Association between Iodine Nutrition Status and Thyroid Disease-Related Hormone in Korean Adults: Korean National Health and Nutrition Examination Survey VI (2013–2015)


Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Population
2.2. Measurement of TSH, FT4, and UIC
2.3. Estimated Iodine Intake
2.4. Establishment of Iodine Database of Commercial Foods in Korea
2.5. Measurement of Dietary Iodine Intake Using 24-hr-Dietary Recall
2.6. Statistics
3. Results
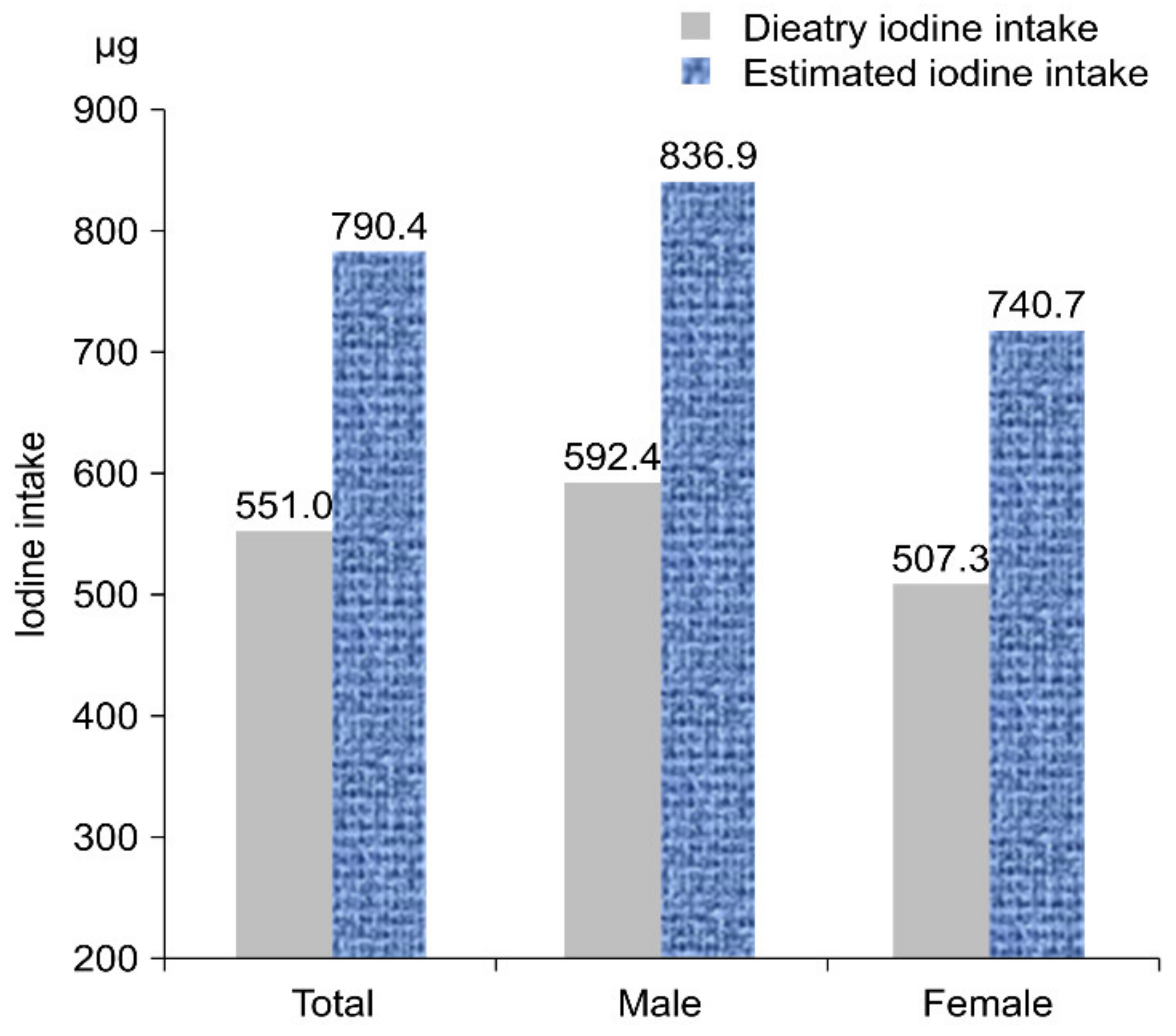
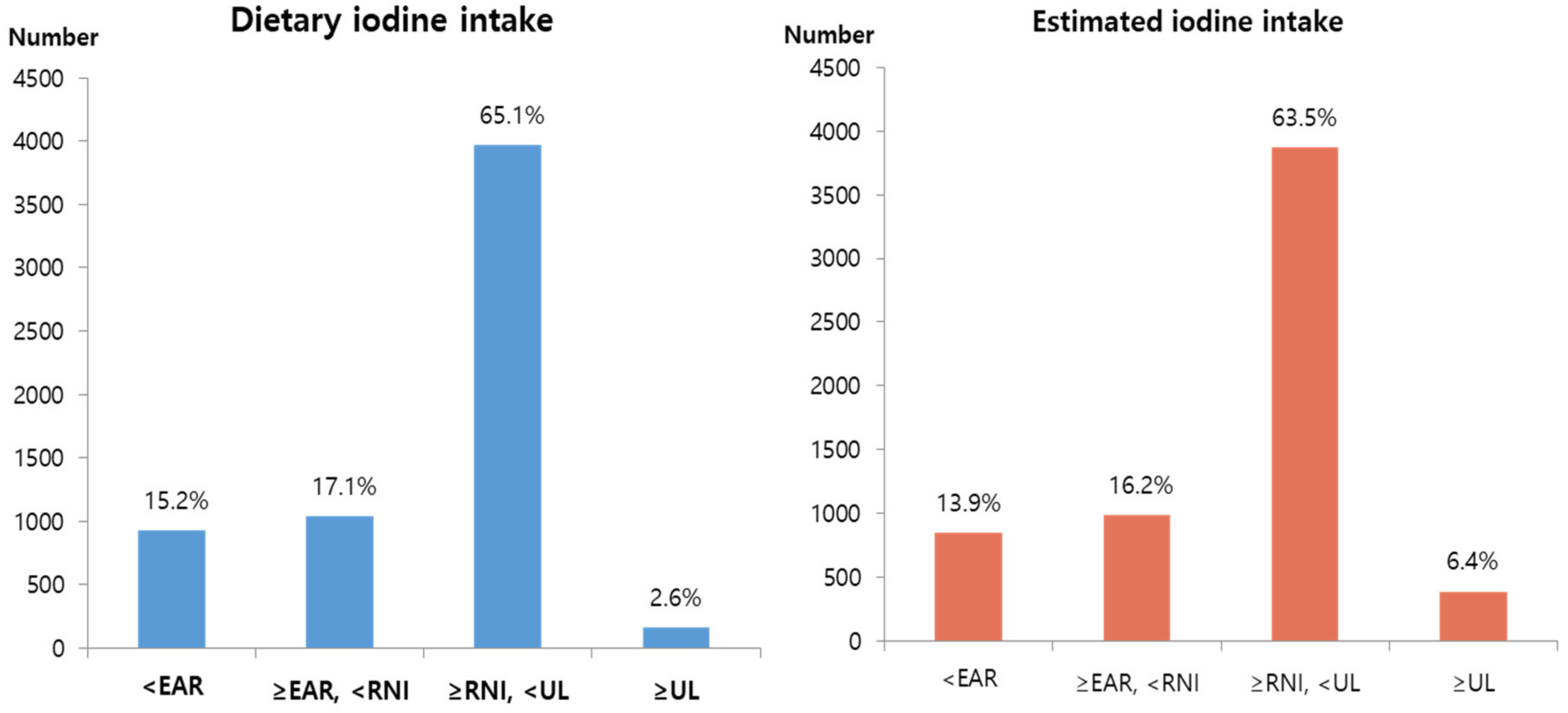
3.1. Iodine Nutrition Status
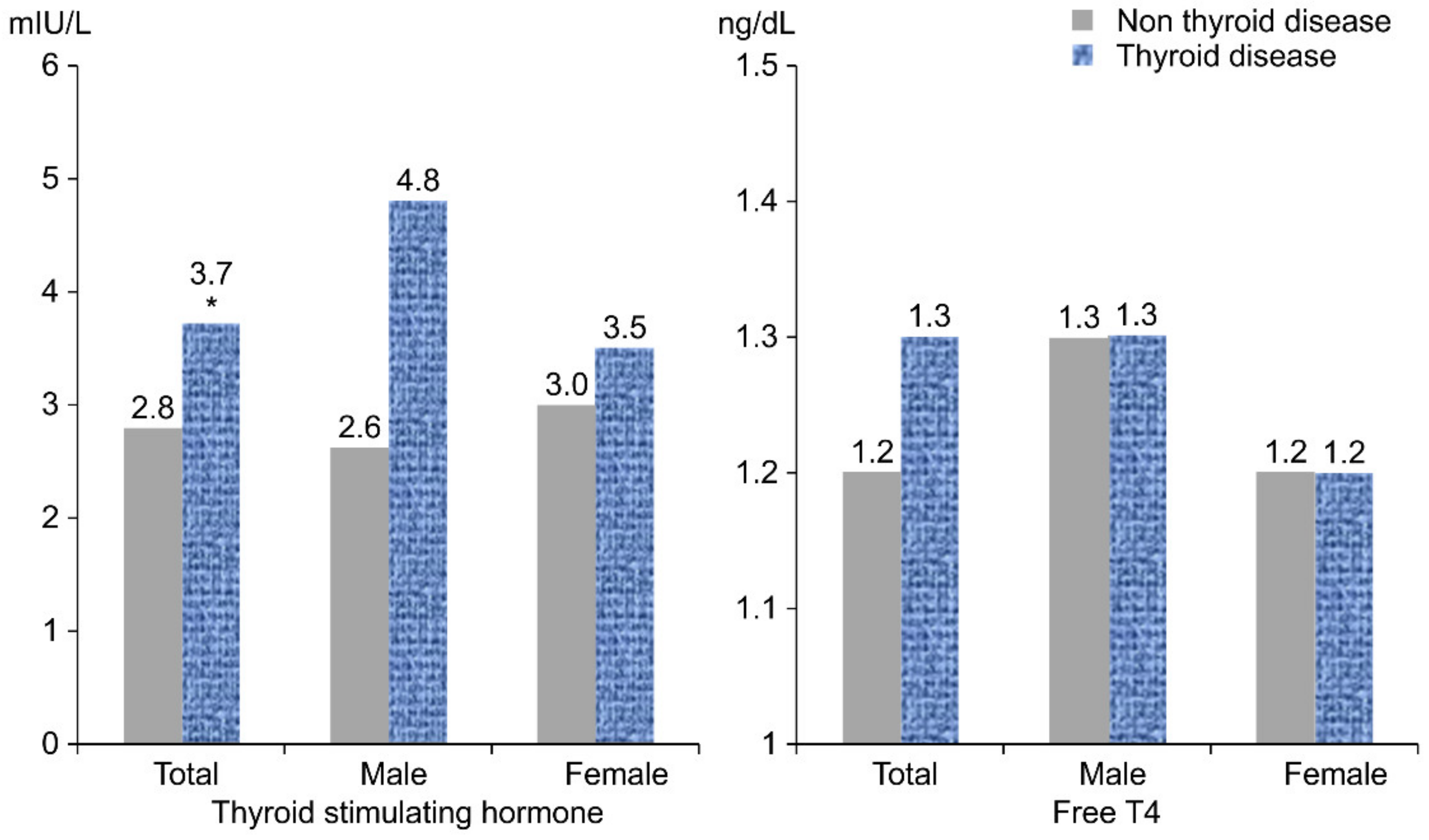
3.2. TSH and FT4 of the Subjects
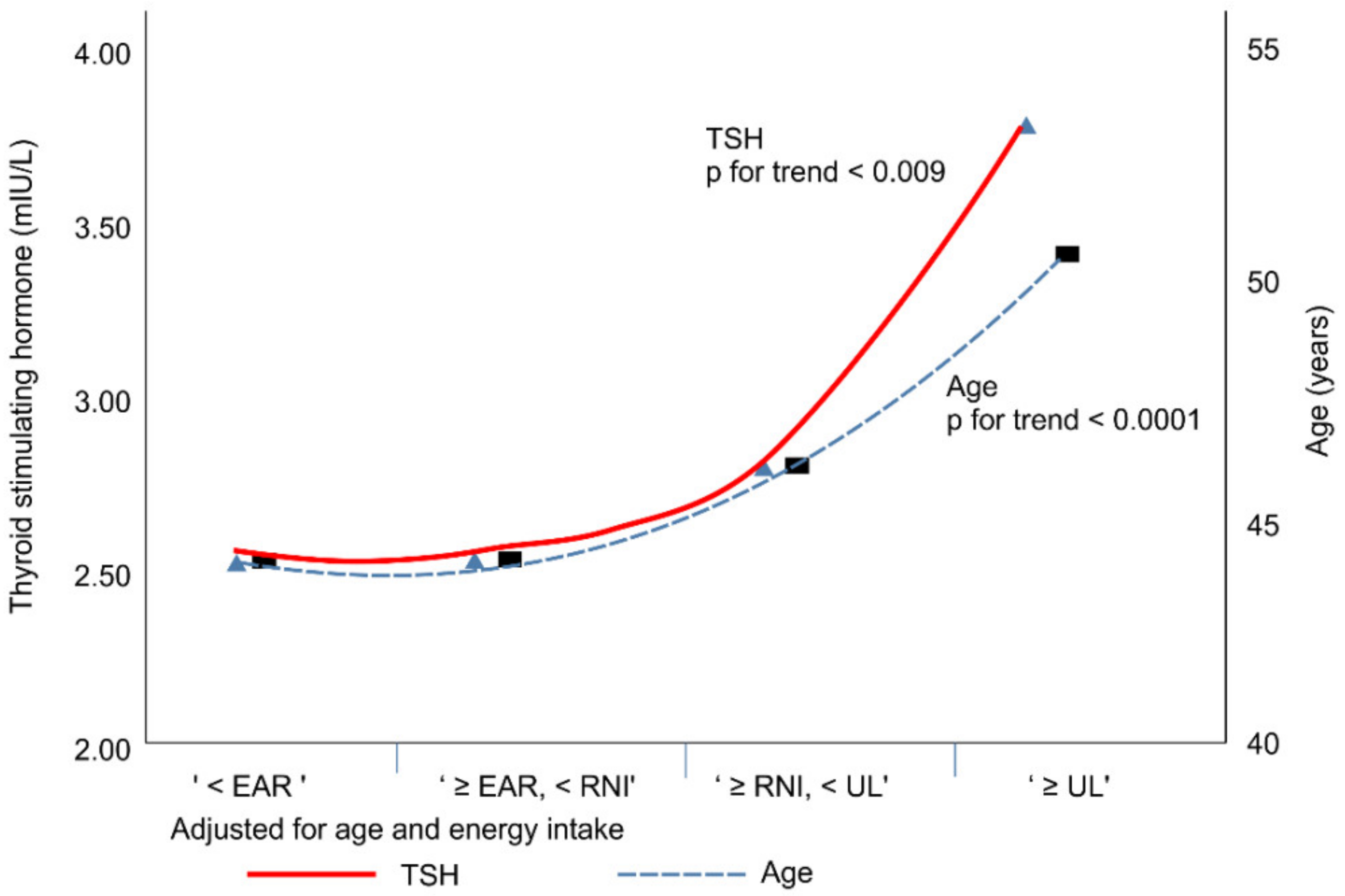
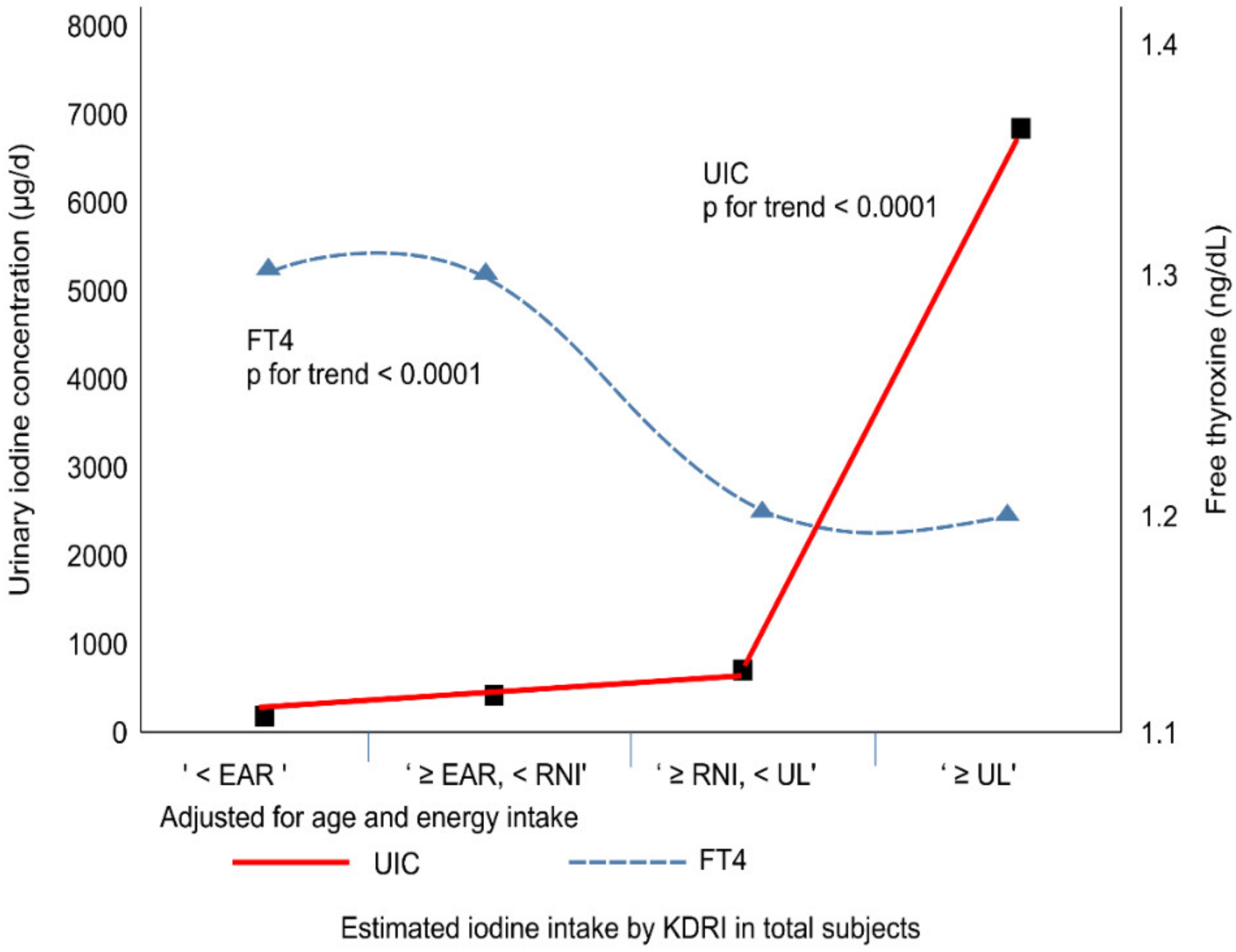
3.3. UIC, TSH, and FT4 According to KDRI of the Estimated Iodine Intake
3.4. Prevalence of Thyroid Disease and Distribution of Iodine Intake According to the Estimated Iodine Intake by KDRI
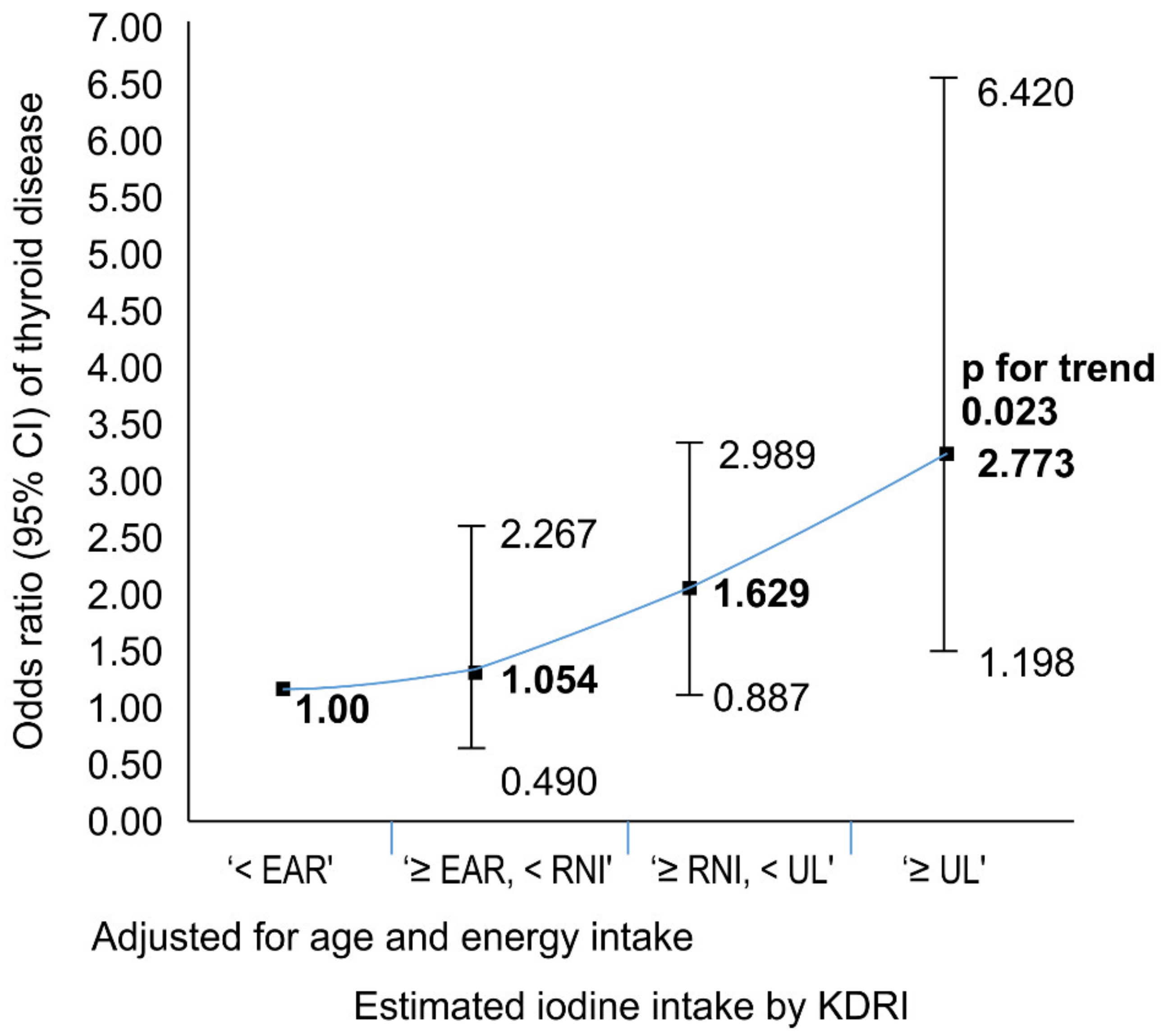
3.5. Relation between Thyroid Disease and the Estimated Iodine Intake by KDRI
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Korean Food & Drug Administration. Report on the Intake of Sugar, Sodium, and the Rest of Korean; Korean Food & Drug Administration: Cheongju, Korea, 2007. [Google Scholar]
- Han, M.R.; Ju, D.L.; Park, Y.J.; Paik, H.Y.; Song, Y. An iodine database for common Korean foods and the association between iodine intake and thyroid disease in Korean adults. Int. J. Thyroidol. 2015, 8, 170–182. [Google Scholar] [CrossRef]
- Ko, Y.M.; Kwon, Y.S.; Park, Y.K. An iodine database establishment and iodine intake in Korean adults: Based on the 1998~2014 Korea National Health and Nutrition Examination Survey. J. Nutr. Health 2017, 50, 624–644. [Google Scholar] [CrossRef]
- The Korean Nutrition Society. Dietary Reference Intakes for Koreans; The Korean Nutrition Society: Seoul, Korea, 2010. [Google Scholar]
- Choi, J.; Kim, H.S.; Hong, D.J.; Lim, H.; Kim, J.H. Urinary iodine and sodium status of urban Korean subjects: A pilot study. Clin. Biochem. 2012, 45, 596–598. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Molybdenum, Nickel, Silicon, Vanadium and Zinc. Food and Nutrition Board; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Hwang, S.; Lee, E.Y.; Lee, W.K.; Shin, D.Y.; Lee, E.J. Correlation between iodine intake and thyroid function in subjects with normal thyroid function. Biol. Trace Elem. Res. 2011, 143, 1393–1397. [Google Scholar] [CrossRef]
- Lee, H.S.; Min, H. Iodine intake and tolerable upper intake level of iodine for Koreans. Korean J. Nutr. 2011, 44, 82–91. [Google Scholar] [CrossRef]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; Rasmussen, L.B.; Perrild, H.; Andersen, S.; Pedersen, I.B.; Carlé, A. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 13–27. [Google Scholar] [CrossRef]
- Braverman, L.E. Iodine and the thyroid: 33 years of study. Thyroid 1994, 4, 351–356. [Google Scholar] [CrossRef]
- Roti, E.; Uberti, E.D. Iodine excess and hyperthyroidism. Thyroid 2001, 11, 493–500. [Google Scholar] [CrossRef]
- Laurberg, P.; Bulow Pedersen, I.; Knudsen, N.; Ovesen, L.; Andersen, S. Environmental iodine intake affects the type of nonmalignant thyroid disease. Thyroid 2001, 11, 457–469. [Google Scholar] [CrossRef]
- Burgi, H. Iodine excess. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 107–115. [Google Scholar] [CrossRef]
- Clark, O.H. Excess iodine intake and thyroid function and growth. Thyroid 1990, 1, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Shan, Z.; Teng, W. Effects of increased iodine intake on thyroid disorders. Endocrinol. Metab. 2014, 29, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: Past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M. Iodine deficiency and excess in children: Worldwide status in 2013. Endocr. Pract. 2013, 19, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.S.; Burch, H.B.; Cooper, D.S.; Greenlee, M.C.; Laurberg, P.; Maia, A.L.; Rivkees, S.A.; Samuels, M.; Sosa, J.A.; Stan, M.N.; et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 2016, 26, 1343–1421. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, M.T. Biochemical testing of the thyroid: TSH is the best and, oftentimes, only test needed—A review for primary care. Clin. Med. Res. 2016, 14, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Korevaar, T.I.; Medici, M.; Uitterlinden, A.G.; Hofman, A.; Dehghan, A.; Franco, O.H.; Peeters, R.P. Thyroid function characteristics and determinants: The Rotterdam study. Thyroid 2016, 26, 1195–1204. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Korea National Health and Nutrition Examination Survey (KNHANES VI). 2016. Available online: https://knhanes.cdc.go.kr/knhanes/main.do 2016.
- Kim, W.G.; Kim, W.B.; Woo, G.; Kim, H.; Cho, Y.; Kim, T.Y.; Kim, S.W.; Shin, M.-H.; Park, J.W.; Park, H.-L.; et al. Thyroid stimulating hormone reference range and prevalence of thyroid dysfunction in the Korean population: Korea National Health and Nutrition Examination Survey 2013 to 2015. Endocrinol. Metab. 2017, 32, 106–114. [Google Scholar] [CrossRef]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2014, 10, 136. [Google Scholar] [CrossRef]
- Kim, H.I.; Oh, H.K.; Park, S.Y.; Jang, H.W.; Shin, M.H.; Kim, S.W.; Kim, T.H.; Chung, J.H. Urinary iodine concentration and thyroid hormones: Korea National Health and Nutrition Examination Survey 2013–2015. Eur. J. Nutr. 2019, 58, 233–240. [Google Scholar] [CrossRef]
- The Korean Nutrition Society. Food Values; The Korean Nutrition Society: Seoul, Korea, 2009. [Google Scholar]
- National Rural Resources Development Institute. Administration RD 9th Revision; Rural Development Administration: Jeonju, Korea, 2018. [Google Scholar]
- Ministry of Education, Culture, Sports, Science and Technology. Japan Standard Tables of Food Composition in Japan; Seventh Revised Version; Ministry of Education, Culture, Sports, Science and Technology: Tokyo, Japan, 2015.
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S.; Commins, J.M.; Moler, J.E.; Willett, W.; Tinker, L.F.; Subar, A.F.; Spiegelman, D.; Rhodes, D.; Potischman, N.; Neuhouser, M.L. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for potassium and sodium intake. Am. J. Epidemiol. 2015, 181, 473–487. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Woeber, K.A. Iodine and thyroid disease. Med. Clin. N. Am. 1991, 75, 169–178. [Google Scholar] [CrossRef]
- Winichagoon, P.; Svasti, S.; Munkongdee, T.; Chaiya, W.; Boonmongkol, P.; Chantrakul, N.; Fucharoen, S. Rapid diagnosis of thalassemias and other hemoglobinopathies by capillary electrophoresis system. Transl. Res. 2008, 152, 178–184. [Google Scholar] [CrossRef]
- World Health Organization. Urinary Iodine Concentrations for Determining Iodine Status in Populations; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Nath, S.; Moinier, B.; Thuillier, F.; Rongier, M.; Desjeux, J. Urinary excretion of iodide and fluoride from supplemented food grade salt. Int. J. Vitam. Nutr. Res. 1992, 62, 66–72. [Google Scholar]
- Jolin, T.; Escobar, D.R. Evaluation of iodine/creatinine ratios of casual samples as indices of daily urinary iodine output during field studies. J. Clin. Endocrinol. Metab. 1965, 25, 540–542. [Google Scholar] [CrossRef]
- Kim, H.; Lee, H.; Park, K.; Joo, H.; Kim, K.; Hong, C.; Huh, K.; Lee, S.; Ryu, K. A study on the urinary iodide excretion in normal subjects and patients with thyroid disease. Korean J. Intern. Med. 1985, 29, 625–631. [Google Scholar]
- Kim, J.Y.; Kim, K.R. Dietary iodine intake and urinary iodine excretion in patients with thyroid diseases. Yonsei Med. J. 2000, 41, 22–28. [Google Scholar] [CrossRef]
- Kim, J.Y.; Moon, S.J.; Kim, K.R.; Sohn, C.Y.; Oh, J.J. Dietary iodine intake and urinary iodine excretion in normal Korean adults. Yonsei Med. J. 1998, 39, 355–362. [Google Scholar] [CrossRef]
- Haymart, M.R.; Glinberg, S.L.; Liu, J.; Sippel, R.S.; Jaume, J.C.; Chen, H. Higher serum TSH in thyroid cancer patients occurs independent of age and correlates with extrathyroidal extension. Clin. Endocrinol. 2009, 71, 434–439. [Google Scholar] [CrossRef]
- Hadlow, N.C.; Rothacker, K.M.; Wardrop, R.; Brown, S.J.; Lim, E.M.; Walsh, J.P. The relationship between TSH and free T4 in a large population is complex and monlinear and differs by age and sex. J. Clin. Endocrinol. Metab. 2013, 98, 2936–2943. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.K.; Kim, J.E.; Oh, H.J.; Park, K.S.; Kim, S.K.; Park, S.W.; Kim, M.J.; Cho, Y.W. Serum TSH level in healthy Koreans and the association of TSH with serum lipid concentration and metabolic syndrome. Korean J. Intern. Med. 2011, 26, 432–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollowell, J.G.; Staehling, N.W.; Flanders, W.D.; Hannon, W.H.; Gunter, E.W.; Spencer, C.A.; Braverman, L.E. Serum TSH, T4, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J. Clin. Endocrinol. Metab. 2002, 87, 489–499. [Google Scholar] [CrossRef]
- Ishii, K.; Hayashi, A.; Tamaoka, A.; Mizusawa, H.; Shoji, S. A case of Hashimoto′s encephalopathy with a relapsing course related to menstrual cycle. Clin. Neurol. 1993, 33, 995–997. [Google Scholar]
- Leo, V.D.; D′Antona, D.; Lanzetta, D. Thyrotropin secretion before and after ovariectomy in premenopausal women. Gynecol. Endocrinol. 1993, 7, 279–283. [Google Scholar] [CrossRef]
- Fujimoto, N.; Watanabe, H.; Ito, A. Blockade of the estrogen induced increase in progesterone receptor caused by propylthiouracil, an anti-thyroid drug, in a transplantable pituitary tumor in rats. Endocr. J. 1996, 43, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Ogard, C.G.; Ogard, C.; Almdal, T.P. Thyroid-associated orbitopathy developed during hormone replacement therapy. Acta Ophthalmol. Scand. 2001, 79, 426–427. [Google Scholar] [CrossRef]
- Abalovich, M.; Gutierrez, S.; Alcaraz, G.; Maccallini, G.; Garcia, A.; Levalle, O. Overt and subclinical hypothyroidism complicating pregnancy. Thyroid 2002, 12, 63–68. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 6095) | Unadjusted p-Value a | Adjusted p-Value a,b | Male (n = 2852) | Unadjusted p-Value | Adjusted p-Value | Female (n = 3243) | Unadjusted p-Value | Adjusted p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Thyroid Disease (n = 5908) | Thyroid Disease (n = 187) | Non-Thyroid Disease (n = 2827) | Thyroid Disease (n = 25) | Non-Thyroid Disease (n = 3081) | Thyroid Disease (n = 162) | |||||||
| Mean ± SE | Mean ± SE | Mean ± SE | Mean ± SE | Mean ± SE | Mean ± SE | |||||||
| Dietary Iodine (μg/day) | 554.0 ± 35.8 | 458.8 ± 93.6 | 0.348 | 0.483 | 592.9 ± 60.0 | 533.2 ± 190.8 | 0.766 | 0.715 | 510.9 ± 34.3 | 445.8 ± 101.5 | 0.547 | 0.502 |
| Estimated Iodine (μg/day) | 780.0 ± 56.1 | 1108.1 ± 195.8 | 0.107 | 0.162 | 837.5 ± 97.8 | 775.7 ± 241.2 | 0.813 | 0.624 | 716.4 ± 39.0 | 1166.3 ± 226.2 | 0.051 | 0.067 |
| UIC c (μg/L) | 883.2 ± 92.1 | 1085.9 ± 183.9 | 0.322 | 0.400 | 913.5 ± 164.5 | 745.1 ± 235.8 | 0.558 | 0.462 | 849.8 ± 52.5 | 1145.5 ± 211.5 | 0.172 | 0.195 |
| Estimated Iodine Intake (µg/day) | Korean Dietary Reference Intakes (KDRI) | Unadjusted p for Trend d | Adjusted p for Trend d,e | |||
|---|---|---|---|---|---|---|
| <EAR a (<95) (n = 850) | ≥EAR, <RNI b (≥95, <150) (n = 987) | ≥RNI, <UL c (≥150, 2400) (n = 3869) | ≥UL (≥2400) (n = 389) | |||
| Mean ± SE | Mean ± SE | Mean ± SE | Mean ± SE | |||
| Total | ||||||
| Age | 44.3 ± 0.8 | 44.4 ± 0.6 | 46.8 ± 0.3 | 50.7 ± 0.9 | <.0001(+) | <.0001(+) |
| TSH (mIU/L) | 2.5 ± 0.1 | 2.5 ± 0.1 | 2.8 ± 0.1 | 3.7 ± 0.4 | 0.008(+) | 0.009(+) |
| UIC (μg/L) | 111.1 ± 2.6 | 168.5 ± 3.4 | 632.6 ± 13.6 | 6903.2 ± 1202.3 | <.0001(+) | <.0001(+) |
| FT4 (ng/dL) | 1.3 ± 0.01 | 1.3 ± 0.01 | 1.2 ± 0.005 | 1.2 ± 0.01 | <.0001(−) | <.0001(−) |
| Male | ||||||
| Age | 41.7 ± 1.1 | 42.8 ± 0.8 | 45.6 ± 0.3 | 50.1 ± 1.1 | <.0001(+) | <.0001(+) |
| TSH (mIU/L) | 2.1 ± 0.1 | 2.3 ± 0.1 | 2.6 ± 0.1 | 4.0 ± 0.7 | 0.024(+) | 0.024(+) |
| UIC (μg/L) | 109.8 ± 3.5 | 154.8 ± 3.9 | 580.0 ± 15.4 | 7404.0 ± 2222.9 | 0.002(+) | 0.002(+) |
| FT4 (ng/dL) | 1.3 ± 0.01 | 1.3 ± 0.0 | 1.3 ± 0.01 | 1.2 ± 0.02 | <.0001(−) | 0.002(−) |
| Female | ||||||
| Age | 46.0 ± 0.9 | 45.9 ± 0.8 | 48.3 ± 0.4 | 51.3 ± 1.3 | 0.002(+) | 0.003(+) |
| TSH (mIU/L) | 2.8 ± 0.1 | 2.8 ± 0.1 | 3.1 ± 0.1 | 3.4 ± 0.2 | 0.062(+) | 0.079(+) |
| UIC (μg/L) | 112.0 ± 3.3 | 181.6 ± 5.2 | 694.9 ± 21.6 | 6350.5 ± 597.7 | <.0001(+) | <.0001(+) |
| FT4 (ng/dL) | 1.2 ± 0.01 | 1.2 ± 0.01 | 1.2 ± 0.01 | 1.1 ± 0.01 | 0.0001(−) | 0.001(−) |
| Estimated Iodine Intake (µg/day) | Korean Dietary Reference Intake (KDRI) a | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| <EARc (<95) | ≥EAR, <RNI d (≥95, <150) | ≥RNI, <UL e (≥150, 2400) | ≥UL (≥2400) | Total | |||||
| Total | n = 850 | n = 987 | n = 3869 | n = 389 | n = 6095 | ||||
| Intake Range | 1.29–94.99 | 95.01–149.95 | 150.02–2399.36 | 2409.77–80672.0 | 1.29–80672.0 | ||||
| Median ± SE b | 72.0 ± 1.2 | 122.5 ± 1.1 | 362.5 ± 7.1 | 4102.9 ± 152.3 | 256.4 ± 5.5 | ||||
| Mean ± SE | 69.4 ± 0.8 | 122.2 ± 0.6 | 558.0 ± 9.7 | 6301.4 ± 672.7 | 790.1 ± 54.7 | ||||
| Prevalence of Thyroid Disease (n, weighted %) | |||||||||
| Non-Thyroid Disease | 830 | 97.2 | 964 | 97.6 | 3744 | 96.9 | 370 | 94.4 | 5908 |
| Thyroid Disease | 20 | 2.8 | 23 | 2.4 | 125 | 3.1 | 19 | 5.6 | 187 |
| Male | n = 296 | n = 453 | n = 1910 | n = 193 | n = 2852 | ||||
| Intake Range | 2.79–94.99 | 95.03–149.76 | 150.02–2391.91 | 2414.16–80672.0 | 2.79–80672.0 | ||||
| Median ± SE | 74.6 ± 1.7 | 122.0 ± 1.4 | 355.7 ± 8.3 | 3823.3 ± 227.3 | 270.9 ± 6.5 | ||||
| Mean ± SE | 71.7 ± 1.2 | 122.1 ± 0.9 | 543.5 ± 12.8 | 6772.6 ± 1228.9 | 836.9 ± 96.9 | ||||
| Prevalence of Thyroid Disease (n, weighted %) | |||||||||
| Non-Thyroid Disease | 293 | 98.2 | 449 | 99.1 | 1894 | 99.2 | 191 | 99.3 | 2827 |
| Thyroid Disease | 3 | 1.8 | 4 | 0.9 | 16 | 0.8 | 2 | 0.7 | 25 |
| Female | n = 554 | n = 534 | n = 1959 | n = 196 | n = 3243 | ||||
| Intake Range | 1.29–94.97 | 95.01–149.95 | 150.29–2399.36 | 2409.77–36494.0 | 1.29–36494.0 | ||||
| Median ± SE | 70.3 ± 1.6 | 122.7 ± 1.8 | 372.8 ± 12.7 | 4285.4 ± 189.5 | 235.4 ± 8.1 | ||||
| Mean ± SE | 67.9 ± 1.0 | 122.3 ± 0.9 | 575.3 ± 13.7 | 5781.4 ± 399.6 | 740.7 ± 38.7 | ||||
| Prevalence of thyroid disease (n, weighted %) | |||||||||
| Non-Thyroid Disease | 537 | 96.4 | 515 | 96.1 | 1850 | 94.2 | 179 | 89.0 | 3081 |
| Thyroid Disease | 17 | 3.6 | 19 | 3.9 | 109 | 5.8 | 17 | 11.0 | 162 |
| Estimated Iodine Intake (µg/day) | Korean Dietary Reference Intake (KDRI) | p for Trend d | |||
|---|---|---|---|---|---|
| <EAR a (<95) | ≥EAR, <RNI b (≥95, <150) | ≥RNI, <UL c (≥150, 2400) | ≥UL (≥2400) | ||
| Total | |||||
| Model 1 | 1 e | 0.832(0.409–1.692) f | 1.084(0.634–1.854) | 1.788(0.820–3.898) | 0.059(+) |
| Model 2 | 1 | 0.854(0.416–1.750) | 1.092(0.631–1.891) | 1.692(0.773–3.704) | 0.096(+) |
| Model 3 | 1 | 0.887(0.428–1.838) | 1.144(0.657–1.992) | 1.796(0.815–3.960) | 0.076(+) |
| Model 4 | 1 | 0.891(0.422–1.882) | 1.166(0.662–2.056) | 1.846(0.840–4.058) | 0.066(+) |
| Model 5 | 1 | 0.847(0.390–1.836) | 1.095(0.612–1.957) | 1.726(0.760–3.923) | 0.085(+) |
| Male | |||||
| Model 1 | 1 | 0.499(0.095–2.620) | 0.440(0.108–1.792) | 0.414(0.051–3.359) | 0.720(−) |
| Model 2 | 1 | 0.474(0.089–2.528) | 0.390(0.095–1.609) | 0.325(0.041–2.568) | 0.607(−) |
| Model 3 | 1 | 0.397(0.075–2.098) | 0.317(0.073–1.378) | 0.251(0.034–1.839) | 0.549(−) |
| Model 4 | 1 | 0.405(0.080–2.054) | 0.353(0.079–1.566) | 0.278(0.036–2.161) | 0.582(−) |
| Model 5 | 1 | 0.419(0.084–2.084) | 0.311(0.070–1.378) | 0.240(0.029–1.954) | 0.5573(−) |
| Female | |||||
| Model 1 | 1 | 1.056(0.492–2.263) | 1.667(0.908–3.061) | 2.940(1.267–6.823) | 0.014(+) |
| Model 2 | 1 | 1.054(0.490–2.267) | 1.629(0.887–2.989) | 2.773(1.198–6.420) | 0.023(+) |
| Model 3 | 1 | 1.063(0.488–2.315) | 1.608(0.873–2.961) | 2.686(1.161–6.215) | 0.026(+) |
| Model 4 | 1 | 1.048(0.479–2.292) | 1.561(0.846–2.881) | 2.554(1.113–5.861) | 0.034(+) |
| Model 5 | 1 | 0.979(0.438–2.192) | 1.426(0.766–2.654) | 2.418(1.010–5.787) | 0.038(+) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kwon, Y.S.; Kim, J.Y.; Hong, K.H.; Park, Y.K. Association between Iodine Nutrition Status and Thyroid Disease-Related Hormone in Korean Adults: Korean National Health and Nutrition Examination Survey VI (2013–2015). Nutrients 2019, 11, 2757. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112757
Kim S, Kwon YS, Kim JY, Hong KH, Park YK. Association between Iodine Nutrition Status and Thyroid Disease-Related Hormone in Korean Adults: Korean National Health and Nutrition Examination Survey VI (2013–2015). Nutrients. 2019; 11(11):2757. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112757
Chicago/Turabian StyleKim, Sohye, Yong Seok Kwon, Ju Young Kim, Kyung Hee Hong, and Yoo Kyoung Park. 2019. "Association between Iodine Nutrition Status and Thyroid Disease-Related Hormone in Korean Adults: Korean National Health and Nutrition Examination Survey VI (2013–2015)" Nutrients 11, no. 11: 2757. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112757