The Effect of the Body Mass Indexes of Young Healthy Individuals on the Glyacemic Indexes of Traditional and Modified Vegetarian Meals


Abstract
:1. Introduction
2. Materials and Methods
2.1. Determination of the Nutritional Value of the Analysed Meals
2.1.1. Recipes and Preparing the Meals
- -
- Curd cheese, fatty—34 g;
- -
- Chicken eggs, whole—4 g;
- -
- Butter—10 g (5 g for stuffing, 5 g for direct consumption);
- -
- Wheat flour type 471—54 g (18 g for brewing);
- -
- Onion—30 g (15 g for stuffing, 15 g for direct consumption);
- -
- Potatoes—110 g;
- -
- Water—30 g;
- -
- Cake salt—0.07 g;
- -
- Salt for stuffing—0.7 g;
- -
- Pepper for stuffing—0.12 g.
- -
- Curd cheese, lean cheese—100 g;
- -
- Chicken egg, yolk—10 g;
- -
- Butter—5 g;
- -
- Wheat flour type 471—50 g;
- -
- Bread crumbs—6 g;
- -
- Icing sugar—12 g (7 g for the dough, 5 g for direct consumption).
- -
- Milk, 2% fat—55 g;
- -
- Curd cheese, fatty—90 g;
- -
- Chicken eggs, whole—15 g (added to the dough);
- -
- Chicken egg, yolk—10 g (added to the stuffing);
- -
- Oil—3 g;
- -
- Butter—4 g;
- -
- Wheat flour type 471—50 g;
- -
- Icing sugar—14 g (10 g for stuffing, 4 g for direct consumption);
- -
- Salt—0.05 g;
- -
- Water—45 g.
2.1.2. Nutritional Value Analysis
- -
- The contents of moisture and dry matter (gravimetric-drying method). The method consisted of drying the specimens, first by pre-drying at 60 °C. The food samples were mixed with roasted sand. This increases the evaporation surface. The samples were dried at 105 °C to constant weight.
- -
- Total ash: The method consisted of determining the mass of the residue after ashing the samples. The combustion of the sample was carried out in two-step process: carbonization of the sample and roasting in a muffle furnace at 600 °C.
- -
- Protein (Kjeldahl method): The method consisted of the mineralization of the tested substance in boiling sulphuric acid which resulted in proteins being oxidized to CO2 and H2O. Nitrogen from amino protein groups was released in the form of ammonia and it bound to sulfuric acid. After alkalising the sample, the ammonia was distilled to boric acid and then titrated with a standard solution of hydrochloric acid.
- -
- Fat (Soxhlet method): The method consisted of an extraction with ethyl ether. The solvent was then evaporated, and the residue weighed.
- -
- Dietary fibre (enzymatic-gravimetric method): The method consisted of etching the degreased sample successively with thermo-resistant α-amylase, protease, and amyloglucosidase. After precipitation of the soluble fibre, the undigested parts were determined by weight.
2.2. Study Design and Participant Characteristics
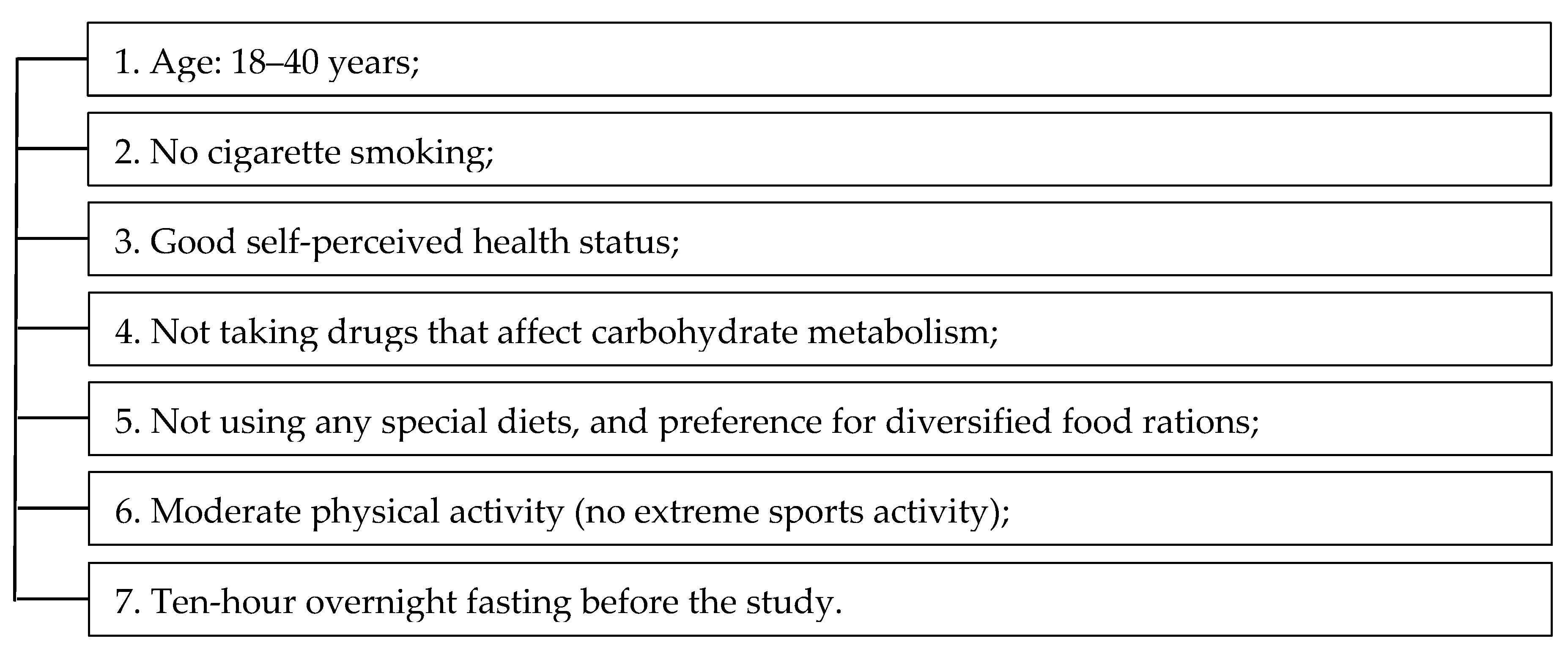
2.2.1. Stage I: Recruitment
2.2.2. Stage II: Anthropometric Measurements and Filling in the Questionnaire
2.2.3. Stage III: Completion of 24-h Dietary Diaries
2.2.4. Stage IV: Fasting Glucose Measurement
2.2.5. Stage V: Oral Glucose Tolerance Test (OGTT)
2.3. Administration of Test Meals and GI Determination of Meals
2.4. Statistical Analysis
3. Results
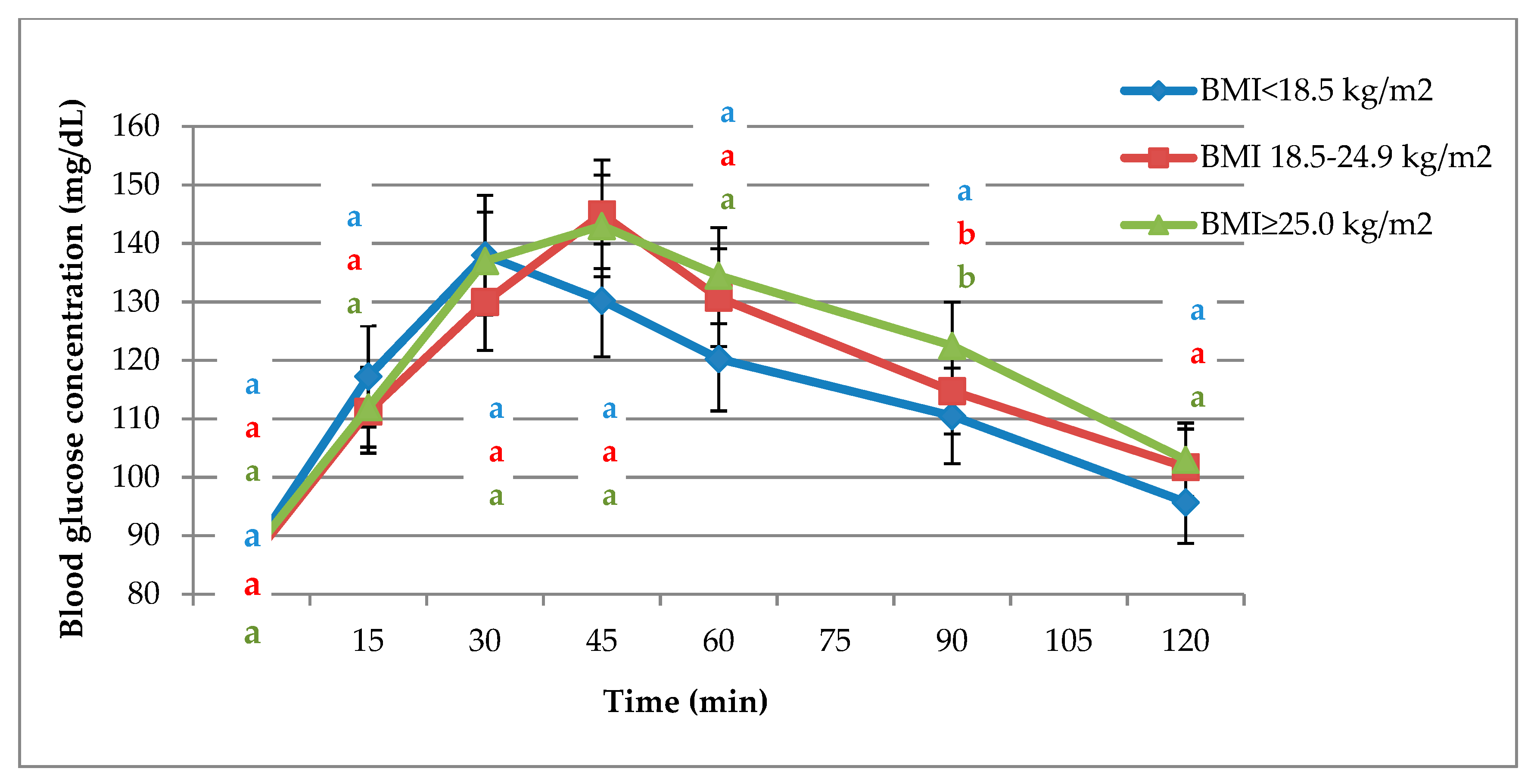
3.1. Glycaemic Responses to OGTT and the Tested Meals
3.2. GI of the Tested Meals
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mitchell, H.L. The glycemic index concept in action. Am. J. Clin. Nutr. 2008, 87, 244S–246S. [Google Scholar] [CrossRef] [PubMed]
- Wolever, T.M.S. Physiological mechanisms and observed health impacts related to the glycaemic index: Some observations. Int. J. Obes. 2006, 30, S72–S78. [Google Scholar] [CrossRef]
- Venn, B.J.; Green, T.J. Glycemic index and glycemic load: Measurement issues and their effect on diet–disease relationships. Eur. J. Clin. Nutr. 2007, 61, S122–S131. [Google Scholar] [CrossRef] [PubMed]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary glycemic index and load and the risk of type 2 diabetes: A systematic review and updated meta-analyses of prospective cohort studies. Nutrients 2019, 11, 1280. [Google Scholar] [CrossRef] [PubMed]
- Karpe, F.; Dickmann, J.R.; Frayn, K.N. Fatty acids, obesity and insulin resistance: Time for a reevaluation. Diabetes 2011, 60, 2441–2449. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Agrawal, M.K.; Kumari, T.; Kumar, S. Correlation between body mass index and blood glucose levels in Jharkhand population. Int. J. Contemp. Med. Res. 2017, 4, 1633–1636. [Google Scholar]
- Ritchie, S.A.; Connell, J.M.C. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Snijder, M.B.; Dekker, J.M.; Visser, M.; Yudkin, J.S.; Stehouwer, C.D.A.; Bouter, L.M.; Heine, R.J.; Nijpels, G.; Seidell, J.C. Larger thigh and hip circumferences are associated with better glucose tolerance: The Hoorn study. Obes. Res. 2003, 11, 104–111. [Google Scholar] [CrossRef]
- Snijder, M.B.; Dekker, J.M.; Visser, M.; Bouter, L.M.; Stehouwer, C.D.A.; Yudkin, J.S.; Heine, R.J.; Nijpels, G.; Seidell, J.C. Trunk fat and leg fat have independent and opposite associations with fasting and postload glucose levels: The Hoorn study. Diabetes Care 2004, 27, 372–377. [Google Scholar] [CrossRef]
- Brochu, M.; Tchernof, A.; Dionne, I.J.; Sites, C.K.; Eltabbakh, G.H.; Sims, E.A.H.; Poehlman, E.T. What are the physical characteristics associated with a normal metabolic profile despite a high level of obesity in postmenopausal women? J. Clin. Endocrinol. Metab. 2001, 86, 1020–1025. [Google Scholar] [CrossRef]
- Borczak, B.; Sikora, M.; Sikora, E.; Dobosz, A.; Kapusta-Duch, J. Glycaemic index of wheat bread. Starch/Stärke 2018, 70, 1700022. [Google Scholar] [CrossRef]
- Zeinali, F.; Samani, H.A.; Toupchian, O.; Abdollahi, S.; Samadi, M. A review of the relationship between dietary glycemic index and glycemic load and type 2 diabetes. J. Nutr. Food Secur. 2016, 1, 73–79. [Google Scholar]
- Pérez-Quirce, S.; Lazaridou, A.; Biliaderis, C.G.; Ronda, F. Effect of β-glucan molecular weight on rice flour dough rheology, quality parameters of breads and in vitro starch digestibility. LWT-Food Sci. Technol. 2017, 82, 446–453. [Google Scholar] [CrossRef]
- Lu, J.; Shan, L.; Xie, Y.; Min, F.; Gao, J.; Guo, L.; Ren, C.; Yuan, J.; Gilissen, L.; Chen, H. Effect of fermentation on content, molecule weight distribution and viscosity of β-glucans in oat sourdough. Int. J. Food Sci. Technol. 2019, 54, 62–67. [Google Scholar] [CrossRef]
- Elmaliklis, N.; Liveri, A.; Ntelis, B.; Paraskeva, K.; Goulis, I.; Koutelidakis, A.E. Increased functional foods’ consumption and Mediterranean diet adherence may have a protective effect in the appearance of gastrointestinal diseases: A case-control study. Medicines 2019, 6, 50. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, M.D.; Iriondo-DeHond, A.; Martirosyan, D.M. Are functional foods essential for sustainable health? Ann. Nutr. Food Sci. 2018, 2, 1015. [Google Scholar]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Bressiani, J.; Oro, T.; Santetti, G.S.; Almeida, J.L.; Bertolin, T.E.; Gómez, M.; Gutkoski, L.C. Properties of whole grain wheat flour and performance in bakery products as a function of particle size. J. Cereal Sci. 2017, 75, 269–277. [Google Scholar] [CrossRef]
- Gronowska-Senger, A. Analiza Żywności. Zbiór Ćwiczeń [Food Analysis. Collection of Exercises]; SGGW: Warsaw, Poland, 2010; ISBN 978-83-7583-224-2. (In Polish) [Google Scholar]
- Horwitz, W.; Latimer, G., Jr. Methods of Analysis of AOAC International, 18th ed.; Association of Official Analytical Chemists: Arlington, VA, USA, 2005; ISBN 978-09-3558-475-2. [Google Scholar]
- International Standards Organisation. ISO 26642:2010. Food Products—Determination of the Glycaemic Index (GI) and Recommendation for Food Classification; International Standards Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Agriculture and Consumer Protection Department, Food and Agriculture Organization of the United Nations. Carbohydrates in Human Nutrition. In Proceedings of the Joint FAO/WHO Expert Consultation; FAO Food and Nutrition Paper No. 66; FAO: Rome, Italy, 1997; ISBN 92-5-104114-8. [Google Scholar]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef]
- O’Grady, J.; O’Connor, E.M.; Shanahan, F. Review article: Dietary fibre in the era of microbiome science. Aliment Pharmacol. Ther. 2019, 49, 506–515. [Google Scholar] [CrossRef]
- Kristek, A.; Schär, M.Y.; Soycan, G.; Alsharif, S.; Kuhnle, G.G.C.; Walton, G.; Spencer, J.P.E. The gut microbiota and cardiovascular health benefits: A focus on wholegrain oats. Nutr. Bull. 2018, 43, 358–373. [Google Scholar] [CrossRef] [Green Version]
- Călinoiu, L.F.; Vodnar, D.C. Whole grains and phenolic acids: A review on bioactivity, functionality, health benefits and bioavailability. Nutrients 2018, 10, 1615. [Google Scholar] [CrossRef] [PubMed]
- Kurek, M.A.; Wyrwisz, J.; Karp, S.; Wierzbicka, A. Effect of fiber sources on fatty acids profile, glycemic index, and phenolic compound content of in vitro digested fortified wheat bread. J. Food Sci. Technol. 2018, 55, 1632–1640. [Google Scholar] [CrossRef] [PubMed]
- Matthan, N.R.; Ausman, L.M.; Meng, H.; Tighiouart, H.; Lichtenstein, A.H. Estimating the reliability of glycemic index values and potential sources of methodological and biological variability. Am. J. Clin. Nutr. 2016, 104, 1004–1013. [Google Scholar] [CrossRef]
- Dolna, A.; Ciok, J.; Szponar, L. Oznaczenie indeksu glikemicznego wybranych potraw typowych dla kuchni polskiej [Determination of glycemic index value of selected dishes typical of Polish cuisine]. Żywienie Człowieka Metab. 2006, 33, 199–211. [Google Scholar]
- Jiang, H.; Hettiararchchy, N.S.; Horax, R. Physical properties and estimated glycemic index of protein-enriched sorghum based chips. J. Food Sci. Technol. 2018, 55, 891–898. [Google Scholar] [CrossRef]
- Wolever, T.M.S.; Vorster, H.H.; Björck, I.; Brand-Miller, J.; Brighenti, F.; Mann, J.I.; Ramdath, D.D.; Granfeldt, Y.; Holt, S.; Perry, T.L.; et al. Determination of the glycaemic index of foods: Interlaboratory study. Eur. J. Clin. Nutr. 2003, 57, 475–482. [Google Scholar] [CrossRef]
- Basu, R.; Breda, E.; Oberg, A.L.; Powell, C.C.; Dalla, M.C.; Basu, A.; Vittone, J.L.; Klee, G.G.; Arora, P.; Jensen, M.D.; et al. Mechanisms of the age-associated deterioration in glucose tolerance: Contribution of alterations in insulin secretion, action, and clearance. Diabetes 2003, 52, 1738–1748. [Google Scholar] [CrossRef]
- Mikołajewska, A.; Jasińska, M.; Paradowski, L. Oznaczanie elastazy trzustkowej w kale w diagnostyce czynności zewnątrzwydzielniczej trzustki [Determination of pancreatic elastase in the feces in the diagnosis of pancreatic exocrine]. Pol. Gastroenterol. 2002, 9, 225–229. [Google Scholar]
- Teichmann, J.; Riemann, J.F.; Lange, U. Prevalence of exocrine pancreatic insufficiency in women with obesity syndrome: Assessment by pancreatic fecal elastase 1. ISRN Gastroenterol. 2011, 2011, 951686. [Google Scholar] [CrossRef]
- Pereda, J.; Pérez, S.; Escobar, J.; Arduini, A.; Asensi, M.; Serviddio, G.; Sabater, L.; Aparisi, L.; Sastre, J. Obese rats exhibit high levels of fat necrosis and isoprostanes in taurocholate-induced acute pancreatitis. PLoS ONE 2012, 7, e44383. [Google Scholar] [CrossRef] [PubMed]
- Chasapi, A.; Balampanis, K.; Kourea, E.; Kalfarentzos, F.; Lambadiari, V.; Lambrou, G.I.; Melachrinou, M.; Sotiropoulou-Bonikou, G. Can obesity-induced inflammation in skeletal muscle and intramuscular adipose tissue accurately detect liver fibrosis? J. Musculoskelet. Neuronal Interact. 2018, 18, 509–524. [Google Scholar] [PubMed]
- Knight, K. The biology of fat. J. Exp. Biol. 2018, 221, jeb178020. [Google Scholar] [CrossRef] [Green Version]
- Lê, K.A.; Ventura, E.E.; Fisher, J.Q.; Davis, J.N.; Weigensberg, M.J.; Punyanitya, M.; Hu, H.H.; Nayak, K.S.; Goran, M.I. Ethnic differences in pancreatic fat accumulation and its relationship with other fat depots and inflammatory markers. Diabetes Care 2011, 34, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.; Lee, H.I.; Ko, A.; Lee, H.G. Substituting whole grain flour for wheat flour: Impact on cake quality and glycemic index. Food Sci. Biotechnol. 2013, 22, 1–7. [Google Scholar] [CrossRef]
- Ferrer-Mairal, A.; Peñalva-Lapuente, C.; Iglesia, I.; Urtasun, L.; De Miguel-Etayo, P.; Remón, S.; Cortés, E.; Moreno, L.A. In vitro and in vivo assessment of the glycemic index of bakery products: Influence of the reformulation of ingredients. Eur. J. Nutr. 2012, 51, 947–954. [Google Scholar] [CrossRef]
- Raczkowska, E.; Łoźna, K.; Bienkiewicz, M.; Jurczok, K.; Bronkowska, M. Relation between the recipe of yeast dough dishes and their glycaemic indices and loads. Foods 2019, 8, 377. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | BMI < 18.5 kg/m2 (n = 32) | BMI 18.5–24.9 kg/m2 (n = 34) | BMI ≥ 25.0 kg/m2 (n = 39) | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | |
| age (years) | 23.70 ± 1.76 | 20.00–27.00 | 24.20 ± 0.55 | 23.00–26.00 | 23.30 ± 1.12 | 21.00–26.00 |
| body weight (kg) | 48.54 ± 3.07 | 41.73–54.64 | 63.54 ± 9.28 | 49.64–93.92 | 76.82 ± 10.36 | 64.05–99.02 |
| height (m) | 1.65 ± 0.04 | 1.55–1.73 | 1.68 ± 0.09 | 1.53–1.95 | 1.66 ± 0.07 | 1.53–1.84 |
| BMI (kg/m2) | 17.82 ± 0.59 | 15.72–18.41 | 22.3 ± 1.53 | 20.02–24.83 | 28.01 ± 3.10 | 25.04–36.52 |
| fasting glucose (mg/dL) | 83.00 ± 0.10 | 78.00–94.00 | 81.00 ± 0.20 | 73.00–88.00 | 81.00 ± 0.10 | 78.00–94.00 |
| gender (female/male) | 28/4 | - | 29/5 | - | 30/9 | - |
| Place of residence (persons): | ||||||
| city ≥ 300,000 inhabitants | 25 | - | 22 | - | 27 | - |
| city 100,000–300,000 inhabitants | 4 | - | 3 | - | 2 | - |
| city 10,000–100,000 inhabitants | 2 | - | 5 | - | 1 | - |
| city ≤ 10,000 inhabitants | 0 | - | 1 | - | 5 | - |
| village | 1 | - | 3 | - | 4 | - |
| Week | Monday | Tuesday | Wednesday |
|---|---|---|---|
| BMI Group 1 (n =32) | BMI Group 2 (n = 34) | BMI Group 3 (n = 39) | |
| 1 | OGTT | OGTT | OGTT |
| 2 | T1 (n = 10), T2 (n = 12), T3 (n = 10) | T1 (n = 10), T2 (n = 12), T3 (n = 12) | T1 (n = 13), T2 (n = 11), T3 (n = 15) |
| 3 | M1 (n = 10), M2 (n = 12), M3 (n = 10) | M1 (n = 10), M2 (n = 12), M3 (n = 12) | M1 (n = 13), M2 (n = 11), M3 (n = 15) |
| 4 | OGTT | OGTT | OGTT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raczkowska, E.; Bronkowska, M. The Effect of the Body Mass Indexes of Young Healthy Individuals on the Glyacemic Indexes of Traditional and Modified Vegetarian Meals. Nutrients 2019, 11, 2546. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102546
Raczkowska E, Bronkowska M. The Effect of the Body Mass Indexes of Young Healthy Individuals on the Glyacemic Indexes of Traditional and Modified Vegetarian Meals. Nutrients. 2019; 11(10):2546. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102546
Chicago/Turabian StyleRaczkowska, Ewa, and Monika Bronkowska. 2019. "The Effect of the Body Mass Indexes of Young Healthy Individuals on the Glyacemic Indexes of Traditional and Modified Vegetarian Meals" Nutrients 11, no. 10: 2546. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11102546