Chemical Characterization and Antiplatelet Potential of Bioactive Extract from Tomato Pomace (Byproduct of Tomato Paste)

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tomato Pomace Extract
2.2. Physical-Chemical Characterization of Tomato Pomace Extract
2.3. Detection and Quantification of Bioactive Compounds by High-Performance Liquid Chromatography-Mass Spectrometry (HPLC-MS)
2.4. Clinical Pilot Study
2.4.1. Study Population
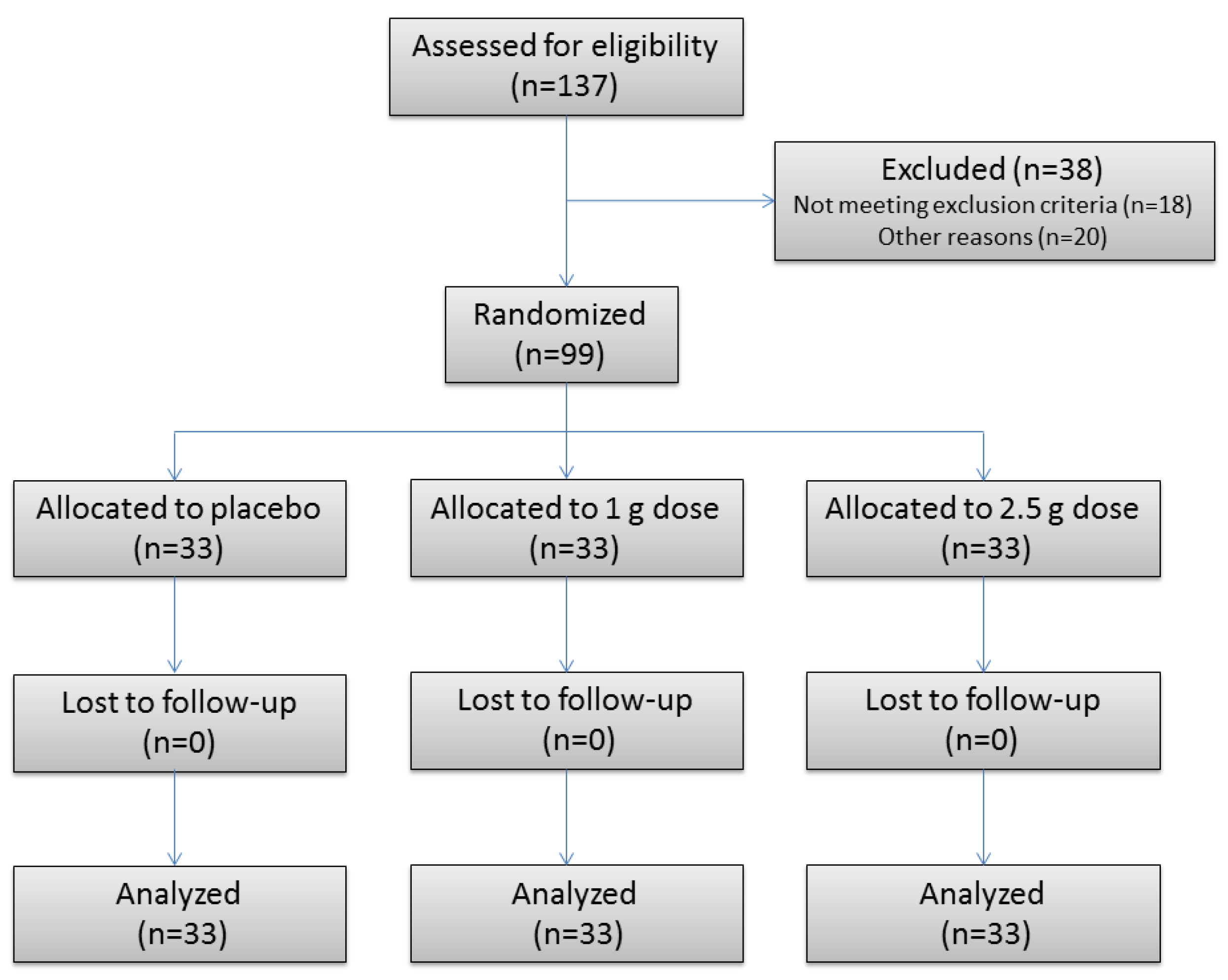
2.4.2. Study Design
2.5. Platelet Aggregation Assay
2.6. Statistical Analysis
3. Results
3.1. Physical-Chemical Characterization of Tomato Pomace Extract
3.2. Detection and Quantification of Bioactive Compounds by HPLC-MS
3.2.1. Phase 1: Outcome of Safety Assessment
3.2.2. Phase 2: Effects of Treatment on Platelet Aggregation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sesso, H.D.; Liu, S.; Gaziano, J.M.; Buring, J.E. Dietary lycopene, tomato-based food products and cardiovascular disease in women. J. Nutr. 2003, 133, 2336–2341. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Lyass, A.; Massaro, J.M.; Vasan, R.S.; D’Agostino, R.B. Relationship of lycopene intake and consumption of tomato products to incident CVD. Br. J. Nutr. 2013, 110, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuevas-Ramos, D.; Almeda-Valdes, P.; Chavez-Manzanera, E.; Meza-Arana, C.E.; Brito-Cordova, G.; Mehta, R.; Perez-Mendez, O.; Gomez-Perez, F.J. Effect of tomato consumption on high-density lipoprotein cholesterol level: a randomized, single-blinded, controlled clinical trial. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Silaste, M.L.; Alfthan, G.; Aro, A.; Kesaniemi, Y.A.; Horkko, S. Tomato juice decreases LDL cholesterol levels and increases LDL resistance to oxidation. Br. J. Nutr. 2007, 98, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Valderas-Martinez, P.; Chiva-Blanch, G.; Casas, R.; Arranz, S.; Martinez-Huelamo, M.; Urpi-Sarda, M.; Torrado, X.; Corella, D.; Lamuela-Raventos, R.M.; Estruch, R. Tomato sauce enriched with olive oil exerts greater effects on cardiovascular disease risk factors than raw tomato and tomato sauce: A randomized trial. Nutrients 2016, 8, 170. [Google Scholar] [CrossRef]
- O’Kennedy, N.; Crosbie, L.; Whelan, S.; Luther, V.; Horgan, G.; Broom, J.I.; Webb, D.J.; Duttaroy, A.K. Effects of tomato extract on platelet function: A double-blinded crossover study in healthy humans. Am. J. Clin. Nutr. 2006, 84, 561–569. [Google Scholar] [CrossRef]
- O’Kennedy, N.; Crosbie, L.; van Lieshout, M.; Broom, J.I.; Webb, D.J.; Duttaroy, A.K. Effects of antiplatelet components of tomato extract on platelet function in vitro and ex vivo: A time-course cannulation study in healthy humans. Am. J. Clin. Nutr. 2006, 84, 570–579. [Google Scholar] [CrossRef]
- Huo, Y.; Ley, K.F. Role of platelets in the development of atherosclerosis. Trends Cardiovasc. Med. 2004, 14, 18–22. [Google Scholar] [CrossRef]
- Vandvik, P.O.; Lincoff, A.M.; Gore, J.M.; Gutterman, D.D.; Sonnenberg, F.A.; Alonso-Coello, P.; Akl, E.A.; Lansberg, M.G.; Guyatt, G.H.; Spencer, F.A. Primary and secondary prevention of cardiovascular disease: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012, 141, e637S–e668S. [Google Scholar] [CrossRef]
- Anand, S.S.; Hawkes, C.; de Souza, R.J.; Mente, A.; Dehghan, M.; Nugent, R.; Zulyniak, M.A.; Weis, T.; Bernstein, A.M.; Krauss, R.M.; et al. Food consumption and its impact on cardiovascular disease: Importance of solutions focused on the globalized food system: A report from the workshop convened by the World Heart Federation. J. Am. Coll. Cardiol. 2015, 66, 1590–1614. [Google Scholar] [CrossRef]
- Haminiuk, C.W.I.; Maciel, G.M.; Plata-Oviedo, M.S.V.; Peralta, R.M. Phenolic compounds in fruits—An overview. Int. J. Food Sci. Technol. 2012, 47, 2023–2044. [Google Scholar] [CrossRef]
- Lazos, E.S.; Kalathenos, P. Technical Note: Composition of tomato processing wastes. Int. J. Food Sci. Technol. 1988, 23, 649–652. [Google Scholar] [CrossRef]
- Albanese, D.; Adiletta, G.; D′Acunto, M.; Cinquanta, L.; Di Matteo, M. Tomato peel drying and carotenoids stability of the extracts. Int. J. Food Sci. Technol. 2014, 49, 2458–2463. [Google Scholar] [CrossRef]
- Fuentes, E.; Forero-Doria, O.; Carrasco, G.; Marican, A.; Santos, L.S.; Alarcon, M.; Palomo, I. Effect of tomato industrial processing on phenolic profile and antiplatelet activity. Molecules 2013, 18, 11526–11536. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, E.; Pereira, J.; Alarcon, M.; Valenzuela, C.; Perez, P.; Astudillo, L.; Palomo, I. Protective mechanisms of S. lycopersicum aqueous fraction (nucleosides and flavonoids) on platelet activation and thrombus formation: In vitro, ex vivo and in vivo studies. Evid. Based Complement. Altern. Med. 2013, 2013, 609714. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Azua, R.; Treuer, A.; Moore-Carrasco, R.; Cortacans, D.; Gutierrez, M.; Astudillo, L.; Fuentes, E.; Palomo, I. Effect of tomato industrial processing (different hybrids, paste, and pomace) on inhibition of platelet function in vitro, ex vivo, and in vivo. J. Med. Food 2014, 17, 505–511. [Google Scholar] [CrossRef] [PubMed]
- O’Kennedy, N.; Crosbie, L.; Song, H.J.; Zhang, X.; Horgan, G.; Duttaroy, A.K. A randomised controlled trial comparing a dietary antiplatelet, the water-soluble tomato extract Fruitflow, with 75 mg aspirin in healthy subjects. Eur. J. Clin. Nutr. 2017, 71, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Lutz, M. Science Behind the Substantiation of Health Claims in Functional Foods: Current Regulations. In Functional Foods and Biotechnology; Shetty, K., Sarkar, D., Eds.; CRC Press/Taylor & Francis Group: Boca Raton, FL, USA, 2018. [Google Scholar]
- Latimer, G.W. (Ed.) Official Methods of Analysis, 19th ed.; Association of Official Analytical Chemists: Arlington, VA, USA, 2012. [Google Scholar]
- Born, G.V.; Cross, M.J. The aggregation of blood platelets. J. Physiol. 1963, 168, 178–195. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, F.; Alarcon, M.; Badimon, L.; Fuentes, M.; Klotz, K.N.; Vilahur, G.; Kachler, S.; Padro, T.; Palomo, I.; Fuentes, E. Guanosine exerts antiplatelet and antithrombotic properties through an adenosine-related cAMP-PKA signaling. Int. J. Cardiol. 2017, 248, 294–300. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- O’Kennedy, N.; Raederstorff, D.; Duttaroy, A.K. Fruitflow(R): The first European Food Safety Authority-approved natural cardio-protective functional ingredient. Eur. J. Nutr. 2017, 56, 461–482. [Google Scholar] [CrossRef]
- Kelebek, H.; Selli, S.; Kadiroglu, P.; Kola, O.; Kesen, S.; Ucar, B.; Cetiner, B. Bioactive compounds and antioxidant potential in tomato pastes as affected by hot and cold break process. Food Chem. 2017, 220, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Huélamo, M.; Vallverdú-Queralt, A.; Di Lecce, G.; Valderas-Martínez, P.; Tulipani, S.; Jáuregui, O.; Escribano-Ferrer, E.; Estruch, R.; Illan, M.; Lamuela-Raventós, R.M. Bioavailability of tomato polyphenols is enhanced by processing and fat addition: Evidence from a randomized feeding trial. Mol. Nutr. Food. Res. 2016, 60, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Dehghan-Shoar, Z.; Hardacre, A.K.; Meerdink, G.; Brennan, C.S. Lycopene extraction from extruded products containing tomato skin. Int. J. Food Sci. Technol. 2011, 46, 365–371. [Google Scholar] [CrossRef]
- Fuentes, E.; Castro, R.; Astudillo, L.; Carrasco, G.; Alarcon, M.; Gutierrez, M.; Palomo, I. Bioassay-guided isolation and HPLC determination of bioactive compound that relate to the antiplatelet activity (adhesion, secretion, and aggregation) from Solanum Lycopersicum. Evid. Based Complement. Altern. Med. 2012, 2012, 147031. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, E.; Pereira, J.; Mezzano, D.; Alarcon, M.; Caballero, J.; Palomo, I. Inhibition of platelet activation and thrombus formation by adenosine and inosine: Studies on their relative contribution and molecular modeling. PLoS ONE 2014, 9, e112741. [Google Scholar] [CrossRef] [PubMed]
- Koh, E.; Charoenprasert, S.; Mitchell, A.E. Effects of industrial tomato paste processing on ascorbic acid, flavonoids and carotenoids and their stability over one-year storage. J. Sci. Food Agric. 2012, 92, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, E.; Carle, R.; Astudillo, L.; Guzman, L.; Gutierrez, M.; Carrasco, G.; Palomo, I. Antioxidant and antiplatelet activities in extracts from green and fully ripe tomato fruits (Solanum lycopersicum) and pomace from industrial tomato processing. Evid. Based. Complement. Alternat. Med. 2013, 2013, 867578. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Bioactive Compound | TP Extract |
|---|---|
| Flavonoids (mg/100 g dw) | |
| Gallic Acid | 0.83 |
| Ferulic Acid | 2.44 |
| Coumaric Acid | 88.56 |
| Floridzin | 4.71 |
| Floretin | 97.31 |
| Procyanidin B2 | 1868.49 |
| Apigenin-7-O-glucoside | <0.001 |
| Kaempferol-3-O-glucoside | 2032.58 |
| Luteolin-7-O-glucoside | 63.34 |
| Genistein | <0.001 |
| Kaempferol | 77.090 |
| Daidzein | <0.001 |
| Quercitin | 408.23 |
| Quercitrin | 1.96 |
| Rutin | 0.262 |
| Epicatechin | 0.13 |
| Nucleosides (ug/100 g dw) | |
| Adenosine | 42.90 |
| Inosine | 57.20 |
| Guanosine | 20.97 |
| Carotenoids (mg/100 g dw) | |
| Lycopene | <0.001 |
| Beta-carotene | 55.5 |
| Dose/Variable | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 h | 3 h | 0 h | 3 h | 0 h | 3 h | 0 h | 3 h | 0 h | 3 h | |
| TP extract = 1.0 g | ||||||||||
| SBP | 120 ± 8 | 120 ± 11 | 113 ± 11 | 113 ± 7 | 116 ± 6 | 112 ± 11 | 117 ± 12 | 110 ± 7 | 108 ± 8 | 119 ± 10 |
| DBP | 74 ± 14 | 70 ± 8 | 70 ± 8 | 68 ± 10 | 71 ± 8 | 72 ± 4 | 67 ± 8 | 64 ± 4 | 64 ± 7 | 68 ± 11 |
| HR | 65 ± 5 | 69 ± 4 | 62 ± 4 | 72 ± 9 | 69 ± 11 | 74 ± 13 | 64 ± 8 | 72 ± 8 | 63 ± 5 | 69 ± 6 |
| TP extract = 2.5 g | ||||||||||
| SBP | 110 ± 12 | 104 ± 10 | 116 ± 4 | 109 ± 8 | 118 ± 11 | 109 ± 8 | 116 ± 7 | 108 ± 8 | 112 ± 4 | 109 ± 3 |
| DBP | 62 ± 7 | 62 ± 8 | 68 ± 7 | 61 ± 2 | 64 ± 5 | 63 ± 5 | 64 ± 9 | 64 ± 4 | 64 ± 4 | 64 ± 5 |
| HR | 71 ± 11 | 66 ± 5 | 70 ± 11 | 70 ± 8 | 68 ± 5 | 71 ± 10 | 71 ± 12 | 73 ± 7 | 72 ± 7 | 74 ± 11 |
| TP extract = 10 g | ||||||||||
| SBP | 110 ± 12 | 104 ± 6 | 98 ± 9 | 100 ± 8 | 104 ± 9 | 110 ± 9 | 112 ± 6 | 108 ± 9 | 111 ± 7 | 113 ± 11 |
| DBP | 65 ± 9 | 68 ± 10 | 64 ± 5 | 65 ± 5 | 62 ± 5 | 67 ± 10 | 67 ± 3 | 62 ± 6 | 64 ± 5 | 60 ± 3 |
| HR | 73 ± 5 | 66 ± 10 | 65 ± 6 | 67 ± 8 | 71 ± 6 | 76 ± 5 | 76 ± 3 | 79 ± 4 | 75 ± 5 | 80 ± 9 |
| Biochemical Parameter | TP (1 g) | TP (2.5 g) | TP (10 g) | |||
|---|---|---|---|---|---|---|
| Baseline | Day 6 | Baseline | Day 6 | Baseline | Day 6 | |
| Haemoglobin (g/dL) | 15.0 ± 0.7 | 14.6 ± 0.7 | 15.3 ± 0.7 | 15.1 ± 0.5 | 15.7 ± 0.7 | 15.3 ± 0.7 |
| Hematocrit (%) | 45.2 ± 1.6 | 44.3 ± 1.8 | 45.6 ± 1.8 | 45.0 ± 1.6 | 47.3 ± 1.9 | 46.1 ± 1.5 |
| Erythrocytes (×106/µL) | 5.0 ± 0.2 | 4.9 ± 0.3 | 5.2 ± 0.3 | 5.1 ± 0.2 | 5.2 ± 0.3 | 5.1 ± 0.1 |
| MCHC (%) | 33.1 ± 0.6 | 32.9 ± 0.6 | 33.5 ± 0.3 | 33.6 ± 0.6 | 33.2 ± 0.5 | 33.1 ± 0.6 |
| MCV (fl) | 89.9 ± 2.1 | 90.2 ± 2.1 | 87.4 ± 1.8 | 88.0 ± 1.8 | 89.9 ± 5.1 | 90.6 ± 4.6 |
| MCH (pg) | 29.7 ± 0.9 | 29.6 ± 1.1 | 29.3 ± 0.5 | 29.6 ± 0.9 | 29.8 ± 1.9 | 30.0 ± 1.9 |
| Platelets (×103/µL) | 245 ± 55 | 239 ± 45 | 222 ± 45 | 222 ± 51 | 251 ± 89 | 246 ± 67 |
| WBC (×103/µL) | 6.7 ± 0.8 | 6.7 ± 1.6 | 6.5 ± 1.2 | 6.1 ± 0.6 | 7.1 ± 1.5 | 7.2 ± 2.3 |
| Transaminase GOT/AST (U/L) | 29.0 ± 7.7 | 24.9 ± 2.3 | 20.1 ± 6.3 | 22.6 ± 6.3 | 27.4 ± 13.8 | 26.7 ± 6.9 |
| Alkaline phosphatase (U/L) | 101 ± 29 | 88 ± 19 | 105 ± 25 | 99 ± 23 | 105 ± 18 | 98 ± 18 |
| Lactic dehydrogenase (U/L) | 200 ± 81 | 157 ± 17 | 155 ± 15 | 155 ± 18 | 196 ± 62 | 174 ± 45 |
| Total bilirubin (mg/dL) | 1.1 ± 0.5 | 1.3 ± 0.9 | 0.9 ± 0.4 | 0.6 ± 0.2 | 0.6 ± 0.2 | 0.6 ± 0.2 |
| Glycaemia (mg/dL) | 83.1 ± 7.5 | 86.6 ± 8.5 | 90.7 ± 4.4 | 88.9 ± 5.2 | 85.6 ± 4.1 | 86.3 ± 2.7 |
| Uric acid (mg/dL) | 4.7 ± 1.6 | 5.0 ± 1.7 | 5.1 ± 0.7 | 4.7 ± 1.0 | 4.7 ± 1.7 | 4.5 ± 1.0 |
| Total cholesterol (mg/dL) | 141 ± 21 | 138 ± 18 | 151 ± 33 | 143 ± 20 | 170 ± 28 | 156 ± 27 |
| Uric nitrogen (mg/dL) | 14.7 ± 2.9 | 14.3 ± 3.2 | 16.4 ± 3.2 | 14.5 ± 2.9 | 12.6 ± 1.6 | 12.4 ± 5.1 |
| Uraemia (mg/dL) | 31.4 ± 6.2 | 30.6 ± 6.8 | 35.0 ± 7.0 | 31.0 ± 6.2 | 27.0 ± 3.4 | 26.6 ± 10.9 |
| Calcium (mg/dL) | 9.8 ± 0.2 | 9.6 ± 0.2 | 9.8 ± 0.3 | 9.5 ± 0.3 | 9.8 ± 0.1 | 9.7 ± 0.2 |
| Phosphorous (mg/dL) | 4.0 ± 0.5 | 3.7 ± 0.6 | 3.6 ± 0.3 | 3.6 ± 0.6 | 3.5 ± 0.5 | 3.3 ± 0.5 |
| Total protein (g/dL) | 7.0 ± 0.5 | 7.0 ± 0.3 | 7.0 ± 0.4 | 7.0 ± 0.4 | 7.1 ± 0.2 | 7.1 ± 0.3 |
| Albumin (g/dL) | 4.7 ± 0.1 | 4.6 ± 0.1 | 4.7 ± 0.2 | 4.6 ± 0.2 | 4.7 ± 0.1 | 4.7 ± 0.2 |
| Dose/Time | n | ADP 4 µmol/L | ADP 8 µmol/L | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Maximal Amplitude (%) | AUC | Slope | Lag Time (s) | Maximal Amplitude (%) | AUC | Slope | Lag Time (s) | ||
| Placebo | |||||||||
| d1 0h | 33 | 68 ± 3 | 227 ± 12 | 84 ± 4 | 10 ± 0 | 79 ± 2 | 261 ± 9 | 93 ± 5 | 11 ± 0 |
| d1 3h | 33 | 70 ± 3 | 221 ± 10 | 80 ± 3 | 10 ± 0 | 82 ± 2 | 270 ± 10 | 95 ± 4 | 9 ± 0 |
| d5 0h | 33 | 67 ± 3 | 220 ± 10 | 81 ± 3 | 11 ± 0 | 83 ± 2 | 267 ± 8 | 93 ± 3 | 11 ± 0 |
| d5 3h | 32 | 65 ± 3 | 209 ± 9 | 77 ± 3 | 11 ± 0 | 80 ± 2 | 258 ± 8 | 91 ± 3 | 11 ± 0 |
| TP extract = 1.0 g | |||||||||
| d1 0h | 33 | 62 ± 3 | 206 ± 8 | 77 ± 6 | 11 ± 0 | 78 ± 2 | 258 ± 6 | 91 ± 7 | 11 ± 0 |
| d1 3h | 33 | 63 ± 3 | 208 ± 10 | 73 ± 3 | 11 ± 0 | 82 ± 2 | 259 ± 9 | 86 ± 4 | 10 ± 0 |
| d5 0h | 33 | 59 ± 3 | 193 ± 11 | 74 ± 3 | 12 ± 0 | 79 ± 3 | 250 ± 11 | 87 ± 4 | 12 ± 0 |
| d5 3h | 33 | 54 ± 4 * | 179 ± 12 * | 67 ± 3 | 12 ± 0 | 71 ± 4 | 228 ± 12 | 79 ± 4 | 12 ± 0 |
| TP extract = 2.5 g | |||||||||
| d1 0h | 33 | 65 ± 3 | 213 ± 11 | 81 ± 5 | 11 ± 0 | 80 ± 2 | 262 ± 7 | 97 ± 7 | 11 ± 0 |
| d1 3h | 31 | 62 ± 3 | 202 ± 12 | 74 ± 3 | 10 ± 0 | 78 ± 2 | 251 ± 7 | 84 ± 3 | 9 ± 0 |
| d5 0h | 33 | 64 ± 3 | 208 ± 9 | 76 ± 3 | 12 ± 0 | 81 ± 3 | 269 ± 7 | 91 ± 3 | 13 ± 0 |
| d5 3h | 32 | 62 ± 3 | 203 ± 9 | 77 ± 3 | 12 ± 0 | 82 ± 2 | 262 ± 7 | 88 ± 3 | 10 ± 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo, I.; Concha-Meyer, A.; Lutz, M.; Said, M.; Sáez, B.; Vásquez, A.; Fuentes, E. Chemical Characterization and Antiplatelet Potential of Bioactive Extract from Tomato Pomace (Byproduct of Tomato Paste). Nutrients 2019, 11, 456. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020456
Palomo I, Concha-Meyer A, Lutz M, Said M, Sáez B, Vásquez A, Fuentes E. Chemical Characterization and Antiplatelet Potential of Bioactive Extract from Tomato Pomace (Byproduct of Tomato Paste). Nutrients. 2019; 11(2):456. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020456
Chicago/Turabian StylePalomo, Ivan, Anibal Concha-Meyer, Mariane Lutz, Macarena Said, Bárbara Sáez, Adriana Vásquez, and Eduardo Fuentes. 2019. "Chemical Characterization and Antiplatelet Potential of Bioactive Extract from Tomato Pomace (Byproduct of Tomato Paste)" Nutrients 11, no. 2: 456. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11020456