Dietary Polyphenols—Important Non-Nutrients in the Prevention of Chronic Noncommunicable Diseases. A Systematic Review


Chair and Department of Food and Nutrition, Faculty of Pharmacy, Medical University of Lublin, 4a Chodźki Str., 20-093 Lublin, Poland
Nutrients 2019, 11(5), 1039; https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051039
Submission received: 23 April 2019
/
Revised: 25 April 2019
/
Accepted: 6 May 2019
/
Published: 9 May 2019
(This article belongs to the Special Issue Dietary Polyphenols and Cardiometabolic Diseases)
Abstract
:The improvement of the social and economic conditions of society has eliminated the threat of death from the majority of infectious diseases. However, the rapid progress of civilization has created new possibilities for the appearance of factors with adverse effects for the health of society. This has led to increased morbidity from certain diseases, the presence of which had not been observed several centuries ago. Chronic noncommunicable diseases (e.g., cancers, cardio-vascular disorders, diabetes, obesity, neurodegenerative diseases) result from an inappropriate relationship between people and their environment. The common characteristic for all chronic diseases is a “new” form of inflammation, very often called metaflammation, which is considered as a subclinical, permanent inflammation. As a result, metabolic cascade, including cellular oxidative stress, atherosclerotic process, and insulin resistance, occurs, which slowly generates significant deterioration in the organism. Polyphenols are the major group of non-nutrients, considering their diversity, food occurrence, and biological properties. The current review aims to present a wide spectrum of literature data, including the molecular mechanism of their activity and experimental model used, and summarize the recent findings on the multitude of physiological effects of dietary polyphenols towards the prevention of several chronic diseases. However, despite several studies, the estimation of their dietary intake is troublesome and inconclusive, which will be also discussed.
Highlights
During recent decades; a significant increase in chronic noncommunicable diseases has been observed; Polyphenols are the main group of biologically active non-nutrients present in food; Estimation of dietary intake of polyphenols is difficult; Beneficial effects of phenolics towards the prevention of lifestyle diseases are reviewed
1. Introduction
The rapid progress of humanity observed starting from the Industrial Revolution and especially after World War II has led to an increase in the length and quality of life. Rapid development of medical and pharmaceutical sciences has led to an improvement in diagnosis and the introduction of new drugs (e.g., vaccination or antibiotics). Together with the improvement of the social and economic conditions of society, this has eliminated the threat of death from the majority of infectious diseases [1,2]. However, the rapid progress of civilization has created new possibilities for the appearance of factors with adverse effects for the health of society. The Western diet, with its high saturated fat and sugar intake, physical inactivity, insufficient sleep, strong psychological stress, low sun exposure, environmental pollution, and smoking or alcohol abuse, are some of the most important factors which have been discussed during the last 20 years in numerous papers and reports, leading to the description of the many so-called “diseases of civilization” [1,3,4].
2. Chronic Noncommunicable Diseases
Lifestyle diseases are classified as diseases resulting from an inappropriate relationship between people and their environment and lifestyle [2]. They are often described as chronic noncommunicable diseases (NCDs) and are, in general, treated as the same group of diseases. The list of impairments of such a type is increasing. Recently, Egger and Dixon [5] classified chronic diseases with lifestyle or environmental determinants into ten categories:
- cardio- and cerebrovascular diseases
- cancers with lifestyle components
- endocrine/metabolic disorders
- gastrointestinal disorders
- kidney disease
- mental/central nervous system (CNS) health
- musculoskeletal disorders
- respiratory diseases
- reproductive disorders
- dermatological disorders
2.1. Historical Background
On the basis of anthropological and medical reports, several authors suggest that these diseases are not observed or are rare in hunter-gatherer or nonwesternized populations [6,7,8]. This hypothesis is supported by historical records of explorers and adventurers which support the evidence of the superior health of pre-agriculture traditional populations [6]. Deterioration of diet did not start in the last 50 or 100 years; rather, it started much earlier. The Agricultural Revolution started about 11,000 years ago in the Middle East and quickly spread around the globe [3,9,10]. “Industrial” food production significantly altered the human diet and lifestyle, which was associated with the introduction of cereal grains as staple foods, domesticated meats, nonhuman milk, legumes, and other cultivated plant foods and later a common use of sucrose and alcoholic drinks [3,9]. According to Carrera-Bastos et al. [1], the superior physical health and body composition of hunter-gatherers and other traditional populations minimally affected by modern diet and lifestyle were not primarily due to genetics, but to environmental factors. They also suggest that during the last several thousand years, no significant gene changes have occurred to protect humans from chronic diseases caused by modern habits. Based on the anatomical, biomechanical, and isotope analysis of the hominin skeletons, several typical diet and lifestyle characteristics of the hunter-gatherers and traditional populations may be observed; these are presented in Table 1.
The 20th century brought an improvement in sanitation, hygiene, and immunization and the development of antibiotics, which resulted in the overcoming of “germ diseases” [24]. In the 1970s and 1980s in the developed countries of North America, Europe, and the Asian-Pacific region, the process of the “epidemiological transition” started, when chronic diseases began to be more frequent compared to infectious. Currently, this can be observed in developing countries such as Brazil, China, Russia, or India [5,25]. According to Egger and Dixon, the progress of civilization tamed infectious diseases, but surprisingly instigated an unhealthy style of life, which resulted in the rapid outbreak of NCDs [5].
2.2. Current Findings on NCDs
The background of NCDs is rather complicated, in contrast to infectious diseases which are always connected with germs. The common characteristic for all chronic diseases is a “new” form of inflammation, which from the beginning of the 1990s has been called metaflammation [5]. This term is used to describe a form of low-grade, chronic, and systemic inflammation, originally associated with obesity. Recent findings have revealed that “metaflammation” is not limited to obesity, but also related to other lifestyle diseases and conditions, for example heart disease, type 2 diabetes, many forms of cancer, osteoporosis, and even central nervous system diseases (depression or dementia) [26,27,28,29]. Metaflammation is considered a part of a metabolic cascade, including cellular oxidative stress, atherosclerotic process, and insulin resistance. As a result, dysmetabolism, induced allostatic overload, and finally chronic impairment can be observed [30,31]. Factors which induce metaflammation have largely arisen since the industrial revolution and have been named “anthropogens” or man-made environmental inducers [32,33,34].
Anthropogens induce low, subclinical, but persistent immune-response to a nonlife-threating situation. This situation could become dysmetabolic if exposure starts to be prolonged [5]. Moreover, low-grade chronic inflammation is often associated with man-made environmental inducers; for example, chronic psychological stress, improper diet, environmental pollution, smoking, and drug and alcohol abuse [35,36,37,38,39]. Numerous studies have been performed indicating different factors regarding the progress of low-grade chronic inflammation and finally its contribution to NCDs. The most important are insufficient sleep (fewer than 6 h per 24-h day), chronic vitamin D deficiency, physical inactivity, and broadly understood nutritional changes [3,17,40,41,42]. Surprisingly, these are in contrast to the factors presented in Table 1, which were characteristic for hunter-gatherers and other traditional populations.
2.3. Nutritional Changes Associated with NCDs—Potential Role of Antioxidants
The important role of nutrition for the prevention of chronic diseases is already well known. Inadequate as well as overnutrition may lead to serious consequences [5,43]. Recent statistics have shown that improper nutrition accounts for up to two-thirds of the risk for type 2 diabetes, cardiovascular diseases (CVD) [44], and other chronic impairments [45]. The diets of industrialized societies are significantly changed compared to Paleolithic or even Ancient Egyptian or Medieval populations [1]. Chronic disease progress has been associated with important nutritional aberrations which have occurred during last few centuries, regarding specific nutrient intake [46], overall meal patterns, food processing, and general food product characteristics, including glycemic index and macro- and micronutrient density [1,47]. Numerous studies have indicated dietary risk factors associated with the increased risk of developing noncommunicable diseases:
During the last two decades, it has been proposed that oxidative stress, caused by reactive oxygen species (ROS), may be a key factor in the development of insulin resistance, diabetes, cardiovascular diseases, neurodegenerative disorders, and other NCDs [56,57,58]. Prolonged exposure of β-cells to oxidative agents (e.g., H2O2) results in their dysfunction and induced insulin resistance [59] and that the use of antioxidants improves insulin sensitivity, which has been proved in in vitro and animal model studies [60]. The role of ROS in the initiation, progression, and clinical consequences of cardiovascular diseases is already well known and has been described in several research papers proposing different mechanisms of antioxidant action in the prevention of CVD [61,62,63,64,65].
Although changes in lifestyle and diet (according to the characteristics presented above) are still considered crucial, many authors suggest that increased dietary intake of antioxidants is one of the most important factors in the prevention of NCDs, especially when those antioxidants are taken with a normal diet and not via dietary supplements [66,67,68,69]. The human diet contains many different antioxidants, including vitamins (C, E, β-carotene), trace elements (copper, iron, zinc, selenium), or plant metabolites (polyphenols, carotenoids) [70,71]. Although phytochemicals are often considered antinutrients or non-nutrients, during the last 15 years several findings have shed new light on their positive impact on the human organism, including their significant role in the prevention of chronic diseases [72,73]. Plant foods contain a wide spectrum of secondary metabolites among which polyphenols are one of the most abundant and nutritionally important phytochemicals [73]. There are over 8000 phenolic structures currently known and over 500 are present in plant foods and are considered dietary polyphenols. Polyphenols are synthetized from the combination of derivates formed from phenylalanine and acetic acid in two biochemical pathways—the shikimate and the acetate pathways. This is a very wide and complex group of phytochemicals, for which the common feature is the presence in their structure of at least one or more phenolic groups, which are responsible for the strong reducing properties of polyphenols. In nature, they occur as simple molecules, for example phenolic acids or flavonoids, or as very complicated polymerized macromolecules with molecular weights of greater than 30,000 Da, such as tannins. The diversity of polyphenols is increased, as they appear in the form of glycosides with one or two sugars, of which glucose is the most abundant molecule. Other sugar residues involve galactose, rhamnose, arabinose, xylose or glucuronic and galacturonic acids, and many others. Direct connections between sugar residues and aromatic carbon atoms (C–C binding) are also common.
3. Polyphenols—Estimation of Daily Dietary Intake Problems
Major classes of polyphenols involve simple phenols, phenolic acids, acetophenones, phenylacetic acids, coumarins, anthraquinones, xanthones, stilbenes, lignans, and flavonoids. The latter are the most complicated and the most widely distributed in plants. Flavonoids account for approximately two-thirds of dietary polyphenols and the remaining one-third are phenolic acids, being the second most important group of phenolics present in foods [74]. Flavonoids are an integral part of animal and human diets and plants are their only sources, as they cannot be synthesized by animals [75]. The most frequent class of flavonoids found in foods are flavonols, which are predominant in fruits in the form of different glycosides. In vegetables, the quercetin derivates are the most abundant flavonoid [76,77]. Exact estimation of daily dietary intake of flavonoids is difficult given their complicated distribution in plants, variety of classes, techniques used (analytical or calculating methods), and food habits. Moreover, several factors that influence their level in plants (germination, degree of ripeness, light), different flavonoid structures which still have not been identified and food processing cannot be ignored [66,78,79]. Another question is whether the study quantify glucoside forms, aglycones, or both. There are plenty of data on phenolic content in plants and assessments of dietary intake found in literature. However, these values mostly do not represent the total intake of all polyphenols, even not all flavonoids. In 1976, Kühnau estimated daily dietary intake of polyphenols at 1 g [78]. Later, those values were very often questioned as being almost impossible to attain from natural sources. Studies from the 1990s suggested that daily dietary intake is much lower, e.g., (values in mg/day):
However, those values mostly referred to only three flavonols and two flavones and therefore were underestimated. Later findings shed new light on polyphenolic intake, including flavonoids. A recent study performed by Pozzo and coworkers on 1658 Italian individuals, aged 45–64 years, revealed a mean intake of flavonoids at 320 mg/person/day, with a median of 251 mg/person/day. Food consumption data were based on the semiquantitative food-frequency questionnaire used in the EPIC (European Prospective Investigation into Cancer and Nutrition) and the flavonoid intake was calculated using the latest food composition tables published by the US Department of Agriculture (USDA) and extended by European data. The database contained information on the food content of seven major classes of flavonoids. Flavonoid intake was calculated by multiplying the specific flavonoid content in food servings (expressed as mg aglycone equivalent/100 g food) by the daily consumption of the selected food item (g/day). The study revealed that the main consumed classes of flavonoids were proanthocyanidins and flavan-3-ols with median intakes of 96.1 and 50.4, respectively. The major consumed substances were, among others, polymers of flavon-3-ols, simple and condensed catechins (theaflavins, thearubigins), hesperetin, myricetin, or quercetin. The major sources of flavonoids were fruits, red wine, vegetables, and tea [84].
Recent studies on polyphenols intake found in the literature are based on calculations using US or European databases, among which the Phenol-Explorer database is one of the most important and widely used. It contains information on the content of 502 polyphenol glycosides, esters, and aglycones in 452 foods and may be helpful in the estimation of daily dietary intake of phenolics [85]. However, values based on estimations using databases are inaccurate, as the content of flavonoids and other polyphenols may vary significantly according to place, harvest time or food processing. Therefore, these values are only approximate and may differ significantly from analytical data, which are hard to collect considering the multitude and structure diversity of dietary polyphenols.
A study performed in Poland on 648 students was based on analytical determinations of selected flavonoids and phenolic acids in reconstructed daily food rations using the HPLC method. Moreover, total phenolic content (TPC) was determined using the Folin–Ciocalteu method. The mean intake of phenolics over the 3-year study period was determined to be 245.8 and 172.7 mg/day in women and men, respectively. The major polyphenol, in both the food rations of women and men, was hesperidin, while quercetin was also consumed in significant amounts—32.6 mg/day among women and 35.8 mg/day among men. The study was limited to the intake of seven phenolic compounds; however, TPC values expressed as gallic acid equivalents were much higher and close to 1 g/day [66].
According to Pérez-Jiménez and coworkers and based on the Phenol-Explorer database, cloves and dried peppermint are the foodstuffs richest in polyphenols, with content of 15 and 12 g/100 g. Later, food products such as star anise, cocoa powder, Mexican oregano (dried), or celery seed were classified, with contents between 2 and 5 g/100 g [85,86,87]. However, the consumption of these products is so low that they cannot be considered important dietary sources of polyphenols. The Phenol-Explorer database suggests that products rich in phenolics, where the intake may be considered significant (amounts and frequency of consumption), contain between 1756 mg (black chokeberry) to 45 mg/100 g (broccoli) of polyphenols. Although black (102 mg/100 g) and green tea (89 mg/100 g) infusions were classified 52 and 54, respectively, according to the classification of the 100 foods with the highest polyphenol content [87], recently they have been considered the most important sources of dietary polyphenols. The multitude of methods used to evaluate dietary intake of polyphenols caused significant differences between particular results. Figure 1 gathers the most important methods used to estimate the intake of dietary phenolics.
4. Dietary Polyphenols—Natural Substances Beneficial in the Prevention and Treatment of Lifestyle Diseases
A wide spectrum of biological activity of polyphenols has previously been extensively described in numerous scientific papers, including in vitro and in vivo studies. We can see from Figure 2. These natural components of human diet are probably the most extensively described in the scientific literature. Some of their properties may be used in the prevention and treatment of lifestyle diseases. One of the targets of the present review was to gathered some of the interesting and recent findings on the biological properties of selected dietary polyphenols, including molecular mechanism of action, regarding their potential role in reducing the incidence of civilization diseases. Since scientific literature is filled with hundreds of studies focused on biological properties of polyphenols, only research on compounds which dietary intake is significant were considered and described.
4.1. Antioxidant Activities of Dietary Polyphenols
This is probably the most extensively and the most frequently described biological activity of phenolics, which because of their structure, may be related to almost all compounds from this group. Experimental studies revealed that the mechanism of action may include several different pathways: direct ROS scavenging; inhibition of enzymes or trace elements chelation, which are involved in free radicals generation (e.g., copper or iron); increase in endogenic antioxidant production (e.g., SOD (SuperOxide Dismutase), glutathione). Flavonoids are known for their properties to inhibit enzymes which are involved in ROS generation, like glutathione S-transferase, microsomal monooxygenase, mitochondrial succinoxidase or NADH oxidase. Protective role, against free radicals, for other antioxidants (e.g., vitamin C and E) was also proved [66,88,89,90,91,92,93]. In vitro experiments showed that quercetin, epicatechin, and rutin are described by strong antioxidant properties. Quercetin possess strong iron-chelating and iron-stabilizing properties. Epicatechin and rutin were proved to be strong ROS scavengers and inhibitors of lipid peroxidation. Moreover, it was shown that glycosidic forms of polyphenols are usually weaker antioxidants than the corresponding aglycones [90]. Green tea polyphenols were confirmed to significantly increase the antioxidant capacity of human blood serum. Clinical study performed on ten healthy Korean subjects (aged 23–25), which consume 150 mL of green tea infusion in the first week, 300 mL in the second, and 450 mL in the third, showed increased total capacity of serum and plasma. The highest changed was observed after drinking of 300 and 450 mL, whereas after ingestion of 150 mL, no significant differences were observed. Moreover, this study elucidated that the highest increase was observed 120 min after tea consumption [94].
Not only simple polyphenols derived from tea, but also the products of their condensation, synthesized during the production of fermented and semifermented teas, possess strong antioxidant properties. Theaflavins, which are one of the most important phenolic constituents present in black tea, were proved to be stronger antioxidants in comparison to EGCG ((-)-epigallocatechin-3-gallate), which is considered one of the most active antiradical molecules present in food. Randomized, double-blind, crossover study performed by Arent and co-investigators revealed that consumption of black tea, enriched in theaflavins, led to better recovery and decreased the oxidative stress in humans subjected to acute anaerobic interval training. It was also observed that theaflavins reduced muscle pain after training in comparison to control group [95]. Imran and coworkers studied the influence of theaflavins and thearubigins, which are a dominant fraction of polymeric polyphenols present in black tea, on antioxidant status and lipid peroxidation in rats. They have proved that theaflavins showed higher antioxidant activity compared to thearubigins. A diet rich in both TFs and TRs (thearubigins) showed significant reduction in lipid profile, glucose content, and renal function. Animals receiving TFs were characterized by lower values in the TBARS (thiobarbituric acid reactive substances) test, compared to thearubigins or a mixture of TFs and TRs (1:1). However, theaflavins+thearubigins diets caused the highest glucose, urea, and creatinine reduction and maximum level of insulin and antioxidant parameters compared to diets containing TFs or TRs alone [96]. Another clinical study showed beneficial effects of oolong tea drinking, which is considered the richest source of another condensed compounds of phenolic nature—theasinensins. Research performed on athletes showed that consumption of oolong tea for 30 days caused significant antioxidant effect observed as strong reduction of malondialdehyde at rest and after exercise, decreased levels of SOD at the rest. It was also observed that oolong tea drinking significantly reduced lipid peroxidation and normalized the cholesterol profiles [97]. Among all thesinensins isomers, theasinensin A was considered as the strongest antioxidant agent against lipid peroxidation [98].
4.2. Anti-Inflammatory Effect
Since low-grade, chronic inflammation is a key factor in the development and progression of lifestyle diseases beneficial effects of polyphenols towards inhibition and reduction of any form of inflammation may be crucial in prevention and treatment of this type of disorders. Several studies revealed positive role of tea polyphenols considering inhibition of different mechanisms of inflammation. EGCG was proved to reduce autoimmune response by affecting the differentiation of the dysregulated CD 4(+) T cells to potential autoimmune agents. Animals experiments proved beneficial effects of EGCG treatment towards the improvement of autoimmune diseases [99]. It was also shown that EGCG inhibits proliferation of autoreactive T cells, production of proinflammatory cytokines and Th1 and Th 17 subpopulations, and increases the amount of regulatory T cells populations in lymphoid tissues and the central nervous system. All these findings suggest that EGCG may have preventive and therapeutic potential regarding T-cell mediated autoimmune diseases [100]. Epigallocatechin-3-gallate was also shown to reduce inflammation in connective tissue. EGCG was injected intraperitoneally 3 times/week into mice with collagen-induced arthritis. Significant reduction in cytokines, phosphorylated-signal transducer and activator of transcription-3, 705 and 727 and oxidative stress proteins production was observed. Moreover, the inhibition of osteoclast and Th 17 production was proved associated with increased regulatory T cells production. As a result, significant reduction in arthritis symptoms has been observed [101]. Not only tea catechins, but also other dietary flavonoids were recently described to have immune-response modulation properties. The recruitment of neutrophils to the site of injury or damage is an early sign of inflammation. Significant reduction of NO (nitric oxide), MPO (myeloperoxidase), and TNF-α (inflammatory mediators) production in human peripheral blood neutrophils by rutin, quercetin, and vitexin in the concentration of 25 µM was observed. These result suggests that dietary flavonoids may have a potential role in treating patients with neutrophil-mediated inflammatory diseases [102,103]. Apigenin administrated orally significantly reduced the infiltration of the inflammatory cells in the experimental autoimmune myocardiatitis in mice. The production of proinfalammatory cytokines—Th1 cytokines, TNF-α, interferon-gamma (IFN-γ), and interleukin-2 (IL-2) was also limited [104].
4.3. Anticancer Activity
One of the diseases most frequently associated with improper changes in lifestyle, including dietary habits, are different forms of cancer. Among the biological properties of dietary polyphenols, the cancer-chemopreventive properties in various in vitro and animal models have been extensively reported. This activity may originate from their antioxidant and anti-inflammatory properties. Recently, one of the most frequently investigated phenolics towards potential cancer prevention and treatment are simple and condensed tea polyphenols. Zhang and coworkers revealed induction of apoptosis of hepatocellular carcinoma LM6 cells (HCCLM6), associated with the reduction of mitochondrial membrane potential and promotion of G0/G1 phase cell cycle arrest caused by EGCG. The induced apoptosis of HCCLM6 cells was connected with a significant decrease in Bcl-2 and NF-κB expression. No influence on noncancerous liver cells was proved (HL-7702) [105]. Anticancer activity of epigallocatechin-3-galltae was also proved in animal model. Chemopreventive effect of EGCG and TF (theaflavin) in the treatment of tongue and liver cancer induced by N-nitrosodiethylamine in mice was shown. The mechanism of action was associated with the modulation of cellular proliferation/apoptosis and prevalence of CD 44 positive regulation [106]. Significant chemopreventive activity of theaflavins towards prostate cancer was also proved. Two independent studies showed reduction of proliferation and apoptosis induction in human prostate carcinoma (LNaCP and PC-3 cells). Theaflavin caused tumor cell death by induction of p53 suppressor expression and inhibition of nuclear transcription factor NF-κβ and mitogen-activated MAPK-kinase, which are important carcinogenesis factors. The cell cycle blocking in the phase G2/M was also observed [107,108]. Theaflavins are considered as a promising chemopreventive agent in human prostate cancer as their relative bioavailability in prostate tissue was 70% higher in comparison to EGCG [109]. Other dietary flavonoids are also considered as strong, natural anticancer agents. Recently, numerous studies indicated interesting findings on anticancer properties of the most abundant polyphenolic aglycones in the human diet—quercetin, apigenin, and hesperidin. Recently, quercetin was shown to inhibit of the human retinoblastoma (RB Y79 cell line) growth. Inhibition of tumor progression and invasion in the dose dependent manner was proved. The strongest effect was revealed at the quercetin concentration of 100 µM. Additionally antiangiogenesis effect was also reported [110]. Another recent study performed by Hashemzaei and co-investigators showed significant anticancer activity in in vitro and in vivo models. Quercetin used at the concentrations of 10, 20, 40, 80, and 120 µM was found to induce apoptosis of cancer cells of nine different cancer cell lines, i.e., colon, prostate, breast, and ovarian carcinomas. These results were confirmed in animal model, as mice bearing colon and breast cancers exhibited a significant reduction of tumors in groups treated with quercetin [111]. Apigenin, a common dietary flavonoid, present in many fruits and vegetables was recently widely investigated for its anticancer properties. Animal studies showed significant reduction of proliferation, invasion, and migration and increased apoptosis of colonorectal, breast, prostate, melanoma, renal cell, and ovarian cancers [112,113,114,115,116,117,118]. Hesperidin, a flavonoid derived from citrus fruit, was reported to inhibit human hepatic cancer HepG2 cells growth through the activation of caspase-9, -8, and -3, downregulation of Bcl-xL protein, and upregulation of Bax, Bak, and tBid protein levels in a dose-dependent manner. It was interesting that the sensitivity of HepG2 cancer cells to hesperidin was much higher compared to naringin, neohesperidin, and naringenin [119]. Other in vitro experiments, performed on MCF-7 human breast, androgen-independent PC-3, and DU-145 prostate cancer cells, and androgen-dependent LNCa cancer cells, revealed significant antitumor effect of hesperidin. The mechanism of action was different to antimitosis and involved inhibition of the proliferation of MCF-7-GFP-Tubulin cells and both basal and testosterone-induced proliferation of LNCaP cells [120]. Hesperidin was also proved to inhibit ovarian cancer cell viability and increase cytotoxicity in a dose- and time-dependent manner. The mechanism of action involved induction of apoptosis through activation of protein expression of antigrowth arrest- and DNA damage-inducible gene 153, anti-CCAAT’enhancer-binding protein homologous protein, glucose-regulated protein 78, and cytochrome c. This mechanism may shed new light on a potential role of this dietary flavonoid in the prediction of ovarian carcinoma [121].
4.4. Cardiovascular Diseases Prevention
A population-based cohort study performed by Pozzo and coworkers over 12 years on 1658 individuals showed that higher dietary intake of flavonoids was associated with reduced risk of CVDs after a mean 12-year follow-up and a 40–50% lower risk of nonfatal CV events. No influence of different subclasses of flavonoids on CV diseases prevention was observed. The intake of flavan-3-ols, anthocyanidins, and flavanones were the most significantly inversely associated with all-cause mortality [84]. Although results from numerous studies and RCTs are inconclusive, a recent meta-analysis performed by Sarrias and coworkers (based on 117 articles published between 1997–2015) revealed significant effect of flavanols on blood lipids. Flavanols from tea, cocoa, and apples (catechins and dimeric procyanidins) were proved to significantly reduce total and LDL cholesterol and increase HDL fraction. No influence on TAGs level was observed [122].
During the last 10 years, several studies and clinical trials have confirmed that catechins have strong antihypertensive activity. The mechanism involves regulation of NADPH production and inhibition of RNA expression of Il-6 and MMP-9 in blood patients with hypertension [123,124,125,126,127,128]. Bogdanski and co-investigators in a double-blind, placebo-controlled trial on 56 obese, hypertensive subjects, revealed that green tea polyphenols are effective in reduction of both systolic and diastolic blood pressures. Additionally, increased intake of these flavonoids caused significant reduction of TNF-α, C-reactive protein levels, fasting serum glucose, insulin levels, and insulin resistance [123].
Rats treated for five weeks with (-)-epicatechin at 2 or 10 mg/kg per day were shown to be resistant to a systolic blood pressure increase caused by administration of deoxycorticosterone acetate (DOCA). Epicatechin was proved to improve the impaired endothelium-dependent relaxation response to acetylcholine and reduce plasma endothelin-1 and malondialdehyde levels [126]. Among other catechins, EGCG was especially responsible for the inhibition of calcium-activated chloride channels. Further, based on that mechanism, calcium dependent phosphorylation of inositol triphosphate, calmodulin antibodies, and calmodulin-dependent protein kinase II were improved, which resulted in strong antihypertensive effect [129,130]. Studies performed on spontaneously hypertensive rats revealed significant decrease of blood pressure after administration of EGCG (200 mg/kg/day). The effect was comparable to observed after treatment with 3 mg/kg/day of enalapril—a common hypotensive drug. Moreover, it was shown that EGCG increased production and release of nitric oxide from endothelium via a PI-3-kinase pathway. Obtained results suggested that EGCG may play beneficial role in the treatment of hypertension and metabolic syndrome [131]. EGCG was also proved to inhibit renin—a crucial enzyme in the treatment of hypertension. This in vitro study also revealed that the specific structure of EGCG—a galloyl moiety and ortho-trihydroxy phenyl structure—may be responsible for the inhibitory activity of EGCG towards renin [132].
Catechins can also play a beneficial role in the prevention of hypertension through the increased release of NO, which is endogenous relaxing factor, responsible, among others, for lowering blood pressure. EC was proved to increase the activity of endogenous NO synthetase, protect endothelial cells from strong stress, and stabilize EDRF (endothelium-derived relaxing factor) when blood vessels are damaged [128].
4.5. Anti-Obesity Effect/Weight-Reducing Properties
According to Huang and coworkers, until 2013 there were about 24 different clinical trials performed on obese participants, which have proved the weight-reducing properties of tea polyphenols [133]. Numerous studies performed in vitro and on animals have also confirmed beneficial effects of green tea infusions on weight reduction. The precise molecular mechanism is still discussed. However, the key findings involve reduction of food intake, deterioration of lipid emulsification and absorption, adipogenesis and lipid synthesis suppression, and increase of energy expenditure via thermogenesis. Acceleration of fat oxidation and fecal lipid excretion were also confirmed. As a result, total body mass, fat tissue content, and waist to hip ratio were reduced. Blood lipids levels were also improved [133,134,135,136]. Not only flavan-3-ols present in tea, but also other flavonoids present in commonly consume foods may have a positive effect on the reduction of the body weight. Supplementation with a mixture of quercetin and green tea extract for four weeks in mice fed a high fat diet for 12 weeks revealed significant changes in genes expression. Over 100 genes in adipose tissue were downregulated, including those involved in leukocyte extravasation and phagocytosis. Downregulation of cholesterol metabolism was also observed and cholesterol congeries in adipose and muscle tissue is frequently observed in obesity and sarcopenia. A mild improvement of glucose tolerance in animals fed with quercetin only was proved. This study confirmed other findings suggesting an important role of quercetin, which improved blood glucose tolerance and insulin sensitivity [137,138,139]. Quercetin was also shown to regulate hepatic gene expression related to lipid metabolism in high-fat diet (HFD)-induced obesity in mice. The supplementation with this dietary flavonoid caused significant reduction of liver and white adipose tissue weight as well as hepatic lipid accumulation. Moreover, the size of lipid droplets in the animal epididymal fat pads was also decreased [140].
Luteolin, was also found to increase insulin sensitivity and decrease low-grade chronic inflammation observed in the obesity through the enhanced uptake of glucose by adipocytes and reduction of proinflammatory chemokines blood levels. Moreover, luteolin treatment decreased mRNA levels of tumor necrosis factor α, IL-6, and MCP-1, while it increased the gene expression of adiponectin and leptin in 3T3-L1 adipocytes and primary mouse adipose cells. A potent transcriptional activation of PPARγ (peroxisome proliferator-associated receptor) target genes in animal adipose cells was also revealed [141].
4.6. Antidiabetic Activity
Diabetes is the only disease that in the twentieth first century was referred to as an epidemic by the United Nations. It is the most frequently observed chronic noncommunicable disease, which is a major public health problem worldwide. Over 9% of adults have diabetes, which corresponds to 415 million people. Since diabetes is a dominant cause of mortality, morbidity, disability, and increasing healthcare expenditures, this disease is one of the biggest medical challenges of the present time [142]. Several antioxidant, anti-inflammatory, and increasing the insulin sensitivity activities of dietary polyphenols were described above. However, in recent years, many different properties of phenolics towards the regulation of carbohydrates metabolism have been described in the scientific literature. Apigenin, a flavone commonly present in celery, red pepper, parsley, and lemon, was described to have beneficial effects on AMP-dependent regulation of lipid and glucose metabolism. Apigenin was found to be a 200-fold more potent AMPK (5’ adenosine monophosphate-activated protein kinase) activator compared to metformin, a well-known antidiabetes drug. Apigenin administrated intraperitoneally for seven days (4 mg/kg body weight/day) had a strong antihyperglycemic effect in mice with STZ (streptozocin)-induced diabetes. This effect was more marked in the oral glucose tolerance test. The protective effect of these compounds over liver and kidneys of STZ-diabetic models was also shown [143,144,145]. Another study showed that apigenin increased glucose uptake, thyroid hormones level, and insulin secretion in alloxan-induced diabetic mice [146]. Increased level of glucose led to intensified toxicity, which contributes to progressive pancreatic β-cell failure and the development of overt diabetes. Increased production of ROS is one of the major aspects of glucose toxicity. A study performed on HIT-T15 pancreatic β-cells subjected to oxidative stress caused by 2-deoxy-D-ribose (dRib) revealed the protective effect of apigenin against cell damage. The results revealed that this dietary flavonoid caused significant reduction of the intracellular ROS level, increased cell survival and mitochondrial membrane potential, and decreased cell apoptosis. Taken together, it was concluded that administration of apigenin attenuated all the pancreatic β-cell failures caused by dRib [147]. Naringin and naringenin (the aglycone form of naringin), the most abundant representatives of flavanones in foods, possess a wide spectrum of antidiabetic activity. In mice with type 2 diabetes, naringin and hesperidin, which were separately administrated, significantly influenced glycolysis and gluconeogenesis and thus improved hyperglycemia. The proposed mechanism involved the upregulation of hepatic and adipocyte PPARγ and GLUT 4, important for the regulation of glucose metabolism. Additionally, both flavonoids improved lipid metabolism by reducing free fatty acid and TAGs (Triglycerides) plasma levels, inhibition of hepatic (HMG-CoA) reductase activity, and increasing fecal cholesterol [145,148,149]. On the other hand, recent findings on rodents suggest that naringenin and quercetin attenuates glucose uptake in adipose tissue, thus deteriorating glucose metabolism. This was observed after oral administration of these two dietary flavonoids in the amount equal to a consumption of a one glass of grapefruit juice. Glucose tolerance impairment was probably due to inhibition of hypothalamic PI3K signaling, an enzyme which is crucial for the neuronal control of glucose homoeostasis in the organism. These inconclusive actions may be due to individuals’ differences in absorption and metabolism of these polyphenols [150]. Recently, several studies revealed that diet supplementation with hesperidin in db/db, C57BL6 mice resulted in the regulation of hepatic enzymes involved in glucose metabolism in liver, which finally improved hyperglycemia. The reported mechanism was due to the upregulation of hepatic glucokinase, PPARγ, and adipocyte GLUT4. Reduction of G6Pase (glucose-6-phosphatase) and increased expression of GK (glucokinase), which, when combined, decreased glucose export through glucose transporter membrane proteins was observed in rats with STZ-induced type 1 diabetes [148,151,152,153,154]. Quercetin and its glycosylated forms are another example of the flavonoids which are present in human diet in the highest amounts, for which many findings on their antidiabetic activity were recently described. Berry extract with high quercetin concentration was proved to induced AMPK signaling pathways in muscle tissue and oxygen utilization in mitochondria—an analogous mechanism to that of metformin [155]. Quercetin glycosides like hyperoside or isoquercetin also stimulated AMPK in muscle tissue and improved insulin resistance. High effectiveness of quercetin was also reported in the treatment of STZ-induced diabetes in mice. Significant enhancement of liver glucose uptake and reduction of liver glycogenolysis and gluconeogenesis together was proved. Moreover, depletion of GLUT4 and GK stimulated by hyperglycemia was also observed [156,157,158].
Rutin at the concentration of 100 mg/kg in the diet showed significant reduction in blood glucose levels and increased production of insulin in mice with induced diabetes. Moreover, reestablishment of glycogen content and activities of enzymes involved in carbohydrates metabolism was also proved in this study [159].
Several studies proved that supplementation of 0.04–0.045% quercetin in the diet significantly reduced serum glucose and insulin resistance, measured as HOMA-IR parameter, in obese rats and a mouse model. No influence on body weight or adipose tissue size was observed. It was also concluded that quercetin is more effective as an antidiabetic than as an anti-obesity agent [160,161].
Polyphenolic compounds from green, black, and oolong tea were shown to be strong noncompetitive inhibitors of α-glucosidase—the enzyme responsible for intestinal maltose, maltotriose, and α-dextrin hydrolysis, which increases blood glucose levels. Among the tested products, polyphenols derived from oolong tea were characterized by the strongest inhibitory potential [162]. The study performed by Johnston and coworkers on polarized Caco-2 intestinal cells revealed that catechins from green tea are effective inhibitors of glucose intestinal uptake through regulation of the SGLT-1 and GLUT 2 pathways. The authors concluded that such a mechanism may be beneficial in reducing sugar intestinal absorption and an important dietary tool in the management of diabetes [163].
4.7. The Activity of Dietary Polyphenols toward CNS Disorders
Neurodegenerative diseases are progressive disorders of the nervous system that are associated with abnormal functioning or destruction of neurons in the brain and/or spinal cord. These diseases are the result of many toxic processes, eventually leading to the death of nerve cells [164]. Factors that may induce neurodegeneration include: deficiency of endogenous antioxidants, inflammation, excitotoxicity of glutamate, expression of proapoptotic proteins, and increases in iron and nitric oxide, leading to oxidative stress [165,166]. Alzheimer’s and Parkinson’s diseases are considered the most common neurodegenerative disorders.
4.7.1. Parkinson’s Disease
PD (Parkinson’s disease) affects about 1% of the population over the age of 50. Symptoms are caused by degenerative changes of dopaminergic neurons, mainly in the substantia nigra pars compacta with the presence of Lewy bodies and Lewy neurites, which results in a decrease in dopamine concentration [167,168]. Other neuropathological changes observed in the disease include: activation of microglial cells and increase in α-synuclein concentration [169]. Despite the many hypotheses and speculations about PD etiology, oxidative stress seems to be a crucial factor in the development of the disease [170]. Although the estimation of daily dietary intake of polyphenols is complicated and their bioavailability and the chemical forms in which they directly act in cells are even harder to explain, recent studies have shown that phenolics can cross the blood–brain barrier and exert biological effects in CNS [171,172,173]. The precise protective mechanism of polyphenols toward the dopaminergic neurons is still unclear and a matter of discussion. Recent studies have confirmed that their major antioxidant mechanism of action is probably not the only one responsible for cellular protection [174]. Fraga suggests that changes in membrane and protein functioning, even at very low polyphenol concentrations, could significantly change molecular mechanisms and therefore possess important biological activity in vivo [175]. Interactions between polyphenols and proteins, even at concentrations lower than those required to act as an antioxidant, leading to inhibition of protein aggregation, play a key role in the prevention of PD. Several studies during the last decade have proved that polyphenols significantly inhibit the expression of α-synuclein—a key protein in the formation of oligomeric aggregates, which is one of the most important factors in the pathogenesis of PD [176,177].
Masuda et al. [178] tested 79 compounds belonging to 12 different chemical classes (including 39 polyphenols) for their potential to inhibit the deposition of α-synuclein into the filaments in vitro. A significant decrease in sarkosyl-insoluble α-synuclein and a corresponding increase in the level of sarkosyl-soluble protein was observed in the presence of exifone, gossypetin, myricetin, and purpurogallin. The most effective polyphenols for the inhibition of α-synuclein filament deposition were baicalein, delphinidin, EGCG, exifone, GC ((-)-gallocatechin), GCG ((-)-gallocatechin gallate), gossypetin, hinokiflavone, hypericin, procyanidin B1, procyanidin B2, rosmarinic acid, and theaflavine. These findings proved that the inhibitory potential of some dietary polyphenols against the formation of insoluble oligomers and reduction of their toxicity to nerve cells may be a crucial mechanism in the prevention of PD development.
In a similar study, Meng et al. [179] investigated the ability of 48 flavonoids belonging to different classes for their effectiveness to inhibit the fibrillation of α-synuclein in vitro. The investigation revealed that the majority of the tested polyphenols inhibit α-synuclein fibrillation and aggregation (e.g., luteolin, rutin, C, ECG (epicatechin-3-gallate)), with EGCG, myricetin, baicalein, eriodictyol, and quercetin being the strongest inhibitors. On the other hand, diosmetin, hesperetin, and hesperidin possessed no inhibitory activity.
Several studies have proved that EGCG can strongly reduce α-synuclein neurocytotoxicity by transforming large, harmful fibrils into smaller, nontoxic, amorphous protein aggregates [180,181,182].
In vitro studies by Lu et al. [183] performed on the rat liver cytosol demonstrated that EGCG is a strong inhibitor of the catechol-O-methyltransferase enzyme (COMT), which can significantly improve the bioavailability of L-Dopa—the most important drug in the therapy of PD.
The protective role of tea polyphenols against neurotoxins has been proved in vivo in mice with MPTP (N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)-induced Parkinsonism. This study demonstrated that green tea flavonoids, as well as isolated EGCG, strongly decrease striatal dopamine depletion and loss of neurons of the substantia nigra [184]. The neuroprotective role of EGCG was associated with its iron-chelation and antioxidant properties, which led to decreased accumulation of iron and α-synuclein in the substantia nigra pars compacta of the brain [185].
Another study on a mice model revealed that tea consumption decreases, by about 30–60%, the risk of PD. Oral administration of black tea infusions before or after 6-OHDA (a neurotoxin of dopaminergic system applied to rat neonates which develops persistent brain damage) has been reported to reduce the impairment of dopaminergic neurons and improve motor efficiency [186].
Since oxidative stress, accumulation of transition metals, and inflammation play key roles in neuronal damage, the strong antioxidant and metal chelating properties of polyphenols also seem to be crucial in the prevention of neurodegenerative disorders. However, other mechanisms are also significant, as presented above.
Although several in vitro or in vivo experiments have demonstrated the beneficial role of polyphenols against PD, there are still little data from epidemiological studies. One of the few such studies is research performed by Checkoway and co-investigators [187], which proved that consumption of at least two cups of tea per day significantly reduces the risk of PD development. In another study, Gao and coworkers [188] investigated the influence of flavonoid intake on the risk of PD. They concluded that there is a significant negative correlation between a diet rich in flavonoids and PD incidence; however, the protective role of other dietary substances of plant origin also cannot be precluded. They also determined the most important dietary sources of flavonoids in relation to PD, which were berries, red wine, orange/orange juice, and apples (in men), but surprisingly not tea. They also found significant associations between higher anthocyanin intake and PD risk. For other subclasses of flavonoids, such a correlation was not observed.
The pathogenesis of PD is still not clear. Therefore, the future discovery of new findings and mechanisms of action of flavonoids in terms of the prevention of this disease are probably only a matter of time. However, data on the flavonoids dosages necessary to prevent PD incidence and progression and results from clinical studies are currently scarce.
4.7.2. Alzheimer’s Disease
Alzheimer’s disease (AD) is the most common neurodegenerative disorder worldwide and the most frequent observed form of dementia [189]. As reported in 2015, the prevalence of this disease has exceeded 44 million people across the world and it is expected that this number will double by 2050 [190]. The abnormal extracellular accumulation of amyloid-β-peptide in amyloid plaques and hyperphosphorylation of tau proteins and their excessive aggregation in intracellular neurofibrillary tangles are considered to be the most important neuropathological features of AD [191]. Additionally, epidemiological and clinical data support other hypotheses of the disease development: the reduction of the choline acetyltransferase activity [192]; impairment of the brain mitochondria functioning [193]; metabolic changes connected with lifestyle diseases such as diabetes or obesity [194] or vascular problems leading to a deterioration in cerebral blood flow [195].
The positive role of flavonoid-rich products and diets toward the prevention of AD and improving cognitive functions has been extensively described throughout the last 20 years [196,197,198]. In general, their mechanism of action is connected with antioxidant activity and thus anti-aging properties. Protective effects of various polyphenols have been confirmed in several experiments regarding the use of single phenolics, as well as total extracts. Joseph et al. [199] revealed that mice fed for eight months with a diet containing blueberry extract (20 g/kg) rich in polyphenols showed a significant improvement in memory and cognitive functions. Polyphenols from the extract enhanced neuronal signaling via the influence on the extracellular signal-regulated kinase and decreased activity of N-Sase (neutral sphingomyelin-specific phospholipase C) in the hippocampus and striatum. The latter enzyme activity increases as a function of age; thus, its inhibition may have a nootropic effect. The authors concluded that a diet rich in antioxidant phytochemicals may overcome genetic predispositions to AD. However, they did not investigate which particular polyphenols were responsible for such activity.
Of all the dietary polyphenols, it seems that the strongest potential in the prevention of AD has been confirmed for EGCG. This main green tea polyphenol, via activation of PKC (protein kinase C), promotes the nonamyloidogenic α-secretase pathway of APP in neuronal cell cultures and thus reduces the formation of β-amyloid fibrils. These results are supported by in vivo studies—a two-week treatment of mice with EGCG revealed a significant decrease in APP production and an increased synthesis of sAPP (soluble form of APP) in the hippocampus [200,201].
Another clinical parameter associated with a higher prevalence of AD is homocysteine. Increased levels of this amino acid may be responsible for vascular impairment and further neurotoxic alterations [202]. Higher homocysteine levels are determined in the moderate phase of AD, rather than in initial stage and control groups. Recent findings suggest that consumption of beverages rich in polyphenols may reduce inflammation and vascular impairments associated with AD. Antioxidants decrease the levels of thiol groups (from homocysteine), which are involved in the autocatalytic oxidation process in plasma and increased production of ROS. As a result, lower amounts of free radicals and reduced cell damage are observed [203]. A population-based prospective study preformed on 1836 Japanese-Americans demonstrated that consumption of fruit and vegetable juices at least three times per week significantly delayed the onset of AD, especially among patients who are at high risk of developing the disease. In particular, polyphenols from grapes were emphasized as being active toward the reduction of the disease progression [203,204].
Moderate consumption of red wine (rich in stilbenes, ex. resveratrol) has been proved to reduce β-amyloid progression and thus attenuates cognitive impairment and the prevalence of AD [205,206].
Table 2 summarizes recent findings on the biological properties of dietary polyphenols, which may be crucial in the potential prevention of lifestyle diseases incidence.
5. Conclusions
Polyphenols are the most common non-nutrients present in the human diet. Considering the significant amounts of compounds consumed in this class and the multitude of their activities, it should be noted that they can play an important role in the prevention of numerous disorders, including civilization diseases. However, it should be remembered that despite many promising results obtained in in vitro or animal experiments regarding their beneficial effects towards the organism, there is still not enough convincing evidence from human studies, especially with large populations. More research of this type is needed to better understand the real value of dietary polyphenols in the context of their ability to prevent the progress of civilization diseases.
Funding
This research received no external funding.
List of Abbreviations
| AD | Alzheimer’s disease |
| AMPK | 5’ adenosine monophosphate-activated protein kinase |
| APP | amyloid precursor protein |
| b.w. | body weight |
| C | (+)-catechin |
| CNS | central nervous system |
| ECG | epicatechin-3-gallate |
| EDRF | endothelium-derived relaxing factor |
| EGC | epigallocatechin |
| EGCG | (-)-epigallocatechin-3-gallate |
| G6Pase | glucose-6-phosphatase |
| GC | (-)-gallocatechin |
| GCG | (-)-gallocatechin gallate |
| GK | glucokinase |
| GLUT 2 and 4 | glucose transporters type 2 and 4 |
| HMG-CoA | 3-hydroxy-3-methylglutaryl-coenzyme |
| IRS-1 | insulin receptor substrate 1 |
| MPO | myeloperoxidase |
| MPTP | N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine |
| NO | nitric oxide |
| N-Sase | neutral sphingomyelin-specific phospholipase C |
| 6-OHDA | 6-hydroxyydopamine |
| PD | Parkinson’s disease |
| PEPCK | Phosphoenolpyruvate carboxykinase |
| PI3K | phosphoinositide-3-kinase |
| PKC | protein kinase C |
| PPARγ | peroxisome proliferator-associated receptor |
| RCTs | randomized controlled trials |
| ROS | reactive oxygen species |
| sAPP | soluble form of APP |
| SGLT 1 | sodium-glucose co-transporter type 1 |
| SOD | SuperOxide Dismutase |
| STZ | streptozocin |
| TAGs | Triglycerides |
| TBARS | thiobarbituric acid reactive substances |
| TF | theaflavin |
| TFs | theaflavins |
| TRs | thearubigins |
References
- Carrera-Bastos, P.; Fontes-Villalba, M.; O’Keefe, J.H.; Lindeberg, S.; Cordain, L. The western diet and lifestyle and diseases of civilization. Res. Rep. Clin. Cardiol. 2011, 2, 15–35. [Google Scholar] [CrossRef]
- Betlejewski, S. Social diseases, civilization diseases or lifestyle diseases? Wiad. Lek. 2007, 60, 489–492. [Google Scholar]
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and evolution of the Western diet: Health implications for the 21st century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [CrossRef]
- Booth, F.W.; Lees, S.J. Fundamental questions about genes, inactivity, and chronic diseases. Physiol. Genom. 2007, 28, 146–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, G.; Dixon, J. Beyond obesity and lifestyle: A review of 21st century chronic diseases determinants. BioMed Res. Int. 2014, 2014, 731685. [Google Scholar] [CrossRef]
- Lindeberg, S. Food and Western Disease: Health and Nutrition from an Evolutionary Perspective; Wiley-Blackwell: Chichester, UK, 2010. [Google Scholar]
- Eaton, S.B.; Konner, M.; Shostak, M. Stone agers in the fast lane: Chronic degenerative diseases in evolutionary perspective. Am. J. Med. 1988, 84, 739–749. [Google Scholar] [CrossRef]
- Jönsson, T.; Olsson, S.; Ahrén, B.; Bøg-Hansen, T.C.; Dole, A.; Lindeberg, S. Agrarian diet and diseases of affluence: Do evolutionary novel dietary lectins cause leptin resistance? BMC Endocr. Disord. 2005, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L. Implications of Plio-Pleistocene hominin diets for modern humans. In Evolution of the Human Diet: The Known, the Unknown, and the Unknowable; Ungar, P., Ed.; Oxford University Press: New York, NY, USA, 2007; pp. 363–383. [Google Scholar]
- Cordain, L. Cereal grains: Humanity’s double-edged sword. World Rev. Nutr. Diet 1999, 84, 19–73. [Google Scholar]
- Chaplin, G.; Jablonski, N.G. Vitamin D and the evolution of human depigmentation. Am. J. Phys. Anthropol. 2009, 139, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R. What is the optimal vitamin D status for health? Prog. Biophys. Mol. Biol. 2006, 92, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Deutch, B.; Dyerberg, J.; Pedersen, H.S.; Aschlund, E.; Hansen, J.C. Traditional and modern Greenlandic food: Dietary composition, nutrients and contaminants. Sci. Total Environ. 2007, 384, 106–119. [Google Scholar] [CrossRef]
- Kuhnlein, H.V.; Receveur, O. Local cultural animal food contributes high levels of nutrients for Arctic Canadian indigenous adults and children. J. Nutr. 2007, 137, 1110–1114. [Google Scholar] [CrossRef]
- Wiley, T.S.; Formby, B. Lights Out: Sleep, Sugar and Survival; Pocket Books: New York, NY, USA, 2000. [Google Scholar]
- Rook, G.A. 99th Dahlem conference on infection, inflammation and chronic inflammatory disorders: Darwinian medicine and the ‘hygiene’ or ‘old friends’ hypothesis. Clin. Exp. Immunol. 2010, 160, 70–79. [Google Scholar] [CrossRef]
- Booth, F.W.; Chakravarthy, M.V.; Gordon, S.E.; Spangenburg, E.E. Waging war on physical inactivity: Using modern molecular ammunition against an ancient enemy. J. Appl. Physiol. 2002, 93, 3–30. [Google Scholar] [CrossRef] [PubMed]
- Pettee, K.K.; Ainsworth, B.E. The Building Healthy Lifestyles Conference: Modifying lifestyles to enhance physical activity, diet, and reduce cardiovascular disease. Am. J. Lifestyle Med. 2009, 3, 6–10. [Google Scholar] [CrossRef]
- Cordain, L.; Gotshall, R.W.; Eaton, S.B.; Eaton, S.B., 3rd. Physical activity, energy expenditure and fitness: An evolutionary perspective. Int. J. Sports Med. 1998, 19, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Eaton, S.B. The ancestral human diet: What was it and should it be a paradigm for contemporary nutrition? Proc. Nutr. Soc. 2006, 65, 1–6. [Google Scholar] [CrossRef]
- Fox, L.C.; Juan, J.; Albert, R.M. Phytolith analysis on dental calculus, enamel surface, and burial soil: Information about diet and paleoenviroment. Am. J. Phys. Anthropol. 1996, 101, 101–113. [Google Scholar] [CrossRef]
- Cordain, L.; Brand Miller, J.; Eaton, S.B.; Mann, N.; Holt, S.H.A.; Speth, J.D. Plant to animal subsistence ratios and macronutrient energy estimations in worldwide huntergatherer diets. Am. J. Clin. Nutr. 2000, 71, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, R.S.; Luxwolda, M.F.; Janneke Dijck-Brouwer, D.A.; Eaton, S.B.; Crawford, M.A.; Cordain, L.; Muskiet, F.A. Estimated macronutrient and fatty acid intakes from an East African Paleolithic diet. Br. J. Nutr. 2010, 104, 1666–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeown, T. The Origins of Human Disease; Basil Blackwell: New York, NY, USA, 1998. [Google Scholar]
- Sanders, J.W.; Fuhrer, G.S.; Johnson, M.D.; Riddle, M.S. The epidemiological transition: The current status of infectious diseases in the developed world versus the developing world. Sci. Prog. 2008, 91, 1–38. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Hotamisligil, G.S.; Shargill, N.S.; Spiegelman, B.M. Adipose expression of tumor necrosis factor-α: Direct role in obesity-linked insulin resistance. Science 1993, 259, 87–91. [Google Scholar] [CrossRef]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 2008, 454, 428–435. [Google Scholar] [CrossRef]
- Libby, P. Inflammatory mechanisms: The molecular basis of inflammation and disease. Nutr. Rev. 2007, 65, 140–146. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Ann. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef]
- Hanson, G.K. Inflammation, atherosclerosis and coronary artery disease. N. Engl. J. Med. 2005, 352, 1658–1695. [Google Scholar] [CrossRef]
- Egger, G.; Dixon, J. Inflammatory effects of nutritional stimuli: Further support for the need for a big picture approach to tackling obesity and chronic disease. Obes. Rev. 2010, 11, 137–149. [Google Scholar] [CrossRef]
- Egger, G.; Dixon, J. Non-nutrient causes of low-grade, systemic inflammation: Support for a “canary in the mineshaft” view of obesity in chronic disease. Obes. Rev. 2011, 12, 339–345. [Google Scholar] [CrossRef]
- Egger, G. In search of a “germ theory” equivalent for chronic Disease. Prev. Chronic Dis. 2012, 9, 1–7. [Google Scholar] [CrossRef]
- Black, P.H. The inflammatory response is an integral part of the stress response: Implications for atherosclerosis, insulin resistance, type II diabetes and metabolic syndrome X. Brain Behav. Immun. 2003, 17, 350–364. [Google Scholar] [CrossRef]
- Mills, N.L.; Donaldson, K.; Hadoke, P.W.; Boon, N.A.; MacNee, W.; Cassee, F.R.; Sandström, T.; Blomberg, A.; Newby, D.E. Adverse cardiovascular effects of air pollution. Nat. Clin. Pract. Cardiovasc. Med. 2009, 6, 36–44. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Panagiotakos, D.B. The causal relationship between passive smoking and inflammation on the development of cardiovascular disease: A review of the evidence. Inflamm. Allergy Drug Targets 2009, 8, 328–333. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Inflammatory mechanisms in the regulation of insulin resistance. Mol. Med. 2008, 14, 222–231. [Google Scholar] [CrossRef]
- Kolb, H.; Mandrup-Poulsen, T. The global diabetes epidemic as a consequence of lifestyle-induced low-grade inflammation. Diabetologia 2010, 53, 10–20. [Google Scholar] [CrossRef]
- Tasali, E.; Leproult, R.; Spiegel, K. Reduced sleep duration or quality: Relationships with insulin resistance and type 2 diabetes. Prog. Cardiovasc. Dis. 2009, 51, 381–391. [Google Scholar] [CrossRef]
- Krueger, P.M.; Friedman, E.M. Sleep duration in the United States: A cross-sectional population-based study. Am. J. Epidemiol. 2009, 169, 1052–1063. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Nicholas, L.; Roberts, D.; Pond, D. The role of the general practitioner and the dietitian in patient nutrition management. Asia Pac. J. Clin. Nutr. 2003, 12, 3–8. [Google Scholar]
- Australian Institute of Health and Welfare, Chronic Diseases. Available online: http://www.aihw.gov.au/chronic-diseases (accessed on 3 March 2018).
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–664. [Google Scholar] [CrossRef]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nothlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Food sources of energy and nutrients among adults in the US: NHANES 2003-2006. Nutrients 2012, 4, 2097–2120. [Google Scholar] [CrossRef]
- Cordain, L.; Eades, M.R.; Eades, M.D. Hyperinsulinemic diseases of civilization: More than just Syndrome X. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2003, 136, 95–112. [Google Scholar] [CrossRef]
- Barclay, A.W.; Petocz, P.; McMillan-Price, J.; Flood, V.M.; Prvan, T.; Mitchell, T.; Brand-Miller, J.C. Glycemic index, glycemic load, and chronic disease risk: A meta-analysis of observational studies. Am. J. Clin. Nutr. 2008, 87, 627–637. [Google Scholar] [CrossRef]
- Alas-Salvadó, J.; Farrés, X.; Luque, X.; Narejos, S.; Borrel, M.; Basora, J.; Anguera, A.; Torres, F.; Bullo, M.; Balanza, R. Effect of two doses of a mixture of soluble fibres on body weight and metabolic variables in overweight or obese patients: A randomised trial. Br. J. Nutr. 2008, 99, 1380–1387. [Google Scholar] [CrossRef]
- Tarini, J.; Wolever, T.M. The fermentable fibre inulin increases postprandial serum short-chain fatty acids and reduces free fatty acids and ghrelin in healthy subjects. Appl. Physiol. Nutr. Metab. 2010, 35, 9–16. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. Available online: http://www.cdc.gov/nchs/nhanes.htm (accessed on 7 April 2018).
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.; Ezzati, M. The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009, 6, e1000058. [Google Scholar] [CrossRef]
- Xiao, Y.; Zhang, Y.; Wang, M.; Li, X.; Xia, M.; Ling, W. Dietary protein and plasma total homocysteine, cysteine concentrations in coronary angiographic subjects. Nutr. J. 2013, 12, 144. [Google Scholar] [CrossRef]
- Miller, D.B.; O’Callaghan, J.P. Biomarkers of Parkinson’s disease: Present and future. Metabolism 2015, 64, 40–46. [Google Scholar] [CrossRef]
- Ceriello, A.; Motz, E. Is oxidative stress the pathogenic mechanism underlying insulin resistance, diabetes, and cardiovascular disease? The common soil hypothesis revisited. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 816–823. [Google Scholar] [CrossRef]
- De la Monte, S.M.; Neely, T.R.; Cannon, J. Oxidative stress and hypoxia, molecular abnormalities in central nervous system neurons. Cell. Mol. Life Sci. 2000, 57, 1471–1481. [Google Scholar] [CrossRef]
- Robertson, R.P.; Harmon, J.; Tran, P.O.; Tanaka, Y.; Takahashi, H. Glucose toxicity in-cells: Type 2 diabetes, good radicals gone bad, and the glutathione connection. Diabetes 2003, 52, 581–587. [Google Scholar] [CrossRef]
- Paolisso, G.; Giugliano, D. Oxidative stress and insulin action. Is there a relationship? Diabetologia 1996, 39, 357–363. [Google Scholar] [CrossRef]
- Kinkade, K.; Streeter, J.; Miller, F.J., Jr. Inhibition of NADPH oxidase by apocynin attenuates progression of atherosclerosis. Int. J. Mol. Sci. 2013, 14, 17017–17028. [Google Scholar] [CrossRef]
- Sugiyama, S.; Kugiyama, K.; Aikawa, M.; Nakamura, S.; Ogawa, H.; Libby, P. Hypochlorous acid, a macrophage product, induces endothelial apoptosis and tissue factor expression: Involvement of myeloperoxidase-mediated oxidant in plaque erosion and thrombogenesis. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1309–1314. [Google Scholar] [CrossRef]
- Csanyi, G.; Yao, M.; Rodriguez, A.I.; Al Ghouleh, I.; Sharifi-Sanjani, M.; Frazziano, G.; Huang, X.; Kelley, E.E.; Isenberg, J.S.; Pagano, P.J. Thrombospondin-1 regulates blood flow via CD47 receptor-mediated activation of NADPH oxidase 1. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2966–2973. [Google Scholar] [CrossRef]
- Touyz, R.M.; Briones, A.M. Reactive oxygen species and vascular biology: Implications in human hypertension. Hypertens. Res. 2011, 34, 5–14. [Google Scholar] [CrossRef]
- Heitzer, T.; Schlinzig, T.; Krohn, K.; Meinertz, T.; Münzel, T. Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation 2001, 104, 2673–2678. [Google Scholar] [CrossRef]
- Koch, W.; Baj, T.; Kukula-Koch, W.; Marzec, Z. Dietary intake of specific phenolic compounds and their effect on the antioxidant activity of daily food rations. Open Chem. 2015, 13, 869–876. [Google Scholar] [CrossRef]
- Huxley, R.R.; Neil, H.A. The relation between dietary flavonol intake and coronary heart disease mortality: A meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2003, 57, 904–908. [Google Scholar] [CrossRef]
- Jarząb, A.; Kukula-Koch, W. Recent advances in obesity: The role of turmeric tuber and its metabolites in the prophylaxis and therapeutical strategies. Curr. Med. Chem. 2017, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.J.; Myung, S.-K.; Chung, S.T.; Lee, Y.K.; Jeon, Y.-J.; Park, C.-H.; Seo, H.G.; Huh, B.Y. Effects of vitamin treatment or supplements with purported antioxidant properties on skin cancer prevention: A meta-analysis of randomized controlled trials. Dermatology 2011, 223, 36–44. [Google Scholar] [CrossRef]
- Puertollano, M.A.; Puertollano, E.; de Cienfuegos, G.Á.; de Pablo, M.A. Dietary antioxidants: Immunity and host defense. Curr. Top. Med. Chem. 2011, 11, 1752–1766. [Google Scholar] [CrossRef]
- Katta, R.; Brown, D.C. Diet and skin cancer: The potential role of dietary antioxidants in nonmelanoma skin cancer prevention. J. Skin Cancer 2015, 893149. [Google Scholar] [CrossRef] [PubMed]
- Lugasi, A.; Hóvári, J.; Sági, K.V.; Bíró, L. The role of antioxidant phytonutrients in the prevention of diseases. Acta Biol. Szeged. 2003, 47, 119–125. [Google Scholar]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Galvano, F.; Giovannucci, E.L. Dietary flavonoid and lignan intake and mortality in prospective cohort studies: Systematic review and dose-response meta-analysis. Am. J. Epidemiol. 2017, 1–13. [Google Scholar] [CrossRef]
- Robbins, R.J. Phenolic acids in foods: An overview of analytical methodology. J. Agric. Food Chem. 2003, 51, 2866–2887. [Google Scholar] [CrossRef]
- Koes, R.; Verweij, W.; Quattrocchio, F. Flavonoids: A colourful model for the regulation and evolution of biochemical pathways. Trends Plant Sci. 2005, 10, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Hertog, M.G.L.; Hollman, P.C.H.; Venema, D.P. Optimization of a quantitative HPLC determination of potentially anticarcinogenic flavonoids in vegetables and fruits. J. Agric. Food Chem. 1992, 40, 1591–1598. [Google Scholar] [CrossRef]
- Yao, L.H.; Jiang, Y.M.; Shi, J.; Tomás-Barberán, F.A.; Datta, N.; Singanusong, R.; Chen, S.S. Flavonoids in food and their health benefits. Plant Foods Hum. Nutr. 2004, 59, 113–122. [Google Scholar] [CrossRef]
- Kühnau, J. The flavonoids, a class of semi-essential food components: Their role in human nutrition. World Rev. Nutr. Diet. 1976, 24, 117–191. [Google Scholar] [CrossRef]
- Tomás-Barberán, F.A.; Clifford, M.N. Flavanones, chalcones and dihydrochalcones-nature, occurrence and dietary burden. J. Sci. Food Agric. 2000, 80, 1073–1080. [Google Scholar] [CrossRef]
- Justesen, U.; Knuthsen, P.; Leth, T. Determination of plant polyphenols in Danish foodstuffs by HPLC-UV and LC-MS detection. Cancer Lett. 1997, 114, 165–167. [Google Scholar] [CrossRef]
- Knekt, P.; Jarvinen, R.; Revnanen, A.; Moatela, J. Flavonoid intake and coronary mortality in Finland: A cohort study. BMJ 1996, 312, 478–481. [Google Scholar] [CrossRef]
- Hertog, M.G.L.; Kromhout, D.; Aravanis, C.; Blackburn, H.; Buzina, R.; Fidanza, F.; Giampaoli, S.; Jansen, A.; Menotti, A.; Nedeljkovic, S. Flavonoid intake and long term risk of coronary heart disease and cancer in the Seven Countries Study. Arch. Intern. Med. 1995, 155, 381–386. [Google Scholar] [CrossRef]
- Rimm, E.B.; Katan, M.B.; Ascherio, A.; Stampfer, M.J.; Willett, W.C. Relation between intake of flavonoids and risk for coronary heart disease in male health professionals. Ann. Intern. Med. 1996, 12, 384–389. [Google Scholar] [CrossRef]
- Pozzo, V.; Goitre, I.; Fadda, M.; Gambion, R.; De Francesco, A.; Soldati, L.; Gentile, L.; Magistroni, P.; Cassader, M.; Bo, S. Dietary flavonoid intake and cardiovascular risk: A population-based cohort study. J. Transl. Med. 2015, 13, 218. [Google Scholar] [CrossRef]
- Pérez-Jiménez, J.; Neveu, V.; Vos, F.; Scalbert, A. A systematic analysis of the content of 502 polyphenols in 452 foods and beverages—An application of the Phenol-Explorer database. J. Agric. Food Chem. 2010, 58, 4959–4969. [Google Scholar] [CrossRef] [PubMed]
- Neveu, V.; Pérez-Jiménez, J.; Vos, F.; Crespy, V.; Du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Jiménez, J.; Neveu, V.; Vos, F.; Scalbert, A. Identification of the 100 richest dietary sources of polyphenols: An application of the Phenol-Explorer database. Eur. J. Clin. Nutr. 2010, 64, 112–120. [Google Scholar] [CrossRef]
- Mishra, A.; Kumar, S.; Pandey, A.K. Scientific validation of the medicinal efficacy of Tinospora cordifolia. Sci. World. J. 2013, 292934. [Google Scholar] [CrossRef]
- Kukula-Koch, W.; Aligiannis, N.; Halabalaki, M.; Skaltsounis, A.L.; Glowniak, K.; Kalpoutzakis, E. Influence of extraction procedures on phenolic content and antioxidant activity of Cretan barberry herb. Food Chem. 2013, 138, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Mishra, A. Chemistry and biological activities of flavonoids: An overview. Sci. World. J. 2013, 162750. [Google Scholar] [CrossRef]
- Pinto, M.S. Tea: A new perspective on health benefits. Food Res. Int. 2013, 53, 558–567. [Google Scholar] [CrossRef]
- Bruno, R.S.; Bomser, J.A.; Ferruzzi, M.G. Antioxidant Capacity of Green Tea (Camellia sinensis). In Processing and Impact on Antioxidants in Beverages; Preedy, V.R., Ed.; Academic Press: Oxford, UK, 2014. [Google Scholar]
- Kukula-Koch, W.; Koch, W.; Angelis, A.; Halabalaki, M.; Aligiannis, N. Application of pH-zone refining hydrostatic countercurrent chromatography (hCCC) for the recovery of antioxidant phenolics and the isolation of alkaloids from Siberian barberry herb. Food Chem. 2016, 203, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Nah, J.; Chun, S.; Park, H.; Yang, S.E.; Min, W.K. In vivo antioxidant effect of green tea. Eur. J. Clin. Nutr. 2000, 54, 527–529. [Google Scholar] [CrossRef] [Green Version]
- Arent, S.M.; Senso, M.; Golem, D.L. The effects of theaflavin-enriched black tea extract on muscle soreness, oxidative stress, inflammation, and endocrine responses to acute anaerobic interval training: A randomized, double-blind, crossover study. J. Int. Soc. Sport. Nutr. 2010, 7, 11. [Google Scholar] [CrossRef]
- Imran, A.; Arshad, M.U.; Arshad, M.S.; Imran, M.; Saeed, F.; Sohaib, M. Lipid peroxidation diminishing perspective of isolated theaflavins and thearubigins from black tea in arginine induced renal malfunctional rats. Lipid. Health. Dis. 2018, 17, 157. [Google Scholar] [CrossRef]
- Tsai, P.H.; Kan, N.B.; Ho, S.C.; Liu, C.C.; Lin, C.C. Effects of oolong tea supplementationon lipid peroxidation of athletes at rest and post-exhaustive exercise. J. Food Sci. 2005, 70, 581–585. [Google Scholar] [CrossRef]
- Weerawatanakorn, M.; Hung, W.-L.; Pan, M.-H.; Li, S.; Li, D.; Wan, X.; Ho, C.-T. Chemistry and health beneficial effects of oolong tea and theasinensins. Food Sci. Hum. Well. 2015, 4, 133–146. [Google Scholar] [CrossRef] [Green Version]
- Pae, M.; Wu, D. Immunomodulating effect of epigallocatechin-3-gallate from green tea: Mechanisms and applications. Food Funct. 2013, 4, 1287–1303. [Google Scholar] [CrossRef]
- Wu, D. Green tea EGCG, T-cell function, and T-cell-mediated autoimmune encephalomyelitis. J. Investig. Med. 2016, 64, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Jung, Y.O.; Ryu, J.G.; Oh, H.J.; Son, H.J.; Lee, S.H.; Kwon, J.E.; Kim, E.K.; Park, M.K.; Park, S.H.; et al. Epigallocatechin-3-gallate ameliorates autoimmune arthritis by reciprocal regulation of T helper-17 regulatory T cells and inhibition of osteoclastogenesis by inhibiting STAT3 signaling. J. Leucoc. Biol. 2016, 100, 559–568. [Google Scholar] [CrossRef] [Green Version]
- Nikfarjam, B.A.; Adineh, M.; Hajiali, F.; Nassiri-Asl, M. Treatment with rutin—A therapeutic strategy for neutrophil-mediated inflammatory and autoimmune diseases: Anti-inflammatory effects of rutin on neutrophils. J. Pharmacopunct. 2017, 20, 52–56. [Google Scholar] [CrossRef]
- Nikfarjam, B.A.; Hajiali, F.; Adineh, M.; Nassiri-Asl, M. Anti-inflammatory Effects of Quercetin and Vitexin on Activated Human Peripheral Blood Neutrophils. J. Pharmacopunct. 2017, 20, 127–131. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, X.; Sun, C.; Yang, J.; Wang, L.; Liu, J.; Gong, L.; Jing, Y. Apigenin attenuates experimental autoimmune myocarditis by modulating Th1/Th2 cytokine balance in mice. Inflammation 2016, 39, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Duan, W.; Owusu, L.; Wu, D.; Xin, Y. Epigallocatechin-3-gallate induces the apoptosis of hepatocellular carcinoma LM6 cells but not non-cancerous liver cells. Int. J. Mol. Med. 2015, 35, 117–124. [Google Scholar] [CrossRef]
- Sur, S.; Pal, D.; Roy, R.; Barua, A.; Roy, A.; Saha, P.; Panda, C.K. Tea polyphenols EGCG and TF restrict tongue and liver carcinogenesis simultaneously induced by N-nitrosodiethylamine in mice. Toxicol. Appl. Pharmacol. 2016, 300, 34–46. [Google Scholar] [CrossRef]
- Kalra, N.; Seth, K.; Prasad, S.; Singh, M.; Pant, A.B.; Shukla, Y. Theaflavins induced apoptosis of LNCaP cells is mediated through induction of p53, down-regulation of NF-kappa B and mitogen-activated protein kinases pathways. Life Sci. 2007, 80, 2137–2146. [Google Scholar] [CrossRef]
- Prasad, S.; Kaur, J.; Roy, P.; Kalra, N.; Shukla, Y. Theaflavins induce G2/M arrest by modulating expression of p21waf1/cip1, cdc25C and cyclin B in human prostate carcinoma PC-3 cells. Life Sci. 2007, 81, 1323–1331. [Google Scholar] [CrossRef]
- He, H.-F. Research progress on theaflavins: Efficacy, formation, and preparation. Food Nutr. Res. 2017, 61, 1344521. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Zhao, X.; Xu, J.; Zhang, H. Quercetin inhibits angiogenesis-mediated human retinoblastoma growth by targeting vascular endothelial growth factor receptor. Oncol. Lett. 2017, 14, 3343–3348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemzaei, M.; Far, A.D.; Yari, A.; Heravi, R.E.; Tabrizian, K.; Taghdisi, S.M.; Sadegh, S.E.; Tsarouhas, K.; Kouretas, D.; Tzanakakis, G.; et al. Anticancer and apoptosis-inducing effects of quercetin in vitro and in vivo. Oncol. Rep. 2017, 38, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Dai, J.; Van Wie, P.G.; Fai, L.Y.; Kim, D.; Wang, L.; Poyil, P.; Luo, J.; Zhang, Z. Downregulation of NEDD9 by apigenin suppresses migration, invasion, and metastasis of colorectal cancer cells. Toxicol. Appl. Pharmacol. 2016, 311, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Tseng, T.H.; Chien, M.H.; Lin, W.L.; Wen, Y.C.; Chow, J.M.; Chen, C.K.; Kuo, T.C.; Lee, W.J. Inhibition of MDA-MB-231 breast cancer cell proliferation and tumor growth by apigenin through induction of G2/M arrest and histone H3 acetylation-mediated p21WAF1/CIP1 expression. Environ. Toxicol. 2017, 32, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Fu, P.; Gupta, S. Apigenin induces apoptosis by targeting inhibitor of apoptosis proteins and Ku70-Bax interaction in prostate cancer. Apoptosis 2014, 19, 883–894. [Google Scholar] [CrossRef]
- Shukla, S.; Shankar, E.; Fu, P.; MacLennan, G.T.; Gupta, S. Suppression of NF-κB and NF-κB-Regulated gene expression by apigenin through IκBα and IKK pathway in TRAMP mice. PLoS ONE 2015, 10, e0138710. [Google Scholar] [CrossRef]
- Cao, H.H.; Chu, J.H.; Kwan, H.Y.; Su, T.; Yu, H.; Cheng, C.Y.; Fu, X.Q.; Guo, H.; Li, T.; Tse, A.K.; et al. Inhibition of the STAT3 signaling pathway contributes to apigenin-mediated anti-metastatic effect in melanoma. Sci. Rep. 2016, 6, 21731. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.W.; Meng, D.; Fang, J. Apigenin inhibited migration and invasion of human ovarian cancer A2780 cells through focal adhesion kinase. Carcinogenesis 2008, 29, 2369–2376. [Google Scholar] [CrossRef] [Green Version]
- Meng, S.; Zhu, Y.; Li, J.F.; Wang, X.; Liang, Z.; Li, S.Q.; Xu, X.; Chen, H.; Liu, B.; Zheng, X.Y.; et al. Apigenin inhibits renal cell carcinoma cell proliferation. Oncotarget 2017, 8, 19834–19842. [Google Scholar] [CrossRef] [Green Version]
- Banjerdpongchai, R.; Wudtiwai, B.; Khaw-on, P.; Rachakhom, W.; Duangnil, N.; Kongtawelert, P. Hesperidin from Citrus seed induces human hepatocellular carcinoma HepG2 cell apoptosis via both mitochondrial and death receptor pathways. Tumour Biol. 2016, 37, 227–237. [Google Scholar] [CrossRef]
- Lee, C.J.; Wilson, L.; Jordan, M.A.; Nguyen, V.; Tang, J.; Smiyun, G. Hesperidin suppressed proliferations of both human breast cancer and androgen-dependent prostate cancer cells. Phytother. Res. 2010, 24, 15–19. [Google Scholar] [CrossRef]
- Zhao, J.; Li, Y.; Gao, J.; De, Y. Hesperidin inhibits ovarian cancer cell viability through endoplasmic reticulum stress signaling pathways. Oncol. Lett. 2017, 14, 5569–5574. [Google Scholar] [CrossRef] [Green Version]
- González-Sarrías, A.; Combet, E.; Pinto, P.; Mena, P.; Dall’Asta, M.; Garcia-Aloy, M.; Rodríguez-Mateos, A.; Gibney, E.R.; Dumont, J.; Massaro, M.; et al. A systematic review and meta-analysis of the effects of flavanol-containing tea, cocoa and apple products on body composition and blood lipids: Exploring the factors responsible for variability in their efficacy. Nutrients 2017, 9, 746. [Google Scholar] [CrossRef]
- Bogdanski, P.; Suliburska, J.; Szulinska, M.; Stepien, M.; Pupek-Musialik, D.; Jablecka, A. Green tea extract reduces blood pressure, inflammary biomarkers, and oxidative stress and improves, parameters associated with insulin resistance in obese, hypertensive patients. Nutr. Res. 2012, 32, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Ademiluyi, A.O.; Oboh, G.; Ogunsuyi, O.B.; Oloruntoba, F.M. A comparative study on antihypertensive and antioxidant properties of phenolic extracts from fruit and leaf of some guava (Psidium guajava L.) varieties. Comp. Clin. Pathol. 2016, 25, 363–374. [Google Scholar] [CrossRef]
- Tounekti, T.; Joubert, E.; Hernandez, I.; Munne-Bosch, S. Improving the polyphenol content of tea. Crit. Rev. Plant Sci. 2013, 32, 192–215. [Google Scholar] [CrossRef]
- Gómez-Guzmán, M.; Jiménez, R.; Sánchez, M.; Zarzuelo, M.J.; Galindo, P.; Quintela, A.M.; Lopez-Sepulveda, R.; Romero, M.; Tamargo, J.; Vargas, F.; et al. Epicatechin lowers blood pressure, restores endothelial function, and decreases oxidative stress and endothelin-1 and NADPH oxidase activity in DOCA-salt hypertension. Free Radic. Biol. Med. 2012, 52, 70–79. [Google Scholar] [CrossRef]
- Mahajan, N.; Dhawan, V.; Sharma, G.; Jain, S.; Kaul, D. Induction of inflammatory gene expression by THP-1 macrophages cultured in normocholesterolaemic hypertensive sera and modulatory effects of green tea polyphenols. J. Hum. Hypertens. 2008, 22, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.Q.; Hu, T.; Han, Y.; Huang, W.; Yuan, H.B.; Zhang, Y.T.; Du, Y.; Jiang, Y.W. Preventive Effects of Catechins on Cardiovascular Disease. Molecules 2016, 21, 1759. [Google Scholar] [CrossRef]
- Namkung, W.; Thiagarajah, J.R.; Phuan, P.W.; Verkman, A.S. Inhibition of Ca2+-activated Cl¯ channels by gallotannins as a possible molecular basis for health benefits of red wine and green tea. FASEB J. 2010, 24, 4178–4186. [Google Scholar] [CrossRef]
- Ohno, S.; Yokoi, H.; Mori, K.; Kasahara, M.; Kuwahara, K.; Fujikura, J.; Naito, M.; Kuwabara, T.; Imamaki, H.; Ishii, A.; et al. Ablation of the N-type calcium channel ameliorates diabetic nephropathy with improved glycemic control and reduced blood pressure. Sci. Rep. 2016, 6, 27192. [Google Scholar] [CrossRef] [Green Version]
- Potenza, M.A.; Marasciulo, F.L.; Tarquinio, M.; Tiravanti, E.; Colantuono, G.; Federici, A.; Kim, J.A.; Quon, M.J.; Montagnani, M. EGCG, a green tea polyphenol, improves endothelial function and insulin sensitivity, reduces blood pressure, and protects against myocardial I/R injury in SHR. Am. J. Physiol. Endocrinol. Metab. 2007, 292, 1378–1387. [Google Scholar] [CrossRef]
- Li, F.; Takahashi, Y.; Yamaki, K. Inhibitory effect of catechin-related compounds on renin activity. Biomed. Res. 2013, 34, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Wang, Y.; Xie, Z.; Zhou, Y.; Zhang, Y.; Wan, X. The anti-obesity effects of green tea in human intervention and basic molecular studies. Eur. J. Clin. Nutr. 2014, 68, 1075–1087. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.S.; Lee, H.G.; Choi, Y.J.; Kim, T.G.; Cho, C.S. Proposed mechanisms of (-)-epigallocatechin-3-gallate for anti-obesity. Chem. Biol. Interact. 2007, 167, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Bose, M.; Lambert, J.D.; Ju, J.; Reuhl, K.R.; Shapses, S.A.; Yang, C.S. The major green tea polyphenol, (-)-epigallocatechin-3 gallate, inhibits obesity, metabolic syndrome, and fatty liver disease in high-fat-fed mice. J. Nutr. 2008, 138, 1677–1683. [Google Scholar] [CrossRef] [PubMed]
- Nagao, T.; Hase, T.; Tokimitsu, I. A green tea extract high in catechins reduces body fat and cardiovascular risks in humans. Obesity 2007, 15, 1473–1483. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Parashar, A.; Sharma, A.; Singh, T.R.; Udayabanu, M. Quercetin ameliorates chronic unpredicted stress-mediated memory dysfunction in male Swiss albino mice by attenuating insulin resistance and elevating hippocampal GLUT4 levels independent of insulin receptor expression. Horm Behav. 2017, 89, 13–22. [Google Scholar] [CrossRef]
- Cialdella-Kam, L.; Ghosh, S.; Meaney, M.P.; Knab, A.M.; Shanely, R.A.; Nieman, D.C. Quercetin and green tea extract supplementation downregulated genes related to tissue inflammatory responses to a 12-week high fat-diet in mice. Nutrients 2017, 9, 773. [Google Scholar] [CrossRef]
- Henagan, T.M.; Lenard, N.R.; Gettys, T.W.; Stewart, L.K. Dietary quercetin supplementation in mice increases skeletal muscle PGC1alpha expression, improves mitochondrial function and attenuates insulin resistance in a time-specific manner. PLoS ONE 2014, 9, e89365. [Google Scholar] [CrossRef]
- Jung, C.H.; Cho, I.; Ahn, J.; Jeon, T.-I.; Ha, T.-Y. Quercetin reduces high-fat diet-induced fat accumulation in the liver by regulating lipid metabolism genes. Phytother. Res. 2013, 27, 139–143. [Google Scholar] [CrossRef]
- Ding, L.; Jin, D.; Chen, X. Luteolin enhances insulin sensitivity via activation of PPARγ transcriptional activity in adipocytes. J. Nutr. Biochem. 2010, 21, 941–947. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Siegel, K.R.; Gujral, U.P.; Narayan, K.M. Type 2 diabetes: A 21st century epidemic. Best Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 331–343. [Google Scholar] [CrossRef]
- Rauter, A.P.; Martins, A.; Borges, C.; Mota-Filipe, H.; Pinto, R.; Sepodes, B.; Justino, J. Antihyperglycaemic and protective effects of flavonoids on streptozotocin-induced diabetic rats. Phytother. Res. 2010, 24, 133–138. [Google Scholar] [CrossRef]
- Zang, M.; Xu, S.; Maitland-Toolan, K.A.; Zuccollo, A.; Hou, X.; Jiang, B.; Wierzbicki, M.; Verbeuren, T.J.; Cohen, R.A. Polyphenols stimulate amp-activated protein kinase, lower lipids, and inhibit accelerated atherosclerosis in diabetic ldl receptor-deficient mice. Diabetes 2006, 55, 2180–2191. [Google Scholar] [CrossRef]
- Hossain, M.K.; Dayem, A.A.; Han, J.; Yin, Y.; Kim, K.; Saha, S.K.; Yang, G.-M.; Choi, H.Y.; Cho, S.-G. Molecular mechanism of the anti-obesity and anti-diabetic properties of flavonoids. Int. J. Mol. Sci. 2016, 17, 569. [Google Scholar] [CrossRef]
- Panda, S.; Kar, A. Apigenin (4′,5,7-trihydroxyflavone) regulates hyperglycaemia, thyroid dysfunction and lipid peroxidation in alloxan induced diabetic mice. J. Pharm. Pharmacol. 2007, 59, 1543–1548. [Google Scholar] [CrossRef]
- Suh, K.S.; Oh, S.; Woo, J.-T.; Kim, S.-W.; Kim, J.-W.; Kim, Y.S.; Chon, S. Apigenin attenuates 2-deoxy-d-ribose-induced oxidative cell damage in HIT-T15 pancreatic. β-cells. Biol. Pharm. Bull. 2012, 35, 121–126. [Google Scholar] [CrossRef]
- Jung, U.J.; Lee, M.K.; Park, Y.B.; Kang, M.A.; Choi, M.S. Effect of citrus flavonoids on lipid metabolism and glucose-regulating enzyme mRNA levels in type-2 diabetic mice. Int. J. Biochem. Cell Biol. 2006, 38, 1134–1145. [Google Scholar] [CrossRef]
- Pu, P.; Gao, D.-M.; Mohamed, S.; Chen, J.; Zhang, J.; Zhou, X.-Y.; Zhou, N.-J.; Xie, J.; Jiang, H. Naringin ameliorates metabolic syndrome by activating amp-activated protein kinase in mice fed a high-fat diet. Arch. Biochem. Biophys. 2012, 518, 61–70. [Google Scholar] [CrossRef]
- Koch, C.E.; Ganjam, G.K.; Steger, J.; Legler, K.; Stohr, S.; Schumacher, D.; Hoggard, N.; Heldmaier, G.; Tups, A. The dietary flavonoids naringenin and quercetin acutely impair glucose metabolism in rodents possibly via inhibition of hypothalamic insulin signalling. Br. J. Nutr. 2013, 109, 1040–1051. [Google Scholar] [CrossRef]
- Akiyama, S.; Katsumata, S.; Suzuki, K.; Ishimi, Y.; Wu, J.; Uehara, M. Dietary hesperidin exerts hypoglycemic and hypolipidemic effects in streptozotocin-induced marginal type 1 diabetic rats. J. Clin. Biochem. Nutr. 2010, 46, 87–92. [Google Scholar] [CrossRef]
- Jung, U.J.; Lee, M.-K.; Jeong, K.-S.; Choi, M.-S. The hypoglycemic effects of hesperidin and naringin are partly mediated by hepatic glucose-regulating enzymes in C57BL/KsJ-db/db mice. J. Nutr. 2004, 134, 2499–2503. [Google Scholar] [CrossRef]
- Jung, U.J.; Choi, M.-S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef]
- Agrawal, Y.O.; Sharma, P.K.; Shrivastava, B.; Ojha, S.; Upadhya, H.M.; Arya, D.S.; Goyal, S.N. Hesperidin produces cardioprotective activity via PPAR- pathway in ischemic heart disease model in diabetic rats. PLoS ONE 2014, 9, e111212. [Google Scholar] [CrossRef]
- Eid, H.M.; Martineau, L.C.; Saleem, A.; Muhammad, A.; Vallerand, D.; Benhaddou-Andaloussi, A.; Nistor, L.; Afshar, A.; Arnason, J.T.; Haddad, P.S. Stimulation of AMP-activated protein kinase and enhancement of basal glucose uptake in muscle cells by quercetin and quercetin glycosides, active principles of the antidiabetic medicinal plant vaccinium vitis-idaea. Mol. Nutr. Food Res. 2010, 54, 991–1003. [Google Scholar] [CrossRef]
- Alam, M.M.; Meerza, D.; Naseem, I. Protective effect of quercetin on hyperglycemia, oxidative stress and DNA damage in alloxan induced type 2 diabetic mice. Life Sci. 2014, 109, 8–14. [Google Scholar] [CrossRef]
- Kobori, M.; Masumoto, S.; Akimoto, Y.; Takahashi, Y. Dietary quercetin alleviates diabetic symptoms and reduces streptozotocin-induced disturbance of hepatic gene expression in mice. Mol. Nutr. Food Res. 2009, 53, 859–868. [Google Scholar] [CrossRef]
- Xu, M.; Hu, J.; Zhao, W.; Gao, X.; Jiang, C.; Liu, K.; Liu, B.; Huang, F. Quercetin differently regulates insulin-mediated glucose transporter 4 translocation under basal and inflammatory conditions in adipocytes. Mol. Nutr. Food Res. 2014, 58, 931–941. [Google Scholar] [CrossRef]
- Prince, P.; Kamalakkannan, N. Rutin improves glucose homeostasis in streptozotocin diabetic tissues by altering glycolytic and gluconeogenic enzymes. J. Biochem. Mol. Toxicol. 2006, 20, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.M.; Kang, M.J.; Choi, H.N.; Kim, J.H.; Kim, J.I. Quercetin ameliorates hyperglycemia and dyslipidemia and improves antioxidant status in type 2 diabetic db/db mice. Nutr. Res. Pract. 2012, 6, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Arias, N.; Macarulla, M.T.; Aguirre, L.; Martinez-Castano, M.G.; Portillo, M.P. Quercetin can reduce insulin resistance without decreasing adipose tissue and skeletal muscle fat accumulation. Genes Nutr. 2014, 9, 361. [Google Scholar] [CrossRef]
- Yang, X.; Kong, F. Evaluation of the in vitro α-glucosidase inhibitory activity of green tea polyphenols and different tea types. J. Sci. Food Agric. 2016, 96, 777–782. [Google Scholar] [CrossRef]
- Johnston, K.; Sharp, P.; Clifford, M.; Morgan, L. Dietary polyphenols decrease glucose uptake by human intestinal Caco-2 cells. FEBS Lett. 2005, 579, 1653–1657. [Google Scholar] [CrossRef] [Green Version]
- Mandel, S.; Grunblatt, E.; Riederer, P.; Gerlach, M.; Levites, Y.; Youdim, M.B.H. Neuroprotective strategies in Parkinson’s disease: An update on progress. CNS Drugs 2003, 17, 729–762. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.; Gerlach, M.; Youdim, M.B.H.; Double, K.L.; Zecca, L.; Riederer, P.; Becker, G. Brain iron pathways and their relevance to Parkinson’s disease. J. Neurochem. 2001, 79, 225–236. [Google Scholar] [CrossRef]
- Dauer, W.; Przedborski, S. Parkinson’s disease: Mechanisms and models. Neuron 2003, 39, 889–909. [Google Scholar] [CrossRef]
- Cardoso, S.M.; Moreira, P.I.; Agostinho, P.; Pereira, C.; Oliveira, C.R. Neurodegenerative pathways in Parkinson’s disease: Therapeutic strategies. Curr. Drug Targets CNS Neurol. Disord. 2005, 4, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Ghebremedhin, E.; Rüb, U.; Bratzke, H.; Del Tredici, K. Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 2004, 318, 121–134. [Google Scholar] [CrossRef]
- McGeer, P.L.; Itagaki, S.; Akiyama, H.; McGeer, E.G. Rate of cell death in parkinsonism indicates active neuropathological process. Ann. Neurol. 1988, 24, 574–576. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; James-Kracke, M.; Sun, G.Y.; Sun, A.Y. Oxidative and inflammatory pathways in Parkinson’s disease. Neurochem. Res. 2009, 34, 55–65. [Google Scholar] [CrossRef]
- Hamaguchi, T.; Ono, K.; Murase, A.; Yamada, M. Phenolic compounds prevent Alzheimer’s pathology through different effects on the amyloid-beta aggregation pathway. Am. J. Pathol. 2009, 175, 2557–2565. [Google Scholar] [CrossRef]
- Smith, A.; Giunta, B.; Bickford, P.C.; Fountain, M.; Tan, J.; Shytle, R.D. Nanolipidic particles improve the bioavailability and alpha-secretase inducing ability of epigallocatechin-3-gallate (EGCG) for the treatment of Alzheimer’s disease. Int. J. Pharm. 2010, 389, 207–212. [Google Scholar] [CrossRef]
- Janle, M.E.; Lila, M.A.; Grannan, M.; Wood, L.; Higgins, A.; Yousef, G.G.; Rogers, R.B.; Kim, H.; Jackson, G.S.; Ho, L.; et al. Pharmacokinetics and tissue distribution of 14C-labeled grape polyphenols in the periphery and the central nervous system following oral administration. J. Med. Food. 2010, 13, 926–933. [Google Scholar] [CrossRef]
- Stevenson, D.E.; Hurst, R.D. Polyphenolic phytochemicals—Just antioxidants or much more? Cell Mol. Life Sci. 2007, 64, 2900–2916. [Google Scholar] [CrossRef]
- Fraga, C.G. Plant polyphenols: How to translate their in vitro antioxidant actions to in vivo conditions. Life 2007, 59, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Karpinar, D.P.; Balija, M.B.; Kügler, S.; Opazo, F.; Rezaei-Ghaleh, N.; Wender, N.; Kim, H.Y.; Taschenberger, G.; Falkenburger, B.H.; Heise, H.; et al. Pre-fibrillar alpha-synuclein variants with impaired beta-structure increase neurotoxicity in Parkinson’s disease models. EMBO J. 2009, 28, 3256–3268. [Google Scholar] [CrossRef]
- Marques, O.; Outeiro, T.F. Alpha-synuclein: From secretion to dysfunction and death. Cell Death Dis. 2012, 3, e350. [Google Scholar] [CrossRef]
- Masuda, M.; Suzuki, N.; Taniguchi, S.; Oikawa, T.; Nonaka, T.; Iwatsubo, T.; Hisanaga, S.; Goedert, M.; Hasegawa, M. Small molecule inhibitors of alpha-synuclein filament assembly. Biochemistry 2006, 45, 6085–6094. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Munishkina, L.A.; Fink, A.L.; Uversky, V.N. Effects of various flavonoids on the alpha-synuclein fibrillation process. Parkinsons Dis. 2010, 650794, 1–16. [Google Scholar] [CrossRef]
- Ehrnhoefer, D.E.; Bieschke, J.; Boeddrich, A.; Herbst, M.; Masino, L.; Lurz, R.; Engemann, S.; Pastore, A.; Wanker, E.E. EGCG redirects amyloidogenic polypeptides into unstructured, off-pathway oligomers. Nat. Struct. Mol. Biol. 2008, 15, 558–566. [Google Scholar] [CrossRef]
- Bae, S.Y.; Kim, S.; Hwang, H.; Kim, H.K.; Yoon, H.C.; Kim, J.H.; Lee, S.; Kim, T.D. Amyloid formation and disaggregation of alpha-synuclein and its tandem repeat (alpha-TR). Biochem. Biophys. Res. Commun. 2010, 400, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Bieschke, J.; Russ, J.; Friedrich, R.P.; Ehrnhoefer, D.E.; Wobst, H.; Neugebauer, K.; Wanker, E.E. EGCG remodels mature alpha-synuclein and amyloid-beta fibrils and reduces cellular toxicity. Proc. Natl. Acad. Sci. USA 2010, 107, 7710–7715. [Google Scholar] [CrossRef]
- Lu, H.; Meng, X.; Yang, C.S. Enzymology of methylation of tea catechins and inhibition of catechol-O-methyltransferase by (−)-epigallocatechin gallate. Drug Metab. Dispos. 2003, 31, 572–579. [Google Scholar] [CrossRef]
- Levites, Y.; Weinreb, O.; Maor, G.; Youdim, M.B.H.; Mandel, S. Green tea polyphenol (-)-epigallocatechin-3-gallate prevents N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced dopaminergic neurodegeneration. J. Neurochem. 2001, 78, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Mandel, S.; Maor, G.; Youdim, M.B.H. Iron and alpha synuclein in the substantia nigra of MPTP-treated mice: Effect of neuroprotective drugs R-apomorphine and green tea polyphenol epigallocatechin-3-gallate. J. Mol. Neurosci. 2004, 24, 401–416. [Google Scholar] [CrossRef]
- Chaturvedi, R.K.; Shukla, S.; Seth, K.; Chauhan, S.; Sinha, C.; Shukla, Y.; Agrawal, A.K. Neuroprotective and neurorescue effect of black tea extract in 6-hydroxydopamine-lesioned rat model of Parkinson’s disease. Neurobiol. Dis. 2006, 22, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Checkoway, H.; Powers, K.; Smith-Weller, T.; Franklin, G.M.; Longstreth, W.T., Jr.; Swanson, P.D. Parkinson’s disease risks associated with cigarette smoking, alcohol consumption, and caffeine intake. Am. J. Epidemiol. 2002, 155, 732–738. [Google Scholar] [CrossRef]
- Gao, X.; Cassidy, A.; Schwarzschild, M.A.; Rimm, E.B.; Ascherio, A. Habitual intake of dietary flavonoids and risk of Parkinson disease. Neurology 2012, 78, 1138–1145. [Google Scholar] [CrossRef] [Green Version]
- Baptista, F.I.; Henriques, A.G.; Silva, A.M.S.; Wiltfang, J.; da Cruz a Silva, O.A.B. Flavonoids as therapeutic compounds targeting key proteins involved in Alzehimer’s disease. ACS Chem. Neurosci. 2014, 5, 83–92. [Google Scholar] [CrossRef]
- Van Cauwenberghe, C.; Van Broeckhoven, C.; Sleegers, K. The genetic landscape of Alzheimer disease: Clinical implications and perspectives. Genet. Med. 2015, 18, 421–430. [Google Scholar] [CrossRef]
- Mendiola-Precoma, J.; Berumen, L.C.; Padilla, K.; Garcia-Alcocer, G. Therapies for prevention and treatment of Alzheimer’s disease. Biomed. Res. Int. 2016, 2589276. [Google Scholar] [CrossRef]
- Contestabile, A. The history of the cholinergic hypothesis. Behav. Brain Res. 2011, 221, 334–340. [Google Scholar] [CrossRef]
- Cervellati, C.; Wood, P.L.; Romani, A.; Valacchi, G.; Squerzanti, M.; Sanz, J.M.; Ortolani, B.; Zuliani, G. Oxidative challenge in Alzheimer’s disease: State of knowledge and future needs. J. Investig. Med. 2016, 64, 21–32. [Google Scholar] [CrossRef]
- Folch, J.; Patraca, I.; Martínez, N.; Pedrós, I.; Petrov, D.; Ettcheto, M.; Abad, S.; Marin, M.; Beas-Zarate, C.; Camins, A. The role of leptin in the sporadic form of Alzheimer’s disease. Interactions with the adipokines amylin, ghrelin and the pituitary hormone prolactin. Life Sci. 2015, 140, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Talbot, K.; Wang, H.Y.; Kazi, H.; Han, L.Y.; Bakshi, K.P.; Stucky, A.; Fuino, R.L.; Kawaguchi, K.R.; Samoyedny, A.J.; Wilson, R.S.; et al. Demonstrated brain insulin resistance in Alzheimer’s disease patients is associated with IGF-1 resistance, IRS-1 dysregulation, and cognitive decline. J. Clin. Investig. 2012, 122, 1316–1338. [Google Scholar] [CrossRef] [Green Version]
- Commenges, D.; Scotet, V.; Renaud, S.; Jacqmin-Gadda, H.; Barberger-Gateau, P.; Dartigues, J.F. Intake of flavonoids and risk of dementia. J. Epidemiol. 2000, 16, 357–363. [Google Scholar] [CrossRef]
- Le Bars, P.L.; Kieser, M.; Itil, K.Z. A 26-week analysis of a double-blind, placebo-controlled trial of the ginkgo biloba extract EGb 761 in dementia. Dement. Geriatr. Cognit. Disord. 2000, 11, 230–237. [Google Scholar] [CrossRef]
- Youdim, K.A.; Joseph, J.A. A possible emerging role of phytochemicals in improving age-related neurological dysfunctions: A multiplicity of effects. Free Radic. Biol. Med. 2001, 30, 583–594. [Google Scholar] [CrossRef]
- Joseph, J.A.; Denisova, N.A.; Arendash, G.; Gordon, M.; Diamond, D.; Shukitt-Hale, B.; Morgan, D. Blueberry supplementation enhances signaling and prevents behavioral deficits in an Alzheimer disease model. Nat. Neurosci. 2003, 6, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Levites, Y.; Amit, T.; Mandel, S.; Youdim, M.B.H. Neuroprotection and neurorescue against amyloid beta toxicity and PKC-dependent release of non-amyloidogenic soluble precursor protein by green tea polyphenol (-)-epigallocatechin-3-gallate. FASEB J. 2003, 17, 952–954. [Google Scholar] [CrossRef]
- Ono, K.; Yoshiike, Y.; Takashima, A.; Hasegawa, K.; Naiki, H.; Yamada, M. Potent anti-amyloidogenic and fibril-destabilizing effects of polyphenols in vitro: Implications for the prevention and therapeutics of Alzheimer’s disease. J. Neurochem. 2003, 87, 172–181. [Google Scholar] [CrossRef]
- Morris, M.S. Homocysteine and Alzheimer’s disease. Lancet. Neurol. 2003, 7, 425–428. [Google Scholar] [CrossRef]
- Wojtunik-Kulesza, K.A.; Oniszczuk, A.; Oniszczuk, T.; Waksmundzka-Hajnos, M. The influence of common free radicals and antioxidants on development of Alzheimer’s Disease. Biomed. Pharmacother. 2016, 78, 39–45. [Google Scholar] [CrossRef]
- Dai, Q.; Borenstein, A.R.; Wu, Y.; Jackson, J.C.; Larson, E.B. Fruit and vegetable juices and Alzheimer’s disease: The Kame Project. Am. J. Med. 2006, 119, 751–759. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, Z.; Ho, L.; Seror, I.; Humala, N.; Percival, S. Moderate consumption of Cabernet Sauvignon attenuates β-amyloid neuropathology in a mouse model of Alzheimer’s disease. FASEB J. 2006, 20, 2313–2320. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Tang, M.-X.; Siddiqui, M.; Shea, S.; Mayeux, R. Alcohol intake and risk of dementia. J. Am. Geriatr. Soc. 2004, 52, 540–546. [Google Scholar] [CrossRef]
Figure 1.
The most common methods used to estimate dietary intake of polyphenols.

Figure 2.
Biological properties of dietary polyphenols important in lifestyle diseases prevention.


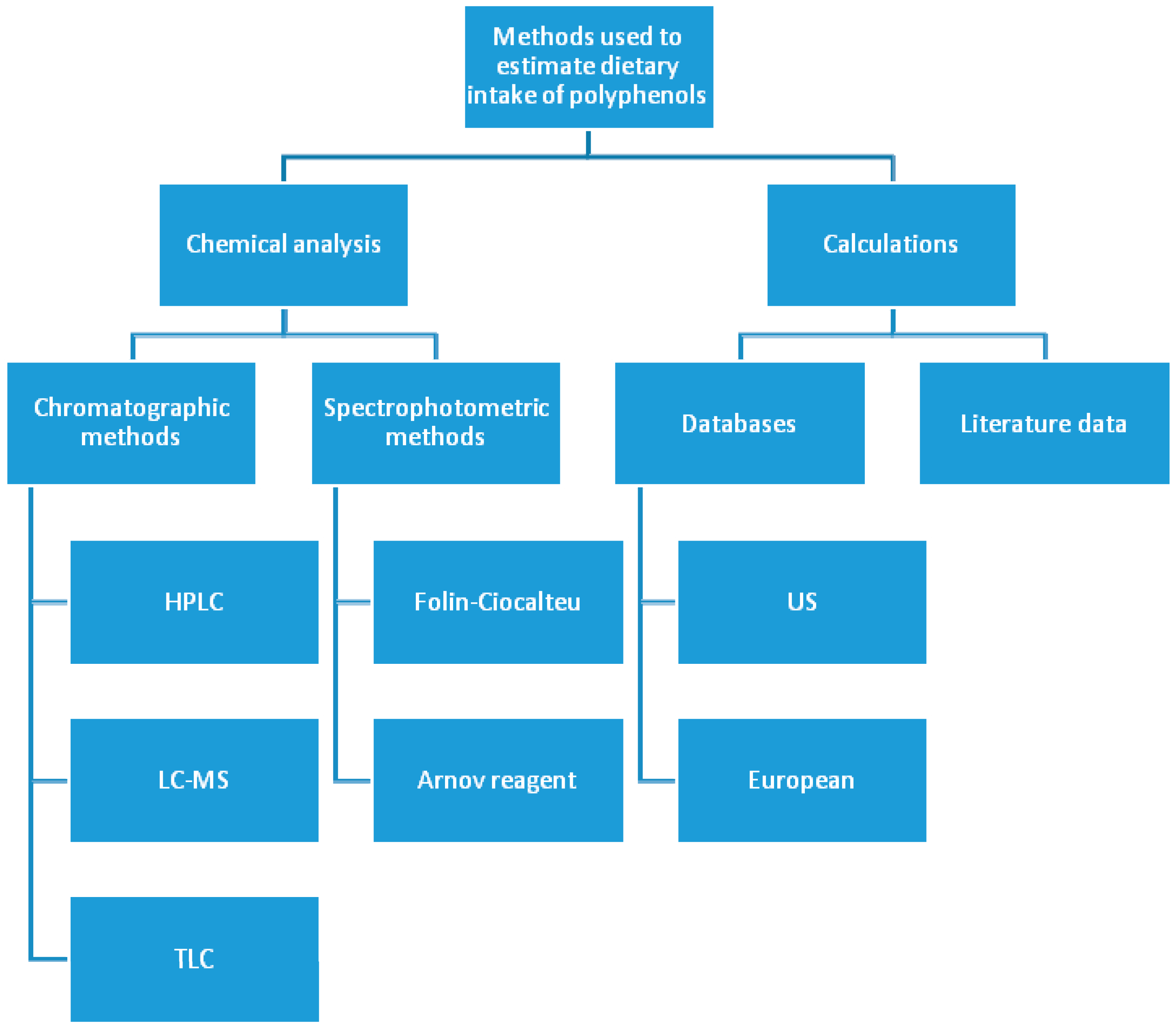{kind=link}
{kind=link}
Table 1.
Diet and lifestyle characteristic of hunter-gathers which resembled the habits of Paleolithic societies.
Table 1.
Diet and lifestyle characteristic of hunter-gathers which resembled the habits of Paleolithic societies.
| No | Characteristic | References |
|---|---|---|
| 1 | regular sun exposure (except the populations with high intake of vitamin D3 from fish and marine mammals, for which endogenous synthesis was less relevant, e.g., the Inuit) | [11,12,13,14] |
| 2 | sleep patterns according to natural day/night rhythm | [15] |
| 3 | lack of chronic stress/presence of acute stress | [16] |
| 4 | regular high physical activity—required to get food, to protect against predators or enemies, to building shelters, and to make social interactions | [17,18,19] |
| 5 | low environmental exposure to anthropological pollutants (e.g., pesticides, toxic heavy metals, cancerogenic carbohydrates etc.) | [16] |
| 6 | fresh (generally unprocessed) food a. plant leaves, seaweed, sea grasses, and algae b. roots and tubers c. berries and wild fruits d. insects, fish, marine animals, reptiles, and birds e. wild terrestrial mammals and eggs f. nuts and seeds g. honey (occasional intake) | [3,9,10,20,21,22,23] |
Table 2.
Health benefits of dietary polyphenols.
| Bioactivity | Experimental Model | Compound | Mechanism of Action/Effect | Ref. | |
|---|---|---|---|---|---|
| In Vitro | In Vivo | ||||
| Antioxidant | DPPH, ABTS, FRAP assays | Quercetin, rutin, EC, | —direct ROS scavenging —trace elements chelation —increasing the endogenic antioxidant enzymes production | [66,88,89,90,91,92,93] | |
| Ten healthy Korean subjects | Green tea polyphenols | —increased total capacity of blood plasma and serum | [90] | ||
| People subjected to anaerobic trainning | Theaflavins | —decreasing the oxidative stress in humans subjected to acute anaerobic interval training | [95] | ||
| Rats | Theaflavins and thearubigins | —increasing the antioxidant parameters of blood —significant reduction in lipid profile, glucose content and renal function —increasing the insulin level —the best results after administration of both theaflavins and thearubigins simultaneously | [96] | ||
| Athletes | Theasinensins from oolong tea | —strong reduction of malondialdehyde at rest and after exercise —decreased levels of SOD —reduced lipid peroxidation and cholesterol profile | [97] | ||
| Anti-inflammatory | Different immune cells | EGCG | —decreasing the production of proinflammatory chemokines —inhibition of the proliferation of autoreactive T cells —reducing the production of autoimmune agents | [99,100] | |
| Mice with collagen-induced arthritis | EGCG | —significant reduction in cytokines, phosphorylated-signal transducer and activator of transcription-3, 705 and 727 and oxidative stress proteins production —inhibition of osteoclast and Th 17 production —increased regulatory T cells production | [101] | ||
| Human peripheral blood neutrophils | Rutin, quercetin and vitexin | —significant reduction of NO, MPO and TNF-α (inflammatory mediators) production | [102,103] | ||
| Mice with an experimental autoimmune myocardiatitis | Apigenin | —inhibition of the proinflammatory cytokines production - Th1 cytokines, TNF-α, interferon-gamma (IFN-γ), and interleukin-2 (IL-2) | [104] | ||
| Anticancer | hepatocellular carcinoma LM6 cells (HCCLM6) | EGCG | —induction of apoptosis —reduction of mitochondrial membrane potential and promotion of G0/G1 phase cell cycle arrest —significant decrease in Bcl-2 and NF-κB expression. | [105] | |
| Mice with tongue and liver cancer induced by N-nitrosodiethylamine | Theaflavins and EGCG | —modulation of cellular proliferation/apoptosis and prevalence of CD 44 positive regulation | [106] | ||
| human prostate carcinoma (LNaCP and PC-3 cells) | Theaflavins | —tumor cell death by induction of p53 suppressor expression and inhibition of nuclear transcription factor NF-κβ and mitogen-activated MAPK-kinase, —the cell cycle blocking in the phase G2/M | [107,108] | ||
| human retinoblastoma (RB Y79 cell line) | Quercetin | —inhibition of tumor progression and invasion —angiogenesis inhibition | [110] | ||
| 9 different cancer cell lines (i.a. colon, prostate, breast and ovarian carcinomas). These results were confirmed in animal model, as | Mice with induced colon and breast cancers | Quercetin | —cell growth inhibition of all tested cell lines due to the induction of apoptosis —reduction of the tumor volume in a mouse model and increased animal survival | [111] | |
| Animal models with induced colorectal, breast, prostate, melanoma, renal cell and ovarian cancers | Apigenin | —reduction of proliferation, invasion and migration —increased apoptosis | [112,113,114,115,116,117,118] | ||
| human hepatic cancer HepG2 cells | Hesperidin | —activation of caspase-9, -8, and -3 —downregulation of Bcl-xL protein —upregulation of Bax, Bak, and tBid protein levels | [119] | ||
| MCF-7 human breast, androgen-independent PC-3 and DU-145 prostate cancer cells, and androgen-dependent LNCa cancer cells | Hesperidin | —inhibition of the proliferation of MCF-7-GFP-Tubulin cells and both basal and testosterone-induced proliferation of LNCaP cells | [120] | ||
| A2780 ovarian cancer cell line | Hesperidin | —induction of apoptosis —increasing cleaved caspase-3 protein expression levels —elevating the expression of proteins of antigrowth arrest- and DNA damage-inducible gene 153 —increasing anti-CCAAT’ enhancer-binding protein homologous protein expression —increasing the expression of glucose-regulated protein 78 and cytochrome c | [121] | ||
| Prevention of cardiovascular diseases | population-based cohort study on 1658 individuals | different subclasses of dietary flavonoids | —significant reduction of a risk of nonfatal CV events - the reduction of all-cause mortality parameters was the most significantly correlated with the intake of flavan-3-ols, anthocyanidins and flavanones | [84] | |
| a double-blind, placebo-controlled trial, on 56 obese, hypertensive subjects | Green tea polyphenols | —reduction of both systolic and diastolic blood pressures —significant reduction of TNF-α, C-reactive protein levels, fasting serum glucose, insulin levels and insulin resistance | [123] | ||
| Rats with induced hypertension caused by deoxycorticosterone acetate (DOCA) | EC | —inhibition of blood pressure increase —improving the impaired endothelium-dependent relaxation response to acetylcholine —reduction of plasma endothelin-1 and malondialdehyde levels | [126] | ||
| FRT cells transfected with human TMEM16A | Green tea polyphenols | —strong inhibition of calcium-activated Cl− channels —ECG and EGCG more strongly inhibited Cl− currents than the other polyphenols | [129] | ||
| Rats with induced hypertension | EGCG | —significant decrease of blood pressure —stimulated nitric oxide production from endothelium through a PI-3-kinase pathway | [131] | ||
| human recombinant renin inhibitor screening assay kit | EGCG | —inhibition of renin with IC50 value of 44.53 µg | [132] | ||
| Anti-obesity effect/weight reducing properties | 24 clinical, placebo-controlled trials, performed on obese patients | Green tea polyphenols (mostly 600–900 mg/day, which is equal to 3–4 cups of green tea) | —significant decrease in total abdominal fat are —inhibition of lipid synthesis —reduced serum triglycerides —reduction of food intake —deterioration of lipid emulsification and absorption, —induction of adipogenesis —increase of energy expenditure —Acceleration of fat oxidation —improvement of fecal lipid excretion | [133,134,135,136] | |
| Mice fed a high fat diet for 12 weeks | Mixture of quercetin and green tea extract administrated for four weeks | —downregulation of over 100 genes in adipose tissue, including those involved in leukocyte extravasation and phagocytosis —downregulation of cholesterol metabolism —reduction of cholesterol congeries in adipose and muscle tissue —mild improvement of glucose tolerance | [138] | ||
| Mice fed a high fat diet for 9 weeks | Diet enriched with quercetin in the concentration of 0.025% (w/w) | —regulation of hepatic gene expression related to lipid —significant reduction of liver and white adipose tissue weight —decrease in hepatic lipid accumulation —reduction of the size of lipid droplets in the animal epididymal fat pads | [140] | ||
| 3T3-L1 cells/isolated mouse epididymal adipose cells from C57BL/6J mice | Luteolin (20 μmol/L) | —insulin sensitivity increase —decrease of low-grade chronic inflammation —improved uptake of glucose by adipocytes —reduction of proinflammatory chemokines —reduction of mRNA levels of tumor necrosis factor α, IL-6 and MCP-1 —increasing the gene expression of adiponectin and leptin —activation of PPARγ target genes in animal adipose cells | [141] | ||
| Antidiabetic activity | streptozotocin-induced diabetic Wistar rats | Apigenin/rutin/geinistein/luteolin administrated intraperitoneal-ly for seven days (4 mg/kg body weight/day) | —strong hypoglycemic effect, especially observed in the oral glucose tolerance test —protective effect towards liver and kidneys | [143] | |
| HepG2 hepatocytes | type 1 diabetic LDL receptor-deficient mice (DMLDLR(-/-) | Apigenin <0.1% in DMSO (in vitro) 130 mg/kg/day (in vivo) for six weeks | —regulation of lipid and glucose metabolism through AMP-dependent kinase —prevention of lipid accumulation in the liver —inhibition of hyperlipidemia —slowing the aortic lesion development | [144] | |
| HIT-T15 pancreatic β-cells | Apigenin (20 mM in DMSO) | —inhibition of pancreatic β-cells damage through different oxidative stress related signaling pathways (decreasing ROS production, apoptosis and increasing the mitochondrial membrane potential) | [147] | ||
| Alloxan-treated diabetic mice | Apigenin (0.78 mg/kg/day in DMSO), s.c. for ten consecutive days | —increased serum insulin and thyroid hormone levels —reduction of blood glucose —reduction of hepaticG-6-Pase activity —reduction of serum cholesterol level —hepatoprotective activity (observed as decreased levels of lipid peroxidation and increased levels of catalase, SOD or glutathione) | [146] | ||
| Mice fed with high-fat diet | Naringin (0.2 g/kg diet, administrated orally) | —inhibition of inflammation and insulin resistance by blocking activation of the MAPKs pathways and by activating IRS-1 —lipid reduction by synthesis inhibition and increased fatty acid oxidation —hypoglycemic effect through the regulation of PEPCK and G6pase activity in the liver | [149] | ||
| Male diabetic C57BL/KsJ-db/db mice | Naringin and hesperidin (0.2 g/kg diet, administrated orally, separately) | —increasing the glucokinase mRNA level (both flavonoids) —reducing the mRNA expression of PEPCK and G6pase in the liver (naringin) —reducing the expression of hepatic glucose transporter 2 protein in the liver —upregulation of the expression of adipocyte GLUT-4 and hepatic and adipocyte PPARγ (both flavonoids) —reducing free fatty acid and TAGs plasma levels (both flavonoids) —inhibition of hepatic (HMG-CoA) reductase activity —increasing fecal cholesterol | [148] | ||
| Adult Djungarian hamsters/ Female C57BL/6JRj-mic | Naringenin and quercetin (10 mg/kg administered orally) | —impaired glucose tolerane —no influence on circulating levels of insulin and insulin-like growth factor-binding proteins —reduced respiratory quotient (impaired glucose utilization) (oral quercetin) | [150] | ||
| Rats with streptozotocin (STZ)-induced marginal type 1 diabetes | Hesperidin (10 g/kg diet) | —reduced blood glucose level by decreased activity of G6Pase and increased expression of GK —decreased glucose export through glucose transporter membrane proteins | [151] | ||
| Male C57BL/KsJ-db/db mice | Diet supplemented with hesperidin (0.2 g/kg diet) or naringin (0.2 g/kg diet) | —significant reduction of blood glucose (both flavonoids) —significant increase of GK activity and glycogen concentration (both flavonoids) —reduced activity of hepatic G6pase and PEPCK (naringin) —increased levels of Plasma insulin, C-peptide, and leptin (both flavonoids) | [152] | ||
| Male Wistar diabetic rats | Hesperidin (100 mg/kg/day) administrated orally | —significant mean arterial pressure improvement —reduced left ventricular end-diastolic pressure —improved both inotropic and lusitropic function of the heart —decreased level of TBARs —anti-apoptotic and protective effect | [154] | ||
| C2C12 murine skeletal myoblasts and H4IIE murine hepatocytes | Quercetin and its glycosylated forms isolated from Vaccinium vitis-idaea extract | —significant glucose uptake through the insulin-independent AMPK pathway —mild inhibition of mitochondrial ADP-stimulated oxygen consumption —inhibition of ATP synthase in mitochondria (only the aglycone) | [155] | ||
| Alloxan induced Swiss albino mice | Oral supplementation with quercetin (20 mg/kg body weight) for three weeks | —significant decrease of fasting blood glucose level —reduced markers of liver and kidneys injury —increased levels of antioxidant enzymes (SOD, glutathione, catalase and glutathione-S-transferase) —decreased concentration of TBARs —increased level of GLUT4 expression | [156] | ||
| STZ-induced diabetic mice | Quercetin administrated orally (0.1 and 0.5% of the diet) | —decreased blood glucose —increased insulin plasma level —suppression of the STZ-induced alteration of gene expression (0.5% of quercetin) —the strongest inhibitory effect towards elevated expression of cyclin-dependent kinase inhibitor p21(WAF1/Cip1) (Cdkn1a) | [157] | ||
| 3T3-L1 adipocyte cells | Quercetin | —inhibition of insulin-mediated GLUT4 translocation —improved glucose metabolism through the regulation AMPK activity —improvement of insulin cell sensitivity by inhibition of IκB kinase β (IKKβ) phosphorylation and insulin signaling facilitation | [158] | ||
| Diabetic mice | Quercetin administrated orally (0.04 and 0.08% of the diet) for six weeks | —dose dependent decrease of blood level glucose —decreased values of the HOMA-IR parameter —increased plasma adiponectin level (0.08% of quercetin) —reduced levels of LDL, total cholesterol, TAGs and increased HDL —decreased TBARs —increased concentration of the liver SOD, catalase and glutathione peroxidase | [160] | ||
| Rats fed with high sucrose diet | Oral supplementation with quercetin (30 mg/kg body weight per day) for six weeks | —no reduction on body weight or adipose tissue size was observed —reduced levels of fructosamine, basal glucose, insulin, and HOMA-IR —no influence on lipogenic enzymes and lipoprotein lipase activity was noticed —no change in muscle TAGs content was observed | [161] | ||
| STZ-induced diabetic rats | Rutin administrated orally (100 mg/kg body weight) for 45 days | —decrease of plasma glucose concentration —increased blood insulin level —restoration of glycogen content —protective effect towards pancreatic cells (reduced fatty infiltrate of the Langerhans islets) | [159] | ||
| α-glucosidase inhibition assay | Green, black and oolong tea extracts | —dose dependent inhibitory potential towards α-glucosidase —the strongest activity was revealed for oolong tea extract, followed by black and green tea —the activity of particular extract was attributed to the content of polyphenols | [162] | ||
| polarized Caco-2 intestinal cells | Green tea catechins | —inhibition of intestinal glucose uptake —nonglycosylated dietary polyphenols were the most effective in reduction of glucose uptake under both sodium-dependent and sodium-free conditions | [163] | ||
| Protective activity towards Parkinson’s Disease | Human α-synuclein assembly inhibitory test | Several dietary polyphenols (e.g., Tea catechins, apigenin, quercetin, rutin) | —dietary polyphenols are a major class of compounds active towards the inhibition of α-synuclein —tea catechins were characterized by the highest inhibitory activity —common dietary polyphenols (rutin, quercetin or naringenin) were less active | [178] | |
| α-synuclein fibrillation inhibitory assay | 48 flavonoids dissolved in DMSO at concentration of 5, 10, and 20 mM | —majority of flavonoids inhibited the fibrillation of α-synuclein (EGCG, rutin, luteolin) —the inhibition of α-synuclein fibrillogenesis was due to the inhibition of nucleus formation and the inhibition of fibril elongation —structure-activity dependency was noticed (a vicinal dihydroxyphenyl moiety was crucial for the inhibitory activity) —EGCG, myricetin, baicalein, eriodictyol and quercetin were the strongest inhibitors —diosmetin, hesperetin or hesperidin possessed no inhibitory activity —diosmetin, hesperetin or hesperidin possessed no inhibitory activity | [179] | ||
| α-synuclein fibrillation inhibitory assay | EGCG (50 µM) | —EGCG directly converted fibrillar species into benign protein aggregates —inhibition of α-synuclein and amyloid-β fibrillogenesis by EGCG through a direct binding to β-sheet-rich aggregates was proofed —EGCG did not reverse the process of fibril formation —no increase in toxic intermediates formation was noticed | [182] | ||
| Rat liver cytosol | Green tea catechins (EGCG and EGC) | —significant inhibition of catechol-O-methyltransferase enzyme (COMT) —dose-dependent methylation of EGCG by COMT was proofed —EGCG inhibited methylation of L-DOPA, a common drug used in the therapy of PD, and improved its bioavailability | [183] | ||
| Mice with MPTP induced Parkinsonism | Green tea extract and EGCG (0.5 and 1 mg/kg i.p.) | —increased activity of striatal antioxidant enzymes (SOD and catalase) —significant decrease loss of neurons and increase production of dopamine in substantia nigra —protective mechanism was proofed to be other than inhibition of MPTP transformation to its active metabolite —the protective effect of green tea polyphenols was identified with brain penetrating activity of polyphenols, its antioxidant activity and iron chelating properties | [184] | ||
| Male C57-BL Mice with MPTP induced Parkinsonism | EGCG (2mg/kg/day, per os, for 10 days) | —decreased levels of striatal tyrosine hydroxylase protein and increased activity of this enzyme —increased in PKCα protein expression inside the striatal dopaminergic fibers —neuroprotective activity through iron-chelating and antioxidant action | [185] | ||
| Rats with 6-OHDA-induced PD | Black tea extract 1.5% (administrated orally before and after 6-OHDA injection) | —a significant neuroprotective and neurorescue effects were observed (increased nigral gluthathione and striatal SOD catalase activity and decreased lipid peroxidation level) —improved spontaneous locomotor activity and dopamine (DA)-D2 receptor binding, —increased striatal DA and 3-4 dihydroxy phenyl acetic acid (DOPAC) level —significant increase of antiapoptotic and proapoptotic protein level —higher improvement in motor and neurochemical deficiency was more visible in rats receiving polyphenols before 6-OHDA administration | [186] | ||
| A case-control study conducted in western Washington State in 1992–2000 on 557 individuals | Tea (black or green) | —significant reduced risk of PD development in population drinking 2 cups/day or more of tea | [187] | ||
| Health Professional Follow-up Study performed on 49,281 men and the Nurses’ Health Study performed on 80,336 women | 5 classes of flavonoids (intake based on calculations using database and food frequency questionnaire) | —significant negative correlation between flavonoid intake and PD incidence —the strongest correlation between flavonoids intake and PD risk was found for anthocyanins —the significance of the obtained results was more visible in men, compared to women | [188] | ||
| Protective activity towards Alzheimer’s Disease | A cohort study on 1367 subjects above 65 years of age | Dietary flavonoid intake based on calculations | —significant inverse correlation between flavonoid intake and risk of dementia | [196] | |
| Transgenic mice with genetically induced AD | Diet supplemented with 2% of water blue berry extract | —significant improvement in memory and cognitive functions —improved neuronal signaling through enhanced extracellular signal-regulated kinase and decreased activity of N-Sase in the hippocampus and striatum —diet rich in antioxidant from blue berry extract may overpass genetic predispositions to AD —no influence of particular extract constituents were investigated | [199] | ||
| Human SH-SY5Y neuroblastoma cells/Rat pheochromocytoma PC12 cells | Male C57/BL mice | EGCG (2 mg/kg, per os, for 14 days) (in vivo) | —activation of activates PKCα and PKCε in the membrane and cytosolic fractions of mice hippocampus, which lead to increased production of neuroprotective, nonamyloidogenic sAPPα —reduction of cellular APP holoprotein production, which further reduces the progress of amyloidogenic failure —protective effect against β-amyloid-induced neurotoxicity | [200] | |
| Fresh, nonaggregated β-amyloid fractions | Wine derived polyphenols (myricetin, morin, quercetin, kaempferol, catechin, epicatechin) | —dose-dependent inhibition of β-amyloid formation —dose-dependent destabilization of preformed β-amyloid aggregation —the activity of particular polyphenols was varied in order: myricetin = morin = quercetin > kaempferol > catechin = epicatechin —the effective concentration was within the range of 0.1–1 µM | [201] | ||
| A cohort, population-based prospective study of 1836 Japanese Americans in King County, Washington | Fruit and vegetable juices, containing a high concentration of polyphenols (>3 times per week) | —significant reduction of the hazard ratio for probable Alzheimer’s disease, especially for population drinking more than 3 times per week —the strongest inverse association was revealed for people with an apolipoprotein Eε-4 allele and those who were not physically active | [204] | ||
| Tg2576 mice (model AD-type amyloid beta-protein neuropathology) | Red wine (Cabernet Sauvignon) diluted in drinking water | —improved cognitive functions —attenuation of β-amyloid deposition in neocortex and hippocampus —increased α-secretase activity —significant activity of red wine towards the inhibition of AD development was associated with its polyphenolic composition | [205] | ||
AD—Alzheimer’s disease; AMPK—5’ adenosine monophosphate-activated protein kinase; APP—amyloid precursor protein; EGC—epigallocatechin; PEPCK—Phosphoenolpyruvate carboxykinase; PPARγ—peroxisome proliferator-associated receptor; ROS—reactive oxygen species; TBARS—thiobarbituric acid reactive substances; SOD—SuperOxide Dismutase
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Koch, W. Dietary Polyphenols—Important Non-Nutrients in the Prevention of Chronic Noncommunicable Diseases. A Systematic Review. Nutrients 2019, 11, 1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051039
AMA Style
Koch W. Dietary Polyphenols—Important Non-Nutrients in the Prevention of Chronic Noncommunicable Diseases. A Systematic Review. Nutrients. 2019; 11(5):1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051039
Chicago/Turabian StyleKoch, Wojciech. 2019. "Dietary Polyphenols—Important Non-Nutrients in the Prevention of Chronic Noncommunicable Diseases. A Systematic Review" Nutrients 11, no. 5: 1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051039
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.