Perceptions and Factors Influencing Eating Behaviours and Physical Function in Community-Dwelling Ethnically Diverse Older Adults: A Longitudinal Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants and Recruitment
2.3. Theoretical Framework
2.4. Interviews
- Eating behaviours and factors influencing eating behaviours.
- Physical function and factors influencing physical function.This interview guide was iteratively revised at follow-up to include:
- Changes in factors influencing eating behaviours and physical function over the previous eight months.
2.5. Data Analysis
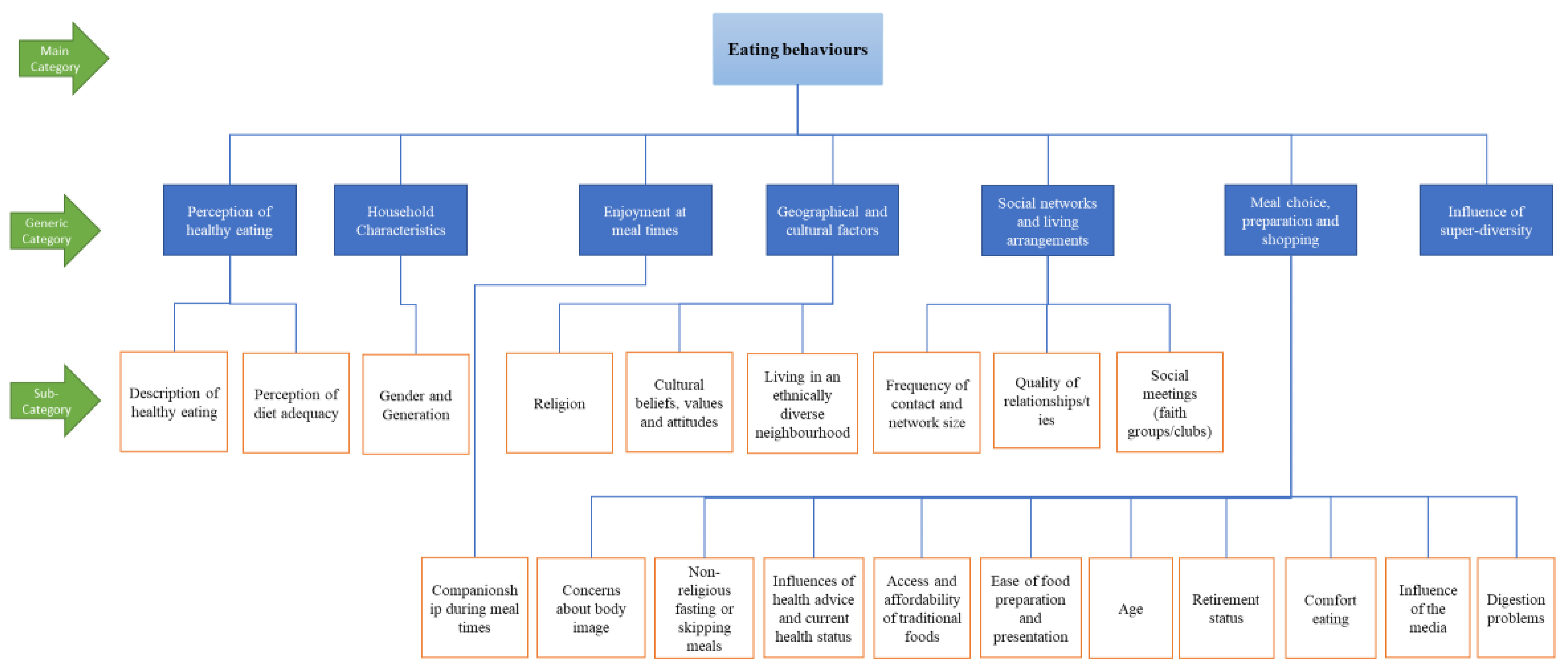
3. Results
- The differing perceptions of healthy eating and physical function.
- The personal, social and cultural/environmental factors influencing eating behaviours and physical function and how these factors differ among the sample.
- Perceived changes to eating behaviours and physical function over the 8-month follow-up period.
3.1. The Differing Perceptions of Healthy Eating and Physical Function
3.1.1. Healthy Eating
3.1.2. Physical Function
3.1.3. Priority and Association between Healthy Eating and Physical Function
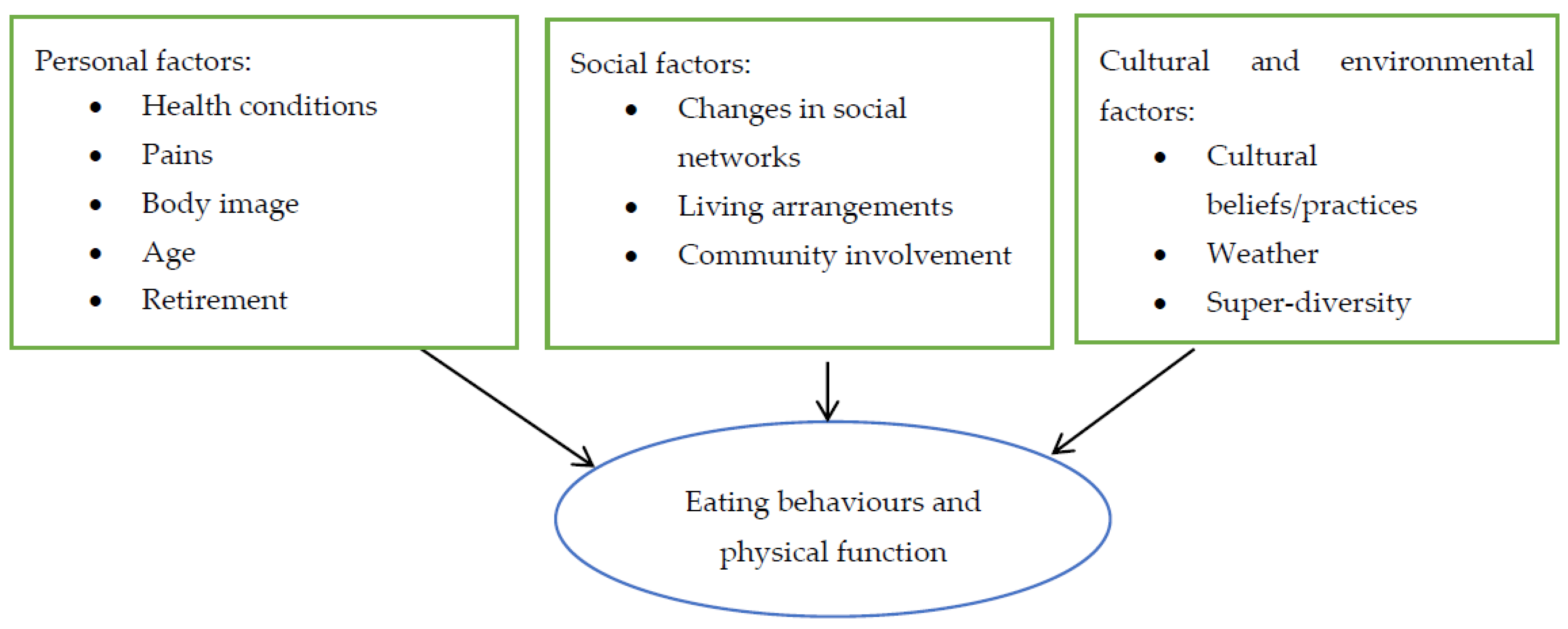
3.2. Factors Influencing Eating Behaviours and Physical Function
3.2.1. Personal Influences
Health Conditions
Pain
Body Image
Age
Retirement
3.2.2. Social Network Influences
3.2.3. Cultural and Environmental Factors
3.3. Perceived Changes at Follow-Up
4. Discussion
4.1. Perceptions of Healthy Eating and Physical Function
4.2. Factors Influencing Eating Behaviours and Physical Function
4.3. Perceived Priority and Association of Healthy Eating and Physical Function
4.3.1. Implications for Policy and Practice
4.3.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data Set and Materials
References
- Office for National Statistics. Ethnicity and National Identity in England and Wales. 2011. Available online: http://webarchive.nationalarchives.gov.uk/20160105160709/http://www.ons.gov.uk/ons/dcp171776_290558.pdf (accessed on 26 November 2018).
- Lievesley, N. The Ageing of the Ethnic Minority Populations of England and Wales: Findings from the 2011 Census; CPA: Bolton, UK, 2013. [Google Scholar]
- Rees, P.; Wohland, P.; Norman, P.; Boden, P. Ethnic Population Projections for the Uk, 2001–2051. J. Popul. Res. 2012, 29, 45–89. [Google Scholar] [CrossRef]
- Evandrou, M. Social Inequalities in Later Life: The Socio-Economic Position of Older People from Ethnic Minority Groups in Britain. Popul. Trends 2000, 101, 11–18. [Google Scholar]
- Nazroo, J.Y. The Health of Britain’s Ethnic Minorities: Findings from a National Survey; PSI: London, UK, 1997. [Google Scholar]
- Sproston, K.; Mindell, J. Health Survey for England 2004; The Health of Minority Ethnic Groups: London, UK, 2006; Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/health-survey-for-england-2004-health-of-ethnic-minorities-headline-results (accessed on 27 March 2019).
- Gilbert, P.A.; Khokhar, S. Changing Dietary Habits of Ethnic Groups in Europe and Implications for Health. Nutr. Rev. 2008, 66, 203–215. [Google Scholar]
- Jamal, A. Food Consumption among Ethnic Minorities: The Case of British-Pakistanis in Bradford, UK. Br. Food J. 1998, 100, 221–227. [Google Scholar] [CrossRef]
- Wyke, S.; Landman, J. Healthy Eating? Diet and Cuisine Amongst Scottish South Asian People. Br. Food J. 1997, 99, 27–34. [Google Scholar]
- Babakus, W.S.; Thompson, J.L. Physical Activity among South Asian Women: A Systematic, Mixed-Methods Review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 150. [Google Scholar] [CrossRef] [PubMed]
- Castaneda-Gameros, D.; Redwood, S.; Thompson, J.L. Physical Activity, Sedentary Time, and Frailty in Older Migrant Women from Ethnically Diverse Backgrounds: A Mixed-Methods Study. J. Aging Phys. Act. 2018, 26, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Emadian, A.; Thompson, J. A Mixed-Methods Examination of Physical Activity and Sedentary Time in Overweight and Obese South Asian Men Living in the United Kingdom. Int. J. Environ. Res. Public Health 2017, 14, 348. [Google Scholar] [CrossRef]
- Misra, A.; Ganda, O.P. Migration and Its Impact on Adiposity and Type 2 Diabetes. Nutrition 2007, 23, 696–708. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.; Stanner, S. Diets of Minority Ethnic Groups in the Uk: Influence on Chronic Disease Risk and Implications for Prevention. Nutr. Bull. 2011, 36, 161–198. [Google Scholar] [CrossRef]
- Age UK. Briefing: Health and Care of Older People in England; Age UK: London, UK, 2017. [Google Scholar]
- Bhopal, R.S.; Douglas, A.; Wallia, S.; Forbes, J.F.; Lean, M.E.; Gill, J.M.; McKnight, J.A.; Sattar, N.; Sheikh, A.; Wild, S.H. Effect of a Lifestyle Intervention on Weight Change in South Asian Individuals in the Uk at High Risk of Type 2 Diabetes: A Family-Cluster Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2014, 2, 218–227. [Google Scholar] [CrossRef]
- Garvin, C.C.; Cheadle, A.; Chrisman, N.; Chen, R.; Brunson, E. A Community-Based Approach to Diabetes Control in Multiple Cultural Groups. Ethn. Dis. 2004, 14, S1–S83. [Google Scholar]
- Two Feathers, J.; Kieffer, E.C.; Palmisano, G.; Anderson, M.; Sinco, B.; Janz, N.; Heisler, M.; Spencer, M.; Guzman, R.; Thompson, J. Racial and Ethnic Approaches to Community Health (Reach) Detroit Partnership: Improving Diabetes-Related Outcomes among African American and Latino Adults. Am. J. Public Health 2005, 95, 1552–1560. [Google Scholar] [CrossRef]
- Emadian, A.; England, C.Y.; Thompson, J.L. Dietary Intake and Factors Influencing Eating Behaviours in Overweight and Obese South Asian Men Living in the Uk: Mixed Method Study. Bmj Open 2017, 7, e016919. [Google Scholar] [CrossRef]
- Osei-Kwasi, H.A.; Powell, K.; Nicolaou, M.; Holdsworth, M. The Influence of Migration on Dietary Practices of Ghanaians Living in the United Kingdom: A Qualitative Study. Ann. Hum. Biol. 2017, 44, 454–463. [Google Scholar] [CrossRef]
- Nicolaou, M.; Doak, C.M.; van Dam, R.M.; Brug, J.; Stronks, K.; Seidell, J.C. Cultural and Social Influences on Food Consumption in Dutch Residents of Turkish and Moroccan Origin: A Qualitative Study. J. Nutr. Educ. Behav. 2009, 41, 232–241. [Google Scholar] [CrossRef]
- Corden, A.; Millar, J. Qualitative Longitudinal Research for Social Policy–Introduction to Themed Section. Soc. Policy Soc. 2007, 6, 529–532. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (Coreq): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Birmingham City Council. Population and Census. Available online: https://www.birmingham.gov.uk/info/20057/about_birmingham/1294/population_and_census/2 (accessed on 27 March 2019).
- Birmingham City Council. 2016 Population Based Projections. Available online: https://www.birmingham.gov.uk/downloads/file/4609/2016_population_based_projections (accessed on 27 March 2019).
- Patton, M. Qualitative Research and Evaluation Methods 2002 Thousand Oaks; Sage Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Penrod, J.; Preston, D.B.; Cain, R.E.; Starks, M.T. A Discussion of Chain Referral as a Method of Sampling Hard-to-Reach Populations. J. Transcult. Nurs. 2003, 14, 100–107. [Google Scholar] [CrossRef]
- Teddlie, C.; Yu, F. Mixed Methods Sampling: A Typology with Examples. J. Mix. Methods Res. 2007, 1, 77–100. [Google Scholar] [CrossRef]
- Garduño-Diaz, S.; Husain, W.; Ashkanani, F.; Khokhar, S. Meeting Challenges Related to the Dietary Assessment of Ethnic Minority Populations. J. Hum. Nutr. Diet. 2014, 27, 358–366. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. The Sage Handbook of Qualitative Research; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Moustakas, C. Phenomenological Research Methods; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [Green Version]
- Bronfenbrenner, U. International Encyclopedia of Education, 2nd ed.; Husen, T., Postlethwaite, T., Eds.; Pergamon Press/Elsevier Science: Oxford, UK, 1994; Volume 3, pp. 1643–1647. [Google Scholar]
- Castaneda-Gameros, D.; Redwood, S.; Thompson, J.L. Low Nutrient Intake and Frailty among Overweight and Obese Migrant Women from Ethnically Diverse Backgrounds Ages 60 Years and Older: A Mixed-Methods Study. J. Nutr. Educ. Behav. 2017, 49, 3–10.e11. [Google Scholar] [CrossRef] [PubMed]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Rubin, H.J.; Rubin, I.S. Qualitative Interviewing: The Art of Hearing Data; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Pope, C.; Ziedland, S.; Mays, N. Qualitative Research in Health Care: Analysing Qualitative Data. BMJ Br. Med. J. 2000, 320, 114. [Google Scholar] [CrossRef] [PubMed]
- QSR International. Nvivo Qualitative Data Analysis Software (Version 12); QSR International Pty Ltd.: Victoria, Australia, 2012. [Google Scholar]
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Castaneda-Gameros, D.; Redwood, S.; Thompson, J.L. Nutrient Intake and Factors Influencing Eating Behaviors in Older Migrant Women Living in the United Kingdom. Ecol. Food Nutr. 2018, 57, 50–68. [Google Scholar] [CrossRef]
- Thorne, S. Data Analysis in Qualitative Research. Evid. Based Nurs. 2000, 3, 68–70. [Google Scholar] [CrossRef]
- Brownie, S.; Coutts, R. Older Australians’ Perceptions and Practices in Relation to a Healthy Diet for Old Age: A Qualitative Study. J. Nutr. Health Aging 2013, 17, 125–129. [Google Scholar] [CrossRef]
- de Rosso Krug, R.; Rodrigues Barbosa, A.; Aita Monego, E.; de Mello, F.; Schaefer, A.L.; Francielle França, V. Perception of the Older Adults Regarding the Practise of Physical Activity and Healthy Eating. Rev. De La Univ. Ind. De Santander Salud 2015, 47, 115–124. [Google Scholar]
- Krahn, V.M.; Lengyel, C.O.; Hawranik, P. Healthy Eating Perceptions of Older Adults Living in Canadian Rural and Northern Communities. J. Nutr. Gerontol. Geriatr. 2011, 30, 261–273. [Google Scholar] [CrossRef]
- Bloom, I.; Lawrence, W.; Barker, M.; Baird, J.; Dennison, E.; Sayer, A.A.; Cooper, C.; Robinson, S. What Influences Diet Quality in Older People? A Qualitative Study among Community-Dwelling Older Adults from the Hertfordshire Cohort Study, UK. Public Health Nutr. 2017, 20, 2685–2693. [Google Scholar] [CrossRef]
- Office for National Statistics. 2011 Census: Detailed Analysis—English Language Proficiency in England and Wales, Main Language and General Health Characteristics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/language/articles/detailedanalysisenglishlanguageproficiencyinenglandandwales/2013-08-30 (accessed on 27 March 2019).
- Bramble, J.; Cornelius, L.J.; Simpson, G.M. Eating as a Cultural Expression of Caring among Afro-Caribbean and African American Women: Understanding the Cultural Dimensions of Obesity. J. Health Care Poor Underserved 2009, 20, 53. [Google Scholar] [CrossRef]
- Hudson, D.L.; Puterman, E.; Bibbins-Domingo, K.; Matthews, K.A.; Adler, N.E. Race, Life Course Socioeconomic Position, Racial Discrimination, Depressive Symptoms and Self-Rated Health. Soc. Sci. Med. 2013, 97, 7–14. [Google Scholar] [CrossRef]
- Evandrou, M.; Falkingham, J.; Feng, Z.; Vlachantoni, A. Ethnic Inequalities in Limiting Health and Self-Reported Health in Later Life Revisited. J. Epidemiol. Community Health 2016, 70, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an Effective Health Interventions Design: An Extension of the Health Belief Model. Online J. Public Health Inform. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Ree, M.; Riediger, N.; Moghadasian, M. Factors Affecting Food Selection in Canadian Population. Eur. J. Clin. Nutr. 2008, 62, 1255. [Google Scholar] [CrossRef]
- Horne, M.; Skelton, D.; Speed, S.; Todd, C. Attitudes and Beliefs to the Uptake and Maintenance of Physical Activity among Community-Dwelling South Asians Aged 60–70 Years: A Qualitative Study. Public Health 2012, 126, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Vertovec, S. Super-Diversity and Its Implications. Ethn. Racial Stud. 2007, 30, 1024–1054. [Google Scholar] [CrossRef]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef]
- Dean, M.; Raats, M.M.; Grunert, K.G.; Lumbers, M. Factors Influencing Eating a Varied Diet in Old Age. Public Health Nutr. 2009, 12, 2421–2427. [Google Scholar] [CrossRef]
- Sriskantharajah, J.; Kai, J. Promoting Physical Activity among South Asian Women with Coronary Heart Disease and Diabetes: What Might Help? Fam. Pract. 2006, 24, 71–76. [Google Scholar] [CrossRef]
- Bloom, I.; Edwards, M.; Jameson, K.A.; Syddall, H.E.; Dennison, E.; Gale, C.R.; Baird, J.; Cooper, C.; Aihie Sayer, A.; Robinson, S. Influences on Diet Quality in Older Age: The Importance of Social Factors. Age Ageing 2017, 46, 277–283. [Google Scholar] [CrossRef]
- Blane, D.; Wiggins, R.D.; Montgomery, S.M.; Hildon, Z.; Netuveli, G. Resilience at Older Ages: The Importance of Social Relations and Implications for Policy. Icls Occassional Pap. 2011, 3, 1–9. [Google Scholar]
- Hughes, G.; Bennett, K.M.; Hetherington, M.M. Old and Alone: Barriers to Healthy Eating in Older Men Living on Their Own. Appetite 2004, 43, 269–276. [Google Scholar] [CrossRef]
- McDonald, J.; Quandt, S.A.; Arcury, T.A.; Bell, R.A.; Vitolins, M.Z. On Their Own: Nutritional Self-Management Strategies of Rural Widowers. Gerontologist 2000, 40, 480–491. [Google Scholar] [CrossRef]
- Kumanyika, S.; Tell, G.S.; Shemanski, L.; Polak, J.; Savage, P.J.; Group, C.H.S.C.R. Eating Patterns of Community-Dwelling Older Adults: The Cardiovascular Health Study. Ann. Epidemiol. 1994, 4, 404–415. [Google Scholar] [CrossRef]
- Salmon, J.; Owen, N.; Crawford, D.; Bauman, A.; Sallis, J.F. Physical Activity and Sedentary Behavior: A Population-Based Study of Barriers, Enjoyment, and Preference. Health Psychol. 2003, 22, 178. [Google Scholar] [CrossRef]
- Judd, P.A.; Khamis, T.K.; Thomas, J.E. The Composition and Nutrient Content of Foods Commonly Consumed by South Asians in the UK; Aga Khan Health Board for the United Kingdom: London, UK, 2000. [Google Scholar]
- Buttriss, J. The Eatwell Guide Refreshed. Nutr. Bull. 2016, 41, 135–141. [Google Scholar] [CrossRef]
- Redwood, S.; Gill, P.S. Under-Representation of Minority Ethnic Groups in Research—Call for Action. Br. J. Gen. Pract. 2013, 63, 342–343. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C. Qualitative Research: Rigour and Qualitative Research. BMJ 1995, 311, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.D.; Wynne, J. Researching Community, Work and Family with an Interpreter. Communitywork Fam. 2001, 4, 157–171. [Google Scholar] [CrossRef]
- Temple, B.; Young, A. Qualitative Research and Translation Dilemmas. Qual. Res. 2004, 4, 161–178. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Baseline | Follow-Up | |||||
|---|---|---|---|---|---|---|---|
| Sex N (%) | Male 57 (57.0) | Female 35 (35.0) | Total 92 (100) | Male 50 (62.0) | Female 32 (38.0) | Total 81 (100) | |
| Age mean (SD) | 71(7.0) | 70 (9.0) | 70.6 (8.1) | 70 (8.0) | 71 (9.0) | 70.7 (8.2) | |
| Ethnicity N (%) | Caribbean | 14 (24.6) | 25 (71.4) | 39 (42.4) | 13 (26.0) | 25 (80.6) | 38 (46.9) |
| Pakistani | 17 (29.8) | 3 (8.6) | 20 (22) | 14 (28.0) | 1 (3.2) | 15 (18.5) | |
| African | 11 (19.3) | 6 (17.1) | 17 (18.5) | 11 (22.0) | 4 (12.9) | 15 (18.5) | |
| Bangladeshi | 4 (7.0) | 0 (0.0) | 4 (4.3) | 2 (4.0) | 0 (0.0) | 2 (2.5) | |
| Indian | 5 (8.8) | 1 (2.9) | 6 (6.5) | 4 (8.0) | 1 (3.2) | 5 (6.2) | |
| Others# | 6 (10.5) | 0 (0.0) | 6 (6.5) | 6 (12.0) | 0 (0.0) | 6 (7.4) | |
| Marital status N (%) | Married | 46 (80.7) | 16 (45.7) | 62 (67.4) | 40 (80.0) | 15 (48.4) | 55 (67.9) |
| Widowed | 6 (10.5) | 8 (22.9) | 14 (15.2) | 4 (8.0) | 7 (22.6) | 11 (13.6) | |
| Divorced | 4 (7.0) | 8 (22.9) | 12 (13.0) | 5 (10.0) | 7 (22.6) | 12 (14.8) | |
| Single | 1 (1.8) | 3 (8.6) | 4 (4.3) | 1 (2.0) | 2 (6.5) | 3 (3.7) | |
| Faith/Religion N (%) | Christian | 23 (40.4) | 30 (85.7) | 53 (57.6) | 22 (44.0) | 28 (90.3) | 50 (61.7) |
| Muslim | 29 (50.9) | 1 (2.9) | 30 (32.6) | 24 (48.0) | 0 (0.0) | 24 (29.6) | |
| Sikh | 3 (5.3) | 3 (8.6) | 6 (6.5) | 2 (4.0) | 2 (6.5) | 4 (4.9) | |
| Hindu | 2 (3.5) | 0 (0.0) | 2 (2.2) | 2 (4.0) | 0 (0.0) | 2 (2.5) | |
| No religion | 0 (0.0) | 1 (2.9) | 1 (1.1) | 0 (0.0) | 1 (3.2) | 1 (1.2) | |
| Education N (%) | College/University | 28 (49.1) | 17 (48.6) | 45 (48.9) | 26 (52.0) | 15 (48.4) | 41 (50.6) |
| Secondary School | 10 (17.5) | 8 (22.9) | 18 (19.6) | 8 (16.0) | 7 (22.6) | 15 (18.5) | |
| Primary School | 9 (15.8) | 6 (17.1) | 15 (16.3) | 9 (18.0) | 5 (16.1) | 14 (17.3) | |
| No education | 10 (17.5) | 4 (11.4) | 14 (15.2) | 7 (14.0) | 4 (12.9) | 11 (13.6) | |
| BMI categories N (%) | Normal | 4 (7.0) | 2 (5.7) | 6 (6.5) | 6 (12.0) | 3 (9.7) | 9 (11.1) |
| Overweight | 22 (38.6) | 7 (20.0) | 29 (34.5) | 13 (26.0) | 8 (25.8) | 21 (25.9) | |
| Obese | 31 (54.4) | 26 (74.3) | 57 (62.0) | 31 (62.0) | 20 (64.5) | 51 (63.0) | |
| IMD Quartile * N (%) | 1 (Most deprived) | 20 (35.1) | 12 (34.3) | 32 (34.8) | 18 (36.0) | 11 (35.5) | 29 (35.8) |
| 2 | 13 (22.8) | 6 (17.1) | 19 (20.7) | 13 (26.0) | 6 (19.4) | 19 (23.5) | |
| 3 | 11 (19.3) | 6 (17.1) | 17 (18.5) | 6 (12.0) | 5 (16.1) | 11 (13.6) | |
| 4 (least deprived) | 13 (22.8) | 11 (31.4) | 24 (26.1) | 13 (26.0) | 9 (29.0) | 22 (27.2) | |
| Self-rated health N (%) | Excellent | 9 (15.8) | 9 (25.7) | 18 (19.6) | 8 (16.0) | 8 (25.8) | 16 (19.8) |
| Good | 35 (61.4) | 17 (48.6) | 52 (56.5) | 31 (62.0) | 14 (45.2) | 45 (55.6) | |
| Fair | 7 (12.3) | 6 (17.1) | 13 (14.1) | 5 (10.0) | 6 (19.4) | 11 (13.6) | |
| Poor | 6 (10.5) | 3 (8.6) | 9 (9.8) | 6 (12.6) | 3 (9.7) | 9 (11.1) | |
| Length of stay in the UK mean (SD) (years) | 41.9 (16.2) | 43.8 (14.9) | 42.71 (15.9) | 41.5 (16.7) | 45.9 (15.5) | 43.2 (16.4) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asamane, E.A.; Greig, C.A.; Aunger, J.A.; Thompson, J.L. Perceptions and Factors Influencing Eating Behaviours and Physical Function in Community-Dwelling Ethnically Diverse Older Adults: A Longitudinal Qualitative Study. Nutrients 2019, 11, 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061224
Asamane EA, Greig CA, Aunger JA, Thompson JL. Perceptions and Factors Influencing Eating Behaviours and Physical Function in Community-Dwelling Ethnically Diverse Older Adults: A Longitudinal Qualitative Study. Nutrients. 2019; 11(6):1224. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061224
Chicago/Turabian StyleAsamane, Evans A., Carolyn A. Greig, Justin A. Aunger, and Janice L. Thompson. 2019. "Perceptions and Factors Influencing Eating Behaviours and Physical Function in Community-Dwelling Ethnically Diverse Older Adults: A Longitudinal Qualitative Study" Nutrients 11, no. 6: 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11061224