Evaluation of a Technological Image-Based Dietary Assessment Tool for Children during Pubertal Growth: A Pilot Study

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| ICC | intra-class correlation |
| 24-HDR | 24-h dietary recall |
| FR | food records |
| TEE | total energy expenditure |
| TPLS | Taipei Puberty Longitudinal Study |
References
- Soliman, A.; De Sanctis, V.; Elalaily, R. Nutrition and pubertal development. Indian J. Endocrinol. Metab. 2014, 18, S39–S47. [Google Scholar] [CrossRef] [PubMed]
- Villamor, E.; Jansen, E.C. Nutritional Determinants of the Timing of Puberty. Annu. Rev. Public Health 2016, 37, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baranowski, T. 24-hour dietary recall and diet record methods. Nutr. Epidemiol. 2012, 40, 49–69. [Google Scholar]
- Livingstone, M.B.E.; Robson, P.J.; Wallace, J.M.W. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [PubMed]
- Illner, A.-K.; Freisling, H.; Boeing, H.; Huybrechts, I.; Crispim, S.; Slimani, N.; Crispim, S. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int. J. Epidemiol. 2012, 41, 1187–1203. [Google Scholar] [CrossRef] [Green Version]
- Davison, B.K.; Quigg, R.; Skidmore, P.M.L. Pilot Testing a Photo-Based Food Diary in Nine- to Twelve-Year Old- Children from Dunedin, New Zealand. Nutrients 2018, 10, 240. [Google Scholar] [CrossRef]
- Olafsdottir, A.S.; Hörnell, A.; Hedelin, M.; Waling, M.; Gunnarsdóttir, I.; Olsson, C. Development and Validation of a Photographic Method to Use for Dietary Assessment in School Settings. PLoS ONE 2016, 11, e0163970. [Google Scholar] [CrossRef]
- Freedman, L.S.; Potischman, N.; Kipnis, V.; Midthune, D.; Schatzkin, A.; Thompson, F.E.; Troiano, R.P.; Prentice, R.; Patterson, R.; Carroll, R.; et al. A comparison of two dietary instruments for evaluating the fat–breast cancer relationship. Int. J. Epidemiol. 2006, 35, 1011–1021. [Google Scholar] [CrossRef]
- Freedman, L.S.; Schatzkin, A.; Midthune, D.; Kipnis, V. Dealing with Dietary Measurement Error in Nutritional Cohort Studies. J. Natl. Cancer Inst. 2011, 103, 1086–1092. [Google Scholar] [CrossRef]
- Gemming, L.; Utter, J.; Ni Mhurchu, C. Image-Assisted Dietary Assessment: A Systematic Review of the Evidence. J. Acad. Nutr. Diet. 2015, 115, 64–77. [Google Scholar] [CrossRef]
- Carter, M.C.; Hancock, N.; Albar, S.A.; Brown, H.; Greenwood, D.C.; Hardie, L.J.; Frost, G.S.; Wark, P.A.; Cade, J.E. Development of a New Branded UK Food Composition Database for an Online Dietary Assessment Tool. Nutrients 2016, 8, 480. [Google Scholar] [CrossRef] [PubMed]
- Stumbo, P.; Sazonov, P.E.; Daugherty, B.L.; Schap, T.E.; Ettienne-Gittens, R.; Zhu, F.M.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; et al. Novel Technologies for Assessing Dietary Intake: Evaluating the Usability of a Mobile Telephone Food Record Among Adults and Adolescents. J. Med Internet Res. 2012, 14, e58. [Google Scholar] [CrossRef]
- Burrows, T.L.; Rollo, M.E.; Williams, R.; Wood, L.G.; Garg, M.L.; Jensen, M.; Collins, C.E. A Systematic Review of Technology-Based Dietary Intake Assessment Validation Studies That Include Carotenoid Biomarkers. Nutrients 2017, 9, 140. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Spoden, M.; Zhu, F.M.; Delp, E.J.; Kerr, D.A. New mobile methods for dietary assessment: Review of image-assisted and image-based dietary assessment methods. Proc. Nutr. Soc. 2017, 76, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, A.L.; Piernas, C.; Illner, A.-K.; Gibney, M.J.; Gurinović, M.A.; De Vries, J.H.; Cade, J.E. Evaluation of New Technology-Based Tools for Dietary Intake Assessment—An ILSI Europe Dietary Intake and Exposure Task Force Evaluation. Nutrients 2018, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, F.J.; Ridgers, N.D.; Worsley, A.; McNaughton, S.A. Evaluation of a smartphone food diary application using objectively measured energy expenditure. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Boushey, C.J.; Spoden, M.; Delp, E.J.; Zhu, F.M.; Bosch, M.; Ahmad, Z.; Shvetsov, Y.B.; Delany, J.P.; Kerr, D.A. Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults. Nutrients 2017, 9, 312. [Google Scholar] [CrossRef]
- Kerr, D.A.; Harray, A.J.; Pollard, C.M.; Dhaliwal, S.S.; Delp, E.J.; Howat, P.A.; Pickering, M.R.; Ahmad, Z.; Meng, X.; Pratt, I.S.; et al. The connecting health and technology study: A 6-month randomized controlled trial to improve nutrition behaviours using a mobile food record and text messaging support in young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 52. [Google Scholar] [CrossRef]
- Timon, C.M.; Astell, A.J.; Hwang, F.; Adlam, T.D.; Smith, T.; Maclean, L.; Spurr, D.; Forster, S.E.; Williams, E.A. The validation of a computer-based food record for older adults: The Novel Assessment of Nutrition and Ageing (NANA) method. Br. J. Nutr. 2015, 113, 654–664. [Google Scholar] [CrossRef]
- Delisle, C.; Sandin, S.; Forsum, E.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Ortega, F.B.; Ruiz, J.R.; Silfvernagel, K.; et al. A web- and mobile phone-based intervention to prevent obesity in 4-year-olds (MINISTOP): A population-based randomized controlled trial. BMC Public Health 2015, 15, 95. [Google Scholar] [CrossRef]
- Delisle Nyström, C.; Forsum, E.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Timpka, T.; Lof, M. A Mobile Phone Based Method to Assess Energy and Food Intake in Young Children: A Validation Study against the Doubly Labelled Water Method and 24 h Dietary Recalls. Nutrients 2016, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, H.; Bonn, S.E.; Bergström, A.; Bälter, K.; Bälter, O.; Delisle, C.; Forsum, E.; Löf, M.; Westerterp, K.; Zepeda, L. A New Mobile Phone-Based Tool for Assessing Energy and Certain Food Intakes in Young Children: A Validation Study. JMIR mHealth uHealth 2015, 3, e38. [Google Scholar] [CrossRef] [PubMed]
- Stumbo, P.J. New technology in dietary assessment: A review of digital methods in improving food record accuracy. Proc. Nutr. Soc. 2013, 72, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Yoder, A.B.; Hingle, M.; Bruening, M.; Casperson, S.L.; Sieling, J.; Moon, J.; Johnson, L.; Roemmich, J.N.; Whigham, L. A Mobile Phone Food Record App to Digitally Capture Dietary Intake for Adolescents in a Free-Living Environment: Usability Study. JMIR mHealth uHealth 2015, 3, e30. [Google Scholar] [CrossRef]
- Rollo, M.E.; Ash, S.; Lyons-Wall, P.; Russell, A.W. Evaluation of a Mobile Phone Image-Based Dietary Assessment Method in Adults with Type 2 Diabetes. Nutrients 2015, 7, 4897–4910. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Food and Drug Administration. Taiwanese Food Composition and Nutrient Database. 2017. Available online: https://consumer.fda.gov.tw/Food/TFND.aspx?nodeID=178 (accessed on 7 December 2018).
- Cade, J.; Thompson, R.; Burley, V.; Warm, D.J.C. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Chang, M.-H. New Growth Charts for Taiwanese Children and Adolescents Based on World Health Organization Standards and Health-related Physical Fitness. Pediatr. Neonatol. 2010, 51, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.K.; Correa, J.B.; Han, H.; Allen, H.R.; Rood, J.C.; Champagne, C.M.; Gunturk, B.K.; Bray, G.A. Validity of the Remote Food Photography Method (RFPM) for estimating energy and nutrient intake in near real-time. Obesity 2012, 20, 891–899. [Google Scholar] [CrossRef]
- Smith, L.P.; Hua, J.; Seto, E.; Du, S.; Zang, J.; Zou, S.; Popkin, B.M.; Mendez, M.A. Development and validity of a 3-day smartphone assisted 24-hour recall to assess beverage consumption in a Chinese population: A randomized cross-over study. Asia Pac. J. Clin. Nutr. 2014, 23, 678–690. [Google Scholar] [CrossRef]
- Williamson, D.A.; Allen, H.R.; Martin, P.D.; Alfonso, A.J.; Gerald, B.; Hunt, A. Comparison of digital photography to weighed and visual estimation of portion sizes. J. Am. Diet. Assoc. 2003, 103, 1139–1145. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. ‘My Meal Mate’ (MMM): Validation of the diet measures captured on a smartphone application to facilitate weight loss. Br. J. Nutr. 2013, 109, 539–546. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | n or Mean | % or SD |
|---|---|---|
| Sex | ||
| Male | 13 | 56.5 |
| Female | 10 | 43.5 |
| Age | 10.47 | 3.36 |
| BMI (kg/m2) | 18.41 | 4.34 |
| Thin | 2 | 8.7 |
| Healthy | 16 | 69.57 |
| Overweight | 3 | 13.04 |
| Obese | 2 | 8.7 |
| COFIT | Food Records | Wilcoxon Signed-Rank Test | 3 SCC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 1 SD | 2 ICC | Mean | SD | ICC | p | r | 95% CI | p | |
| Energy (kcal/day) | 1584.88 | 369.03 | 0.94 | 1779.11 | 316.29 | 0.85 | <0.001 * | 0.64 | 0.30–0.83 | <0.01 |
| Protein (g) | 63.67 | 16.16 | 0.54 | 71.06 | 13.60 | 0.68 | 0.02 * | 0.44 | 0.02–0.72 | <0.01 |
| Amino acid (mg) | 60,229 | 15,835 | 0.83 | 65,140 | 13,262 | 0.73 | 0.10 | 0.50 | 0.11–0.76 | 0.01 |
| Fat (g) | 65.00 | 17.97 | 0.65 | 76.77 | 17.84 | 0.88 | <0.001 * | 0.65 | 0.32–0.84 | <0.01 |
| Fatty acids, total polyunsaturated (mg) | 12,658.8 | 4961.96 | 0.95 | 13,879.95 | 4278.4 | 0.64 | 0.20 | 0.61 | 0.11–0.76 | <0.01 |
| Fatty acids, total monounsaturated (mg) | 7418.10 | 2524.19 | 0.79 | 8714.20 | 2555.6 | 0.46 | 0.01 * | 0.49 | 0.11–0.76 | 0.02 |
| Fatty acids, saturated (mg) | 6.43 | 2.51 | 0.47 | 7.57 | 3.20 | 0.51 | 0.04 * | 0.54 | 0.17–0.78 | <0.01 |
| Carbohydrates (g) | 186.50 | 46.15 | 0.98 | 201.59 | 46.82 | 0.67 | 0.08 | 0.47 | 0.07–0.74 | 0.03 |
| Sugars (g) | 33.48 | 16.78 | 0.87 | 35.27 | 20.85 | 0.89 | 0.60 | 0.67 | 0.35–0.85 | <0.001 |
| Glucose (g) | 6.57 | 3.92 | 0.99 | 6.07 | 4.01 | 0.20 | 0.28 | 0.77 | 0.53–0.90 | <0.001 |
| Fructose (g) | 7.55 | 4.53 | 0.99 | 5.51 | 3.92 | 0.57 | <0.01 * | 0.65 | 0.32–0.84 | <0.001 |
| Maltose (g) | 1.81 | 1.66 | 0.99 | 1.50 | 0.93 | 0.97 | 0.67 | 0.61 | 0.27–0.82 | <0.01 |
| Sucrose (g) | 11.28 | 9.04 | 0.57 | 16.13 | 13.48 | 0.97 | <0.01 * | 0.55 | 0.18–0.79 | <0.01 |
| Lactose (g) | 6.30 | 4.79 | 0.95 | 6.28 | 4.58 | 0.98 | 0.93 | 0.94 | 0.86–0.98 | <0.001 |
| Dietary Fiber (g) | 9.74 | 3.36 | 0.94 | 10.72 | 2.77 | 0.68 | 0.12 | 0.59 | 0.23–0.80 | <0.01 |
| COFIT | Food Records | Wilcoxon Signed-Rank Test | 3 SCC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 1 SD | 2 ICC | Mean | SD | ICC | p | r | 95% CI | p | |
| Na (mg) | 2336.28 | 815.92 | 0.92 | 2020.45 | 730.45 | 0.69 | 0.02 * | 0.66 | 0.33–0.84 | <0.001 |
| Ca (mg) | 513.21 | 286.49 | 0.83 | 574.76 | 265.53 | 0.79 | 0.34 | 0.48 | 0.08–0.74 | 0.02 |
| K (mg) | 1696.45 | 636.88 | 0.80 | 1778.35 | 510.31 | 0.87 | 0.60 | 0.45 | 0.05–0.73 | 0.03 |
| Mg (mg) | 183.33 | 83.11 | 0.82 | 210.90 | 83.34 | 0.63 | 0.27 | 0.28 | −0.14–0.62 | 0.20 |
| Zn (mg) | 8.12 | 2.75 | 0.70 | 8.16 | 1.73 | 0.78 | 0.88 | 0.27 | −0.16–0.61 | 0.22 |
| P (mg) | 882.39 | 224.64 | 0.68 | 938.26 | 186.53 | 0.94 | 0.30 | 0.43 | 0.02–0.71 | 0.04 |
| Fe (mg) | 8.92 | 5.75 | 0.88 | 9.97 | 6.43 | 0.73 | 0.70 | 0.52 | 0.14–0.77 | 0.01 |
| Folic acid (µg) | 188.28 | 56.07 | 0.96 | 202.15 | 56.99 | 0.53 | 0.41 | 0.77 | 0.51–0.89 | <0.001 |
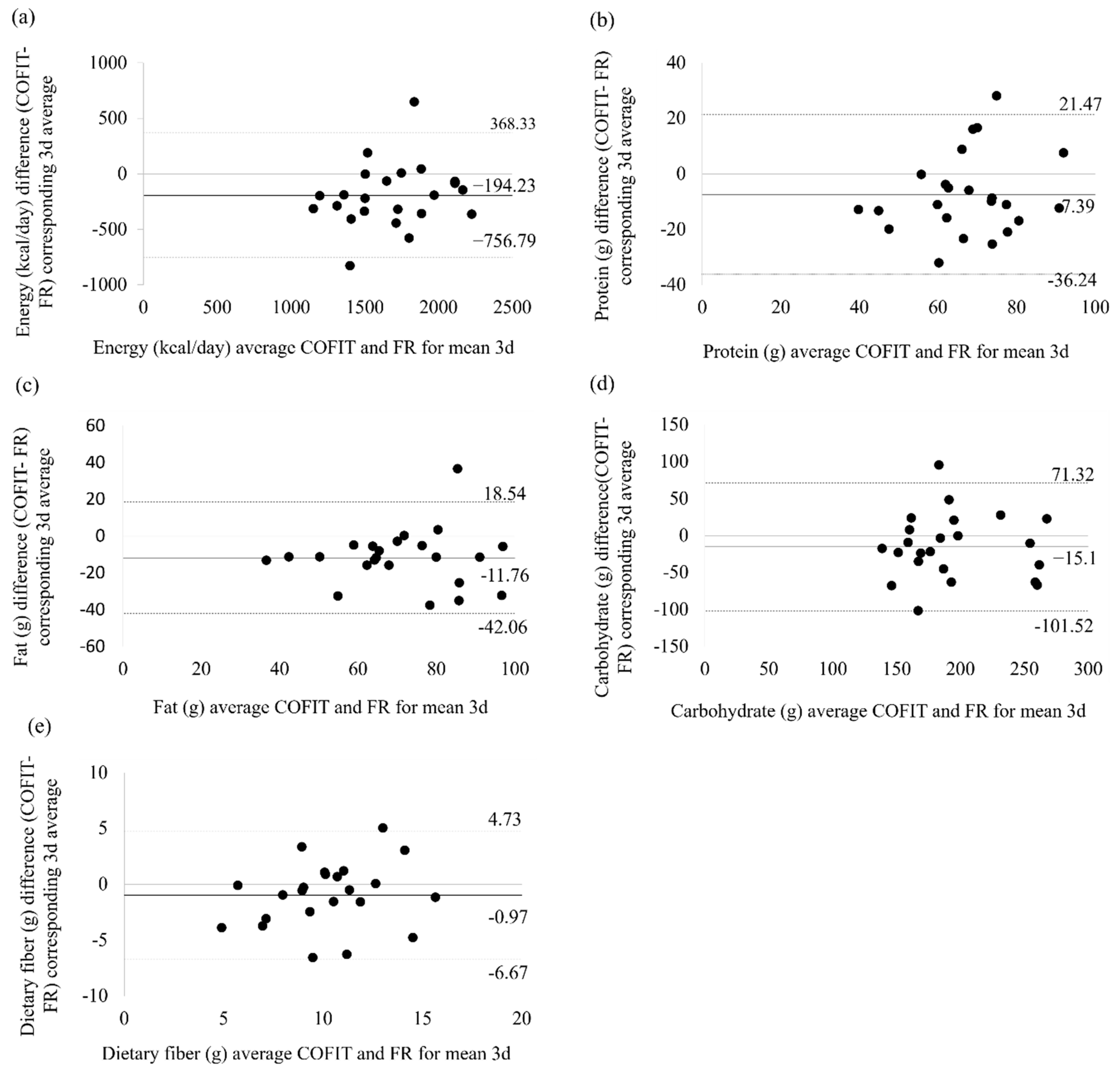
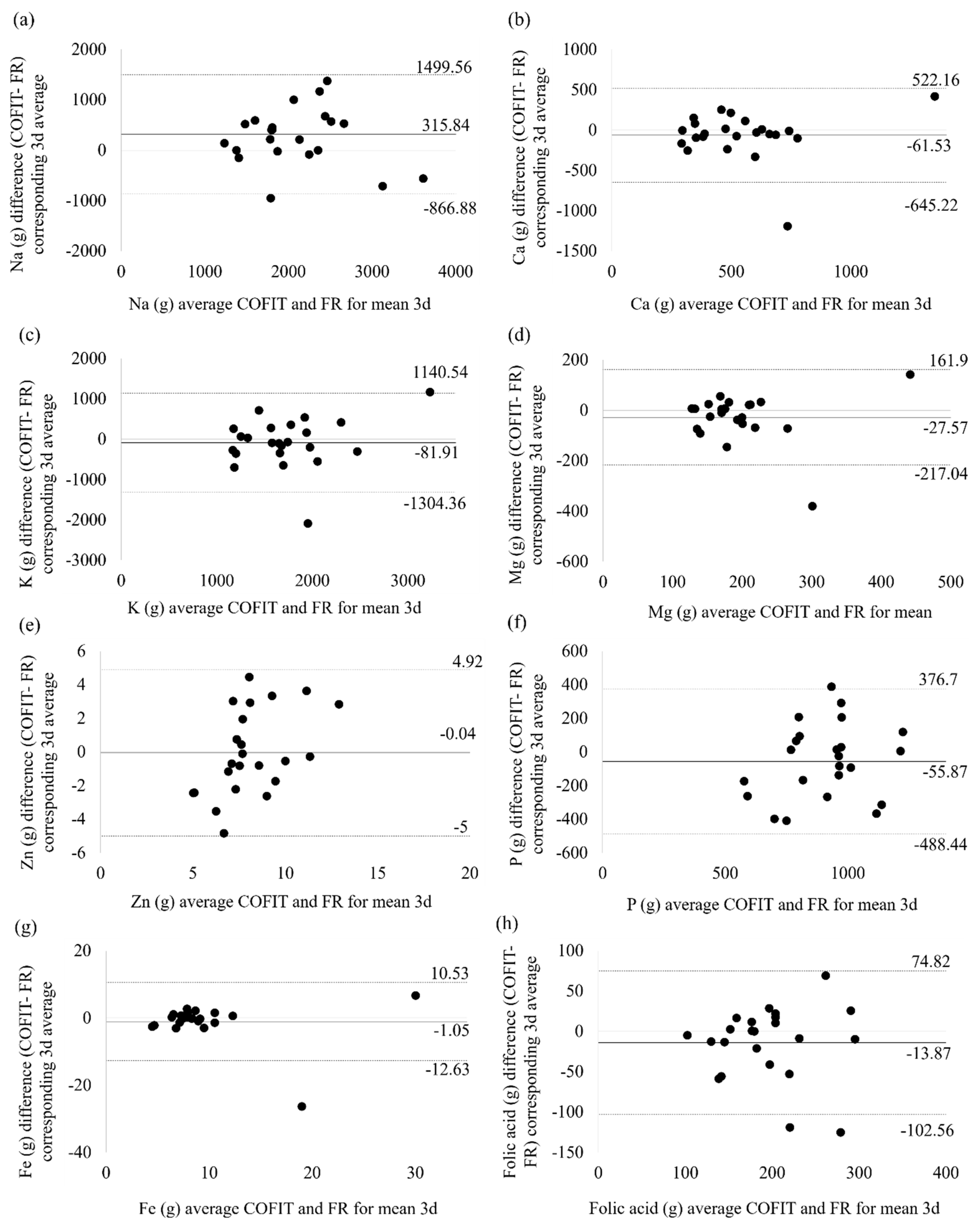
| Bland–Altman Analysis (COFIT−FR) | ||||
|---|---|---|---|---|
| Mean Difference | SD | 95% LOA | ||
| Energy (kcal/day) | −194.23 | 287.02 | −756.79 | 368.33 |
| Protein (g) | −7.39 | 14.72 | −36.24 | 21.46 |
| Fat (g) | −11.76 | 15.46 | −42.06 | 18.54 |
| Carbohydrate (g) | −15.10 | 44.09 | −101.52 | 71.32 |
| Dietary Fiber (g) | −0.97 | 2.91 | −6.67 | 4.73 |
| Na (mg) | 315.84 | 603.43 | −866.88 | 1499.56 |
| Ca (mg) | −61.53 | 297.8 | −645.22 | 522.16 |
| K (mg) | −81.91 | 623.70 | −1304.36 | 1140.54 |
| Mg (mg) | −27.57 | 96.67 | −217.04 | 161.90 |
| Zn (mg) | −0.04 | 2.53 | −5.00 | 4.92 |
| P (mg) | −55.87 | 220.70 | −488.44 | 376.70 |
| Fe (mg) | −1.05 | 5.91 | −12.63 | 10.53 |
| Folic acid (µg) | −13.87 | 45.25 | −102.56 | 74.82 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-S.; Hsieh, R.-H.; Tung, Y.-T.; Chen, Y.-H.; Yang, C.; Chen, Y.C. Evaluation of a Technological Image-Based Dietary Assessment Tool for Children during Pubertal Growth: A Pilot Study. Nutrients 2019, 11, 2527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102527
Wang J-S, Hsieh R-H, Tung Y-T, Chen Y-H, Yang C, Chen YC. Evaluation of a Technological Image-Based Dietary Assessment Tool for Children during Pubertal Growth: A Pilot Study. Nutrients. 2019; 11(10):2527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102527
Chicago/Turabian StyleWang, Jiao-Syuan, Rong-Hong Hsieh, Yu-Tang Tung, Yue-Hwa Chen, Chen Yang, and Yang Ching Chen. 2019. "Evaluation of a Technological Image-Based Dietary Assessment Tool for Children during Pubertal Growth: A Pilot Study" Nutrients 11, no. 10: 2527. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102527