Modelling the Association between Core and Discretionary Energy Intake in Adults with and without Obesity

 , , , and
, , , and
Abstract
:1. Background
2. Methods
2.1. Study Participants
2.2. Anthropometry
2.3. Background Questionnaires
2.4. Dietary Intake
2.5. Nutrient Analysis and Coding
2.6. Validity of Dietary Intake
2.7. Study Procedures
2.8. Statistical Analysis
3. Results
3.1. Relationship between Sociodemographic Variables and DEI and CEI
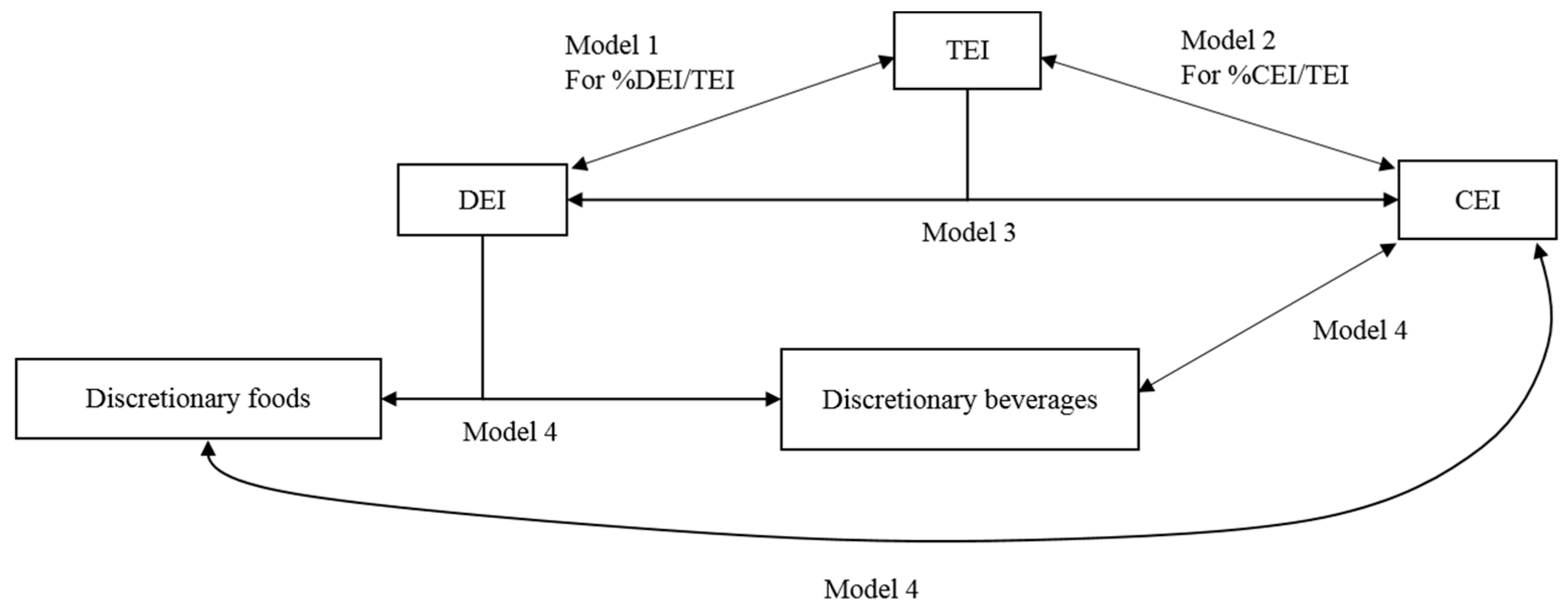
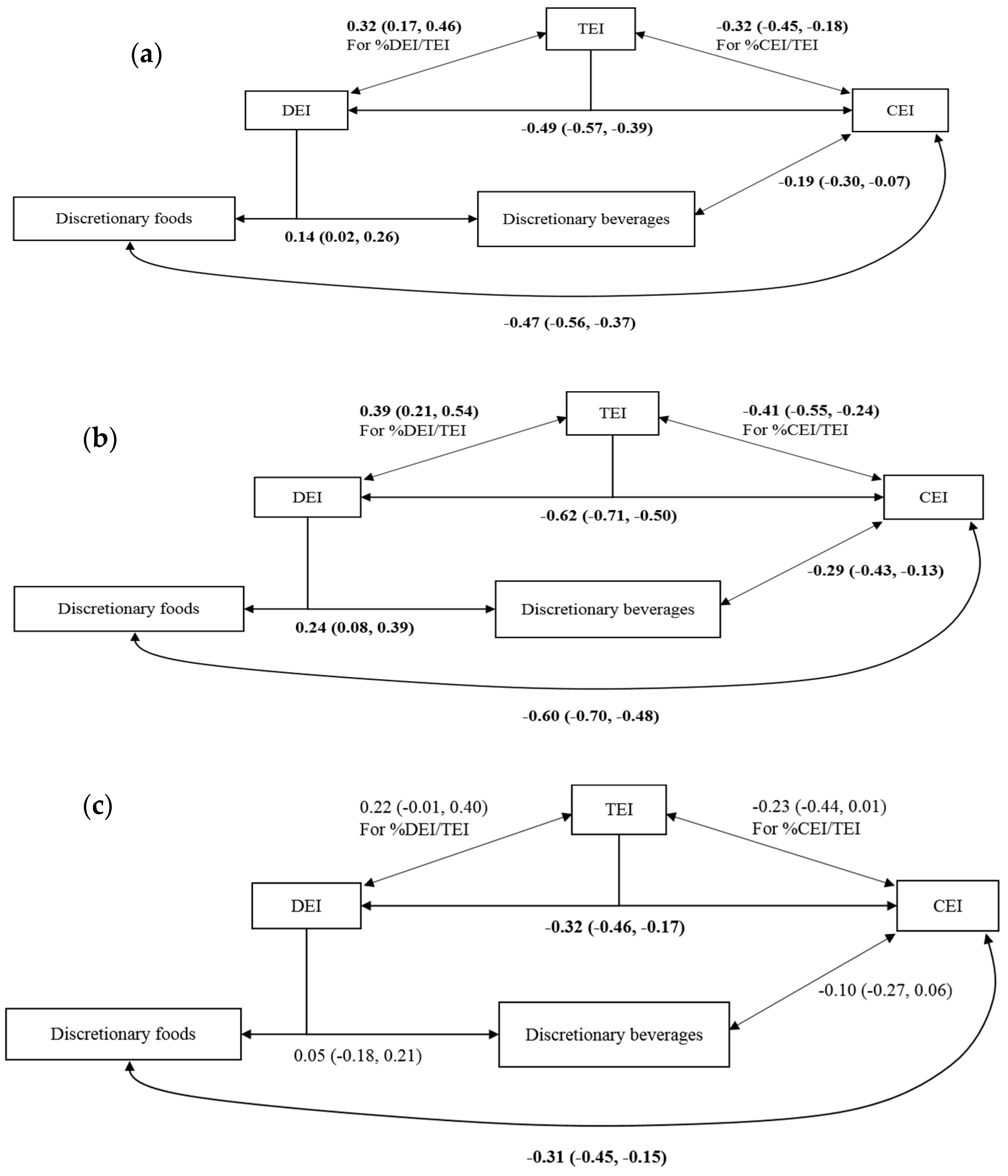
3.2. Relationship between TEI, DEI, and CEI by Obesity Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CEI | core energy intake |
| DEI | discretionary energy intake |
| SEIFA | socioeconomic indexes for areas |
| SSB | sugar-sweetened beverage |
| TEI | total energy intake |
References
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011−12 2015. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.007~2011-12~Main%20Features~Discretionary%20foods~700 (accessed on 17 September 2018).
- Cohen, D.A.; Sturm, R.; Scott, M.; Farley, T.A.; Bluthenthal, R. Not Enough Fruit and Vegetables or Too Many Cookies, Candies, Salty Snacks, and Soft Drinks? Public Health Rep. 2010, 125, 88–95. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines Canberra: Australian Government Department of Health. 2013. Available online: https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/n55_australian_dietary_guidelines_130530.pdf (accessed on 17 September 2018).
- Blundell, J.E.; Macdiarmid, J.I. Passive overconsumption. Fat intake and short-term energy balance. Ann. N. Y. Acad. Sci. 1997, 827, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–2015 Canberra, Australia: The Australian Government. 2015. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Overweight%20and%20obesity~22 (accessed on 2 December 2018).
- Tak, N.I.; Velde, S.J.; Singh, A.S.; Brug, J. The effects of a fruit and vegetable promotion intervention on unhealthy snacks during mid-morning school breaks: Results of the Dutch Schoolgruiten Project. J. Hum. Nutr. Diet. 2010, 23, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Øverby, N.C.; Klepp, K.-I.; Bere, E. Introduction of a school fruit program is associated with reduced frequency of consumption of unhealthy snacks. Am. J. Clin. Nutr. 2012, 96, 1100–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Human Services. Nutrition and Your Health: Dietary Guidelines for Americans. Part D: Discretionary Calories. 2005. Available online: https://health.gov/dietaryguidelines/dga2005/report/HTML/D3_DiscCalories.htm (accessed on 2 December 2018).
- Kant, A.K. Consumption of energy-dense, nutrient-poor foods by adult Americans: Nutritional and health implications. The third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Clin. Nutr. 2000, 72, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Sui, Z.X.; Wong, W.K.; Louie, J.C.Y.; Rangan, A. Discretionary food and beverage consumption and its association with demographic characteristics, weight status, and fruit and vegetable intakes in Australian adults. Public Health Nutr. 2017, 20, 274–281. [Google Scholar] [CrossRef]
- World Health Organization. The Challenge of Obesity in the WHO European Region and the Strategies for Response; World Health Organisation: Copenhagen, Denmark, 2007. [Google Scholar]
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; Department on Health and Ageing: Canberra, Australia, 2013.
- Capacci, S.; Mazzocchi, M.; Shankar, B.; Brambila Macias, J.; Verbeke, W.; Pérez-Cueto, F.J.; Kozioł-Kozakowska, A.; Piórecka, B.; Niedzwiedzka, B.; D’addesa, D.; et al. Policies to promote healthy eating in Europe: A structured review of policies and their effectiveness. Nutr. Rev. 2012, 70, 188–200. [Google Scholar] [CrossRef]
- Bell, E.A.; Rolls, B.J. Energy density of foods affects energy intake across multiple levels of fat content in lean and obese women. Am. J. Clin. Nutr. 2001, 73, 1010–1018. [Google Scholar] [CrossRef] [Green Version]
- Rolls, B.J.; Ello-Martin, J.A.; Tohill, B.C. What Can Intervention Studies Tell Us about the Relationship between Fruit and Vegetable Consumption and Weight Management? Blackwell Publishing Ltd.: Oxford, UK, 2004; pp. 1–17. [Google Scholar]
- Tanumihardjo, S.A.; Valentine, A.R.; Zhang, Z.; Whigham, L.D.; Lai, H.J.; Atkinson, R.L. Strategies to Increase Vegetable or Reduce Energy and Fat Intake Induce Weight Loss in Adults. Exp. Biol. Med. 2009, 234, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Batterham, M.J.; Thorne, R.L.; O’shea, J.E.; Grafenauer, S.J.; Probst, Y.C. Weight loss effects from vegetable intake: A 12-month randomised controlled trial. Eur. J. Clin. Nutr. 2014, 68, 778. [Google Scholar] [CrossRef]
- Lapointe, A.; Weisnagel, S.J.; Provencher, V.; Begin, C.; Dufour-Bouchard, A.A.; Trudeau, C.; Lemieux, S. Using restrictive messages to limit high-fat foods or nonrestrictive messages to increase fruit and vegetable intake: What works better for postmenopausal women? Eur. J. Clin. Nutr. 2010, 64, 194–202. [Google Scholar] [CrossRef]
- Looney, S.M.; Raynor, H.A. Are changes in consumption of “Healthy” foods related to changes in consumption of “Unhealthy” foods during pediatric obesity treatment? Int. J. Environ. Res. Public Health 2012, 9, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, K.A.; Brown, A.W.; Bohan Brown, M.M.; Shikany, J.M.; Mattes, R.D.; Allison, D.B. Increased fruit and vegetable intake has no discernible effect on weight loss: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Huda, M.S.B.; Wilding, J.P.H.; Pinkney, J.H. Gut peptides and the regulation of appetite. Obes. Rev. 2006, 7, 163–182. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Roberts, S.B. Dietary energy density and weight regulation. Nutr. Rev. 2001, 59, 247–258. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, F.; Hollis, J.H.; Mattes, R.D. Short-term dietary compensation in free-living adults. Physiol. Behav. 2008, 93, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Flatt, J.-P.; Volaufova, J.; DeLany, J.P.; Champagne, C.M. Corrective responses in human food intake identified from an analysis of 7-d food-intake records. Am. J. Clin. Nutr. 2008, 88, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- Houchins, J.A.; Tan, S.Y.; Campbell, W.W.; Mattes, R.D. Effects of fruit and vegetable, consumed in solid vs beverage forms, on acute and chronic appetitive responses in lean and obese adults. Int. J. Obes. 2013, 37, 1109–1115. [Google Scholar] [CrossRef]
- Mourao, D.M.; Bressan, J.; Campbell, W.W.; Mattes, R.D. Effects of food form on appetite and energy intake in lean and obese young adults. Int. J. Obes. 2007, 31, 1688–1695. [Google Scholar] [CrossRef] [Green Version]
- Cassady, B.A.; Considine, R.V.; Mattes, R.D. Beverage consumption, appetite, and energy intake: What did you expect? Am. J. Clin. Nutr. 2012, 95, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Mattes, R.; Campbell, W. Effects of food form and timing of ingestion on appetite and energy intake in lean young adults and in young adults with obesity. J. Am. Diet. Assoc. 2009, 109, 430–437. [Google Scholar] [CrossRef] [PubMed]
- DiMeglio, D.P.; Mattes, R.D. Liquid versus solid carbohydrate: Effects on food intake and body weight. Int. J. Obes. 2000, 24, 794–800. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Correlates of healthy fruit and vegetable diet in students in low, middle and high income countries. Int. J. Public Health 2015, 60, 79–90. [Google Scholar] [CrossRef]
- Tan, S.Y.; Dhillon, J.; Mattes, R.D. A review of the effects of nuts on appetite, food intake, metabolism, and body weight. Am. J. Clin. Nutr. 2014, 100, 412S–422S. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.A.; Stojanovski, E.; Moran, L.J.; Howe, P.R.C.; Coates, A.M. The Addition of Peanuts to Habitual Diets is Associated with Lower Consumption of Savory Non-Core Snacks by Men and Sweet Non-Core Snacks by Women. Nutr. Res. 2017, 41, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Jonnalagadda, S.S.; Harnack, L.; Hai Liu, R.; McKeown, N.; Seal, C.; Liu, S.; Fahey, G.C. Putting the Whole Grain Puzzle Together: Health Benefits Associated with Whole Grains—Summary of American Society for Nutrition 2010 Satellite Symposium. J. Nutr. 2011, 141, 1011S–1122S. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Perry, C.; Story, M. Correlates of fruit and vegetable intake among adolescents: Findings from Project EAT. Prev. Med. 2003, 37, 198–208. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Heimendinger, J.; Patterson, B.H.; Subar, A.F.; Kessler, R.; Pivonka, E. Psychosocial Factors Associated with Fruit and Vegetable Consumption. Am. J. Health Promot. 1995, 10, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Guillaumie, L.; Godin, G.; Vézina-Im, L.-A. Psychosocial determinants of fruit and vegetable intake in adult population: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 12. [Google Scholar] [CrossRef]
- John, J.H.; Ziebland, S. Reported barriers to eating more fruit and vegetables before and after participation in a randomized controlled trial: A qualitative study. Health Educ. Res. 2004, 19, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Socio-Economic Index for Australia 2011; Census of Population and Housing; The Government of Australia: Canberra, Australia, 2013.
- FoodWorks 9. Professional Edition 9.0.3973 ed.; Xyris: High Gate Hill, Australia, 2017. [Google Scholar]
- Kelly, B.; Halford, J.C.; Boyland, E.J.; Chapman, K.; Bautista-Castaño, I.; Berg, C.; Caroli, M.; Cook, B.; Coutinho, J.G.; Effertz, T.; et al. Television food advertising to children: A global perspective. Am. J. Public Health 2010, 100, 1730–1736. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, E.; Colagiuri, S.; Magnusson, R. An audit of food and beverage advertising on the Sydney metropolitan train network: Regulation and policy implications. Bmc Public Health 2017, 17, 490. [Google Scholar] [CrossRef] [PubMed]
- Flood, J.E.; Rolls, B.J. Soup preloads in a variety of forms reduce meal energy intake. Appetite 2007, 49, 626–634. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy-intake data using fundamental principles of energy physiology—Derivation of cutoff limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Human Basal Metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Greene, W.H. Econometric Analysis; Pearson Education: Delhi, Indian, 2003. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Almiron-Roig, E.; Palla, L.; Guest, K.; Ricchiuti, C.; Vint, N.; Jebb, S.A.; Drewnowski, A. Factors that determine energy compensation: A systematic review of preload studies. Nutr. Rev. 2013, 71, 458–473. [Google Scholar] [CrossRef] [PubMed]
- Lenne, R.L.; Panos, M.E.; Auster-Gussman, L.; Scherschel, H.; Zhou, L.; Mann, T. Behavioral compensation before and after eating at the Minnesota State Fair. Appetite 2017, 118, 113–119. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Sinclair, K.B.; Pereira, M.A.; Garcia-Lago, E.; Feldman, H.A.; Ludwig, D.S. Compensation for energy intake from fast food among overweight and lean adolescents. JAMA 2004, 291, 2828–2833. [Google Scholar] [CrossRef]
- Wiessing, K.R.; Xin, L.; Budgett, S.C.; Poppitt, S.D. No evidence of enhanced satiety following whey protein- or sucrose-enriched water beverages: A dose response trial in overweight women. Eur. J. Clin. Nutr. 2015, 69, 1238. [Google Scholar] [CrossRef]
- Glasbrenner, B.; Pieramico, O.; Brecht-Krau, D.; Baur, M.; Malfertheiner, P. Gastric emptying of solids and liquids in obesity. Clin. Investig. 1993, 71, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Hoad, C.L.; Rayment, P.; Spiller, R.C.; Marciani, L.; Alonso, B.D.; Traynor, C.; Mela, D.J.; Peters, H.P.; Gowland, P.A. In vivo imaging of intragastric gelation and its effect on satiety in humans. J. Nutr. 2004, 134, 2293–2300. [Google Scholar] [CrossRef] [PubMed]
- Lavin, J.H.; French, S.J.; Ruxton, C.H.S.; Read, N.W. An investigation of the role of oro-sensory stimulation in sugar satiety. Int. J. Obes. 2002, 26, 384–388. [Google Scholar] [CrossRef] [PubMed]
- French, S.J.; Cecil, J.E. Oral, gastric and intestinal influences on human feeding. Physiol. Behav. 2001, 74, 729–734. [Google Scholar] [CrossRef]
- Leidy, H.J.; Apolzan, J.W.; Mattes, R.D.; Campbell, W.W. Food form and portion size affect postprandial appetite sensations and hormonal responses in healthy, nonobese, older adults. Obesity 2010, 18, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E.; Gillett, A. Control of food intake in the obese. Obes. Res. 2001, 9, 263S–270S. [Google Scholar] [CrossRef]
- Speechly, D.P.; Buffenstein, R. Appetite dysfunction in obese males: Evidence for role of hyperinsulinaemia in passive overconsumption with a high fat diet. Eur. J. Clin. Nutr. 2000, 54, 225. [Google Scholar] [CrossRef]
- Dalton, M.; Hollingworth, S.; Blundell, J.; Finlayson, G. Weak satiety responsiveness is a reliable trait associated with hedonic risk factors for overeating among women. Nutrients 2015, 7, 7421–7436. [Google Scholar] [CrossRef]
- Hays, N.P.; Bathalon, G.P.; McCrory, M.A.; Roubenoff, R.; Lipman, R.; Roberts, S.B. Eating behavior correlates of adult weight gain and obesity in healthy women aged 55–65 y. Am. J. Clin. Nutr. 2002, 75, 476–483. [Google Scholar] [CrossRef]
- Hendrikse, J.J.; Cachia, R.L.; Kothe, E.J.; McPhie, S.; Skouteris, H.; Hayden, M.J. Attentional biases for food cues in overweight and individuals with obesity: A systematic review of the literature. Obes. Rev. 2015, 16, 424–432. [Google Scholar] [CrossRef]
- Stice, E.; Spoor, S.; Ng, J.; Zald, D.H. Relation of obesity to consummatory and anticipatory food reward. Physiol. Behav. 2009, 97, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Herman, C.P.; Verheijden, M.W. Dietary restraint and body mass change. A 3-year follow up study in a representative Dutch sample. Appetite 2014, 76, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Gersovitz, M.; Madden, J.P.; Smiciklas-Wright, H. Validity of the 24-hr. dietary recall and seven-day record for group comparisons. J. Am. Diet. Assoc. 1978, 73, 48–55. [Google Scholar] [PubMed]
- Chao, A.M.; White, M.A.; Grilo, C.M.; Sinha, R. Examining the effects of cigarette smoking on food cravings and intake, depressive symptoms, and stress. Eat. Behav. 2017, 24, 61–65. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Explanatory Variables | All Participants (n = 93) | |
|---|---|---|
| DEI | CEI | |
| Male | 21 (−893, 935) | 2313 (1430, 3196) |
| 35–64 years | −1246 (−2355, −136) | 929 (−144, 2002) |
| ≥65 years | −2281 (−3494, −1068) | 519 (−654, 1691) |
| Completed or undertaking post-high school education | −342 (−1022, 339) | 457 (−200, 1115) |
| Obesity | 1313 (253, 2373) | −471 (−1496, 555) |
| Weekend | 650 (118, 1182) | −161 (−577, 255) |
| Top SEIFA quintile | 153 (−577, 883) | −855 (−1561, −149) |
| Variables Included in Simultaneous Equations | All Participants | Healthy Weight Participants | Participants with Obesity |
|---|---|---|---|
| Model 1 | |||
| TEI and %DEI/TEI | 0.32 (0.17, 0.46) | 0.39 (0.21, 0.54) | 0.22 (−0.01, 0.40) |
| Model 2 | |||
| TEI and %CEI/TEI | −0.32 (−0.45, −0.18) | −0.41 (−0.55, −0.24) | −0.23 (−0.44, 0.00) |
| Model 3 | |||
| DEI and CEI | −0.49 (−0.57, −0.39) | −0.67 (−0.71, −0.50) | −0.32 (−0.46, −0.17) |
| Model 4 | |||
| Discretionary food and discretionary beverages | 0.14 (0.02, 0.26) | 0.24 (0.08, 0.39) | 0.05 (−0.18, 0.21) |
| Discretionary food and CEI | −0.47 (−0.56, −0.37) | −0.60 (−0.70, −0.48) | −0.31 (−0.45, −0.15) |
| Discretionary beverages and CEI | −0.19 (−0.30, −0.07) | −0.29 (−0.43, −0.13) | −0.10 (−0.27, 0.06) |
| Observations | 364 | 183 | 185 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, M.; Li, A.; Hill, A.J.; Cunich, M.; Skilton, M.R.; Madigan, C.D.; Caterson, I.D. Modelling the Association between Core and Discretionary Energy Intake in Adults with and without Obesity. Nutrients 2019, 11, 683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030683
Fong M, Li A, Hill AJ, Cunich M, Skilton MR, Madigan CD, Caterson ID. Modelling the Association between Core and Discretionary Energy Intake in Adults with and without Obesity. Nutrients. 2019; 11(3):683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030683
Chicago/Turabian StyleFong, Mackenzie, Ang Li, Andrew J Hill, Michelle Cunich, Michael R Skilton, Claire D Madigan, and Ian D Caterson. 2019. "Modelling the Association between Core and Discretionary Energy Intake in Adults with and without Obesity" Nutrients 11, no. 3: 683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11030683