Randomized Trial of Marine n-3 Polyunsaturated Fatty Acids for the Prevention of Cerebral Small Vessel Disease and Inflammation in Aging (PUFA Trial): Rationale, Design and Baseline Results

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. N-3 PUFA Composition and Dose
2.3. Study Population
2.4. Outcome Measures
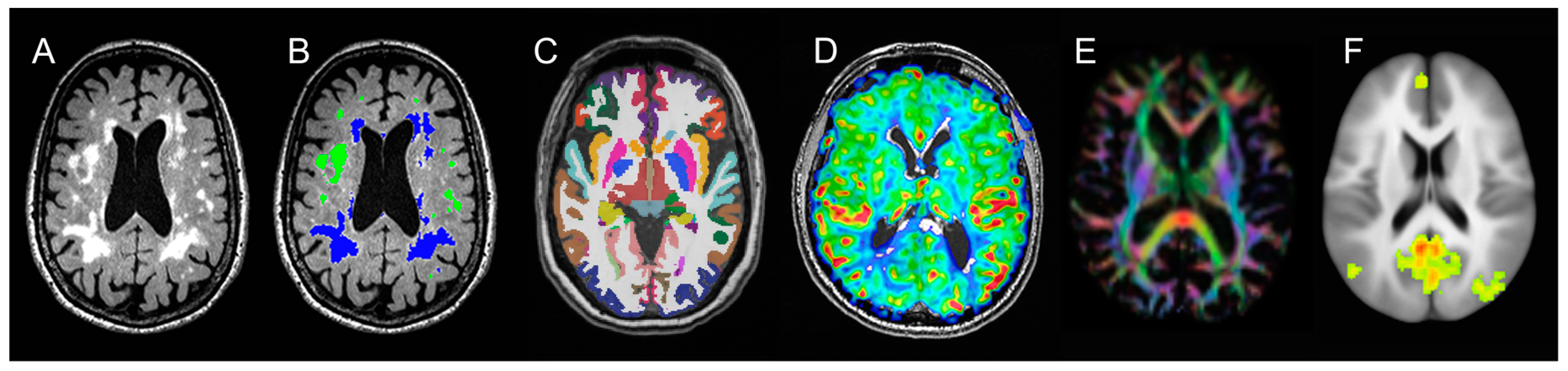
2.4.1. Neuroimaging
2.4.2. Blood-Based Biomarkers
2.4.3. Neuropsychological Test Battery
2.4.4. Diet and Other Measures
2.5. Recruitment and Randomization
2.5.1. Sources of Participants
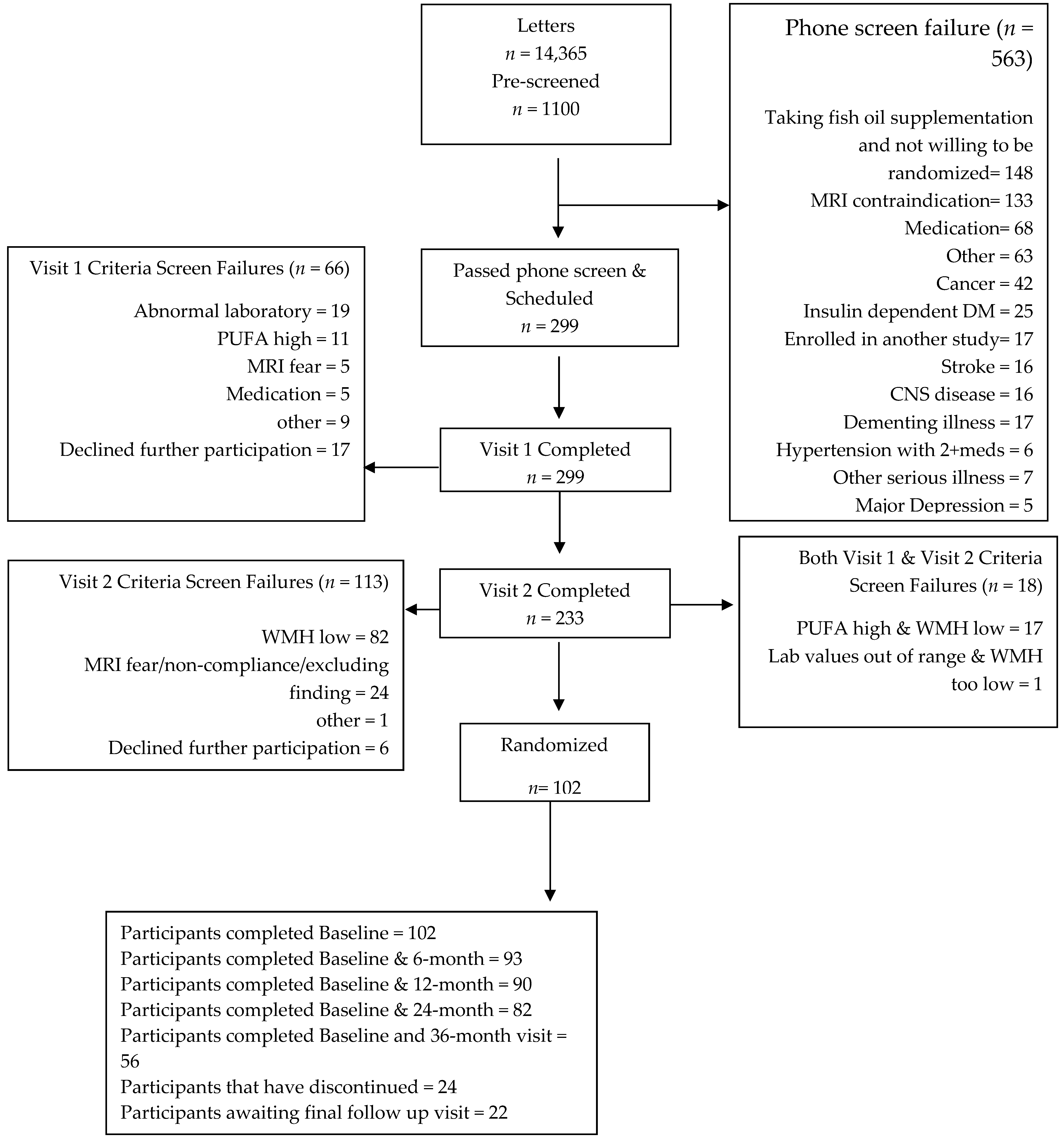
2.5.2. Enrollment
Ethnicity of Study Population
2.5.3. Randomization
2.5.4. Blinding
2.6. Assessment of Compliance
2.7. Analytical Approach and Statistical Power
2.7.1. Analytical Approach
Modified Intention-To-Treat Analysis
Per-Protocol Analysis
2.7.2. Statistical Power
Sample Size Calculations
2.8. Trial Monitoring
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; Decarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American heart association/American stroke association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef]
- Unverzagt, F.W.; McClure, L.A.; Wadley, V.G.; Jenny, N.S.; Go, R.C.; Cushman, M.; Kissela, B.M.; Kelley, B.J.; Kennedy, R.; Moy, C.S.; et al. Vascular risk factors and cognitive impairment in a stroke-free cohort. Neurology 2011, 77, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef]
- Dodge, H.H.; Chang, C.C.; Kamboh, I.M.; Ganguli, M. Risk of Alzheimer’s disease incidence attributable to vascular disease in the population. Alzheimers Dement. 2011, 7, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L.; Quinn, J.F. Alzheimer’s disease and the Blood-Brain Barrier: Past, Present, and Future. Aging Health 2008, 4, 47–55. [Google Scholar] [CrossRef] [PubMed]
- DeKosky, S.T.; Williamson, J.D.; Fitzpatrick, A.L.; Kronmal, R.A.; Ives, D.G.; Saxton, J.A.; Lopez, O.L.; Burke, G.; Carlson, M.C.; Fried, L.P.; et al. Ginkgo biloba for prevention of dementia: A randomized controlled trial. JAMA 2008, 300, 2253–2262. [Google Scholar] [CrossRef]
- Andrieu, S.; Guyonnet, S.; Coley, N.; Cantet, C.; Bonnefoy, M.; Bordes, S.; Bories, L.; Cufi, M.N.; Dantoine, T.; Dartigues, J.F.; et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): A randomised, placebo-controlled trial. Lancet Neurol. 2017, 16, 377–389. [Google Scholar] [CrossRef]
- Silbert, L.C.; Nelson, C.; Howieson, D.B.; Moore, M.M.; Kaye, J.A. Impact of white matter hyperintensity volume progression on the rate of cognitive and motor decline. Neurology 2008, 71, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Silbert, L.C.; Howieson, D.B.; Dodge, H.; Kaye, J.A. Cognitive impairment risk: White matter hyperintensity progression matters. Neurology 2009, 73, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Dufouil, C.; Chalmers, J.; Coskun, O.; Besancon, V.; Bousser, M.G.; Guillon, P.; MacMahon, S.; Mazoyer, B.; Neal, B.; Woodward, M.; et al. Effects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: The PROGRESS (Perindopril Protection Against Recurrent Stroke Study) Magnetic Resonance Imaging Substudy. Circulation 2005, 112, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.K.; Siscovick, D.S.; Longstreth, W.T., Jr.; Kuller, L.H.; Mozaffarian, D. Fish consumption and risk of subclinical brain abnormalities on MRI in older adults. Neurology 2008, 71, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Bowman, G.L.; Silbert, L.C.; Howieson, D.; Dodge, H.H.; Traber, M.G.; Frei, B.; Kaye, J.A.; Shannon, J.; Quinn, J.F. Nutrient biomarker patterns, cognitive function, and MRI measures of brain aging. Neurology 2012, 78, 241–249. [Google Scholar] [CrossRef]
- Tan, Z.S.; Harris, W.S.; Beiser, A.S.; Au, R.; Himali, J.J.; Debette, S.; Pikula, A.; Decarli, C.; Wolf, P.A.; Vasan, R.S.; et al. Red blood cell omega-3 fatty acid levels and markers of accelerated brain aging. Neurology 2012, 78, 658–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtanen, J.K.; Siscovick, D.S.; Lemaitre, R.N.; Longstreth, W.T.; Spiegelman, D.; Rimm, E.B.; King, I.B.; Mozaffarian, D. Circulating omega-3 polyunsaturated fatty acids and subclinical brain abnormalities on MRI in older adults: The Cardiovascular Health Study. J. Am. Heart Assoc. 2013, 2, e000305. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Bouwens, M.; van de Rest, O.; Dellschaft, N.; Bromhaar, M.G.; de Groot, L.C.; Geleijnse, J.M.; Muller, M.; Afman, L.A. Fish-oil supplementation induces antiinflammatory gene expression profiles in human blood mononuclear cells. Am. J. Clin. Nutr. 2009, 90, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cawood, A.L.; Ding, R.; Napper, F.L.; Young, R.H.; Williams, J.A.; Ward, M.J.; Gudmundsen, O.; Vige, R.; Payne, S.P.; Ye, S.; et al. Eicosapentaenoic acid (EPA) from highly concentrated n-3 fatty acid ethyl esters is incorporated into advanced atherosclerotic plaques and higher plaque EPA is associated with decreased plaque inflammation and increased stability. Atherosclerosis 2010, 212, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Bazan, N.G. Docosanoids and elovanoids from omega-3 fatty acids are pro-homeostatic modulators of inflammatory responses, cell damage, and neuroprotection. Mol. Asp. Med. 2018, 64, 18–33. [Google Scholar] [CrossRef]
- Hogg, J.C.; James, A.L.; Pare, P.D. Evidence for inflammation in asthma. Am. Rev. Respir. Dis. 1991, 143, S39–S42. [Google Scholar] [CrossRef]
- Witkowska, A.M.; Borawska, M.H. Soluble intercellular adhesion molecule-1 (sICAM-1): An overview. Eur. Cytokine Netw. 2004, 15, 91–98. [Google Scholar]
- Jun, C.D.; Shimaoka, M.; Carman, C.V.; Takagi, J.; Springer, T.A. Dimerization and the effectiveness of ICAM-1 in mediating LFA-1-dependent adhesion. Proc. Natl. Acad. Sci. USA 2001, 98, 6830–6835. [Google Scholar] [CrossRef] [Green Version]
- Jun, C.D.; Carman, C.V.; Redick, S.D.; Shimaoka, M.; Erickson, H.P.; Springer, T.A. Ultrastructure and function of dimeric, soluble intercellular adhesion molecule-1 (ICAM-1). J. Biol. Chem. 2001, 276, 29019–29027. [Google Scholar] [CrossRef]
- Dietrich, J.B. The adhesion molecule ICAM-1 and it’s regulation in relation to the blood-brain barrier. J. Neuroimmunol. 2002, 128, 58–68. [Google Scholar] [CrossRef]
- Camacho, S.A.; Heath, W.R.; Carbone, F.R.; Sarvetnick, N.; LeBon, A.; Karlsson, L.; Peterson, P.A.; Webb, S.R. A key role for ICAM-1 in generating effector cells mediating inflammatory responses. Nat. Immunol. 2001, 2, 523–529. [Google Scholar] [CrossRef]
- Debette, S.; Markus, H.S. The genetics of cervical artery dissection: A systematic review. Stroke 2009, 40, e459–e466. [Google Scholar] [CrossRef]
- Hassan, A.; Gormley, K.; O’Sullivan, M.; Knight, J.; Sham, P.; Vallance, P.; Bamford, J.; Markus, H. Endothelial nitric oxide gene haplotypes and risk of cerebral small-vessel disease. Stroke 2004, 35, 654–659. [Google Scholar] [CrossRef]
- Markus, H.S.; Hunt, B.; Palmer, K.; Enzinger, C.; Schmidt, H.; Schmidt, R. Markers of endothelial and hemostatic activation and progression of cerebral white matter hyperintensities: Longitudinal results of the Austrian Stroke Prevention Study. Stroke 2005, 36, 1410–1414. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Wong, K.S.; Wang, Y.Y.; Fu, J.H.; Ding, D.; Hong, Z. Plasma level of sICAM-1 is associated with the extent of white matter lesion among asymptomatic elderly subjects. Clin. Neurol. Neurosurg. 2009, 111, 847–851. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, F.E.; de Kleine, M.; Frijns, C.J.; Fijnheer, R.; van Gijn, J.; Kappelle, L.J. Endothelial cell activation is associated with cerebral white matter lesions in patients with cerebrovascular disease. Ann. N. Y. Acad. Sci. 2002, 977, 306–314. [Google Scholar] [CrossRef]
- Ibrahim-Verbaas, C.A.; Bressler, J.; Debette, S.; Schuur, M.; Smith, A.V.; Bis, J.C.; Davies, G.; Trompet, S.; Smith, J.A.; Wolf, C.; et al. GWAS for executive function and processing speed suggests the involvement of the CADM2 gene. Mol. Psychiatry 2016, 21, 189–197. [Google Scholar] [CrossRef]
- Bowman, G.L.; Dayon, L.; Kirkland, R.; Wojcik, J.; Peyratout, G.; Severin, I.C.; Henry, H.; Oikonomidi, A.; Migliavacca, E.; Bacher, M.; et al. Blood-brain barrier breakdown, neuroinflammation, and cognitive decline in older adults. Alzheimers Dement. 2018, 14, 1640–1650. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- Freund-Levi, Y.; Eriksdotter-Jonhagen, M.; Cederholm, T.; Basun, H.; Faxen-Irving, G.; Garlind, A.; Vedin, I.; Vessby, B.; Wahlund, L.O.; Palmblad, J. Omega-3 fatty acid treatment in 174 patients with mild to moderate Alzheimer disease: OmegAD study: A randomized, double-blind trial. Arch. Neurol. 2006, 63, 1402–1408. [Google Scholar] [CrossRef]
- Quinn, J.F.; Raman, R.; Thomas, R.G.; Yurko-Mauro, K.; Nelson, E.B.; Van Dyck, C.; Galvin, J.E.; Emond, J.; Jack, C.R., Jr.; Weiner, M.; et al. Docosahexaenoic acid supplementation and cognitive decline in Alzheimer disease: A randomized trial. JAMA 2010, 304, 1903–1911. [Google Scholar] [CrossRef]
- Huang, T.L.; Zandi, P.P.; Tucker, K.L.; Fitzpatrick, A.L.; Kuller, L.H.; Fried, L.P.; Burke, G.L.; Carlson, M.C. Benefits of fatty fish on dementia risk are stronger for those without APOE epsilon4. Neurology 2005, 65, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Koffie, R.M.; Hashimoto, T.; Tai, H.C.; Kay, K.R.; Serrano-Pozo, A.; Joyner, D.; Hou, S.; Kopeikina, K.J.; Frosch, M.P.; Lee, V.M.; et al. Apolipoprotein E4 effects in Alzheimer’s disease are mediated by synaptotoxic oligomeric amyloid-beta. Brain 2012, 135, 2155–2168. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Serrano-Pozo, A.; Hori, Y.; Adams, K.W.; Takeda, S.; Banerji, A.O.; Mitani, A.; Joyner, D.; Thyssen, D.H.; Bacskai, B.J.; et al. Apolipoprotein E, especially apolipoprotein E4, increases the oligomerization of amyloid beta peptide. J. Neurosci. 2012, 32, 15181–15192. [Google Scholar] [CrossRef]
- Lim, Y.Y.; Mormino, E.C. Alzheimer’s Disease Neuroimaging I: APOE genotype and early beta-amyloid accumulation in older adults without dementia. Neurology 2017, 89, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Corrada, M.M.; Brookmeyer, R.; Berlau, D.; Paganini-Hill, A.; Kawas, C.H. Prevalence of dementia after age 90: Results from the 90+ study. Neurology 2008, 71, 337–343. [Google Scholar] [CrossRef]
- Jellinger, K.A.; Attems, J. Is there pure vascular dementia in old age? J. Neurol. Sci. 2010, 299, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Middleton, L.E.; Lui, L.Y.; Spira, A.P.; Stone, K.; Racine, C.; Ensrud, K.E.; Kramer, J.H. Mild cognitive impairment, dementia, and their subtypes in oldest old women. Arch. Neurol. 2011, 68, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Ammar, R.; Besson, D.; Zhao, X.; Anderson, S.; Frolov, V.V.; Kubota, Y.; Lee, S.J.; Li, S.Z.; Poling, R.; Smith, A.; et al. Observation of the decay Omega(0)(c)-->Omega(-)e(+)nu(e). Phys. Rev. Lett. 2002, 89, 171803. [Google Scholar] [CrossRef]
- Iso, H.; Rexrode, K.M.; Stampfer, M.J.; Manson, J.E.; Colditz, G.A.; Speizer, F.E.; Hennekens, C.H.; Willett, W.C. Intake of fish and omega-3 fatty acids and risk of stroke in women. JAMA 2001, 285, 304–312. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Longstreth, W.T., Jr.; Lemaitre, R.N.; Manolio, T.A.; Kuller, L.H.; Burke, G.L.; Siscovick, D.S. Fish consumption and stroke risk in elderly individuals: The cardiovascular health study. Arch. Intern. Med. 2005, 165, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Leaf, A.; Kang, J.X.; Xiao, Y.F. Omega-3 fatty acids and ventricular arrhythmias. World Rev. Nutr. Diet. 2005, 94, 129–138. [Google Scholar]
- Bowman, G.L.; Dodge, H.H.; Mattek, N.; Barbey, A.K.; Silbert, L.C.; Shinto, L.; Howieson, D.B.; Kaye, J.A.; Quinn, J.F. Plasma omega-3 PUFA and white matter mediated executive decline in older adults. Front. Aging Neurosci. 2013, 5, 92. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liang, X.; Wang, L.; Lu, X.; Huang, J.; Cao, J.; Li, H.; Gu, D. Effect of omega-3 fatty acids supplementation on endothelial function: A meta-analysis of randomized controlled trials. Atherosclerosis 2012, 221, 536–543. [Google Scholar] [CrossRef]
- Serhan, C.N. Pro-resolving lipid mediators are leads for resolution physiology. Nature 2014, 510, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Promjunyakul, N.; Lahna, D.; Kaye, J.A.; Dodge, H.H.; Erten-Lyons, D.; Rooney, W.D.; Silbert, L.C. Characterizing the white matter hyperintensity penumbra with cerebral blood flow measures. Neuroimage Clin. 2015, 8, 224–229. [Google Scholar] [CrossRef] [Green Version]
- Samieri, C.; Maillard, P.; Crivello, F.; Proust-Lima, C.; Peuchant, E.; Helmer, C.; Amieva, H.; Allard, M.; Dartigues, J.F.; Cunnane, S.C.; et al. Plasma long-chain omega-3 fatty acids and atrophy of the medial temporal lobe. Neurology 2012, 79, 642–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovicich, J.; Czanner, S.; Han, X.; Salat, D.; van der Kouwe, A.; Quinn, B.; Pacheco, J.; Albert, M.; Killiany, R.; Blacker, D.; et al. MRI-derived measurements of human subcortical, ventricular and intracranial brain volumes: Reliability effects of scan sessions, acquisition sequences, data analyses, scanner upgrade, scanner vendors and field strengths. Neuroimage 2009, 46, 177–192. [Google Scholar] [CrossRef] [Green Version]
- Desikan, R.S.; Cabral, H.J.; Hess, C.P.; Dillon, W.P.; Glastonbury, C.M.; Weiner, M.W.; Schmansky, N.J.; Greve, D.N.; Salat, D.H.; Buckner, R.L.; et al. Automated MRI measures identify individuals with mild cognitive impairment and Alzheimer’s disease. Brain 2009, 132, 2048–2057. [Google Scholar] [CrossRef]
- Witte, A.V.; Kerti, L.; Hermannstadter, H.M.; Fiebach, J.B.; Schreiber, S.J.; Schuchardt, J.P.; Hahn, A.; Floel, A. Long-chain omega-3 fatty acids improve brain function and structure in older adults. Cereb. Cortex 2014, 24, 3059–3068. [Google Scholar] [CrossRef]
- Johnston, D.T.; Deuster, P.A.; Harris, W.S.; Macrae, H.; Dretsch, M.N. Red blood cell omega-3 fatty acid levels and neurocognitive performance in deployed U.S. Servicemembers. Nutr. Neurosci. 2013, 16, 30–38. [Google Scholar] [CrossRef]
- Bligh, E.G.; Dyer, W.J. A rapid method of total lipid extraction and purification. Can. J. Biochem. Physiol. 1959, 37, 911–917. [Google Scholar] [CrossRef]
- Bowman, G.L.; Shannon, J.; Ho, E.; Traber, M.G.; Frei, B.; Oken, B.S.; Kaye, J.A.; Quinn, J.F. Reliability and validity of food frequency questionnaire and nutrient biomarkers in elders with and without mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 2011, 25, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, E.A.; Geisler, M.W.; Squires, N.K. Construct validity in the Trail Making Test: What makes Part B harder? J. Clin. Exp. Neuropsychol. 1995, 17, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. What do adult age differences in the Digit Symbol Substitution Test reflect? J. Gerontol. 1992, 47, P121–P128. [Google Scholar] [CrossRef]
- Ivanova, I.; Salmon, D.P.; Gollan, T.H. The multilingual naming test in Alzheimer’s disease: Clues to the origin of naming impairments. J. Int. Neuropsychol. Soc. 2013, 19, 272–283. [Google Scholar] [CrossRef]
- Craft, S.; Asthana, S.; Schellenberg, G.; Baker, L.; Cherrier, M.; Boyt, A.A.; Martins, R.N.; Raskind, M.; Peskind, E.; Plymate, S. Insulin effects on glucose metabolism, memory, and plasma amyloid precursor protein in Alzheimer’s disease differ according to apolipoprotein-E genotype. Ann. N. Y. Acad. Sci. 2000, 903, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dong, Y.; Sharma, V.K.; Chan, B.P.; Venketasubramanian, N.; Teoh, H.L.; Seet, R.C.; Tanicala, S.; Chan, Y.H.; Chen, C. The Montreal Cognitive Assessment (MoCA) is superior to the Mini-Mental State Examination (MMSE) for the detection of vascular cognitive impairment after acute stroke. J. Neurol. Sci. 2010, 299, 15–18. [Google Scholar] [CrossRef]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar] [PubMed]
- Galasko, D.; Bennett, D.; Sano, M.; Ernesto, C.; Thomas, R.; Grundman, M.; Ferris, S. An inventory to assess activities of daily living for clinical trials in Alzheimer’s disease. The Alzheimer’s Disease Cooperative Study. Alzheimer Dis. Assoc. Disord. 1997, 11 (Suppl. 2), S33–S39. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.R.; Parsons, T.D.; Sidtis, J.J.; Hanlon Inman, T.; Robertson, W.T.; Hall, C.D.; Price, R.W. Timed Gait test: Normative data for the assessment of the AIDS dementia complex. J. Clin. Exp. Neuropsychol. 2006, 28, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Schouten, H.J. Adaptive biased urn randomization in small strata when blinding is impossible. Biometrics 1995, 51, 1529–1535. [Google Scholar] [CrossRef]
- Little, R.J.A.; Rubin, D.B. Statistical Analysis with Missing Data, 3rd ed.; Wiley Interscience: Hoboken, NJ, USA, 2019. [Google Scholar]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Rossetti, H.C.; Lacritz, L.H.; Cullum, C.M.; Weiner, M.F. Normative data for the Montreal Cognitive Assessment (MoCA) in a population-based sample. Neurology 2011, 77, 1272–1275. [Google Scholar] [CrossRef]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef] [Green Version]
- Zamroziewicz, M.K.; Paul, E.J.; Zwilling, C.E.; Barbey, A.K. Predictors of Memory in Healthy Aging: Polyunsaturated Fatty Acid Balance and Fornix White Matter Integrity. Aging Dis. 2017, 8, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Hughes, M.C.B.; Ungerer, J.P.; Green, A.C. Plasma eicosapentaenoic acid is negatively associated with all-cause mortality among men and women in a population-based prospective study. Nutr. Res. 2016, 36, 1202–1209. [Google Scholar] [CrossRef]
- DeCarli, C.; Massaro, J.; Harvey, D.; Hald, J.; Tullberg, M.; Au, R.; Beiser, A.; D’Agostino, R.; Wolf, P.A. Measures of brain morphology and infarction in the Framingham heart study: Establishing what is normal. Neurobiol. Aging 2005, 26, 491–510. [Google Scholar] [CrossRef]
- Van Leijsen, E.M.C.; Tay, J.; van Uden, I.W.M.; Kooijmans, E.C.M.; Bergkamp, M.I.; van der Holst, H.M.; Ghafoorian, M.; Platel, B.; Norris, D.G.; Kessels, R.P.C.; et al. Memory decline in elderly with cerebral small vessel disease explained by temporal interactions between white matter hyperintensities and hippocampal atrophy. Hippocampus 2018. [Google Scholar] [CrossRef] [PubMed]
- Maillard, P.; Crivello, F.; Dufouil, C.; Tzourio-Mazoyer, N.; Tzourio, C.; Mazoyer, B. Longitudinal follow-up of individual white matter hyperintensities in a large cohort of elderly. Neuroradiology 2009, 51, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.; Wen, W.; Chen, X.; Brodaty, H. Progression of white matter hyperintensities in elderly individuals over 3 years. Neurology 2007, 68, 214–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ten Dam, V.H.; van den Heuvel, D.M.; van Buchem, M.A.; Westendorp, R.G.; Bollen, E.L.; Ford, I.; de Craen, A.J.; Blauw, G.J.; Group, P.S. Effect of pravastatin on cerebral infarcts and white matter lesions. Neurology 2005, 64, 1807–1809. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sequence | Orientation | Number of Volumes | Acquisition Matrix | Slice Thickness (mm) | # of Slices | TR (ms) | TE (ms) | TI (ms) | Flip Angle | In Plane Resolution (mm) |
|---|---|---|---|---|---|---|---|---|---|---|
| T1 MPRAGE | Axial | 1 | 256 × 192 | 1 | 144 | 2300 | 3.45 | 1200 | 12° | 1 × 1 |
| FLAIR | 3D | 1 | 512 × 512 | 1 | 160 | 6000 | 388 | 2100 | 120° | 0.488 × 0.488 |
| PCASL | Axial | 1 M0, 252 | 64 × 64 | 4 | 10 | 3500 | 13 | - | 90° | 3 × 3 |
| DTI | Axial | 30 dirs., 6B0, 2avg | 128 × 128 | 2 | 72 | 9100 | 88 | - | 90° | 2 × 2 |
| Diffusion Field map | Axial | 1 | 120 × 120 | 2 | 72 | 790 | 5.19 | - | 60° | 2 × 2 |
| T2 | Axial | 1 | 256 × 256 | 4 | 28 | 693 | 20 | - | 20° | 0.859 × 0.859 |
| PD—T2 TSE | Axial | 2 | 256 × 232 | 3 | 48 | 3000 | 11 | - | 150° | 0.938 × 0.938 |
| Resting state fMRI | Axial | 170 | 128 × 128 | 4 | 30 | 2020 | 38 | - | 80° | 1.875 × 1.875 |
| N | Total | A | B | p for Diff | |
|---|---|---|---|---|---|
| Age, years; mean (SD), min-max | 102 | 81.1 (4.4) 75–96 | 81.1 (4.4), 75–93 | 81.2 (4.4), 75–96 | 0.92 |
| Female, n (%) | 102 | 62 (60.8%) | 31 (60.8%) | 31 (60.8%) | 1.00 |
| Race, n (%) | |||||
| White | 102 | 98 (96.1%) | 51 (100%) | 47 (92.2%) | 0.12 |
| Education, n (%) | |||||
| High school graduate or less | 102 | 24 (23.5%) | 10 (19.6%) | 14 (27.5%) | 0.48 |
| Some college | 102 | 20 (19.6%) | 11 (21.6%) | 9 (17.6%) | 0.80 |
| College graduate or advanced degree | 102 | 58 (56.9%) | 30 (58.8%) | 28 (54.9%) | 0.84 |
| Body mass index, mean (SD) | 102 | 26.8 (4.3) | 26.2 (3.8) | 27.4 (4.8) | 0.18 |
| Blood pressure, Systolic, mmHg; mean (SD) | 102 | 146.0 (16.3) | 145.2 (18.6) | 146.7 (13.7) | 0.63 |
| Blood pressure, Diastolic, mmHg; mean (SD) | 102 | 69.8 (11.9) | 70.7 (13.0) | 68.9 (10.7) | 0.44 |
| Pulse pressure, mmHg; mean (SD) | 102 | 76.2 (18.3) | 74.5 (19.6) | 77.8 (16.8) | 0.35 |
| Clinical Dementia Rating = 0; n (%) | 102 | 71 (69.6%) | 36 (70.6%) | 35 (68.6%) | 1.00 |
| Geriatric Depression Scale; mean (SD) | 102 | 1.5 (1.4) | 1.3 (1.3) | 1.6 (1.6) | 0.22 |
| Instrumental Activities Daily Living; mean (SD) | 102 | 0.1 (0.4) | 0.1 (0.2) | 0.1 (0.5) | 0.59 |
| Gait speed, seconds; mean (SD) | 99 | 16.0 (4.1) | 15.5 (3.8) | 16.4 (4.4) | 0.29 |
| APOE4 carrier, n (%) | 102 | 28 (27.5%) | 15 (29.4%) | 13 (25.5%) | 0.82 |
| Neuroimaging; mean (SD) | |||||
| MRI, cm3 | |||||
| Intracranial volume, Total | 101 | 1884.1 (165.9) | 1874.3 (151.3) | 1894.2 (180.6) | 0.55 |
| Brain volume, Total | 101 | 882.0 (80.1) | 875 (73.1) | 889.1 (86.8) | 0.38 |
| Ventricular volume, Total | 101 | 49.3 (21.6) | 47.7 (17.5) | 50.9 (25.2) | 0.46 |
| White Matter Hyperintensity volume, Total | 101 | 19.4 (16.1) | 18.9 (15.3) | 19.9 (17.1) | 0.76 |
| Subcortical deep WMH | 101 | 1.9 (1.6) | 2.1 (1.8) | 1.7 (1.2) | 0.16 |
| Periventricular WMH | 101 | 17.4 (16.0) | 16.7 (15.2) | 18.1 (16.9) | 0.66 |
| Hippocampal volume, Total | 101 | 7.5 (0.9) | 7.5 (0.9) | 7.5 (0.9) | 0.74 |
| Neuropsychological battery, mean (SD) | |||||
| Mini-Mental State Examination | 102 | 27.9 (1.7) | 28.2 (1.8) | 27.6 (1.7) | 0.10 |
| Montreal Cognitive Assessment | 102 | 24.4 (3.1) | 24.7 (3.0) | 24.0 (3.2) | 0.24 |
| WAIS-IV Coding Digit Symbol | 100 | 48.8 (12.4) | 51.4 (13.8) | 46.3 (10.5) | 0.04 |
| Trail Making Test A, seconds | 102 | 39.1 (12.9) | 37.6 (12.3) | 40.6 (13.4) | 0.24 |
| Trail Making Test B, seconds | 102 | 118.7 (63.1) | 115.7 (62.2) | 121.6 (64.6) | 0.64 |
| Craft Story immediate, verbatim | 102 | 18.4 (6.7) | 19.1 (7.4) | 17.7 (6.0) | 0.31 |
| Craft Story immediate, paraphrase | 102 | 13.9 (4.0) | 14.1 (4.3) | 13.6 (3.8) | 0.51 |
| Craft Story delayed, verbatim | 102 | 15.0 (6.3) | 15.5 (7.0) | 14.5 (5.5) | 0.42 |
| Craft Story delayed, paraphrase | 102 | 12.5 (4.2) | 12.9 (4.6) | 12.0 (3.7) | 0.30 |
| Category Fluency, Animals | 102 | 19.0 (4.9) | 19.2 (4.7) | 18.9 (5.3) | 0.77 |
| Category Fluency, Vegetables | 102 | 13.5 (4.2) | 13.6 (4.8) | 13.5 (3.5) | 0.94 |
| Multilingual naming test | 102 | 29.7 (2.2) | 29.8 (2.4) | 29.5 (2.0) | 0.59 |
| Biochemical and metabolic measures | |||||
| Plasma eicosapentaenoic acid (EPA), ug/mL | 101 | 22.43 (11.49) | 23.08 (11.87) | 21.78 (11.18) | 0.57 |
| Plasma docosahexaenoic acid (DHA), ug/mL | 101 | 63.20 (20.46) | 62.59 (18.80) | 63.82 (22.21) | 0.76 |
| Plasma EPA+DHA, ug/mL | 101 | 85.64 (29.21) | 85.67 (28.28) | 85.60 (30.41) | 0.99 |
| Plasma vitamin B12, pg/mL | 101 | 694.4 (480.9) | 743.5 (498.2) | 644.4 (462.3) | 0.30 |
| Complete blood count | |||||
| White cells, K/cu mm; mean (SD) | 102 | 6.5 (1.9) | 6.4 (2.1) | 6.5 (1.7) | 0.81 |
| Red cells, M/cu mm; mean (SD) | 102 | 4.4 (0.5) | 4.4 (0.5) | 4.5 (0.5) | 0.34 |
| Hemoglobin, g/dL; mean (SD) | 102 | 13.6 (1.4) | 13.5 (1.4) | 13.7 (1.4) | 0.54 |
| Hematocrit, %; mean (SD) | 102 | 41.1 (3.9) | 40.7 (3.9) | 41.4 (3.8) | 0.35 |
| Platelet count, K/cu mm; mean (SD) | 102 | 221.5 (54.7) | 223.7 (60.2) | 219.3 (49.1) | 0.68 |
| Complete metabolic panel, mean (SD) | |||||
| Sodium, mmol/L | 102 | 138.9 (2.6) | 138.6 (2.9) | 139.2 (2.3) | 0.22 |
| Potassium, mmol/L | 102 | 3.9 (0.3) | 3.9 (0.3) | 4.0 (0.3) | 0.38 |
| Chloride, mmol/L | 102 | 105.0 (3.0) | 104.7 (3.3) | 105.4 (2.7) | 0.23 |
| Carbon Dioxide, mmol/L | 102 | 27.5 (1.9) | 27.3 (1.8) | 27.7 (1.9) | 0.25 |
| Blood Urea Nitrogen, mg/dL | 102 | 18.0 (5.5) | 18.0 (5.7) | 17.9 (5.4) | 0.99 |
| Creatinine, male, mg/dL | 40 | 1.0 (0.2) | 1.0 (0.2) | 1.0 (0.2) | 0.40 |
| Creatinine, female, mg/dL | 62 | 0.8 (0.2) | 0.8 (0.2) | 0.8 (0.1) | 0.66 |
| Glucose, mg/dL | 102 | 98.3 (16.7) | 98.6 (15.7) | 98.1 (17.7) | 0.88 |
| Calcium, mg/dL | 102 | 9.1 (0.4) | 9.1 (0.3) | 9.1 (0.4) | 0.38 |
| Aspartate Aminotransferase Test, U/L | 102 | 23.6 (8.1) | 22.5 (5.9) | 24.8 (9.7) | 0.15 |
| Alanine Aminotransferase Test, U/L | 102 | 25.5 (8.7) | 24.1 (5.9) | 27.0 (10.7) | 0.09 |
| Alkaline Phosphatase, male, U/L | 40 | 74.5 (19.6) | 69.7 (17.4) | 79.4 (20.8) | 0.12 |
| Alkaline Phosphatase, female, U/L | 62 | 82.2 (20.6) | 80.9 (20.5) | 83.5 (21.0) | 0.63 |
| Total Bilirubin, mg/dL | 102 | 0.7 (0.3) | 0.6 (0.3) | 0.7 (0.3) | 0.74 |
| Total Protein, g/dL | 102 | 7.3 (0.4) | 7.4 (0.4) | 7.3 (0.4) | 0.66 |
| Albumin, g/dL | 102 | 3.8 (0.2) | 3.8 (0.2) | 3.8 (0.2) | 0.93 |
| International Normalized Ratio | 100 | 1.0 (0.1) | 1.0 (0.1) | 1.0 (0.1) | 0.28 |
| Thyroid Stimulating Hormone, mIU/L | 101 | 2.2 (1.6) | 1.8 (0.9) | 2.5 (2.0) | 0.03 |
| Uric acid, mmol/L | 96 | 0.33 (0.08) | 0.33 (0.09) | 0.33 (0.08) | 0.89 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowman, G.L.; Silbert, L.C.; Dodge, H.H.; Lahna, D.; Hagen, K.; Murchison, C.F.; Howieson, D.; Kaye, J.; Quinn, J.F.; Shinto, L. Randomized Trial of Marine n-3 Polyunsaturated Fatty Acids for the Prevention of Cerebral Small Vessel Disease and Inflammation in Aging (PUFA Trial): Rationale, Design and Baseline Results. Nutrients 2019, 11, 735. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040735
Bowman GL, Silbert LC, Dodge HH, Lahna D, Hagen K, Murchison CF, Howieson D, Kaye J, Quinn JF, Shinto L. Randomized Trial of Marine n-3 Polyunsaturated Fatty Acids for the Prevention of Cerebral Small Vessel Disease and Inflammation in Aging (PUFA Trial): Rationale, Design and Baseline Results. Nutrients. 2019; 11(4):735. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040735
Chicago/Turabian StyleBowman, Gene L., Lisa C. Silbert, Hiroko H. Dodge, David Lahna, Kirsten Hagen, Charles F. Murchison, Diane Howieson, Jeffrey Kaye, Joseph F. Quinn, and Lynne Shinto. 2019. "Randomized Trial of Marine n-3 Polyunsaturated Fatty Acids for the Prevention of Cerebral Small Vessel Disease and Inflammation in Aging (PUFA Trial): Rationale, Design and Baseline Results" Nutrients 11, no. 4: 735. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040735