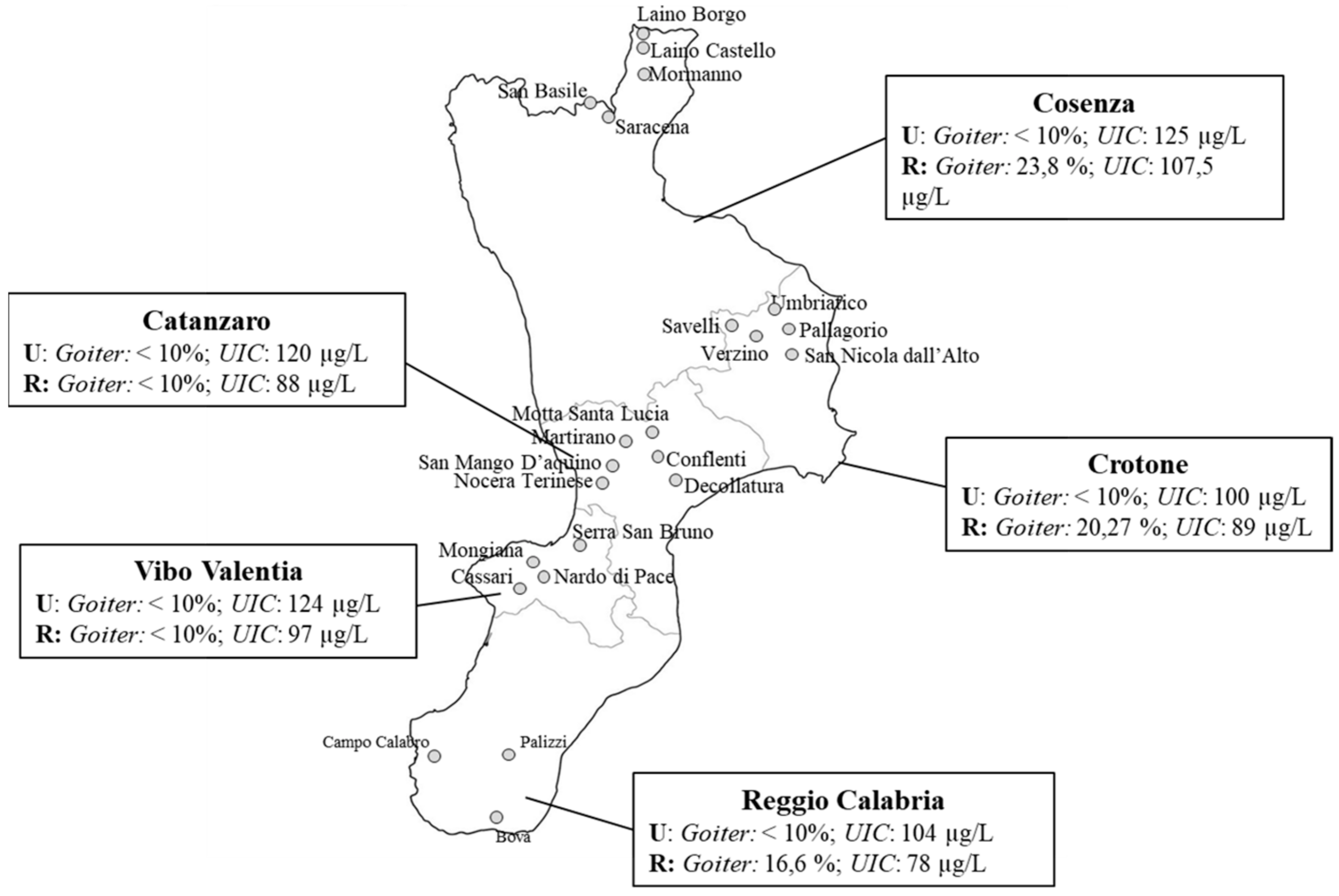
3. Status of Iodine Intake Over the Last Two Decades in the Calabria Region: The Epidemiological Observatory for Endemic Goiter and Iodine Prophylaxis
3.1. Epidemiological Surveys
3.2. Promotional Campaign
3.3. Sale Trend of Iodized Salt
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, M.; Eastman, C.J. The changing epidemiology of iodine deficiency. Nat. Rev. Endocrinol. 2012, 8, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, M.; Azizi, F.; Hedayati, M. Iodine deficiency status in the WHO Eastern Mediterranean Region: A systematic review. Environ. Geochem. Health 2018, 40, 87–97. [Google Scholar] [CrossRef] [PubMed]
- The Iodine Global Network: 2018 Annual Report. Available online: https://www.ign.org/cm_data/IGN_2018_Annual_Report_5_web.pdf (accessed on 5 September 2019).
- Zimmermann, M.B. The role of iodine in human growth and development. Semin Cell Dev. Biol. 2011, 22, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Eastman, C.J.; Zimmermann, M.B. The iodine deficiency disorders. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK285556/ (accessed on 5 September 2019).
- Morreale de Escobar, G.; Obregon, M.J.; Escobar del Rey, F. Role of thyroid hormone during early brain development. Eur. J. Endocrinol. 2004, 151 (Suppl. 3), U25–U37. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Urinary iodine concentrations for determining iodine status in populations. Available online: https://apps.who.int/iris/bitstream/handle/10665/85972/WHO_NMH_NHD_EPG_13.1_eng.pdf (accessed on 5 September 2019).
- Zimmermann, M.B.; Hess, S.Y.; Molinari, L.; De Benoist, B.; Delange, F.; Braverman, L.E.; Fujieda, K.; Ito, Y.; Jooste, P.L.; Moosa, K.; et al. New reference values for thyroid volumen by ultrasound in iodine-sufficient school children: A World Health Organization/Nutrition for Health and Development Iodine Deficiency Study Group Report. Am. J. Nutr. 2004, 79, 231–237. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization/International Council for the Control of the Iodine Deficiency Disorders/United Nations Children’s Fund (WHO/ICCIDD/UNICEF). Assessment of the Iodine Deficiency Disorders and Monitoring Their Elimination; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Zimmermann, M.B.; de Benoist, B.; Corigliano, S.; Jooste, P.L.; Molinari, L.; Moosa, K.; Pretell, E.A.; Al-Dallal, Z.S.; Wei, Y.; Zu-Pei, C.; et al. Assessment of iodine status using dried blood spot thyroglobulin: Development of reference material and establishment of an international reference range in iodine-sufficient children. J. Clin. Endocrinol. Metab. 2006, 91, 4881–4887. [Google Scholar] [CrossRef] [PubMed]
- Principles of Nutritional Assessment; Gibson, R. (Ed.) Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Institute of Medicine. Academy of Sciences 2001 Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Eastman, C.J. Screening for thyroid disease and iodine deficiency. Pathology 2012, 44, 153–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farebrother, J.; Zimmermann, M.B.; Assey, V.; Castro, M.C.; Cherkaoui, M.; Fingerhut, R.; Jia, Q.; Jukic, T.; Makokha, A.; San Luis, T.O.; et al. Thyroglobulin is markedly elevated in 6- to 24-month-old infants at both low and high iodine intakes and suggests a narrow optimal iodine intake range. Thyroid 2019, 29, 268–277. [Google Scholar] [CrossRef]
- World Health Organization/International Council for the Control of the Iodine Deficiency Disorders/United Nations Children’s Fund (WHO/ICCIDD/UNICEF). Assessment of the Iodine Deficiency Disorders and Monitoring Their Elimination; WHO/NHD/01.1; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Guideline: Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; World Health Organization: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/136908 (accessed on 5 September 2019).
- Rasmussen, L.B.; Carlé, A.; Jørgensen, T.; Knudsen, N.; Laurberg, P.; Pedersen, I.B.; Perrild, H.; Vejbjerg, P.; Ovesen, L. Iodine intake before and after mandatory iodization in Denmark: Results from the Danish Investigation of Iodine Intake and Thyroid Diseases (DanThyr) study. Br. J. Nutr. 2008, 100, 166–173. [Google Scholar] [CrossRef]
- Charlton, K.E.; Yeatman, H.; Brock, E.; Lucas, C.; Gemming, L.; Goodfellow, A.; Ma, G. Improvement in iodine status of pregnant Australian women 3 years after introduction of a mandatory iodine fortification programme. Prev. Med. 2013, 57, 26–30. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Aeberli, I.; Torresani, T.; Bürgi, H. Increasing the iodine concentration in the Swiss iodized salt program markedly improved iodine status in pregnant women and children: A 5-y prospective national study. Am. J. Clin. Nutr. 2005, 82, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Family Welfare. Government of India & International Institute of Population Sciences (2007) National Family Health Survey-3 National Report (2005–06). Available online: http://rchiips.org/nfhs/nfhs3_national_report.shtml (accessed on 2 October 2019).
- Pandav, C.S.; Yadav, K.; Srivastava, R.; Pandav, R.; Karmarkar, M.G. Iodine deficiency disorders (IDD) control in India. Indian J. Med. Res. 2013, 138, 418–433. [Google Scholar] [PubMed]
- Pandav, C.S.; Yadav, K.; Salve, H.R.; Kumar, R.; Goel, A.D.; Chakrabarty, A. High national and sub-national coverage of iodised salt in India: Evidence from the first National Iodine and Salt Intake Survey (NISI) 2014–2015. Public Health Nutr. 2018, 21, 3027–3036. [Google Scholar] [CrossRef] [PubMed]
- Randremanana, R.V.; Bastaraud, A.; Rabarijaona, L.P.; Piola, P.; Rakotonirina, D.; Razafinimanana, J.O.; Ramangakoto, M.H.; Andriantsarafara, L.; Randriamasiarijaona, H.; Tucker-Brown, A.; et al. First national iodine survey in Madagascar demonstrates iodine deficiency. Matern. Child. Nutr. 2019, 15, e12717. [Google Scholar] [CrossRef] [PubMed]
- Chuko, T.; Bagriansky, J.; Brown, A.T. Ethiopia’s long road to USI. IDD Newsl. 2015, 43. Available online: https://www.ign.org/cm_data/IDD_may15_1.pdf (accessed on 2 October 2019).
- IFPRI. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030; International Food Policy Research Institute: Washington, DC, USA, 2016; p. 182. Available online: http://www.ifpri.org/publication/global-nutrition-report-2016-promise-impact-ending-malnutrition-2030 (accessed on 2 October 2019).
- OSNAMI—Istituto Superiore di Sanità. Osservatorio Nazionale per il Monitoraggio della Iodoprofilassi in Italia. Available online: http://old.iss.it/osnami/index.php?lang=1 (accessed on 5 September 2019).
- Pellicone, G.; Caloiero, T.; Coletta, V.; Veltri, A. Phytoclimatic map of Calabria (Southern Italy). J. Maps 2014, 10, 109–113. [Google Scholar] [CrossRef]
- Stanbury, J.B.; Ermans, A.M.; Hetzel, B.S.; Pretell, E.A.; Querido, A. Endemic goitre and cretinism: Public health significance and prevention. WHO Chron. 1974, 28, 220–228. [Google Scholar]
- Andò, S.; Maggiolini, M.; Di Carlo, A.; Diodato, A.; Bloise, A.; De Luca, G.P.; Pezzi, V.; Sisci, D.; Mariano, A.; Macchia, V. Endemic goiter in Calabria: Etiopathogenesis and thyroid function. J. Endocrinol. Investig. 1994, 17, 329–333. [Google Scholar] [CrossRef]
- Costante, G.; Grasso, L.; Schifino, E.; Marasco, M.F.; Crocetti, U.; Capula, C.; Chiarella, R.; Ludovico, O.; Nocera, M.; Parlato, G.; et al. Iodine deficiency in Calabria: Characterization of endemic goiter and analysis of different indicators of iodine status region-wide. J. Endocrinol. Investig. 2002, 25, 201–207. [Google Scholar] [CrossRef]
- Aghini-Lombardi, F.; Antonangeli, L.; Vitti, P.; Pinchera, A. Status of iodine nutrition in Italy. In Iodine Deficiency in Europe; Delange, F., Dunn, J.T., Glinoer, D., Eds.; A continuing concern; Plenum Press: New York, NY, USA, 1993; pp. 403–408. [Google Scholar]
- Aghini-Lombardi, F.; Vitti, P.; Antonangeli, L.; Fiore, E.; Piaggi, P.; Pallara, A.; Consiglio, E.; Pinchera, A. Southern Italy Study Group for Iodine Deficiency Disorders. The size of the community rather than its geographical location better defines the risk of iodine deficiency: Results of an extensive survey in Southern Italy. J. Endocrinol. Investig. 2013, 36, 282–286. [Google Scholar] [CrossRef]
- Mazzarella, C.; Terracciano, D.; Di Carlo, A.; Macchia, P.E.; Consiglio, E.; Macchia, V.; Mariano, A. Iodine status assessment in Campania (Italy) as determined by urinary iodine excretion. Nutrition 2009, 25, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Bonofiglio, D.; Catalano, S.; Perri, A.; Baldini, M.P.; Marsico, S.; Tagarelli, A.; Conforti, D.; Guido, R.; Andò, S. Beneficial effects of iodized salt prophylaxis on thyroid volume in an iodine deficient area of southern Italy. Clin. Endocrinol. 2009, 71, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, A.; Di Cosmo, C.; De Angelis, S.; Da Cas, R.; Stacchini, P.; Pastorelli, A.; Vitti, P. Regional Observatories for Goiter Prevention. The way forward in Italy for iodine. Minerva. Med. 2017, 108, 159–168. [Google Scholar] [PubMed]
- Bonofiglio, D.; Catalano, S.; Perri, A.; Santoro, M.; Siciliano, L.; Lofaro, D.; Gallo, M.; Marsico, S.; Bruno, R.; Giordano, C.; et al. Monitoring the effects of iodine prophylaxis in the adult population of southern Italy with deficient and sufficient iodine intake levels: A cross-sectional, epidemiological study. Br. J. Nutr. 2017, 117, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Tomer, Y. Anti-thyroglobulin autoantibodies in autoimmune thyroid disease: Cross-reactive or pathogenic? Clin. Immunol. Immunopathol. 1997, 82, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.R.; Hamidi, S.; Braley-Mullen, H.; Nagayama, Y.; Bresee, C.; Aliesky, H.A.; Rapoport, B.; McLachlan, S.M. Antibodies to thyroid peroxidase arise spontaneously with age in NOD. H-2h4 mice and appear after thyroglobulin antibodies. Endocrinology 2010, 151, 4583–4593. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, A.; De Angelis, S.; Rotondi, D.; Pastorelli, A.; Stacchini, P.; Da Cas, R.; Medda, E. The Regional Observatories for Goiter Prevention. Attività di monitoraggio del programma nazionale per la prevenzione dei disordini da carenza iodica: La situazione italiana a 14 anni dall’approvazione della Legge 55/2005. L’Endocrinologo. 2019, 20, 245–248. [Google Scholar] [CrossRef]
- Osservatorio Epidemiologico e Promozione della Salute. “Sezione Gozzo Endemico e Iodoprofilassi”, Regione Calabria, Italy. Available online: http://oer.unical.it/ (accessed on 5 September 2019).




{kind=link}
{kind=link}
{kind=link}
| Provinces | Samples (n) | UIC Mean (±SD) μg/L | UIC Median μg/L |
|---|---|---|---|
| Catanzaro | 1024 | 85 ± 71 | 65 |
| Cosenza | 701 | 91 ± 71 | 73 |
| Crotone | 257 | 84 ± 78 | 54 |
| Reggio Calabria | 346 | 91 ± 69 | 75 |
| Vibo Valentia | 365 | 83 ± 64 | 67 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giordano, C.; Barone, I.; Marsico, S.; Bruno, R.; Bonofiglio, D.; Catalano, S.; Andò, S. Endemic Goiter and Iodine Prophylaxis in Calabria, a Region of Southern Italy: Past and Present. Nutrients 2019, 11, 2428. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102428
Giordano C, Barone I, Marsico S, Bruno R, Bonofiglio D, Catalano S, Andò S. Endemic Goiter and Iodine Prophylaxis in Calabria, a Region of Southern Italy: Past and Present. Nutrients. 2019; 11(10):2428. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102428
Chicago/Turabian StyleGiordano, Cinzia, Ines Barone, Stefania Marsico, Rosalinda Bruno, Daniela Bonofiglio, Stefania Catalano, and Sebastiano Andò. 2019. "Endemic Goiter and Iodine Prophylaxis in Calabria, a Region of Southern Italy: Past and Present" Nutrients 11, no. 10: 2428. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102428