Eating Healthy, Growing Healthy: Outcome Evaluation of the Nutrition Education Program Optimizing the Nutritional Value of Preschool Menus, Poland


Abstract
:1. Introduction
2. Materials and Methods
2.1. General Information
2.2. Ethical Approval
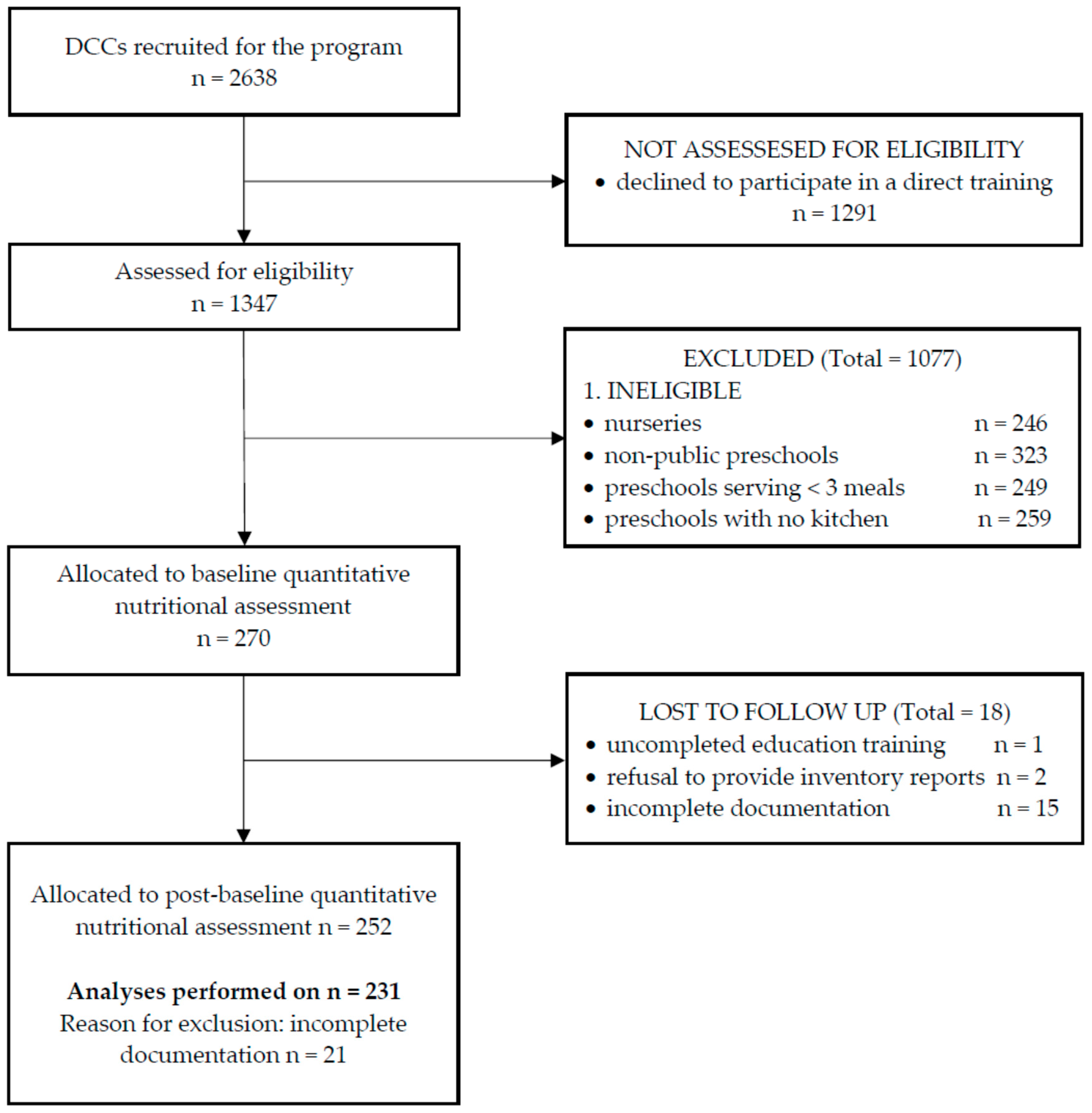
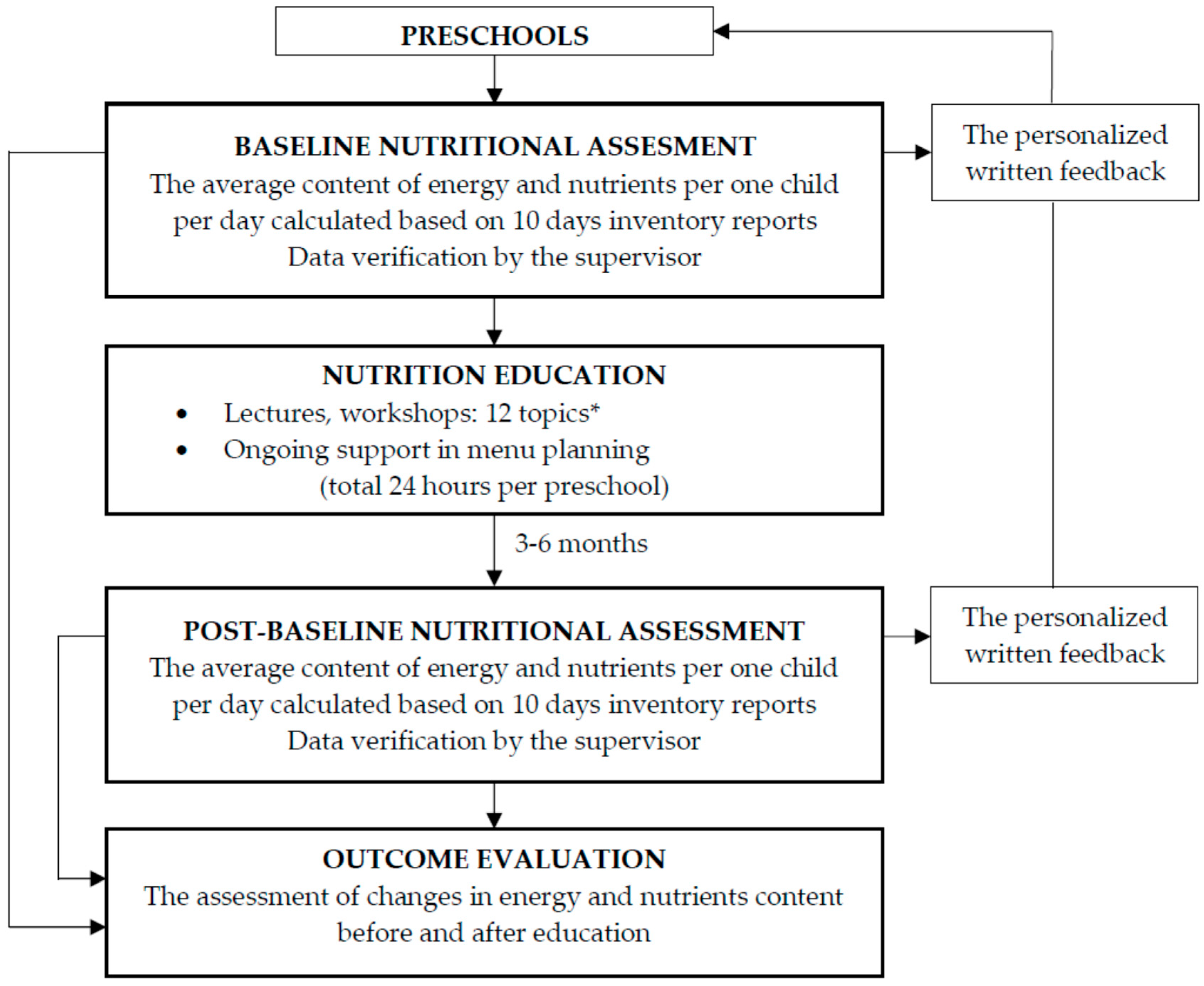
2.3. Study Participants and Design
2.4. Nutritional Analyses of Preschools Menus
2.5. Statistical Analysis
3. Results
3.1. General Characteristic of Preschools
3.2. Energy and Nutrients Content of Prechools Menus
3.3. Vitamins and Minerals Density of Prechools Menus
3.4. Nutrients Important for the Diet Quality
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dev, D.A.; McBride, B.A. Academy of nutrition and dietetics benchmarks for nutrition in child care 2011: Are child-care providers across contexts meeting recommendations? J. Acad. Nutr. Diet. 2013, 113, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Charzewska, J. (Ed.) Recommendations for Nutritionists on the Principles of Proper Nutrition for Children in Kindergartens; IZZ: Warsaw, Poland, 2011. (In Polish) [Google Scholar]
- Ball, S.C.; Benjamin, S.E.; Ward, D.S. Dietary intakes in North Carolina child-care centers: Are children meeting current recommendations? J. Am. Diet. Assoc. 2008, 108, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Central Statistical Office. Education in 2016/2017 School Year. Available online: http://stat.gov.pl/en/topics/education/education/education-in-the-school-year-20152016,1,12.html (accessed on 20 August 2019).
- Yoong, S.L.; Skelton, E.; Jones, J.; Wolfenden, L. Do childcare services provide foods in line with the 2013 Australian Dietary guidelines? A cross-sectional study. Aust. N. Z. J. Public Health 2014, 38, 595–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maalouf, J.; Evers, S.C.; Griffin, M. Assessment of meal time environments and nutrition practices in child care centers in Georgia. Child. Obes. 2013, 9, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Seiquer, I.; Haro, A.; Cabrera-Vique, C.; Munoz-Hoyos, A.; Galdó, G. Nutritional assessment of the menus served in municipal nursery schools in Granada. An. Pediatr. 2016, 85, 197–203. [Google Scholar] [CrossRef]
- Libera, J.; Banach, K.; Latoch, A. Assessment of nutritional quality of food rations in nurseries on the basis of menus during winter season. Żywn Nauka Technol Jakość 2018, 25, 128–138. (in Polish). [Google Scholar] [CrossRef]
- Orkusz, A.; Włodarczyk, A. Assessment of preschool children’s decades menus. Nauki Inż. Technol. 2014, 1, 72–81. (In Polish) [Google Scholar]
- Orkusz, A.; Olech, A. Evaluation of the nutritional value of nursery school meals. Nauki Inż. Technol. 2014, 2, 77–87. (In Polish) [Google Scholar]
- Myszkowska-Ryciak, J.; Harton, A. Implementation of Dietary Reference Intake Standards in Preschool Menus in Poland. Nutrients 2018, 10, 592. [Google Scholar] [CrossRef]
- Merkiel, S.; Chalcarz, W. Preschool diets in children from Piła, Poland, require urgent intervention as implied by high risk of nutrient inadequacies. J. Health Popul. Nutr. 2016, 35, 11. [Google Scholar] [CrossRef]
- Jarosz, M. Human Nutrition Recommendations for Polish Population; IZZ: Warsaw, Poland, 2017. (In Polish) [Google Scholar]
- Regulation of the Minister of Health of 26 July 2016 on Groups of Foodstuffs Intended for Sale to Children and Adolescents in Units of the Education System and the Requirements That Must Be Met by Food Products Used in the Context of Mass Catering for Children and Adolescents in These Units. Dz. U. Poz. 1154. Available online: http://dziennikustaw.gov.pl/du/2016/1154/1 (accessed on 20 August 2019). (In Polish)
- Regulation of the Council of Ministers of 18 March 2009 on the Remuneration of Local Government Employees. Annex 3. Dz. U. 2014 Poz. 1786. Available online: https://www.experto24.pl/oswiata/stosunek-pracy/intendent-wyksztalcenie-srednie-lub-zasadnicze-zawodowe.html?cid=K000KN (accessed on 20 August 2019). (In Polish).
- Stankiewicz, J.; Bogdańska, K. Assessment of the extent of nutritional awareness among kindergarten employees in terms of proper nutrition of preschool children. Probl. Hig. Epidemiol. 2013, 94, 479–483. [Google Scholar]
- Chalcarz, W.; Hodyr, Z.; Drabikowska-Śrama, A. Nutritional knowledge of kindergarten employees. Nowa Medycyna 1999, 7, 62–67. [Google Scholar]
- Harton, A. Poziom Wiedzy Żywieniowej Nauczycieli i Rodziców Dzieci w Wieku 3-6 Lat Jako Podstawa do Opracowania Modelu Edukacji Żywieniowej; Wyd. SGGW: Warsaw, Poland, 2019. (in Polish) [Google Scholar]
- Ward, D.S.; Vaughn, A.; Story, M. Expert and stakeholder consensus on priorities for obesity prevention research in early care and education settings. Child Obes. 2013, 9, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.K.; Hendrie, G.A.; Hartley, J.; Golley, R.K. Impact of a nutrition award scheme on the food and nutrient intakes of 2- to 4-year-olds attending long day care. Public Health Nutr. 2015, 18, 2634–2642. [Google Scholar] [CrossRef] [Green Version]
- Kozioł-Kozakowska, A.; Piórecka, B.; Schlegel-Zawadzka, M. Nutritional education program for kindergarten children and their parents caring out in Cracaw. Stud. Med. 2008, 11, 65–69. [Google Scholar]
- Namenek Brouwer, R.J.N.; Neelon, S.E.B. Watch Me Grow. A garden-based pilot intervention to increase vegetable and fruit intake in preschoolers. BMC Public Health 2013, 13, 363. [Google Scholar] [CrossRef]
- Zalewska, M.; Jamiołkowski, J.; Genowska, A.; Białokoz-Kalinowska, I.; Daszuta-Zalewska, A.; Maciorkowska, E. Change in Knowledge of Kindergarten Employees Participating in the Course “Diet full of life” in the Field of Children’s Nutrition, as Assessed by Generalized Estimating Equations. Stud. Log. Gramm. Rhetor. 2016, 47, 113–128. [Google Scholar] [CrossRef]
- Myszkowska-Ryciak, J.; Harton, A. Education on healthy eating improved nutrition-related practices in Polish preschools. Health Prob. Civil. 2018, 12, 238–246. [Google Scholar] [CrossRef]
- Story, M.; Kaphingst, K.M.; French, S. The Role of Child Care Settings in Obesity Prevention. Fut. Child. 2006, 16, 143–168. [Google Scholar] [CrossRef]
- Ritchie, L.; Boyle, M.; Chandran, K.; Spector, P.; Whaley, S.E.; James, P.; Samuels, S.; Hecht, K.; Crawford, P. Participation in the Child and Adult Care Food Program is associated with more nutritious foods and beverages in child care. Child Obes. 2012, 8, 224–229. [Google Scholar] [CrossRef]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Peñalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 29, e0194555. [Google Scholar] [CrossRef] [PubMed]
- Nathan, N.; Janssen, L.; Sutherland, R.; Hodder, R.K.; Evans, C.L.E.; Booth, D.; Yoong, S.L.; Reilly, K.; Finch, M.; Wolfenden, L. The effectiveness of lunchbox interventions on improving the foods and beverages packed and consumed by children at centre-based care or school: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Hodder, R.; Stacey, F.G.; O’Brien, K.M.; Wyse, R.J.; Clinton-McHarg, T.; Tzelepis, F.; James, E.L.; Bartlem, K.M.; Nathan, N.K.; Sutherland, R.; et al. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane Datab. Syst. Rev. 2018, 25, CD008552. [Google Scholar] [CrossRef]
- Myszkowska-Ryciak, J.; Harton, A. Impact of Nutrition Education on the Compliance with Model Food Ration in 231 Preschools, Poland: Results of Eating Healthy, Growing Healthy Program. Nutrients 2018, 10, 1427. [Google Scholar] [CrossRef]
- Harton, A.; Myszkowska-Ryciak, J. The role of nutrition education for correct nutrition in toddlers. J. Health Inequal. 2017, 3, 58–63. [Google Scholar] [CrossRef]
- DeCosta, P.; Møller, P.; Frøst, M.B.; Olsen, A. Changing children’s eating behaviour—A review of experimental research. Appetite 2017, 1, 327–357. [Google Scholar] [CrossRef]
- Myszkowska-Ryciak, J.; Harton, A. Do Preschools Offer Healthy Beverages to Children? A Nationwide Study in Poland. Nutrients 2017, 9, 1167. [Google Scholar] [CrossRef]
- Turlejska, H.; Pelzner, U.; Szponar, L.; Konecka-Matyjek, E. Principles of Rational Nutrition: Recommended Food Rations for Selected Population Groups in Mass Catering; Wydawnictwo ODDK: Gdańsk, Poland, 2004. (In Polish) [Google Scholar]
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. Data Base: Tables of Nutritional Value of Food Products and Dishes, 3rd ed.; Includes Online Data Covering 932 Food Products and Dishes; National Food and Nutrition Institute: Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- Drewnowski, A.; Dwyer, J.; King, J.C.; Weaver, C.M. A proposed nutrient density score that includes food groups and nutrients to better align with dietary guidance. Nutr. Rev. 2019, 77, 404–416. [Google Scholar] [CrossRef] [Green Version]
- Pyramid of Healthy Nutrition and Physical Activity for Children. Available online: http://www.izz.waw.pl/attachments/article/7/Piramida%20Zdrowego%20%C5%BBywienia%20i%20Aktywno%C5%9Bci%20Fizycznej%20Broszura.pdf (accessed on 20 August 2019). (In Polish).
- Jarosz, M. Human Nutrition Recommendations for Polish Population; IZZ: Warsaw, Poland, 2012. (In Polish) [Google Scholar]
- Larson, N.; Ward, D.S.; Neelon, S.B.; Story, M. What role can child-care settings play in obesity prevention? A review of the evidence and call for research efforts. J. Am. Diet. Assoc. 2011, 111, 1343–1362. [Google Scholar] [CrossRef]
- Hurley, K.M.; Yousafzai, A.K.; López Bóo, F. Early Child Development and Nutrition: A Review of the Benefits and Challenges of Implementing Integrated Interventions. Adv. Nutr. 2016, 7, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Finch, M.; Nathan, N.; Weaver, N.; Wiggers, J.; Yoong, S.L.; Jones, J.; Dodds, P.; Wyse, R.; Sutherland, R.; et al. Factors associated with early childhood education and care service implementation of healthy eating and physical activity policies and practices in Australia: A cross-sectional study. Transl. Behav. Med. 2015, 5, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Sunguya, B.F.; Poudel, K.C.; Mlunde, L.B.; Urassa, D.P.; Yasuoka, J.; Jimba, M. Nutrition training improves health workers’ nutrition knowledge and competence to manage child undernutrition: A systematic review. Front. Public Health 2013, 1, 37. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, L.J.; Langley-Evans, S.C.; McMullen, S. Childhood obesity and risk of the adult metabolic syndrome: A systematic review. Int. J. Obes. 2012, 36, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Halfon, N.; Kandyce, L.; Slusser, W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Suder, A.; Gomula, A.; Koziel, S. Central overweight and obesity in Polish schoolchildren aged 7–18 years: Secular changes of waist circumference between 1966 and 2012. Eur. J. Pediatr. 2017, 176, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Kułaga, Z.; Gurzkowska, B.; Grajda, A.; Wojtyło, M.; Góźdź, M.; Litwin, M. The prevalence of overweight and obesity among Polish pre-school-aged children. Dev. Period Med. 2016, 20, 143–149. [Google Scholar] [PubMed]
- Kling, S.M.R.; Roe, L.S.; Keller, K.L.; Rolls, B.J. Double trouble: Portion size and energy density combine to increase preschool children’s lunch intake. Physiol. Behav. 2016, 162, 18–26. [Google Scholar] [CrossRef]
- Waśkiewicz, A.; Szcześniewska, D.; Szostak-Węgierek, D.; Kwaśniewska, M.; Pająk, A.; Stepaniak, U.; Kozakiewicz, K.; Tykarski, A.; Zdrojewski, T.; Zujko, M.E.; et al. Are dietary habits of the Polish population consistent with the recommendations for prevention of cardiovascular disease?—WOBASZ II project. Kardiol. Pol. 2016, 74, 969–977. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Petersen, K.; Van Horn, L. Convincing evidence supports reducing saturated fat to decrease cardiovascular disease risk. BMJ Nutr. Prev. Health 2018. [Google Scholar] [CrossRef]
- Schwingshack, L.; Hoffmann, G. Monounsaturated fatty acids, olive oil and health status: A systematic review and meta-analysis of cohort studies. Lipids Health Dis. 2014, 13, 154. [Google Scholar] [CrossRef]
- Weker, H.; Barańska, M.; Riahi, A.; Strucińska, M.; Więch, M.; Rowicka, G.; Dyląg, H.; Klemarczyk, W.; Bzikowska, A.; Socha, P. Nutrition of infants and young children in Poland—PITNUTS 2016. Dev Period Med. 2017, XXI, 13–28. [Google Scholar]
- Suliga, E.; Cieśla, E.; Pietraszkiewicz, M.J. Assessment of vitamins and minerals content in the diets of preschool children. J. Educ. Health Sport 2018, 8, 794–802. [Google Scholar] [CrossRef]
- Strand, T.A.; Taneja, S.; Kumar, T.; Manger, M.S.; Refsum, H.; Yajnik, C.S.; Bhandari, N. Vitamin B-12, Folic Acid, and Growth in 6- to 30-Month-Old Children: A Randomized Controlled Trial. Pediatrics 2015, 135, e918–e926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, G.F.M. Vitamins: Their Role in the Human Body; Blackwell Publishing Ltd.: Oxford, UK, 2004. [Google Scholar]
- Kostecka, M. Eating habits of preschool children and the risk of obesity, insulin resistance and metabolic syndrome in adults. Pak. J. Med. Sci. 2014, 30, 1299–1303. [Google Scholar] [CrossRef] [PubMed]
- Bueno, M.B.; Fisberg, R.M.; Maximino, P.; de Padua Rodrigues, G.; Fisberg, M. Nutritional risk among Brazilian children 2 to 6 years old: A multicenter study. Nutrition 2013, 29, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Kmieć, P.; Żmijewski, M.; Waszak, P.; Sworczak, K.; Lizakowska-Kmieć, M. Vitamin D deficiency during winter months among an adult, predominantly urban, population in northern Poland. Endokrynol. Pol. 2014, 65, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K.; Bossowski, A.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dobrzańska, A.; Franek, E.; Helwich, E.; et al. Vitamin D Supplementation Guidelines for General Population and Groups at Risk of Vitamin D Deficiency in Poland—Recommendations of the Polish Society of Pediatric Endocrinology and Diabetes and the Expert Panel With Participation of National Specialist Consultants and Representatives of Scientific Societies—2018 Update. Front. Endocrinol. 2018, 9, 246. [Google Scholar] [CrossRef]
- Płudowski, P.; Ducki, C.; Konstantynowicz, J.; Jaworski, M. Vitamin D status in Poland. Pol. Arch. Intern. Med. 2016, 126, 530–538. [Google Scholar] [CrossRef]
- Balvers, M.G.; Brouwer-Brolsma, E.M.; Endenburg, S.; de Groot, L.C.; Kok, F.J.; Gunnewiek, J.K. Recommended intakes of vitamin D to optimise health, associated circulating 25-hydroxyvitamin D concentrations, and dosing regimens to treat deficiency: Workshop report and overview of current literature. J. Nutr. Sci. 2015, 25, 23. [Google Scholar] [CrossRef]
- Merkiel-Pawłowska, S.; Chalcarz, W. Gender differences and typical nutrition concerns of the diets of preschool children—The results of the first stage of an intervention study. BMC Pediatr. 2017, 17, 207. [Google Scholar] [CrossRef]
- Kwiecień, M.; Winiarska-Mieczan, A.; Danek-Majewska, A.; Kiczorowska, B.; Olcha, M. Assessment of nutritional value of feed rations for preschool children with particular emphasis on mineral content. Probl. Hig. Epidemiol. 2015, 96, 742–745. (In Polish) [Google Scholar]
- Johner, S.A.; Thamm, M.; Nothlings, U.; Remer, T. Iodine status in preschool children and evaluation of major dietary iodine sources: A German experience. Eur. J. Nutr. 2013, 52, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Benoist de, B.; Andersson, M.; Egli, I.; Takkouche, B.; Allen, H. Iodine Status Worldwide: WHO Global Database on Iodine Deficiency; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Szybiński, Z. Poland Remains Iodine Sufficient After 20 Years of IDD Prevention, But Pregnant Women May Be at Risk. IDD Newsletter; Poland, August 2015. Available online: http://www.ign.org/cm_data/IDD_aug15_poland.pdf (accessed on 20 August 2019).
- World Health Organization and Food and Agriculture Organization of the United Nations. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Golden, N.H.; Abrams, S.A.; Committee ON Nutrition. Optimizing Bone Health in Children and Adolescents. Pediatrics 2014, 134, 1229–1243. [Google Scholar] [CrossRef] [PubMed]
- Fleischhacker, S.; Cason, K.L.; Achterberg, C. “You had peas today?”: A pilot study comparing a Head Start child-care center’s menu with the actual food served. J. Am. Diet. Assoc. 2006, 106, 277–280. [Google Scholar] [CrossRef]
- Ritchie, L.D.; Sharma, S.; Gildengorin, G.; Yoshida, S.; Braff-Guajardo, E.; Crawford, P. Policy improves what beverages are served to young children in child care. J. Acad. Nutr. Diet. 2015, 115, 724–730. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Nutrient | DRI for Children Aged 3–6 Years | Daily Supply (per Child/Day) | ∆ % 1/ p-Value * | |||
|---|---|---|---|---|---|---|
| Mean ± SD | % of DRI for Children Aged 3–6 Years | |||||
| Baseline | Post-Baseline | Baseline | Post-Baseline | |||
| Energy [kcal] | 1000 2/1400 3 | 1257.1 ± 203.07 | 1224.3 ± 217.11 | 126 2/90 3 | 122 2/87 3 | −2.7/0.006 |
| Protein [g] | 14 2/21 3 | 45.8 ± 5.55 | 45.2 ± 7.61 | 327 2/218 3 | 323 2/215 3 | −1.4/NS |
| Protein [% of energy] | 10–20 | 14.6 ± 1.64 | 14.8 ± 1.30 | - | - | 1.5/<0.001 |
| Animal protein [g] | NA | 28.0 ± 6.68 | 27.2 ± 5.23 | NA | NA | −2.8/NS |
| Vegetable protein [g] | NA | 17.8 ± 3.41 | 17.9 ± 3.59 | NA | NA | 1.0/NS |
| Fat [g] | 33–44 2/31–54 3 | 46.5 ± 9.75 | 44.7 ± 10.49 | 141–106 2/150–86 3 | 135–101 2/144–83 3 | −4.0/0.002 |
| Fat [% of energy] | 20–35 | 33.2 ± 3.96 | 32.7 ± 4.05 | - | - | −1.4/0.049 ** |
| SFA [% of energy] | as low as possible | 12.9 ± 1.75 | 12.8 ± 1.70 | - | - | −0.2/NS |
| MUFA [% of energy] | NA | 13.1 ± 2.11 | 12.8 ± 2.14 | NA | NA | −2.8/0.006 |
| PUFA [% of energy] | NA | 4.8 ± 1.00 | 4.7 ± 0.94 | NA | NA | −1.2/NS |
| Cholesterol [mg] | <300 | 170.3 ± 37.02 | 167.1 ± 37.27 | 56 | 56 | −1.9/NS |
| CHO [g] | 130 | 162.6 ± 28.76 | 159.0 ± 30.36 | 125 | 122 | −2.3/0.012 |
| CHO [% of energy] | 50–70 | 51.8 ± 3.85 | 52.0 ± 3.88 | 104–74 | 104–74 | 0.4/NS |
| Sucrose [% of energy] | NA | 9.2 ± 2.89 | 8.9 ±2.83 | NA | NA | −3.4/NS |
| Lactose [g] | NA | 10.6 ± 3.28 | 10.9 ± 3.32 | NA | NA | 3.2/NS |
| Starch [g] | NA | 95.8 ± 18.36 | 94. ± 5 19.98 | NA | NA | −1.3/NS |
| Dietary fiber [g] | 10 2/14 3 | 16.1 ± 3.61 | 16.4 ± 4.07 | 161 2/115 3 | 164 2/117 3 | 2.3/NS |
| Nutrient | DRI for Children Aged 3–6 Years | Daily Supply (per Child/Day) | ∆ % 1/ p-Value * | |||
|---|---|---|---|---|---|---|
| Mean ± SD | % of DRI for Children Aged 3–6 Years | |||||
| Baseline | Post-Baseline | Baseline | Post-Baseline | |||
| Vitamin A [μg] | 400 2/450 3 | 1070.5 ± 410.37 | 1121.0 ± 473.16 | 268 2/238 3 | 280 2/249 3 | 4.5/0.043 |
| Retinol [μg] | NA | 336.9 ± 260.97 | 333.6 ± 286.69 | NA | NA | −1.0/NS |
| Beta-carotene [μg] | NA | 4398.3 ± 1721.02 | 4720.4 ± 2012.77 | NA | NA | 6.8/0.004 |
| Vitamin B1 [mg] | 0.5 2/0.6 3 | 0.9 ± 0.17 | 0.9 ± 0.16 | 180 2/150 3 | 180 2/150 3 | −0.3/NS |
| Vitamin B2 [mg] | 0.5 2/0.6 3 | 1.1 ± 0.21 | 1.1 ± 0.21 | 220 2/183 3 | 220 2/183 3 | 0.8/NS |
| Vitamin B6 [mg] | 0.5 2/0.6 3 | 1.6 ± 0.30 | 1.6 ± 0.30 | 320 2/267 3 | 320 2/267 3 | −0.6/NS |
| Vitamin B12 [μg] | 0.9 2/1.2 3 | 2.9 ± 1.16 | 2.9 ± 1.26 | 322 2/167 3 | 322 2/167 3 | −1.8/NS |
| Vitamin C [mg] | 40 2/50 3 | 101.9 ± 29.81 | 105.9 ± 38.58 | 255 2/204 3 | 265 2/212 3 | 3.8/NS |
| Vitamin D [μg] | 15 | 1.8 ± 0.63 | 1.7 ± 0.59 | 12 | 11 | −6.4/0.032 |
| Vitamin E [mg] | 6 | 6.6 ± 1.78 | 6.4 ± 1.60 | 110 | 107 | −3.0/NS |
| Folate [μg] | 150 2/200 3 | 221.1 ± 47.71 | 223.8 ± 49.46 | 147 2/111 3 | 149 2/112 3 | 1.2/NS |
| Niacin [mg] | 6 2/8 3 | 10.3 ± 2.01 | 10.2 ± 1.94 | 172 2/129 3 | 170 2/128 3 | −1.6/NS |
| Nutrient | DRI for Children Aged 3–6 Years | Daily Supply (per Child/Day) | ∆ % 1/ p-Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | % of DRI for Children Aged 3–6 Years | |||||
| Baseline | Post-Baseline | Baseline | Post-Baseline | |||
| Calcium [mg] | 700 2/1000 3 | 454.3 ± 108.56 | 463.6 ± 110.41 | 65 2/45 3 | 66 2/46 3 | 2.0/NS |
| Copper [mg] | 0.3 2/0.4 3 | 0.9 ± 0.27 | 0.9 ± 0.17 | 300 2/225 3 | 300 2/225 3 | −0.3/NS |
| Iodine [μg] | 90 | 108.0 ± 64.48 | 104.1 ± 56.47 | 120 | 116 | −3.8/NS |
| Iron [mg] | 7 2/10 3 | 6.7 ± 1.42 | 6.7 ± 1.33 | 96 2/67 3 | 96 2/67 3 | 0.3/NS |
| Magnesium [mg] | 80 2/130 3 | 206.2 43.08 | 207.0 ± 38.55 | 258 2/159 3 | 259 2/159 3 | 0.4/NS |
| Phosphorus [mg] | 460 2/500 3 | 802.4 ± 139.35 | 809.0 ± 138.66 | 174 2/160 3 | 176 2/162 3 | 0.8/NS |
| Potassium [mg] | 2400 2/3100 3 | 2469.0 ± 472.67 | 2452.8 ± 480.32 | 103 2/80 3 | 102 2/79 3 | −0.7/NS |
| Sodium [mg] | 750 2/1000 3 | 2288.0 ± 1164.02 | 2192.6 ± 1115.27 | 305 2/229 3 | 292 2/219 3 | −4.3/NS |
| Zinc [mg] | 3 2/5 3 | 5.9 ± 1.10 | 6.0 ± 1.05 | 197 2/118 3 | 200 2/120 3 | 0.8/NS |
| Nutrient | Recommended NER 1 | Preschools Menus NER 2 | ∆ % 3/ p-Value * | ||
|---|---|---|---|---|---|
| Aged 1–3 Years | Aged 4–6 Years | Baseline | Post-Baseline | ||
| Mean ± SD | Mean ± SD | ||||
| Vitamin A [μg] | 400 | 321 | 853 ± 303.2 | 927 ± 427.1 | 8.0/<0.001 |
| Vitamin B1 [mg] | 0.5 | 0.4 | 0.7 ± 0.09 | 0.7 ± 0.08 | 2.5/0.002 |
| Vitamin B2 [mg] | 0.5 | 0.4 | 0.9 ± 0.12 | 0.9 ± 0.13 | 3.7/< 0.001 |
| Vitamin B6 [mg] | 0.5 | 0.4 | 1.2 ± 0.17 | 1.3 ± 0.17 | 2.1/0.023 |
| Vitamin B12 [μg] | 0.9 | 0.9 | 2.3 ± 0.88 | 2.4 ± 1.11 | 1.6/NS |
| Vitamin C [mg] | 40 | 36 | 81 ± 19.8 | 87 ± 27.3 | 6.5/0.002 |
| Vitamin D [μg] | 15 | 11 | 1.4 ± 0.49 | 1.3 ± 0.45 | −3.8/NS |
| Vitamin E [mg] | 6 | 4.3 | 5.2 ± 0.99 | 5.2 ± 0.89 | - |
| Folate [μg] | 150 | 143 | 176 ± 26.6 | 184 ± 31.8 | 4.2/<0.001 |
| Niacin [mg] | 6 | 5.7 | 8.2 ± 1.10 | 8.3 ± 1.08 | 1.2/NS |
| Calcium [mg] | 700 | 714 | 363 ± 75.6 | 382 ± 79.6 | 4.8/<0.001 ** |
| Copper [mg] | 0.3 | 0.3 | 0.7 ± 0.17 | 0.7 ± 0.10 | 3.0/<0.001 |
| Iodine [μg] | 90 | 64 | 86 ± 47.6 | 85 ± 41.3 | −1.6/NS |
| Iron [mg] | 7 | 7.1 | 5.3 ± 0.73 | 5.5 ± 0.72 | 3.2/<0.001 |
| Magnesium [mg] | 80 | 93 | 164 ± 24.2 | 170 ± 20.7 | 3.2/<0.001 |
| Phosphorus [mg] | 460 | 357 | 641 ± 70.3 | 665 ± 75.4 | 3.7/<0.001 |
| Potassium [mg] | 2400 | 2214 | 1820 ± 256.2 | 2014 ± 271.1 | 2.2/0.018 |
| Sodium [mg] | 750 | 714 | 1971 ± 851.0 | 1778 ± 783.7 | −2.4/NS |
| Zinc [mg] | 3 | 3.6 | 4.7 ± 0.51 | 4.9 ± 0.52 | 3.7/<0.001 |
| Nutrient | Recommendations for Preschool Menu 1 | Preschools Meeting the Recommendations | p-Value */Cramér’s V | |
|---|---|---|---|---|
| number/% | ||||
| Baseline | Post-Baseline | |||
| Energy [kcal] | 880–1080 | 50/21.6 | 60/26.0 | <0.001/0.32 |
| Total fat [% of Energy] | 20–35% | 163/70.6 | 171/74.0 | <0.001/0.31 |
| SFA [% of Energy] | <10% 2 | 6/2.6 | 11/4.8 | <0.001/0.52 |
| Sucrose [% of Energy] | <10% 3 | 128/55.4 | 152/65.8 | <0.001/0.45 |
| Dietary Fiber [g] | 9.8 | 230/99.6 | 228/98.7 | NS |
| Calcium [mg] | 700 | 3/1.3 | 7/3.0 | 0.002/0.20 |
| Iron [mg] | 7 | 81/35.1 | 88/38.1 | <0.001/0.50 |
| Iodine [μg] | 63 | 182/78.8 | 178/77.0 | <0.001/0.34 |
| Potassium [mg] | 2170 | 169/73.2 | 163/70.0 | <0.001/0.41 |
| Vitamin D [μg] | 10.5 | 0/0 | 0/0 | - |
| Folate [μg] | 140 | 226/97.8 | 226/97.8 | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myszkowska-Ryciak, J.; Harton, A. Eating Healthy, Growing Healthy: Outcome Evaluation of the Nutrition Education Program Optimizing the Nutritional Value of Preschool Menus, Poland. Nutrients 2019, 11, 2438. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102438
Myszkowska-Ryciak J, Harton A. Eating Healthy, Growing Healthy: Outcome Evaluation of the Nutrition Education Program Optimizing the Nutritional Value of Preschool Menus, Poland. Nutrients. 2019; 11(10):2438. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102438
Chicago/Turabian StyleMyszkowska-Ryciak, Joanna, and Anna Harton. 2019. "Eating Healthy, Growing Healthy: Outcome Evaluation of the Nutrition Education Program Optimizing the Nutritional Value of Preschool Menus, Poland" Nutrients 11, no. 10: 2438. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102438