A Critical Appraisal of National and International Clinical Practice Guidelines Reporting Nutritional Recommendations for Age-Related Macular Degeneration: Are Recommendations Evidence-Based?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Appraisal of Clinical Guidelines
2.5. Mapping Clinical Guideline Recommendations to Systematic Review Evidence
3. Results
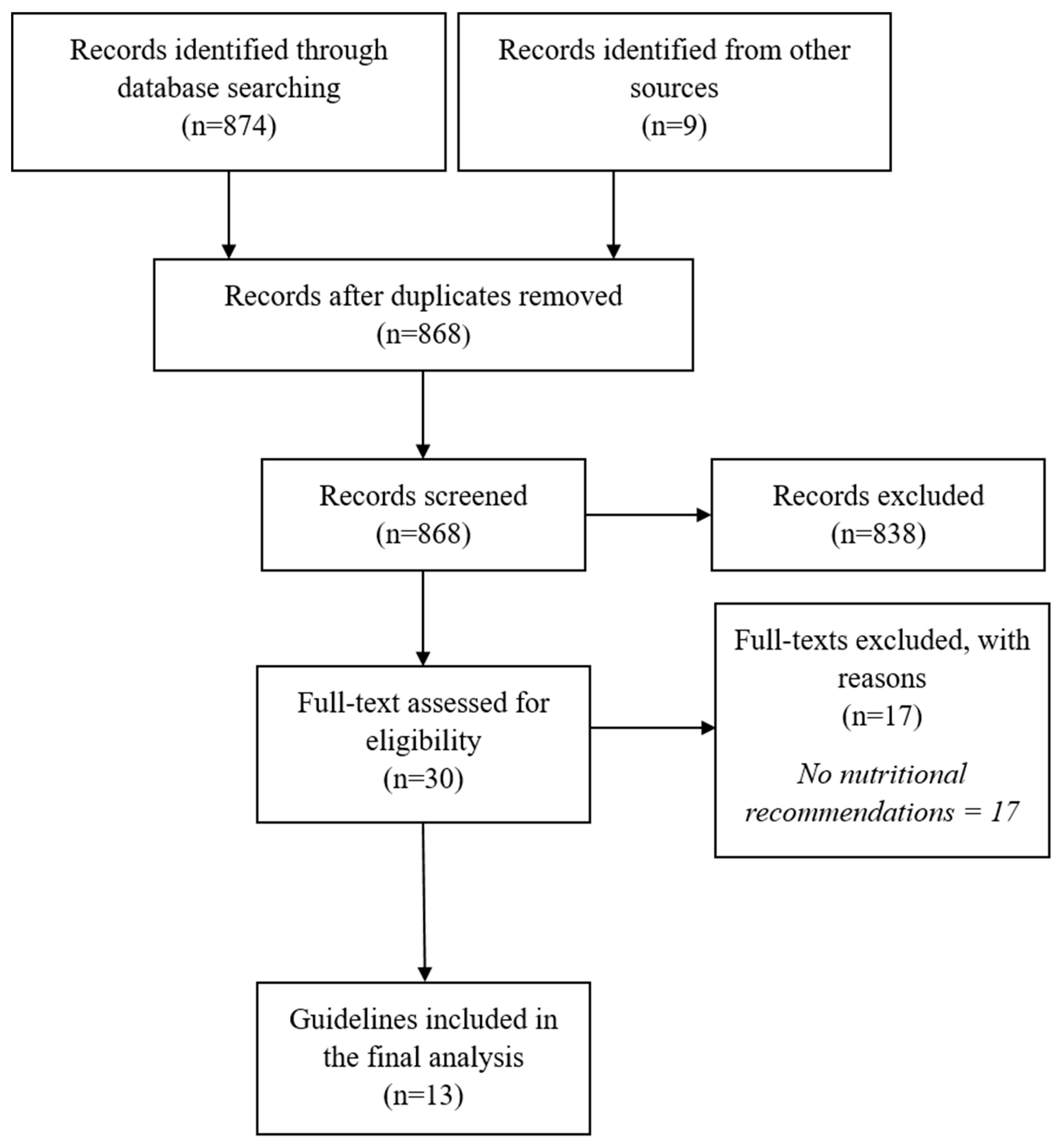
3.1. Search Results
3.2. Characteristics of Included Guidelines and Nutritional Recommendations
3.3. Clinical Guideline Quality Scores
3.4. Mapping Clinical Guideline Recommendations to Systematic Review Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Coleman, H.R.; Chan, C.C.; Ferris, F.L., 3rd; Chew, E.Y. Age-related macular degeneration. Lancet 2008, 372, 1835–1845. [Google Scholar] [CrossRef]
- Bhutto, I.; Lutty, G. Understanding age-related macular degeneration (AMD): Relationships between the photoreceptor/retinal pigment epithelium/Bruch’s membrane/choriocapillaris complex. Mol. Asp. Med. 2012, 33, 295–317. [Google Scholar] [CrossRef]
- Mitchell, J.; Bradley, C. Quality of life in age-related macular degeneration: A review of the literature. Health Qual. Life Outcomes 2006, 4, 97. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Swaminathan, G.; Kulothungan, V.; Raman, R.; Sharma, T.; Medscape. Prevalence and the risk factors for visual impairment in age-related macular degeneration. Eye 2017, 31, 846–855. [Google Scholar] [CrossRef]
- Downie, L.E.; Keller, P.R. Nutrition and age-related macular degeneration: Research evidence in practice. Optom. Vis. Sci. 2014, 91, 821–831. [Google Scholar] [CrossRef]
- Gorusupudi, A.; Nelson, K.; Bernstein, P.S. The Age-Related Eye Disease 2 Study: Micronutrients in the Treatment of Macular Degeneration. Adv. Nutr. 2017, 8, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch. Ophthalmol. 2001, 119, 1417–1436. [Google Scholar] [CrossRef]
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013, 309, 2005–2015. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. Clinical Practice Guidelines We Can Trust; Graham, R.M.M., Wolman, D.M., Greenfield, S., Steinberg, E., Eds.; The National Academies Press: Washington, DC, USA, 2011; p. 290. [Google Scholar]
- Wormald, R.; Evans, J. What Makes Systematic Reviews Systematic and Why are They the Highest Level of Evidence? Ophthalmic Epidemiol. 2018, 25, 27–30. [Google Scholar] [CrossRef]
- Lindsley, K.; Li, T.; Ssemanda, E.; Virgili, G.; Dickersin, K. Interventions for Age-Related Macular Degeneration: Are Practice Guidelines Based on Systematic Reviews? Ophthalmology 2016, 123, 884–897. [Google Scholar] [CrossRef]
- Downie, L.E.; Makrai, E.; Bonggotgetsakul, Y.; Dirito, L.J.; Kristo, K.; Pham, M.N.; You, M.; Verspoor, K.; Pianta, M.J. Appraising the Quality of Systematic Reviews for Age-Related Macular Degeneration Interventions: A Systematic Review. JAMA Ophthalmol. 2018, 136, 1051–1061. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.W.; Wong, T.Y.; Kreis, A.J.; Simpson, J.A.; Guymer, R.H. Dietary antioxidants and primary prevention of age related macular degeneration: Systematic review and meta-analysis. BMJ 2007, 335, 755. [Google Scholar] [CrossRef]
- Evans, J. Antioxidant supplements to prevent or slow down the progression of AMD: A systematic review and meta-analysis. Eye 2008, 22, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Lawrenson, J.G.; Evans, J.R. Omega 3 fatty acids for preventing or slowing the progression of age-related macular degeneration. Cochrane Database Syst. Rev. 2012, 11, CD010015. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.R.; Lawrenson, J.G. Antioxidant vitamin and mineral supplements for preventing age-related macular degeneration. Cochrane Database Syst. Rev. 2012, CD000253. [Google Scholar] [CrossRef]
- Hodge, W.G.; Barnes, D.; Schachter, H.M.; Pan, Y.I.; Lowcock, E.C.; Zhang, L.; Sampson, M.; Morrison, A.; Tran, K.; Miguelez, M.; et al. Evidence for the effect of omega-3 fatty acids on progression of age-related macular degeneration: A systematic review. Retina 2007, 27, 216–221. [Google Scholar] [CrossRef]
- Ma, L.; Liu, R.; Du, J.H.; Liu, T.; Wu, S.S.; Liu, X.H. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients 2016, 8, 426. [Google Scholar] [CrossRef] [PubMed]
- Sin, H.P.; Liu, D.T.; Lam, D.S. Lifestyle modification, nutritional and vitamins supplements for age-related macular degeneration. Acta Ophthalmol. 2013, 91, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Vishwanathan, R.; Chung, M.; Johnson, E.J. A systematic review on zinc for the prevention and treatment of age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3985–3998. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, C.; Zhang, Y.; Gong, Y.; Chen, X.; Zhang, M. Role of lutein supplementation in the management of age-related macular degeneration: Meta-analysis of randomized controlled trials. Ophthalmic Res. 2014, 52, 198–205. [Google Scholar] [CrossRef]
- Evans, J.R. Ginkgo biloba extract for age-related macular degeneration. Cochrane Database Syst. Rev. 2013, CD001775. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.R.; Lawrenson, J.G. Antioxidant vitamin and mineral supplements for slowing the progression of age-related macular degeneration. Cochrane Database Syst. Rev. 2012, 11, CD000254. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Clinical Knowledge Summaries. Macular Degeneration-Age-Related. Available online: https://cks.nice.org.uk/macular-degeneration-age-related (accessed on 25 March 2019).
- Anonymous. Age-Related Macular Degeneration. NICE Guideline [NG82]. Available online: https://www.nice.org.uk/guidance/ng82 (accessed on 25 March 2019).
- Anonymous; American Optical Association. Optometric Clinical Practice Guideline. Care of the Patient with Age-Related Macular Degeneration (CPG6). Available online: https://www.aoa.org/optometrists/tools-and-resources/clinical-care-publications/clinical-practice-guidelines (accessed on 25 March 2019).
- Anonymous. American Academy of Ophthalmology Preferred Practice Pattern. Age-Related Macular Degeneration. Available online: https://www.aao.org/preferred-practice-pattern/age-related-macular-degeneration-ppp-2015 (accessed on 25 March 2019).
- Anonymous. Practical Guidelines for the Treatment of AMD. Available online: https://www.reviewofoptometry.com/publications/ro1017-practical-guidelines-for-the-treatment-of-amd (accessed on 25 March 2019).
- Anonymous. Guidelines for the Collaborative Management of Persons with Age-Related Macular Degeneration by Health- and Eye-Care Professionals. Available online: https://opto.ca/sites/default/files/resources/documents/cjo_journal_online_ehco_guidelines_eng_v2.pdf (accessed on 25 March 2019).
- Cruess, A.F.; Berger, A.; Colleaux, K.; Greve, M.; Harvey, P.; Kertes, P.J.; Sheidow, T.; Tourville, E.; Williams, G.; Wong, D. Canadian expert consensus: Optimal treatment of neovascular age-related macular degeneration. Can. J. Ophthalmol. 2012, 47, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Optometry Australia. 2019 Clinical Practice Guide for the Diagnosis, Treatment and Management of Age-Related Macular Degeneration. Available online: http://www.optometry.org.au/media/1185775/amd_clinical_practice_guide_-_2019_final_designed_v5.pdf (accessed on 25 March 2019).
- Anonymous; National Health Committee. Age-Related Macular Degeneration. Available online: http://www.moh.govt.nz/notebook/nbbooks.nsf/0/1169E93BA82E0E3BCC257F7F0007E835/$file/150620_age-related_macular_degeneration_t2_updated-june15.pdf (accessed on 25 March 2019).
- Ruiz-Moreno, J.M.; Arias-Barquet, L.; Armada-Maresca, F.; Boixadera-Espax, A.; Garcia-Layana, A.; Gomez-Ulla-de-Irazazabal, F.; Mones-Carilla, J.; Pinero-Bustamante, A.; Suarez-de-Figueroa, M.; Sociedad Española de Retina yVítreo. Guidelines of clinical practice of the SERV: Treatment of exudative age-related macular degeneration (AMD). Arch. Soc. Esp. Oftalmol. 2009, 84, 333–344. [Google Scholar] [PubMed]
- Deutsche Ophthalmologische, G. Dietary supplements in age-related macular degeneration. Current observations of the German Ophthalmological Society, the German Retina Society and the Professional Association of German Ophthalmologists (as of October 2014). Klin. Mon. Augenheilkd. 2015, 232, 196–201. [Google Scholar] [CrossRef]
- Anonymous. Age-Related Macular Degeneration (AMD). Preferred Practice Patterns (PPP). Philippines. Available online: http://pao.org.ph/standard/Age%20Related%20Mac%20Degen.pdf (accessed on 25 March 2019).
- Anonymous; International Council of Ophthalmology/International Federation of Ophthalmological Societies (ICO). International Clinical Guidelines. Age-Related Macular Degeneration (Management Recommendations). Available online: http://www.icoph.org/downloads/ICOARMDMa.pdf (accessed on 25 March 2019).
- Downie, L.E.; Keller, P.R. The self-reported clinical practice behaviors of Australian optometrists as related to smoking, diet and nutritional supplementation. PLoS ONE 2015, 10, e0124533. [Google Scholar] [CrossRef]
- Lawrenson, J.G.; Evans, J.R. Advice about diet and smoking for people with or at risk of age-related macular degeneration: A cross-sectional survey of eye care professionals in the UK. BMC Public Health 2013, 13, 564. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Fretheim, A.; Oxman, A.D. Improving the use of research evidence in guideline development: 10. Integrating values and consumer involvement. Health Res. Policy Syst. 2006, 4, 22. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Rueda, J.D.; Gronseth, G.S.; Mullins, C.D. Framework for enhancing clinical practice guidelines through continuous patient engagement. Health Expect. 2017, 20, 3–10. [Google Scholar] [CrossRef]
- Wallace, J.; Nwosu, B.; Clarke, M. Barriers to the uptake of evidence from systematic reviews and meta-analyses: A systematic review of decision makers’ perceptions. BMJ Open 2012, 2. [Google Scholar] [CrossRef]
- Chapman, N.A.; Jacobs, R.J.; Braakhuis, A.J. Role of diet and food intake in age-related macular degeneration: A systematic review. Clin. Exp. Ophthalmol. 2019, 47, 106–127. [Google Scholar] [CrossRef] [PubMed]
- Merle, B.M.J.; Colijn, J.M.; Cougnard-Gregoire, A.; de Koning-Backus, A.P.M.; Delyfer, M.N.; Kiefte-de Jong, J.C.; Meester-Smoor, M.; Feart, C.; Verzijden, T.; Samieri, C.; et al. Mediterranean Diet and Incidence of Advanced Age-Related Macular Degeneration: The EYE-RISK Consortium. Ophthalmology 2019, 126, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Christen, W.G.; Schaumberg, D.A.; Glynn, R.J.; Buring, J.E. Dietary omega-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch. Ophthalmol. 2011, 129, 921–929. [Google Scholar] [CrossRef]
- Seddon, J.M.; George, S.; Rosner, B. Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: The US Twin Study of Age-Related Macular Degeneration. Arch. Ophthalmol. 2006, 124, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.W.; Kreis, A.J.; Wong, T.Y.; Simpson, J.A.; Guymer, R.H. Dietary omega-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration: A systematic review and meta-analysis. Arch. Ophthalmol. 2008, 126, 826–833. [Google Scholar] [CrossRef]
- Sangiovanni, J.P.; Agron, E.; Meleth, A.D.; Reed, G.F.; Sperduto, R.D.; Clemons, T.E.; Chew, E.Y.; Age-Related Eye Disease Study Research Group. {omega}-3 Long-chain polyunsaturated fatty acid intake and 12-y incidence of neovascular age-related macular degeneration and central geographic atrophy: AREDS report 30, a prospective cohort study from the Age-Related Eye Disease Study. Am. J. Clin. Nutr. 2009, 90, 1601–1607. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Hanna, S.E.; Makarski, J.; et al. Development of the AGREE II, part 2: Assessment of validity of items and tools to support application. CMAJ 2010, 182, E472–E478. [Google Scholar] [CrossRef]


{kind=link}
| Domain | Content |
|---|---|
| Scope and Purpose (3 items) | Concerned with the overall aim of the guideline, the specific health questions, and the target population |
| Stakeholder Involvement (3 items) | Focuses on the extent to which the guideline was developed by the appropriate stakeholders and represents the views of its intended users |
| Rigour of Development (8 items) | Relates to the process used to gather and synthesize the evidence, the methods to formulate the recommendations, and to update them |
| Clarity of Presentation (3 items) | Deals with the language, structure, and format of the guideline |
| Applicability (4 items) | Pertains to the likely barriers and facilitators to implementation, strategies to improve uptake, and resource implications of applying the guideline |
| Editorial Independence (2 items) | Concerned with the formulation of recommendations not being unduly biased with competing interests |
| Organisation | Reference | Year | Country | Target Audience |
|---|---|---|---|---|
| American Optical Association | [26] | 2004 | United States | Optometrists |
| International Council of Ophthalmology | [36] | 2007 | International | Optometrists |
| Spanish Retina and Vitreous Society (SERV) | [33] | 2009 | Spain | Ophthalmologists |
| Canadian Expert Consensus | [30] | 2012 | Canada | Ophthalmologists |
| German Ophthalmological Society (in German) | [34] | 2014 | Germany | Ophthalmologists |
| Eye Health Council of Ontario | [29] | 2015 | Canada | Health and eye care professionals |
| National Health Committee | [32] | 2015 | New Zealand | Healthcare professionals involved in the diagnosis and management of AMD |
| American Academy of Ophthalmology | [27] | 2015 | United States | Ophthalmologists |
| Vitreo-retina Society of the Philippines (VRSP) | [35] | 2016 | Philippines | Ophthalmologists |
| National Institute for Health and Care Excellence (NICE; Clinical Knowledge Summaries) | [24] | 2016 | United Kingdom | Primary care healthcare professionals |
| Clinical Advisory Committee [28] | [28] | 2017 | United States | Optometrists |
| NICE (NG82) | [25] | 2018 | United Kingdom | Healthcare professionals involved in the diagnosis and management of AMD |
| Optometry Australia | [31] | 2019 | Australia | Optometrists |
| Clinical Guideline | Dietary Advice | Use of Antioxidant or Mineral Supplements | Use of Omega-3 Fatty Acid Supplements | Contraindications or Side Effects of Supplements | Systematic Review Cited with Recommendation |
|---|---|---|---|---|---|
| American Optical Association 2004 | NR | ✓ 4 | NR | ✓ | None |
| International Council of Ophthalmology 2007 | NR | NR | NR | N/A | N/A |
| Spanish Retina and Vitreous Society 2009 | NR | NR | NR | N/A | N/A |
| Canadian Expert Consensus 2012 | NR | NR | NR | N/A | N/A |
| German Ophthalmological Society 2014 | ✓ 1 | ✓ 5 | NR | N/A | Yes |
| Eye Health Council of Ontario (Canada) 2015 | ✓ 2 | ✓ 5 | NR | N/A | None |
| National Health Committee (New Zealand) 2015 | NR | NR | NR | N/A | N/A |
| American Academy of Ophthalmology 2015 | NR | ✓ 5 | NR | N/A | None |
| Vitreo-Retinal Society of the Philippines 2016 | NR | ✓ 5 | NR | N/A | None |
| NICE Clinical Knowledge Summary (CKS) 2016 | NR | ✓ 5 | NR | N/A | Yes |
| Clinical Advisory Committee (United States) 2017 | NR | ✓ 6 | NR | NR | None |
| NICE Guideline (NG82) 2018 | NR | NR | NR | N/A | N/A |
| Optometry Australia 2019 | ✓ 3 | ✓ 7 | NR | NR | None |
| Clinical Guideline | Dietary Advice | Use of Antioxidant or Mineral Supplements | Use of Omega-3 Fatty Acid Supplements | Contraindications or Side Effects of Supplements | Systematic Review Cited with a Recommendation |
|---|---|---|---|---|---|
| American Optical Association 2004 | NR | ✓ 6 | NR | ✓ | None |
| International Council of Ophthalmology 2007 | NR | ✓ 7a | NR | NR | None |
| Spanish Retina and Vitreous Society 2009 | ✓ 1 | ✓ 7a | NR | ✓ | None |
| Canadian Expert Consensus 2012 | ✓ 2 | ✓ 7a | NR | ✓ | Yes |
| German Ophthalmological Society 2014 | NR | ✓ 7a | ✓ 10 | ✓ | Yes |
| Eye Health Council of Ontario (Canada) 2015 | ✓ 3 | ✓ 7a | ✓ 10 | ✓ | None |
| National Health Committee (New Zealand) 2015 | NR | ✓ 7a | NR | NR | None |
| American Academy of Ophthalmology 2015 | NR | ✓ 7a | NR | ✓ | None |
| Vitreo-Retina Society of the Philippines 2016 | NR | ✓ 7a | NR | ✓ | None |
| NICE Clinical Knowledge Summary (CKS) 2016 | ✓ 3 | ✓ 7a | NR | ✓ | Yes |
| Clinical Advisory Committee (United States) 2017 | ✓ 4 | ✓ 7a | ✓ 9 | NR | None |
| NICE Guideline (NG82) 2018 | NR | ✓ 8 | ✓ 10 | ✓ | Yes |
| Optometry Australia 2019 | ✓ 5 | ✓ 7b | NR | NR | None |
| Clinical Guideline | AGREE II Domains (%) | |||||
|---|---|---|---|---|---|---|
| Scope and Purpose | Stakeholder Involvement | Rigour of Development | Clarity of Presentation | Applicability | Editorial Independence | |
| American Optical Association 2004 | 52.8 | 30.6 | 9.2 | 30.6 | 10.9 | 87.5 |
| International Council of Ophthalmology 2007 | 58.3 | 30.6 | 10.2 | 58.3 | 2.2 | 0.0 |
| Spanish Retina and Vitreous Society 2009 | 63.9 | 41.7 | 21.4 | 36.1 | 13.0 | 0.0 |
| Canadian Expert Consensus 2012 | 75.0 | 47.2 | 36.7 | 75.0 | 28.3 | 20.8 |
| German Ophthalmological Society 2014 | 30.6 | 25.0 | 19.4 | 52.8 | 0.0 | 0.0 |
| Eye Health Council of Ontario (Canada) 2015 | 61.1 | 22.2 | 14.3 | 41.7 | 13.0 | 20.8 |
| National Health Committee (New Zealand) 2015 | 75.0 | 13.9 | 20.4 | 55.6 | 30.4 | 0.0 |
| American Academy of Ophthalmology 2015 | 83.3 | 63.9 | 72.4 | 94.4 | 17.4 | 75.0 |
| Vitreo-Retina Society of the Philippines 2016 | 83.3 | 44.4 | 56.1 | 88.9 | 13.0 | 45.8 |
| NICE Clinical Knowledge Summary (CKS) 2016 | 88.9 | 83.3 | 68.4 | 91.7 | 39.1 | 87.5 |
| Clinical Advisory Committee (United States) 2017 | 52.8 | 22.2 | 9.2 | 44.4 | 4.3 | 0.0 |
| NICE Guideline (NG82) 2018 | 94.4 | 88.9 | 95.9 | 100.0 | 97.8 | 100.0 |
| Optometry Australia 2019 | 83.3 | 41.7 | 19.4 | 75.0 | 19.6 | 0.0 |
| Median (range) | 75.0 (range 30.6 to 94.4%) | 41.7 (range 13.9 to 88.9%) | 20.4 (range 9.2 to 95.9) | 58.3 (range 30.6 to 100%) | 13.0 (range 2.2 to 97.8%) | 20.8 (range 0 to 100%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lawrenson, J.G.; Evans, J.R.; Downie, L.E. A Critical Appraisal of National and International Clinical Practice Guidelines Reporting Nutritional Recommendations for Age-Related Macular Degeneration: Are Recommendations Evidence-Based? Nutrients 2019, 11, 823. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040823
Lawrenson JG, Evans JR, Downie LE. A Critical Appraisal of National and International Clinical Practice Guidelines Reporting Nutritional Recommendations for Age-Related Macular Degeneration: Are Recommendations Evidence-Based? Nutrients. 2019; 11(4):823. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040823
Chicago/Turabian StyleLawrenson, John G., Jennifer R. Evans, and Laura E. Downie. 2019. "A Critical Appraisal of National and International Clinical Practice Guidelines Reporting Nutritional Recommendations for Age-Related Macular Degeneration: Are Recommendations Evidence-Based?" Nutrients 11, no. 4: 823. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11040823