The Effect of Various Doses of Phenylalanine Supplementation on Blood Phenylalanine and Tyrosine Concentrations in Tyrosinemia Type 1 Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Phenylalanine Capsules
2.4. Blood Spot Sampling
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
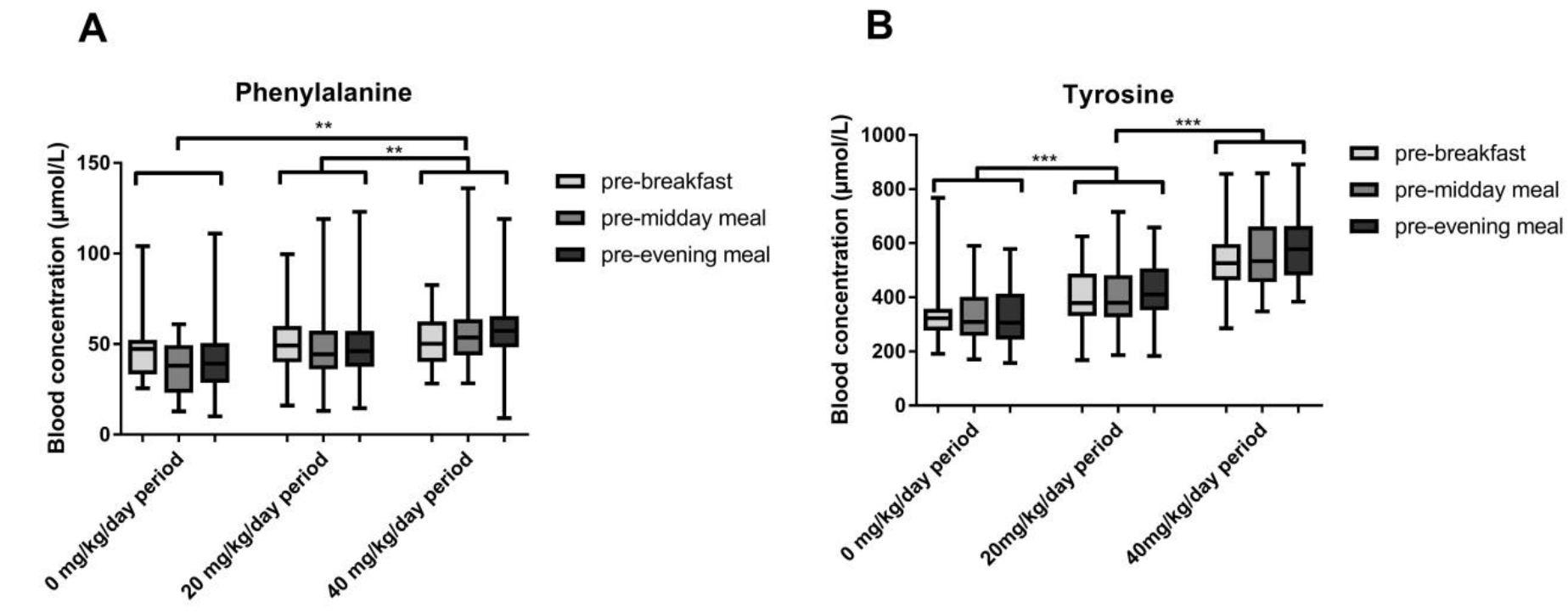
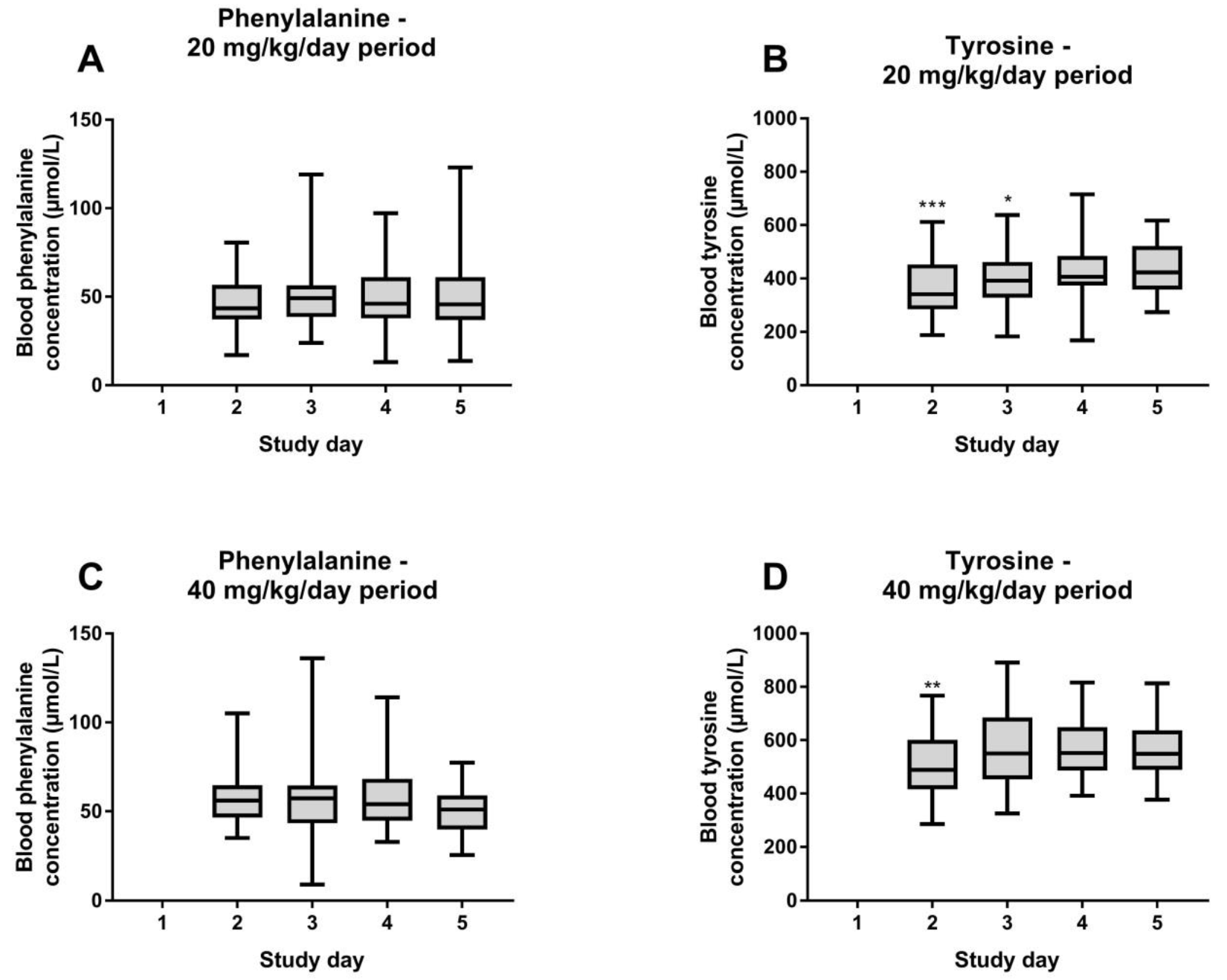
3.2. Blood Phenylalanine and Tyrosine Concentrations
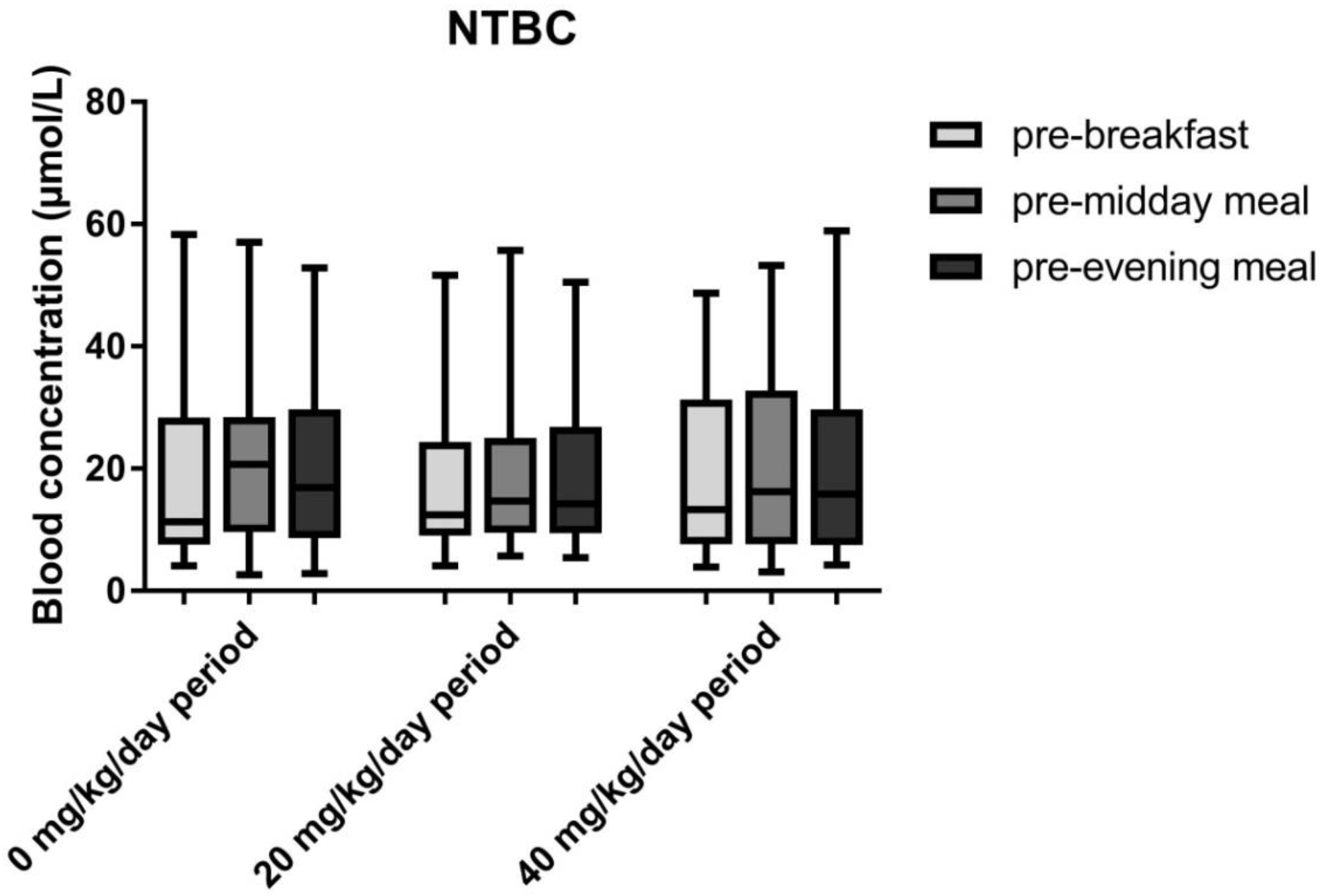
3.3. Blood NTBC and SA Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Morrow, G.; Tanguay, R.M. Biochemical and clinical aspects of hereditary tyrosinemia Type 1. Adv. Exp. Med. Biol. 2017, 959, 9–21. [Google Scholar] [PubMed]
- Mitchell, G.; Larochelle, J.; Lambert, M.; Michaud, J.; Grenier, A.; Ogier, H.; Gauthier, M.; Lacroix, J.; Vanasse, M.; Larbrisseau, A. Neurologic Crises in Hereditary Tyrosinemia. N. Engl. J. Med. 1990, 322, 432–437. [Google Scholar] [CrossRef] [PubMed]
- van Spronsen, F.J.; Thomasse, Y.; Smit, G.P.; Leonard, J.V.; Clayton, P.T.; Fidler, V.; Berger, R.; Heymans, H.S. Hereditary tyrosinemia type I: A new clinical classification with difference in prognosis on dietary treatment. Hepatology 1994, 20, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Lindstedt, S.; Holme, E.; Lock, E.A.; Hjalmarson, O.; Strandvik, B. Treatment of Hereditary Tyrosinaemia Type I by Inhibition of 4-Hydroxyphenylpyruvate Dioxygenase. Lancet 1992, 340, 813–817. [Google Scholar] [CrossRef]
- Holme, E.; Lindstedt, S. Tyrosinaemia Type I and NTBC (2-(2-Nitro-4-Trifluoromethylbenzoyl)-1,3-Cyclohexanedione). J. Inherit. Metab. Dis. 1998, 21, 507–517. [Google Scholar] [CrossRef]
- Holme, E.; Lindstedt, S. Nontransplant Treatment of Tyrosinemia. Clin. Liver Dis. 2000, 4, 805–814. [Google Scholar] [CrossRef]
- Larochelle, J.; Alvarez, F.; Bussieres, J.F.; Chevalier, I.; Dallaire, L.; Dubois, J.; Faucher, F.; Fenyves, D.; Goodyer, P.; Grenier, A.; et al. Effect of Nitisinone (NTBC) Treatment on the Clinical Course of Hepatorenal Tyrosinemia in Quebec. Mol. Genet. Metab. 2012, 107, 49–54. [Google Scholar] [CrossRef]
- van Spronsen, F.J.; van Rijn, M.; Meyer, U.; Das, A.M. Dietary Considerations in Tyrosinemia Type I. Adv. Exp. Med. Biol. 2017, 959, 197–204. [Google Scholar]
- Wilson, C.J.; Van Wyk, K.G.; Leonard, J.V.; Clayton, P.T. Phenylalanine Supplementation Improves the Phenylalanine Profile in Tyrosinaemia. J. Inherit. Metab. Dis. 2000, 23, 677–683. [Google Scholar] [CrossRef]
- Daly, A.; Gokmen-Ozel, H.; MacDonald, A.; Preece, M.A.; Davies, P.; Chakrapani, A.; McKiernan, P. Diurnal Variation of Phenylalanine Concentrations in Tyrosinaemia Type 1: Should we be Concerned? J. Hum. Nutr. Diet. 2012, 25, 111–116. [Google Scholar] [CrossRef]
- van Vliet, D.; van Dam, E.; van Rijn, M.; Derks, T.G.; Venema-Liefaard, G.; Hitzert, M.M.; Lunsing, R.J.; Heiner-Fokkema, M.R.; van Spronsen, F.J. Infants with Tyrosinemia Type 1: Should Phenylalanine be Supplemented? JIMD Rep. 2014, 18, 117–124. [Google Scholar] [PubMed]
- van Ginkel, W.G.; van Vliet, D.; Burgerhof, J.G.M.; de Blaauw, P.; Rubio Gozalbo, M.E.; Heiner-Fokkema, M.R.; van Spronsen, F.J. Presumptive Brain Influx of Large Neutral Amino Acids and the Effect of Phenylalanine Supplementation in Patients with Tyrosinemia Type 1. PLoS ONE 2017, 12, e0185342. [Google Scholar] [CrossRef] [PubMed]
- van Dam, E.; Daly, A.; Venema-Liefaard, G.; van Rijn, M.; Derks, T.G.J.; McKiernan, P.J.; Rebecca Heiner-Fokkema, M.; MacDonald, A.; van Spronsen, F.J. What is the Best Blood Sampling Time for Metabolic Control of Phenylalanine and Tyrosine Concentrations in Tyrosinemia Type 1 Patients? JIMD Rep. 2017, 36, 49–57. [Google Scholar] [PubMed]
- Pohorecka, M.; Biernacka, M.; Jakubowska-Winecka, A.; Biernacki, M.; Kusmierska, K.; Kowalik, A.; Sykut-Cegielska, J. Behavioral and Intellectual Functioning in Patients with Tyrosinemia Type I. Pediatr. Endocrinol. Diabetes Metab. 2012, 18, 96–100. [Google Scholar] [PubMed]
- Rabinowitz, L.G.; Williams, L.R.; Anderson, C.E.; Mazur, A.; Kaplan, P. Painful Keratoderma and Photophobia: Hallmarks of Tyrosinemia Type II. J. Pediatr. 1995, 126, 266–269. [Google Scholar] [CrossRef]
- Scott, C.R. The Genetic Tyrosinemias. Am. J. Med. Genet. C. Semin. Med. Genet. 2006, 142, 121–126. [Google Scholar] [CrossRef]
- de Laet, C.; Dionisi-Vici, C.; Leonard, J.V.; McKiernan, P.; Mitchell, G.; Monti, L.; de Baulny, H.O.; Pintos-Morell, G.; Spiekerkotter, U. Recommendations for the Management of Tyrosinaemia Type 1. Orphanet. J. Rare Dis. 2013, 8, 8. [Google Scholar]
- Chinsky, J.M.; Singh, R.; Ficicioglu, C.; van Karnebeek, C.D.M.; Grompe, M.; Mitchell, G.; Waisbren, S.E.; Gucsavas-Calikoglu, M.; Wasserstein, M.P.; Coakley, K.; et al. Diagnosis and Treatment of Tyrosinemia Type I: A US and Canadian Consensus Group Review and Recommendations. Genet. Med. 2017, 19, 1380. [Google Scholar] [CrossRef]
- Hussein, M.A.; Young, V.R.; Murray, E.; Scrimshaw, N.S. Daily Fluctuation of Plasma Amino Acid Levels in Adult Men: Effect of Dietary Tryptophan Intake and Distribution of Meals. J. Nutr. 1971, 101, 61–69. [Google Scholar] [CrossRef]
- Ozalp, I.; Young, V.R.; Nagchaudhuri, J.; Tontisirin, K.; Scrimshaw, N.S. Plasma Amino Acid Response in Young Men Given Diets Devoid of Single Essential Amino Acids. J. Nutr. 1972, 102, 1147–1158. [Google Scholar] [CrossRef]
- Fernstrom, J.D.; Wurtman, R.J.; Hammarstrom-Wiklund, B.; Rand, W.M.; Munro, H.N.; Davidson, C.S. Diurnal Variations in Plasma Concentrations of Tryptophan, Tryosine, and Other Neutral Amino Acids: Effect of Dietary Protein Intake. Am. J. Clin. Nutr. 1979, 32, 1912–1922. [Google Scholar] [CrossRef] [PubMed]
- van Ginkel, W.G.; Jahja, R.; Huijbregts, S.C.J.; van Spronsen, F.J. Neurological and Neuropsychological Problems in Tyrosinemia Type I Patients. Adv. Exp. Med. Biol. 2017, 959, 111–122. [Google Scholar] [PubMed]
- van Spronsen, F.J.; van Rijn, M.; van Dijk, T.; Smit, G.P.; Reijngoud, D.J.; Berger, R.; Heymans, H.S. Plasma Phenylalanine and Tyrosine Responses to Different Nutritional Conditions (Fasting/Postprandial) in Patients with Phenylketonuria: Effect of Sample Timing. Pediatrics 1993, 92, 570–573. [Google Scholar]
- Pencharz, P.B.; Hsu, J.W.; Ball, R.O. Aromatic Amino Acid Requirements in Healthy Human Subjects. J. Nutr. 2007, 137, 1576S–1578S. [Google Scholar] [CrossRef]
- Kienstra, N.S.; van Reemst, H.E.; van Ginkel, W.G.; Daly, A.; van Dam, E.; MacDonald, A.; Burgerhof, J.G.M.; de Blaauw, P.; McKiernan, P.J.; Heiner-Fokkema, M.R.; et al. Daily Variation of NTBC and its Relation to Succinylacetone in Tyrosinemia Type 1 Patients Comparing a Single Dose to Two Doses a Day. J. Inherit. Metab. Dis. 2018, 41, 181–186. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Period 1 Without Phenylalanine Supplementation | Period 2 First Phenylalanine Supplementation round (20 mg/kg/day) | Wash-out Period | Period 3 Second Phenylalanine Supplementation round (40 mg/kg/day) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study day | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8–14 | 15 | 16 | 17 | 18 | 19 | |
| Time blood spot | Break-fast | X | X | X | X | X | X | X | X | X | X | |||
| Midday meal | X | X | X | X | X | X | X | X | X | X | ||||
| Evening meal | X | X | X | X | X | X | X | X | X | X | ||||
| Pat. Number | Age (year) | Gender | Weight (kg) | Standard Extra Phenyl-Alanine (mg/kg/day) | Natural Protein Intake (g/kg/day) | Total Protein Intake (g/kg/day) | NTBC Intake (mg/kg/day) | Phenylalanine Supplementation during Study | |
|---|---|---|---|---|---|---|---|---|---|
| 20 mg/kg Period | 40 mg/kg Period | ||||||||
| 1 | 7.6 | F | 30 | 25.0 | 0.3 | 1.4 | 1.1 | 20.3 | 40.5 |
| 2 | 12.3 | M | 52 | 14.4 | 0.2 | 1.1 | 1.2 | 18.8 | 40.0 |
| 3 | 19.5 | M | 64 | 0.2 | 0.9 | 1.1 | 21.1 | 39.8 | |
| 4 | 27.0 | M | 65 | 2.5 | 0.4 | 0.9 | 0.9 | 20.8 | 39.2 |
| 5 | 6.9 | F | 25 | 4.0 | 0.9 | 1.9 | 0.7 | 18.0 | 42.0 |
| 6 | 15.6 | M | 46 | 0.5 | 1.8 | 0.9 | 20.8 | 41.7 | |
| 7 | 13.9 | M | 75 | 0.4 | 1.2 | 0.5 | 20.0 | 40.0 | |
| 8 | 13.3 | M | 49 | 0.5 | 1.6 | 0.8 | 20.4 | 40.8 | |
| 9 | 14.2 | F | 59 | 0.3 | 1.4 | 0.5 | 20.3 | 40.7 | |
| 10 | 9.3 | F | 38 | 0.7 | 2.2 | 0.8 | 15.8 | 39.5 | |
| 11 | 14.4 | M | 59 | 0.5 | 1.4 | 0.4 | 20.3 | 39.8 | |
| Breakfast (µmol/L) | Midday Meal (µmol/L) | Evening Meal (µmol/L) | |
|---|---|---|---|
| Period 1 (0 mg/kg/day) | 50 ± 21 | 37 ± 15 | 43 ± 25 |
| Period 2 (20 mg/kg/day) | 51 ± 18 | 47 ± 19 | 48 ± 23 |
| Period 3 (40 mg/kg/day) | 52 ± 14 | 56 ± 20 | 58 ± 20 |
| No Phenylalanine Supplementation | 20 mg/kg Phenylalanine Supplementation | 40 mg/kg Phenylalanine Supplementation | |
|---|---|---|---|
| SA < 0.1 µmol/L | 23 (66%) | 41 (51%) | 44 (57%) |
| SA ≥ 0.1 µmol/L | 12 (34%) | 39 (49%) | 33 (43%) |
| Total | 35 (100%) | 80 (100%) | 77 (100%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Ginkel, W.G.; van Reemst, H.E.; Kienstra, N.S.; Daly, A.; Rodenburg, I.L.; MacDonald, A.; Burgerhof, J.G.M.; de Blaauw, P.; van de Krogt, J.; Santra, S.; et al. The Effect of Various Doses of Phenylalanine Supplementation on Blood Phenylalanine and Tyrosine Concentrations in Tyrosinemia Type 1 Patients. Nutrients 2019, 11, 2816. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112816
van Ginkel WG, van Reemst HE, Kienstra NS, Daly A, Rodenburg IL, MacDonald A, Burgerhof JGM, de Blaauw P, van de Krogt J, Santra S, et al. The Effect of Various Doses of Phenylalanine Supplementation on Blood Phenylalanine and Tyrosine Concentrations in Tyrosinemia Type 1 Patients. Nutrients. 2019; 11(11):2816. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112816
Chicago/Turabian Stylevan Ginkel, Willem G., Hannah E. van Reemst, Nienke S. Kienstra, Anne Daly, Iris L. Rodenburg, Anita MacDonald, Johannes G.M. Burgerhof, Pim de Blaauw, Jennifer van de Krogt, Saikat Santra, and et al. 2019. "The Effect of Various Doses of Phenylalanine Supplementation on Blood Phenylalanine and Tyrosine Concentrations in Tyrosinemia Type 1 Patients" Nutrients 11, no. 11: 2816. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112816