High Adherence to the Nordic Diet Is Associated with Lower Levels of Total and Platelet-Derived Circulating Microvesicles in a Norwegian Population

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Blood Sampling
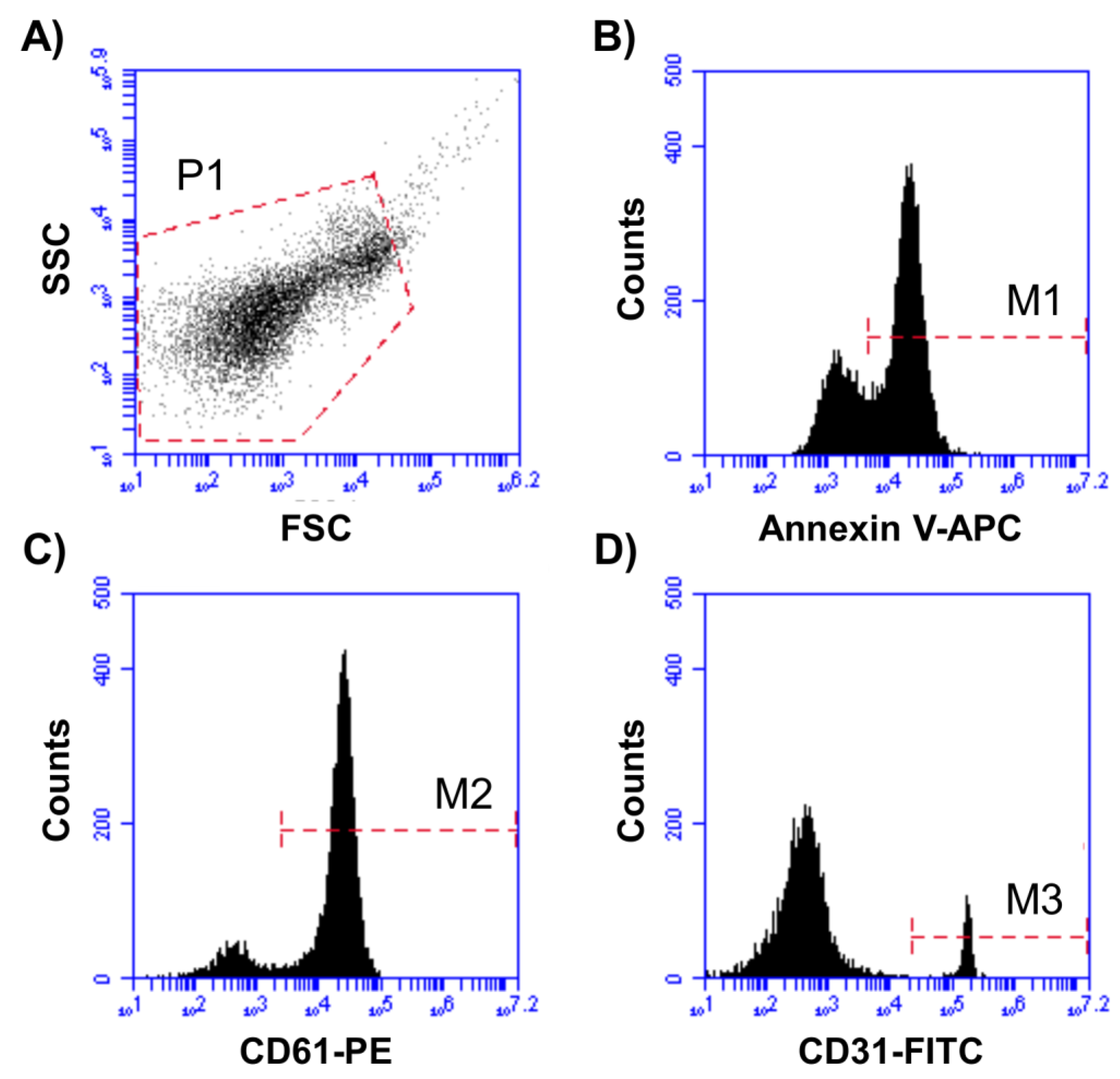
2.3. Circulating Microvesicle Isolation and Quantification
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Food Items and SmartDiet Score
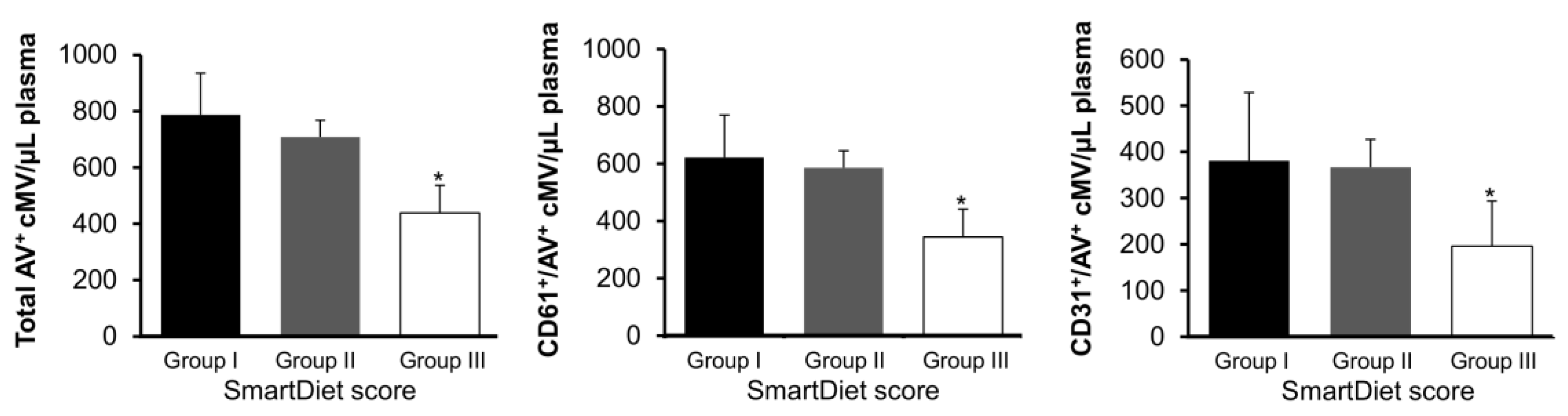
3.3. Associations between Circulating Microvesicles and SmartDiet Score
4. Discussion
4.1. Previous Knowledge
4.2. Main Findings of the Study
4.3. Review of Previous Data
4.4. Limitations and Scope of Future Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- de Mello, V.D.; Schwab, U.; Kolehmainen, M.; Koenig, W.; Siloaho, M.; Poutanen, K.; Mykkänen, H.; Uusitupa, M. A diet high in fatty fish, bilberries and wholegrain products improves markers of endothelial function and inflammation in individuals with impaired glucose metabolism in a randomised controlled trial: The Sysdimet study. Diabetologia 2011, 54, 2755–2767. [Google Scholar] [CrossRef]
- Badimon, L.; Chagas, P.; Chiva-Blanch, G. Diet and Cardiovascular Disease: Effects of Foods and Nutrients in Classical and Emerging Cardiovascular Risk Factors. Curr. Med. Chem. 2019, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Boulanger, C.M.; Loyer, X.; Rautou, P.E.; Amabile, N. Extracellular vesicles in coronary artery disease. Nat. Rev. Cardiol. 2017, 14, 259–272. [Google Scholar] [CrossRef]
- Badimon, L.; Suades, R.; Crespo, J.; Padro, T.; Chiva-Blanch, G. Diet, microparticles and atherothrombosis. Front Biosci. (Landmark Ed.) 2018, 23, 432–457. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Bratseth, V.; Ritschel, V.; Andersen, G.Ø.; Halvorsen, S.; Eritsland, J.; Arnesen, H.; Badimon, L.; Seljeflot, I. Monocyte-derived circulating microparticles (CD14+, CD14+/CD11b+ and CD14+/CD142+) are related to long-term prognosis for cardiovascular mortality in STEMI patients. Int. J. Cardiol. 2017, 227, 876–881. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Laake, K.; Myhre, P.; Bratseth, V.; Arnesen, H.; Solheim, S.; Badimon, L.; Seljeflot, I. Platelet-, monocyte-derived and tissue factor-carrying circulating microparticles are related to acute myocardial infarction severity. PLoS ONE 2017, 12, e0172558. [Google Scholar] [CrossRef] [PubMed]
- Laake, K.; Myhre, P.; Nordby, L.M.; Seljeflot, I.; Abdelnoor, M.; Smith, P.; Tveit, A.; Arnesen, H.; Solheim, S. Effects of omega 3 supplementation in elderly patients with acute myocardial infarction: Design of a prospective randomized placebo controlled study. BMC Geriatr. 2014, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Svilaas, A.; Ström, E.C.; Svilaas, T.; Borgejordet, A.; Thoresen, M.; Ose, L. Reproducibility and validity of a short food questionnaire for the assessment of dietary habits. Nutr. Metab. Cardiovasc. Dis. 2002, 12, 60–70. [Google Scholar] [PubMed]
- Lacroix, R.; Robert, S.; Poncelet, P.; Kasthuri, R.S.; Key, N.S.; Dignat-George, F. ISTH SSC Workshop Standardization of platelet-derived microparticle enumeration by flow cytometry with calibrated beads: Results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop. J. Thromb. Haemost. 2010, 8, 2571–2574. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Suades, R.; Crespo, J.; Vilahur, G.; Arderiu, G.; Padró, T.; Corella, D.; Salas-Salvadó, J.; Arós, F.; Martínez-González, M.A.; et al. CD3+/CD45+ and SMA-α+ circulating microparticles are increased in individuals at high cardiovascular risk who will develop a major cardiovascular event. Int. J. Cardiol. 2016, 208, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Nieuwland, R.; Berckmans, R.J.; McGregor, S.; Böing, A.N.; Romijn, F.P.; Westendorp, R.G.; Hack, C.E.; Sturk, A. Cellular origin and procoagulant properties of microparticles in meningococcal sepsis. Blood 2000, 95, 930–935. [Google Scholar]
- Berild, A.; Holven, K.B.; Ulven, S.M. Anbefalt nordisk kosthold og risikomarkører for hjerte- og karsykdom. Tidsskr. Den Nor. legeforening 2017, 137, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Ramezani-Jolfaie, N.; Mohammadi, M.; Salehi-Abargouei, A. The effect of healthy Nordic diet on cardio-metabolic markers: A systematic review and meta-analysis of randomized controlled clinical trials. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef]
- Adamsson, V.; Reumark, A.; Fredriksson, I.B.; Hammarström, E.; Vessby, B.; Johansson, G.; Risérus, U. Effects of a healthy Nordic diet on cardiovascular risk factors in hypercholesterolaemic subjects: A randomized controlled trial (NORDIET). J. Intern. Med. 2011, 269, 150–159. [Google Scholar] [CrossRef]
- Uusitupa, M.; Hermansen, K.; Savolainen, M.J.; Schwab, U.; Kolehmainen, M.; Brader, L.; Mortensen, L.S.; Cloetens, L.; Johansson-Persson, A.; Önning, G.; et al. Effects of an isocaloric healthy Nordic diet on insulin sensitivity, lipid profile and inflammation markers in metabolic syndrome - a randomized study (SYSDIET). J. Intern. Med. 2013, 274, 52–66. [Google Scholar] [CrossRef]
- Puaschitz, N.G.; Assmus, J.; Strand, E.; Karlsson, T.; Vinknes, K.J.; Lysne, V.; Drevon, C.A.; Tell, G.S.; Dierkes, J.; Nygård, O. Adherence to the Healthy Nordic Food Index and the incidence of acute myocardial infarction and mortality among patients with stable angina pectoris. J. Hum. Nutr. Diet 2019, 32, 86–97. [Google Scholar] [CrossRef]
- Suades, R.; Padró, T.; Vilahur, G.; Badimon, L. Circulating and platelet-derived microparticles in human blood enhance thrombosis on atherosclerotic plaques. Thromb. Haemost. 2012, 108, 1208–1219. [Google Scholar] [CrossRef]
- Elia, E.; Montecucco, F.; Portincasa, P.; Sahebkar, A.; Mollazadeh, H.; Carbone, F. Update on pathological platelet activation in coronary thrombosis. J. Cell Physiol. 2019, 234, 2121–2133. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Padró, T.; Alonso, R.; Crespo, J.; Perez de Isla, L.; Mata, P.; Badimon, L. Liquid biopsy of extracellular microvesicles maps coronary calcification and atherosclerotic plaque in asymptomatic patients with familial hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 945–955. [Google Scholar] [CrossRef]
- Horn, P.; Amabile, N.; Angeli, F.S.; Sansone, R.; Stegemann, B.; Kelm, M.; Springer, M.L.; Yeghiazarians, Y.; Schroeter, H.; Heiss, C. Dietary flavanol intervention lowers the levels of endothelial microparticles in coronary artery disease patients. Br. J. Nutr. 2014, 111, 1245–1252. [Google Scholar] [CrossRef]
- Marin, C.; Ramirez, R.; Delgado-Lista, J.; Yubero-Serrano, E.M.; Perez-Martinez, P.; Carracedo, J.; Garcia-Rios, A.; Rodriguez, F.; Gutierrez-Mariscal, F.M.; Gomez, P.; et al. Mediterranean diet reduces endothelial damage and improves the regenerative capacity of endothelium. Am. J. Clin. Nutr. 2011, 93, 267–274. [Google Scholar] [CrossRef]
- Wu, S.Y.; Mayneris-Perxachs, J.; Lovegrove, J.A.; Todd, S.; Yaqoob, P. Fish-oil supplementation alters numbers of circulating endothelial progenitor cells and microparticles independently of eNOS genotype. Am. J. Clin. Nutr. 2014, 100, 1232–1243. [Google Scholar] [CrossRef]
- Del Turco, S.; Basta, G.; Lazzerini, G.; Evangelista, M.; Rainaldi, G.; Tanganelli, P.; Christensen, J.H.; Schmidt, E.B.; De Caterina, R. Effect of the administration of n-3 polyunsaturated fatty acids on circulating levels of microparticles in patients with a previous myocardial infarction. Haematologica 2008, 93, 892–899. [Google Scholar] [CrossRef]
- Weech, M.; Altowaijri, H.; Mayneris-Perxachs, J.; Vafeiadou, K.; Madden, J.; Todd, S.; Jackson, K.G.; Lovegrove, J.A.; Yaqoob, P. Replacement of dietary saturated fat with unsaturated fats increases numbers of circulating endothelial progenitor cells and decreases numbers of microparticles: Findings from the randomized, controlled Dietary Intervention and VAScular function (DIVAS) study. Am. J. Clin. Nutr. 2018, 107, 876–882. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Least Healthy (1 point) | More Healthy (2 points) | Most Healthy (3 points) | |
|---|---|---|---|
| Milk or yogurt | |||
| What sort of milk do you use more often? | whole milk | low-fat milk or no milk at all | skimmed milk |
| Cream and sour cream | |||
| What sort of cream and sour cream do you use more often? | whole cream | light cream | extra-light cream or less than once weekly consumption |
| Cheese | |||
| What sort of cheese do you use more often? | white cheese | light cheese | cheese with rape and sunflower oil, extra-light cheese or less than once weekly consumption |
| Spreading/cured meat | |||
| What sort of spreading meat do you use more often? | fat meats | - | lean meats or less than once weekly consumption |
| Meat for dinner | |||
| What sort of meat do you consume for dinner more often? | Fat or processed meat | lean met with fat rim or skin | lean meats or less than once weekly consumption |
| Spreading fish | |||
| How often do you spread fish in sandwiches or in salads for lunch? | up to 1 slice of bread per week or never | between 2 and 4 slices of bread per week | about 5 or more slices of bread per week |
| Fish for dinner | |||
| How many times per week do you eat fish, fish products, and/or fish dishes? | between once per week and never | 2 times per week | 3 or more times per week |
| Mayonnaise, remoulade, and kaviar | |||
| How often do you use mayonnaise products on bread food? | Up to 1 slice of bread per week or never or 8 or more times per week | 2–7 slices of bread per week | - |
| Butter and margarine on bread food | |||
| What sort of butter and margarine do you use more often? | dairy butter | margarine | light margarine or low consumption of butter and margarine |
| Fat in cooking | |||
| What sort of fat do you use more often when frying, baking, or in sauce, such as dressings? | dairy butter | margarine | oils or use of fat for cooking |
| Bread and other grain products | |||
| What sort of bread or grain cereals do you use more often? | white bread or low bread consumption | - | whole-grain bread and cereals |
| Vegetables, fruits and berries | |||
| How many portions (150 g, equivalent to approximately 2 carrots or about a big apple) do you consume daily? | fewer than 2 portions (< 300 g) | 2–4 portions (300–600 g) | more than 4 portions (> 600 g) |
| Sweet toppings and sweet drinks | |||
| How often do you use sweet toppings or drinks with glucose or fructose? | 3 or more times per day | 2 times per day | 0–1 times per day |
| Chocolate, snacks, cakes and biscuits | |||
| How often do you eat snacks? | 3 or more times per week | 2 times per week | 0–1 times per week |
| mAb | Alternative Name | Expression | Conjugation | Clone | Company |
|---|---|---|---|---|---|
| AV | PS-binding protein | Widely expressed | APC | BD Biosciences | |
| CD142 | Tissue Factor | Widely expressed | FITC | VD8 | Sekisui diagnostics |
| Platelet-Related | |||||
| CD61 | β3-integrin | Platelets | PE | VI-PL2 | BD Pharmingen |
| CD31 | PECAM-1 | Activated Cells | FITC | AC128 | Miltenyi Biotec |
| CD62P | P-Selectin | Platelets | PE | HI62P | Immunotools |
| CD42b | Glycoprotein Ib alpha chain | Platelets and megakaryocytes | PE | REA185 | MACS Miltenyi |
| Endothelial Cell-Related | |||||
| CD146 | Melanoma Cell Adhesion Molecule | Endothelial Cells | FITC | P1H12 | BD Pharmingen |
| CD62E | E-Selectin | Endothelial Cells | PE | 68-5H11 | BD Biosciences |
| CD309 | VEGFR-2 | HSCs, EPCs, and ECs | FITC | ES8-20E6 | MACS Miltenyi |
| Erythrocyte-Related | |||||
| CD235ab | Glycophorin A and B | Erythrocytes | FITC | HIR2 | Immunotools |
| Leukocyte-Related | |||||
| CD45 | Leukocyte Common Antigen | Leukocytes | PE | MEM-28 | Immunotools |
| CD3 | T-cell co-receptor | T-Lymphocytes | FITC | HIT3b | Immunotools |
| CD14 | LPS-receptor | Macrophages, monocytes | PE | M5E2 | BD Pharmingen |
| CD62L | L-Selectin | Leukocytes | FITC | LT-TD180 | Immunotools |
| CD11b | Macrophage-1 Antigen (Mac-1) | Neutrophils, leukocytes | FITC | M1/70.15.11.5 | MACS Miltenyi |
| Smooth Muscle Cell-Related | |||||
| SMA-α | Smooth Muscle Actin α | Smooth muscle cells | PE | 1A4 | R&D Systems |
| Mean ± SD or n (%) | All Patients (n = 174) | Group I (n = 39) | Group II (n = 106) | Group III (n = 29) | p |
|---|---|---|---|---|---|
| Weeks after an AMI at inclusion | 0.994 | ||||
| 2 up to 4 weeks | 90 (52) | 21 (54) | 53 (50) | 16 (55) | |
| 4 up to 6 weeks | 41 (24) | 9 (23) | 25 (24) | 7 (24) | |
| 6–8 weeks | 43 (25) | 9 (23) | 28 (26) | 6 (21) | |
| Males | 124 (71.2) | 28 (71.8) | 78 (73.6) | 18 (62.1) | 0.371 |
| Age (years) | 75 ± 4 | 75 ± 4 | 74 ± 4 | 73 ± 3 | 0.403 |
| BMI (kg/m2) | 26.11 ± 4.04 | 25.77 ± 3.68 | 26.33 ± 4.46 | 26.16 ± 3.54 | 0.803 |
| Systolic blood pressure (mm Hg) | 139 ± 9 | 138 ± 23 | 139 ± 18 | 130 ± 14 | 0.092 |
| Diastolic blood pressure (mm Hg) | 75 ± 10 | 74 ± 11 | 76 ± 8 | 74 ± 10 | 0.651 |
| Total cholesterol (mmol/L) | 3.88 ± 0.82 | 3.74 ± 0.90 | 3.87 ± 0.83 | 3.93 ± 0.74 | 0.410 |
| HDL cholesterol (mmol/L) | 1.38 ± 0.44 | 1.40 ± 0.52 | 1.37 ± 0.38 | 1.42 ± 0.45 | 0.973 |
| Total cholesterol/HDL ratio | 2.97 ± 0.85 | 2.79 ± 0.57 | 2.95 ± 0.82 | 2.95 ± 0.90 | 0.867 |
| LDL cholesterol (mmol/L) | 2.16 ± 0.64 | 2.05 ± 0.59 | 2.17 ± 0.64 | 2.2 ± 0.64 | 0.525 |
| Triglycerides (mmol/L) | 1.30 ± 0.84 | 1.20 ± 0.33 | 1.24 ± 0.57 | 1.40 ± 1.69 | 0.580 |
| Glucose (mmol/L) | 6.23 ± 1.97 | 5.93 ± 1.66 | 6.22 ± 1.89 | 5.76 ± 0.98 | 0.372 |
| HbA1C (%) | 6.14 ± 1.01 | 6.08 ± 0.78 | 6.19 ± 1.12 | 5.83 ± 0.71 | 0.246 |
| Previous hypertension | 103 (59.2) | 26 (66.7) | 56 (52.8) | 21 (72.4) | 0.400 |
| Previous dyslipidemia | 78 (44.8) | 15 (38.5) | 51 (48.1) | 12 (41.4) | 0.346 |
| Previous diabetes | 41 (23.6) | 10 (25.6) | 25 (23.6) | 6 (20.7) | 0.864 |
| Current smokers | 17 (9.8) | 7 (17.9) | 7 (6.6) | 3 (10.3) | 0.151 |
| Medication after AMI | |||||
| Acetylsalicylic acid | 166 (95.4) | 35 (89.7) | 102 (96.2) | 29 (100) | 0.228 |
| ADP receptor inhibitors | 163 (94.7) | 36 (92.3) | 100 (94.3) | 27 (93.1) | 0.885 |
| Statins | 170 (97.7) | 38 (97.4) | 103 (97.2) | 29 (100) | 0.692 |
| Beta blockers | 153 (87.9) | 34 (87.1) | 91 (85.8) | 28 (96.5) | 0.174 |
| Calcium channel blockers | 31 (17.8) | 7 (17.9) | 22 (20.7) | 2 (6.9) | 0.280 |
| ACE inhibitors | 58 (33.3) | 13 (33.3) | 36 (34.0) | 9 (31.0) | 0.931 |
| ARB | 44 (25.3) | 8 (20.5) | 30 (28.3) | 6 (20.7) | 0.522 |
| Nitrates | 21 (12.1) | 3 (7.7) | 16 (15.1) | 2 (6.9) | 0.283 |
| Diuretics | 41 (23.6) | 8 (20.5) | 29 (27.3) | 4 (13.8) | 0.132 |
| Anticoagulants | 23 (13.2) | 7 (17.9) | 12 (11.3) | 4 (13.8) | 0.503 |
| Omega 3 supplements | 88 (50.6) | 20 (51.3) | 52 (49.1) | 16 (55.2) | 0.456 |
| N (%) | ||||
|---|---|---|---|---|
| Group I (Unhealthy Diet) | Group II (Somewhat Unhealthy Diet) | Group III (Healthy Diet) | p | |
| Milk or yogurt | 2.0 ± 0.5 a | 2.2 ± 0.5 a,b | 2.7 ± 0.5 b | 0.001 |
| Cream and sour cream | 1.7 ± 0.8 a | 2.5 ± 0.6 b | 2.8 ± 0.4 b | <0.0001 |
| Cheese | 1.1 ± 0.3 a | 1.6 ± 0.8 b | 2.7 ± 0.6 c | <0.0001 |
| Spreading/cured meat | 1.7 ± 1.0 c | 2.6 ± 0.8 b | 3.0 ± 0.0 b | <0.0001 |
| Meat for dinner | 1.7 ± 0.9 a | 2.6 ± 0.7 b | 3.0 ± 0.0 b | <0.0001 |
| Spreading fish | 1.8 ± 0.7 a | 2.0 ± 0.7 a | 2.5 ± 0.7 b | 0.027 |
| Fish for dinner | 1.8 ± 0.7 a | 2.2 ± 0.7 b | 2.7 ± 0.4 c | <0.0001 |
| Mayonnaise, remoulade, and kaviar | 1.4 ± 0.5 | 1.4 ± 0.5 | 1.4 ± 0.5 | 0.950 |
| Butter and margarine on bread food | 1.7 ± 1.0 a | 2.5 ± 0.8 b | 2.9 ± 0.3 b | <0.0001 |
| Fat in cooking | 1.4 ± 0.8 a | 2.3 ± 0.9 b | 2.8 ± 0.4 c | <0.0001 |
| Bread and other grain products | 1.5 ± 0.9 a | 2.5 ± 0.9 b | 2.7 ± 0.8 b | <0.0001 |
| Vegetables, fruits, and berries | 1.5 ± 0.5 a | 1.8 ± 0.6 b | 2.2 ± 0.4 c | 0.003 |
| Sweet toppings and sweet drinks | 2.6 ± 0.5 | 2.7 ± 0.6 | 2.9 ± 0.3 | 0.259 |
| Chocolate, snacks, cakes, and biscuits | 2.1 ± 0.8 a | 2.5 ± 0.7 b | 3.0 ± 0.0 c | 0.001 |
| SmartDiet Score | ||||
|---|---|---|---|---|
| cMV | R1 | p1 | β2 | p2 |
| Total cMV (AV+) | ||||
| Unadjusted | −0.179 | 0.027 | - | - |
| Multivariable adjusted* | 0.275 | 0.031 | −0.190 | 0.024 |
| Platelet-Derived cMV | ||||
| CD61+/AV+ | ||||
| Unadjusted | −0.198 | 0.014 | - | - |
| Multivariable adjusted* | 0.288 | 0.043 | −0.229 | 0.006 |
| CD31+/AV+ | ||||
| Unadjusted | −0.168 | 0.037 | - | - |
| Multivariable adjusted* | 0.328 | 0.016 | −0.179 | 0.033 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiva-Blanch, G.; Laake, K.; Myhre, P.; Bratseth, V.; Arnesen, H.; Solheim, S.; Badimon, L.; Seljeflot, I. High Adherence to the Nordic Diet Is Associated with Lower Levels of Total and Platelet-Derived Circulating Microvesicles in a Norwegian Population. Nutrients 2019, 11, 1114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051114
Chiva-Blanch G, Laake K, Myhre P, Bratseth V, Arnesen H, Solheim S, Badimon L, Seljeflot I. High Adherence to the Nordic Diet Is Associated with Lower Levels of Total and Platelet-Derived Circulating Microvesicles in a Norwegian Population. Nutrients. 2019; 11(5):1114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051114
Chicago/Turabian StyleChiva-Blanch, Gemma, Kristian Laake, Peder Myhre, Vibeke Bratseth, Harald Arnesen, Svein Solheim, Lina Badimon, and Ingebjørg Seljeflot. 2019. "High Adherence to the Nordic Diet Is Associated with Lower Levels of Total and Platelet-Derived Circulating Microvesicles in a Norwegian Population" Nutrients 11, no. 5: 1114. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051114