Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
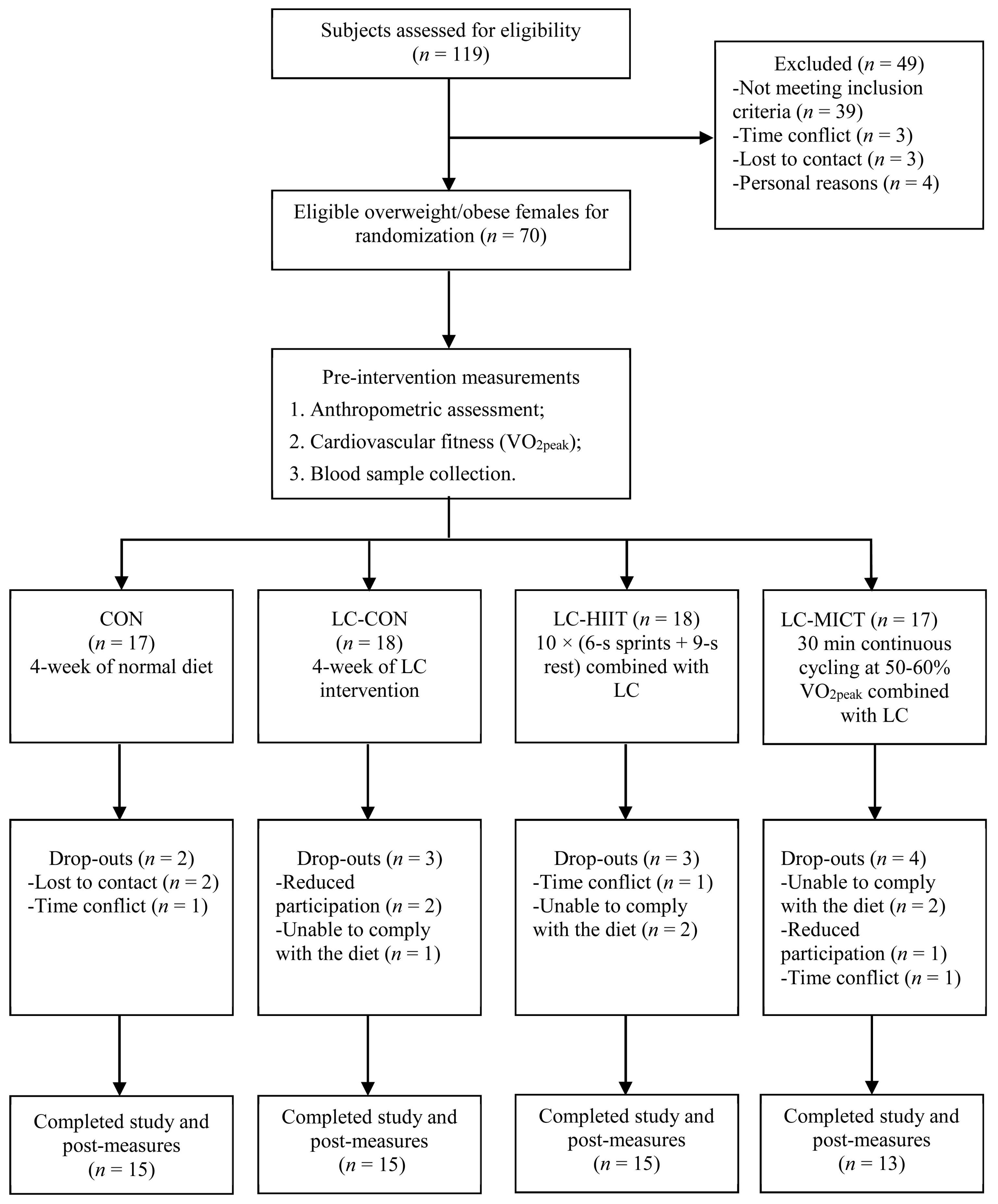
2.1. Participants
2.2. Experimental Design
2.3. Diet Intervention
2.4. Exercise Intervention
2.5. Pre- and Post-Intervention Measurements
2.5.1. Blood Profiles
2.5.2. Anthropometric Assessments
2.5.3. Maximal Incremental Exercise Test
2.6. Statistical Analysis
3. Results
3.1. Compliance, Diet Compositions, and Daily Physical Activities
3.2. Training Data
3.3. Anthropometric Parameters
3.4. Cardiorespiratory Fitness Levels
3.5. Blood Lipids and Fasting Glucose
3.6. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindstrom, J.; Ilanneparikka, P.; Peltonen, M.; Aunola, S.; Eriksson, J.G.; Hemio, K.; Hämäläinen, H.; Härkönen, P.; Keinänen-Kiukaanniemi, S.; Laakso, M. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: Follow-up of the Finnish Diabetes Prevention Study. Lancet 2006, 368, 1673–1679. [Google Scholar] [CrossRef]
- Espeland, M.A.; Pisunyer, X.; Blackburn, G.L.; Brancati, F.L.; Bray, G.A.; Bright, R. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: One-year results of the look AHEAD trial. Diabetes Care 2007, 30, 1374–1383. [Google Scholar]
- Seagle, H.M.; Strain, G.W.; Makris, A.; Reeves, R.S. Position of the American Dietetic Association: Weight management. J. Am. Diet. Assoc. 2009, 109, 330–346. [Google Scholar]
- Bueno, N.B.; de Melo, I.S.V.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Bazzano, L.A.; Hu, T.; Reynolds, K.; Yao, L.; Bunol, C.; Liu, Y.; Chen, C.S.; Klag, M.J.; Whelton, P.K.; He, J. Effects of Low-Carbohydrate and Low-Fat Diets: A Randomized Trial. Ann. Intern. Med. 2014, 161, 309–318. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Benelli, M.; Brancaleoni, M.; Dainelli, G.; Merlini, D.; Negri, R. Middle and Long-Term Impact of a Very Low-Carbohydrate Ketogenic Diet on Cardiometabolic Factors: A Multi-Center, Cross-Sectional, Clinical Study. Ann. Rev. Physiol. 2015, 22, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Gardner, C.D.; Kiazand, A.; Alhassan, S.; Kim, S.; Stafford, R.S.; Balise, R.R.; Kraemer, H.C.; King, A.C. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: The A TO Z Weight Loss Study: A randomized trial. JAMA 2007, 297, 969–977. [Google Scholar] [CrossRef]
- Gu, Y.; Yu, H.; Li, Y.; Ma, X.; Lu, J.; Yu, W.; Xiao, Y.; Bao, Y.; Jia, W. Beneficial Effects of an 8-Week, Very Low Carbohydrate Diet Intervention on Obese Subjects. Evid.-Based Complement. Altern. Med. 2013, 2013, 760804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westman, E.C.; Yancy, W.S.; Mavropoulos, J.C.; Marquart, M.; Mcduffie, J.R. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutr. Metab. 2008, 5, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Xu, N.; Lin, N.; Wu, P.; Yuan, K.; An, S.; Zhang, Z.; Ruan, Y.; Zhang, Y.; Xu, G.; et al. 317-LB: Optimal Weight Loss Effect of Short-Term Low Carbohydrate Diet with Calorie Restriction on Overweight/Obese Subjects in South China—A Multicenter Randomized Controlled Trial. Diabetes 2019, 68. [Google Scholar] [CrossRef]
- Popkin, B.M.; Gordon-Larsen, P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int. J. Obes. 2004, 28, S2–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, F.; Wang, H.; Du, S.; He, Y.; Wang, Z.; Ge, K.; Popkin, B.M. Prospective study on nutrition transition in China. Nutr. Rev. 2009, 67, S56–S61. [Google Scholar] [CrossRef]
- Brinkworth, G.D.; Noakes, M.; Buckley, J.D.; Keogh, J.B.; Clifton, P.M. Long-term effects of a very-low-carbohydrate weight loss diet compared with an isocaloric low-fat diet after 12 mo. Am. J. Clin. Nutr. 2009, 90, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Urbain, P.; Strom, L.; Morawski, L.; Wehrle, A.; Deibert, P.; Bertz, H. Impact of a 6-week non-energy-restricted ketogenic diet on physical fitness, body composition and biochemical parameters in healthy adults. Nutr. Metab. 2017, 14, 17. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Zhang, H.; Kong, Z.; Shi, Q.; Tong, T.K.; Nie, J. Twelve weeks of low volume sprint interval training improves cardio-metabolic health outcomes in overweight females. J. Sports Sci. 2019, 37, 1257–1264. [Google Scholar] [CrossRef]
- Trapp, E.G.; Chisholm, D.J.; Freund, J.; Boutcher, S.H. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int. J. Obes. 2008, 32, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012, 42, 489–509. [Google Scholar] [CrossRef]
- Martins, C.; Kazakova, I.; Ludviksen, M.; Mehus, I.; Wisloff, U.; Kulseng, B.; Morgan, L.; King, N. High-intensity interval training and isocaloric moderate-intensity continuous training result in similar improvements in body composition and fitness in obese individuals. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Borer, K.T.; Lin, P.J. Low-Carbohydrate-High-Fat Diet: Can it Help Exercise Performance? J. Hum. Kinet. 2017, 56, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Okeeffe, K.; Keith, R.E.; Wilson, G.D.; Blessing, D.L. Dietary carbohydrate intake and endurance exercise performance of trained female cyclists. Nutr. Res. 1989, 9, 819–830. [Google Scholar] [CrossRef]
- Gist, N.H.; Fedewa, M.V.; Dishman, R.K.; Cureton, K.J. Sprint interval training effects on aerobic capacity: A systematic review and meta-analysis. Sports Med. 2014, 44, 269–279. [Google Scholar] [CrossRef]
- World Healt Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Commurhoadsnications Austrbya: Sydney, Australia, 2000. [Google Scholar]
- Urbain, P.; Bertz, H. Monitoring for compliance with a ketogenic diet: What is the best time of day to test for urinary ketosis? Nutr. Metab. 2016, 13, 77. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Simple Rating Methods for Estimation of Perceived Exertion. In Physical Work and Effort; Pergamon Press: Oxford, UK, 1976; pp. 39–46. [Google Scholar]
- Rossiter, H.B.; Kowalchuk, J.M.; Whipp, B.J. A test to establish maximum O2 uptake despite no plateau in the O2 uptake response to ramp incremental exercise. J. Appl. Physiol. 2006, 100, 764–770. [Google Scholar] [CrossRef]
- Kirk, R.E. Practical significance: A concept whose time has come. Educ. Psychol. Meas. 1996, 56, 746–759. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Sharman, M.J.; Kraemer, W.J.; Love, D.M.; Avery, N.G.; Gomez, A.L.; Scheett, T.P.; Volek, J.S. A Ketogenic Diet Favorably Affects Serum Biomarkers for Cardiovascular Disease in Normal-Weight Men. J. Nutr. 2002, 132, 1879–1885. [Google Scholar] [CrossRef]
- Nazare, J.; Smith, J.B.; Borel, A.; Aschner, P.; Barter, P.; Van Gaal, L.; Tan, C.E.; Wittchen, H.U.; Matsuzawa, Y.; Kadowaki, T. Usefulness of measuring both body mass index and waist circumference for the estimation of visceral adiposity and related cardiometabolic risk profile (from the INSPIRE ME IAA study). Am. J. Cardiol. 2015, 115, 307–315. [Google Scholar] [CrossRef]
- Neeland, I.J.; Ayers, C.R.; Rohatgi, A.; Turer, A.T.; Berry, J.D.; Das, S.R. Associations of visceral and abdominal subcutaneous adipose tissue with markers of cardiac and metabolic risk in obese adults. Obesity 2013, 21, E439–E447. [Google Scholar] [CrossRef]
- Paoli, A.; Rubini, A.; Volek, J.; Grimaldi, K. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldhorst, M.A.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Gluconeogenesis and energy expenditure after a high-protein, carbohydrate-free diet. Am. J. Clin. Nutr. 2009, 90, 519–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, E.J.; Feinman, R.D. Thermodynamics of weight loss diets. Nutr. Metab. 2004, 1, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, Z.; Fan, X.; Sun, S.; Song, L.; Shi, Q.; Nie, J. Comparison of high-intensity interval training and moderate-to-vigorous continuous training for cardiometabolic health and exercise enjoyment in obese young women: A randomized controlled trial. PLoS ONE 2016, 11, e0158589. [Google Scholar] [CrossRef]
- Kong, Z.; Sun, S.; Liu, M.; Shi, Q. Short-Term High-Intensity Interval Training on Body Composition and Blood Glucose in Overweight and Obese Young Women. J. Diabetes Res. 2016, 2016, 4073618. [Google Scholar] [CrossRef]
- Klement, R.J.; Frobel, T.; Albers, T.; Fikenzer, S.; Prinzhausen, J.; Kämmerer, U. A pilot case study on the impact of a self-prescribed welketogenic diet on biochemical parameters and running performance in healthy and physically active individuals. Nutr. Med. 2013, 1, 10. [Google Scholar]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Almallah, M.H.; Sakr, S.; Alqunaibet, A. Cardiorespiratory Fitness and Cardiovascular Disease Prevention: An Update. Curr. Atheroscler. Rep. 2018, 20, 1. [Google Scholar] [CrossRef]
- Brinkworth, G.D.; Noakes, M.; Clifton, P.M.; Buckley, J.D. Effects of a low carbohydrate weight loss diet on exercise capacity and tolerance in obese subjects. Obesity 2009, 17, 1916–1923. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| LC-HIIT | LC-MICT | |
|---|---|---|
| Weekly training time (min) | 12.5 | 150 |
| Total training time (min) | 50 | 600 |
| Energy expenditure (kcal) | 17.6 (2.2) ** | 148.6 (15.5) |
| Training power (W) | 248.7 (34.1) ** | 53.8 (9.7) |
| Intensity (% VO2peak) | 86.8 (9.5) ** | 59.5 (6.6) |
| Training HR (bpm) | 146 (5) ** | 139 (8) |
| Training HR/HRmax (%) | 81.7 (3.5) ** | 74.9 (3.1) |
| Training RPE | 14 (1) ** | 11 (1) |
| CON (n = 15) | LC-CON (n = 15) | LC-HIIT (n = 15) | LC-MICT (n = 13) | Group Effect | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | p | Partial η2 | |
| Age (y) | 21.6 (3.9) | 20.9 (3.7) | 20.8 (2.7) | 21.5 (3.1) | ||||||
| Height (cm) | 163 (5.6) | 161.3 (4.7) | 162.9 (6.2) | 160.9 (4.3) | ||||||
| Weight (kg) | 66.0 (10.2) | 66.1 (10.8) | 65.1 (7.3) | 62.3 (6.7) * | 67.9 (10.3) | 65.0 (9.7) * | 64.5 (6.4) | 61.9 (6.0) * | 0.000 | 0.510 |
| BMI (kg·m−2) | 24.8 (3.2) | 24.8 (3.4) | 25.0 (2.9) | 24.0 (2.7) * | 25.5 (3.1) | 24.4 (2.9) * | 24.9 (1.9) | 23.9 (1.8) * | 0.000 | 0.504 |
| WC (cm) | 77.7 (9.0) | 78.5 (9.2) | 78.0 (6.9) | 74.0 (6.2) * | 79.5 (9.4) | 75.7 (9.5) * | 75.5 (6.3) | 71.2 (4.8) * | 0.000 | 0.523 |
| HC (cm) | 100.5 (6.1) | 100.4 (6.9) | 100.7 (3.9) | 98.2 (3.9) * | 100.3 (4.8) | 98.5 (5.3) * | 101.0 (5.1) | 97.7 (5.3) * | 0.000 | 0.338 |
| WHR | 0.77 (0.1) | 0.78 (0.1) | 0.77 (0.0) | 0.75 (0.0) * | 0.79 (0.1) | 0.77 (0.1) * | 0.75 (0.0) | 0.73 (0.0) * | 0.000 | 0.313 |
| VO2peak (mL·min−1·kg−1) | 25.6 (4.0) | 25.4 (4.2) | 25.2 (4.3) | 24.8 (2.4) | 23.3 (2.5) | 26.7 (3.4) *# | 23.4 (4.4) | 27.1 (3.8) *# | 0.009 | 0.193 |
| FG (mmol·L−1) | 4.6 (0.5) | 4.7 (0.3) | 4.7 (0.4) | 4.6 (0.4) | 4.9 (0.5) | 4.7 (0.6) | 4.8 (0.3) | 4.8 (0.3) | 0.307 | 0.065 |
| CHOL (mmol·L−1) | 4.6 (0.8) | 4.9 (0.7) | 5.1 (1.0) | 6.1 (1.3) | 4.5 (0.7) | 5.3 (1.0) | 4.5 (0.6) | 5.1 (1.0) | 0.087 | 0.115 |
| HDL-C (mmol·L−1) | 1.6 (0.4) | 1.6 (0.4) | 1.7 (0.3) | 1.7 (0.3) | 1.5 (0.3) | 1.5 (0.4) | 1.5 (0.3) | 1.7 (0.4) | 0.470 | 0.046 |
| LDL-C (mmol·L−1) | 2.7 (0.7) | 3.0 (0.6) | 3.3 (1.0) | 4.2 (1.2) | 2.8 (0.6) | 3.6 (0.8) | 2.8 (0.5) | 3.4 (0.9) | 0.084 | 0.117 |
| TG (mmol·L−1) | 1.1 (1.0) | 1.1 (1.0) | 1.0 (0.5) | 1.1 (0.6) | 1.2 (0.4) | 0.9 (0.3) | 0.9 (0.4) | 0.8 (0.2) | 0.229 | 0.077 |
| CON (n = 15) | LC-CON (n = 15) | LC-HIIT (n = 15) | LC-MICT (n = 13) | ES (d) | |||
|---|---|---|---|---|---|---|---|
| LC-CON | LC-HIIT | LC-MICT | |||||
| ∆ Weight (kg) | 0.09 (1.25) | −2.85 (1.50) ** | −2.85 (1.12) ** | −2.56 (1.31) ** | 2.12 | 2.48 | 2.07 |
| ∆ BMI (kg·m−2) | 0.02 (0.48) | −1.09 (0.56) ** | −1.07 (0.41) ** | −0.98 (0.49) ** | 2.14 | 2.45 | 2.08 |
| ∆ WC (cm) | 0.8 (1.47) | −4.02 (2.36) ** | −3.81 (1.98) ** | −4.36 (2.87) ** | 2.45 | 2.65 | 2.32 |
| ∆ HC (cm) | −0.13 (1.52) | −2.51 (1.93) ** | −1.83 (1.78) * | −3.27 (1.40) ** | 1.37 | 1.03 | 2.14 |
| ∆ WHR | 0.01 (0.01) | −0.02 (0.03) ** | −0.02 (0.02) ** | −0.02 (0.03) ** | 1.35 | 1.96 | 1.41 |
| ∆ VO2peak (ml·min−1·kg−1) | −0.21 (2.46) | −0.37 (3.75) | 3.41 (2.22) **# | 3.67 (3.00) **# | 0.05 | 1.55 | 1.43 |
| ∆ VO2peak% | −0.62 (9.26) | −0.37 (14.06) | 14.76 (9.62) **# | 17.32 (14.24) **# | 0.08 | 1.63 | 1.52 |
| ∆ FG (mmol·L−1) | 0.11 (0.31) | −0.13 (0.41) | −0.21 (0.42) | −0.07 (0.30) | 0.68 | 0.86 | 0.60 |
| ∆ CHOL (mmol·L−1) | 0.31 (0.64) | 0.98 (1.07) | 0.77 (0.84) | 0.61 (0.63) | 0.75 | 0.62 | 0.47 |
| ∆ HDL-C (mmol·L−1) | 0.01 (0.17) | 0.04 (0.25) | 0.09 (0.18) | 0.13 (0.16) | 0.14 | 0.48 | 0.70 |
| ∆ LDL-C (mmol·L−1) | 0.31 (0.52) | 0.89 (0.98) | 0.78 (0.72) | 0.58 (0.54) | 0.74 | 0.74 | 0.50 |
| ∆ TG (mmol·L−1) | −0.03 (0.24) | 0.09 (0.65) | −0.23 (0.43) | −0.16 (0.28) | 0.25 | 0.55 | 0.49 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, S.; Kong, Z.; Shi, Q.; Hu, M.; Zhang, H.; Zhang, D.; Nie, J. Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females. Nutrients 2019, 11, 3051. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123051
Sun S, Kong Z, Shi Q, Hu M, Zhang H, Zhang D, Nie J. Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females. Nutrients. 2019; 11(12):3051. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123051
Chicago/Turabian StyleSun, Shengyan, Zhaowei Kong, Qingde Shi, Mingzhu Hu, Haifeng Zhang, Di Zhang, and Jinlei Nie. 2019. "Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females" Nutrients 11, no. 12: 3051. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123051