Considering Gender Differences in Portion Sizes to Improve the Accuracy of Nutrient Intakes from A Food Frequency Questionnaire

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Dietary Data Collection: QFFQ and 24HDRs
2.3. Gender Specific-Portion Size (GS-PS) Quantification
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Gender Specific-Portion Size (GS-PS)
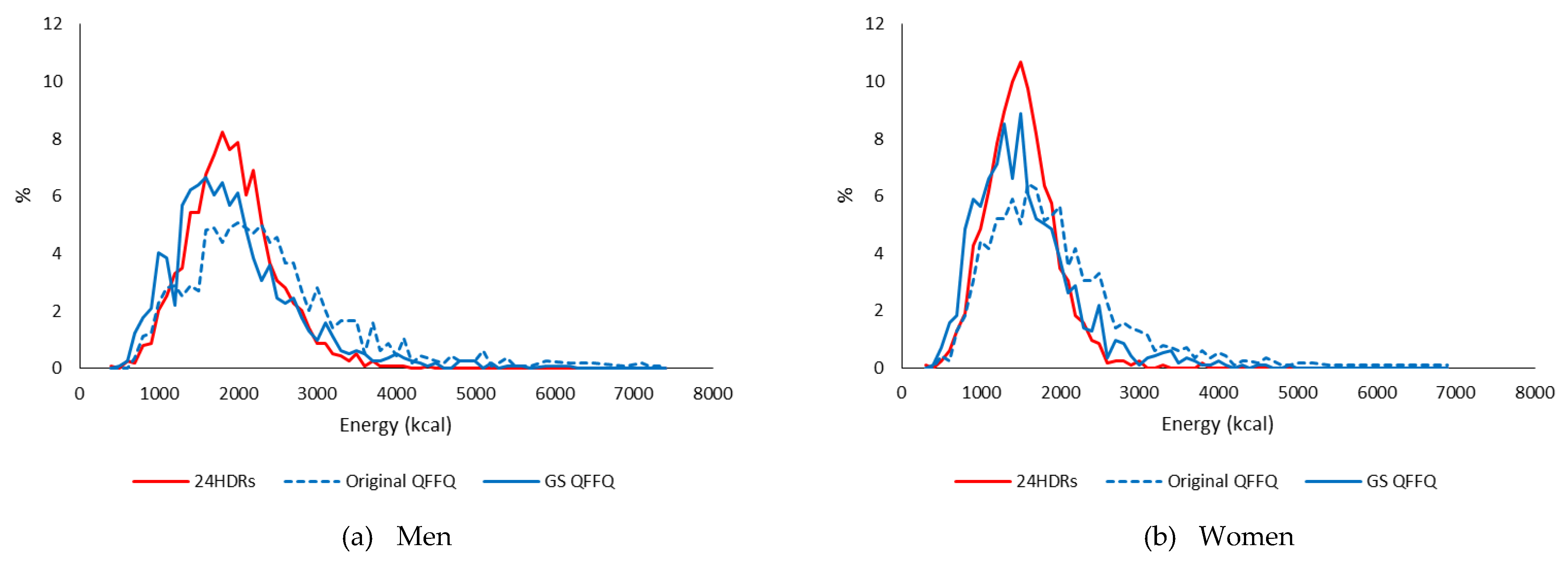
3.3. Utilizing GS-PS to Calculate Dietary Intake by QFFQ
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Coulston, A.M.; Boushey, C.J.; Ferruzzi, M.G.; Delahanty, L.M. Nutrition in the Prevention and Treatment of Disease, 4th ed.; Elsevier Academic Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Freedman, L.S.; Schatzkin, A.; Midthune, D.; Kipnis, V. Dealing with dietary measurement error in nutritional cohort studies. J. Natl. Cancer Inst. 2011, 103, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Beaton, G.H.; Milner, J.; Corey, P.; McGuire, V.; Cousins, M.; Stewart, E.; De Ramos, M.; Hewitt, D.; Grambsch, P.; Kassim, N. Sources of variance in 24-h dietary recall data: Implications for nutrition study design and interpretation. Am. J. Clin. Nutr. 1979, 12, 2546–2559. [Google Scholar] [CrossRef] [PubMed]
- Hankin, J.H. A diet history method for research, clinical, and community use: 23rd Lenna Frances Cooper Memorial Lecture. J. Am. Diet. Assoc. 1986, 86, 868–875. [Google Scholar] [PubMed]
- Hankin, J.H.; Wilkens, L.R. Development and validation of dietary assessment methods for culturally diverse populations. Am. J. Clin. Nutr. 1994, 59, 198S–200S. [Google Scholar] [CrossRef] [PubMed]
- Park, M.K.; Kim, D.W.; Kim, J.; Park, S.; Joung, H.; Song, W.O.; Paik, H.Y. Development of a dish-based, semi-quantitative FFQ for the Korean diet and cancer research using a database approach. Br. J. Nutr. 2011, 105, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Brunstrom, J.M.; Rogers, P.J.; Pothos, E.M.; Calitri, R.; Tapper, K. Estimating everyday portion size using a ‘method of constant stimuli’: In a student sample, portion size is predicted by gender, dietary behaviour, and hunger, but not BMI. Appetite 2008, 51, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Cavazza, N.; Guidetti, M.; Butera, F. Portion size tells who I am, food type tells who you are: Specific functions of amount and type of food in same-and opposite-sex dyadic eating contexts. Appetite 2017, 112, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.T.; Rennie, K.L.; Wallace, J.M.; Robson, P.J.; Welch, R.W.; Hannon-Fletcher, M.P.; Livingstone, M.B.E. Associations between the portion sizes of food groups consumed and measures of adiposity in the british national diet and nutrition survey. Br. J. Nutr. 2009, 101, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.; Sim, A.; Forde, C.; Cheon, B. The role of perceived stress and gender on portion selection patterns. Physiol. Behav. 2018, 194, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.; Jonnalagadda, S.; Clutter, D.; Smiciklas-Wright, H.; Kris-Etherton, P. Comparison of different methods for estimating food portion size: Gender differences. J. Am. Diet. Assoc. 1995, 95, A22. [Google Scholar] [CrossRef]
- O’Brien, S.; McNulty, B.; Nugent, A.; Gibney, E.; Livingstone, M. A comparison of gender differences in food portion sizes consumed by Irish adults during 1997 and 1999. Proc. Nutr. Soc. 2011, 70, OCE6. [Google Scholar] [CrossRef]
- Lee, H.; Kang, M.; Song, W.O.; Shim, J.E.; Paik, H.Y. Gender analysis in the development and validation of ffq: A systematic review. Br. J. Nutr. 2016, 115, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Kolonel, L.N.; Henderson, B.E.; Hankin, J.H.; Nomura, A.M.; Wilkens, L.R.; Pike, M.C.; Stram, D.O.; Monroe, K.R.; Earle, M.E.; Nagamine, F.S. A Multiethnic Cohort in Hawaii and Los Angeles: Baseline characteristics. Am. J. Epidemiol. 2000, 151, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Hankin, J.H.; Wilkens, L.R.; Kolonel, L.N.; Yoshizawa, C.N. Validation of a quantitative diet history method in Hawaii. Am. J. Epidemiol. 1991, 133, 616–628. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Park, S.-Y.; Boushey, C.J.; Wilkens, L.R.; Monroe, K.R.; Le Marchand, L.; Kolonel, L.N.; Murphy, S.P.; Paik, H.Y. Portion sizes from 24 h dietary recalls differed by sex among those who selected the same portion size category on a food frequency questionnaire. J. Acad. Nutr. Diet. 2018, 118, 1711–1718. [Google Scholar] [CrossRef]
- Kang, M.; Park, S.-Y.; Boushey, C.J.; Wilkens, L.R.; Le Marchand, L.; Kolonel, L.N.; Murphy, S.P.; Paik, H.Y. Ratios of food amounts across three portion size categories on a food frequency questionnaire in men and women. J. Acad. Nutr. Diet. 2019. under review. [Google Scholar]
- Stram, D.O.; Hankin, J.H.; Wilkens, L.R.; Pike, M.C.; Monroe, K.R.; Park, S.; Henderson, B.E.; Nomura, A.M.; Earle, M.E.; Nagamine, F.S. Calibration of the dietary questionnaire for a Multiethnic Cohort in Hawaii and Los Angeles. Am. J. Epidemiol. 2000, 151, 358–370. [Google Scholar] [CrossRef]
- Murphy, S.P. Unique nutrition support for research at the cancer research center of Hawaii. Hawaii Med. J. 2002, 61, 15–17. [Google Scholar]
- SAS Statistical Software, version 9.4; SAS Institute, Inc.: Cary, NC, USA, 2013.
- Noöthlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Fitting portion sizes in a self-administered food frequency questionnaire. J. Nutr. 2007, 137, 2781–2786. [Google Scholar] [CrossRef]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef]
- Joshipura, K.J.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Rimm, E.B.; Speizer, F.E.; Colditz, G.; Ascherio, A.; Rosner, B.; Spiegelman, D. The effect of fruit and vegetable intake on risk for coronary heart disease. Ann. Intern. Med. 2001, 134, 1106–1114. [Google Scholar] [CrossRef]
- Park, S.-Y.; Wilkens, L.R.; Kolonel, L.N.; Henderson, B.E.; Le Marchand, L. Inverse associations of dietary fiber and menopausal hormone therapy with colorectal cancer risk in the Multiethnic Cohort Study. Int. J. Cancer 2016, 139, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Kolonel, L.N.; Henderson, B.E.; Wilkens, L.R. Dietary fat and breast cancer in postmenopausal women according to ethnicity and hormone receptor status: The Multiethnic Cohort Study. Cancer Prev. Res. 2012, 5, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Cross, A.J.; Graubard, B.I.; Leitzmann, M.F.; Schatzkin, A. Meat intake and mortality: A prospective study of over half a million people. Arch. Intern. Med. 2009, 169, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S.; Sasazuki, S.; Kobayashi, M.; Sasaki, S. Salt and salted food intake and subsequent risk of gastric cancer among middle-aged Japanese men and women. Br. J. Cancer 2004, 90, 128. [Google Scholar] [CrossRef]
- Beaton, G.H. Approaches to analysis of dietary data: Relationship between planned analyses and choice of methodology. Am. J. Clin. Nutr. 1994, 59, 253S–261S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men (n = 1141) | Women (n = 1150) | p-value 1 | |
|---|---|---|---|
| Race/ethnicity | |||
| African American | 168 (14.7) | 197 (17.1) | 0.4746 |
| Native Hawaiian | 213 (18.7) | 217 (18.9) | |
| Japanese American | 292 (25.6) | 296 (25.7) | |
| Latino | 168 (14.7) | 150 (13.0) | |
| Non-Hispanic white | 300 (26.3) | 290 (25.2) | |
| Age | |||
| 45–54 years | 283 (24.8) | 324 (28.2) | 0.0973 |
| 55–64 years | 342 (30.0) | 352 (30.6) | |
| 65–75 years | 516 (45.2) | 474 (41.2) | |
| Education | |||
| ≤ High school graduate | 388 (34.4) | 449 (39.7) | 0.0160 |
| Vocational school/some college | 357 (31.7) | 352 (31.1) | |
| ≥ College graduate | 382 (33.9) | 330 (29.2) | |
| Body mass index | |||
| <25 kg/m2 | 491 (43.0) | 590 (51.3) | <.0001 |
| 25–30 kg/m2 | 490 (42.9) | 348 (30.3) | |
| ≥30 kg/m2 | 160 (14.0) | 212 (18.4) | |
| Smoking Status | |||
| Never | 369 (32.8) | 628 (55.8) | <.0001 |
| Former smoker | 579 (51.5) | 359 (31.9) | |
| Current smoker | 177 (15.7) | 139 (12.3) |
| Rule | Men | Women | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Portion Size Categories | Overall | Portion Size Categories | Overall | |||||||
| A | B | C | D | A | B | C | D | |||
| I. Using gender specific median values from 24HDRs | 79 (48.5) | 147 (90.2) | 104 (65.8) | 6 (85.7) | 336 (68.4) | 107 (65.6) | 145 (89.0) | 83 (52.5) | 3 (42.9) | 338 (68.8) |
| II. Imputing values using ratios to median values | 54 (33.1) | 4 (2.5) | 26 (16.5) | - | 84 (17.1) | 33 (20.2) | 2 (1.2) | 31 (19.6) | - | 66 (13.4) |
| III. Adapting the values of other portion sizes | 19 (11.7) | 1 (0.6) | 19 (12.0) | - | 39 (7.9) | 12 (7.4) | 5 (3.1) | 35 (22.2) | 1 (14.3) | 53 (10.8) |
| IV. Using the original-portion size | 11 (6.7) | 11 (6.7) | 9 (5.7) | 1 (14.3) | 32 (6.5) | 11 (6.7) | 11 (6.7) | 9 (5.7) | 3 (42.9) | 34 (6.9) |
| Total | 163 | 163 | 158 | 7 | 163 | 163 | 158 | 7 | ||
| Original Portion Size Category | % of Gender Specific-Portion Size Values to Original-Portion Size Values | ||||||
|---|---|---|---|---|---|---|---|
| <50% | 50%–70% | 70%–90% | 90%–110% | 110%–130% | 130%–150% | >150% | |
| Men | |||||||
| A | 1 (0.6) | 6 (3.7) | 12 (7.4) | 50 (30.7) | 16 (9.8) | 26 (16.0) | 52 (31.9) |
| B | 10 (6.1) | 27 (16.6) | 32 (19.6) | 68 (41.7) | 21 (12.9) | 2 (1.2) | 3 (1.8) |
| C | 31 (19.6) | 50 (31.7) | 35 (22.2) | 36 (22.8) | 6 (3.8) | - | - |
| D | 2 (28.6) | - | 2 (28.6) | 3 (42.9) | - | - | - |
| Overall | 44 (9.0) | 83 (16.9) | 81 (16.5) | 157 (32.0) | 43 (8.8) | 28 (5.7) | 55 (11.2) |
| Women | |||||||
| A | - | 14 (8.6) | 16 (9.8) | 50 (30.7) | 14 (8.6) | 27 (16.6) | 42 (25.8) |
| B | 12 (7.4) | 36 (22.1) | 38 (23.3) | 67 (41.1) | 5 (3.1) | 3 (1.8) | 2 (1.2) |
| C | 38 (24.1) | 62 (39.2) | 28 (17.7) | 30 (19.0) | - | - | - |
| D | 2 (28.6) | 1 (14.3) | 1 (14.3) | 3 (42.9) | - | - | - |
| Overall | 52 (10.6) | 113 (23.0) | 83 (16.9) | 150 (30.5) | 19 (3.9) | 30 (6.1) | 44 (9.0) |
| Nutrients by Unit | Men (n = 1141) | Women (n = 1150) | ||||
|---|---|---|---|---|---|---|
| 24HDRs | QFFQ | 24HDRs | QFFQ | |||
| Original-PS | GS-PS | Original-PS | GS-PS | |||
| Daily intake | ||||||
| Energy (kcal) | 1879.2 ± 553.2 | 2304.0 ± 1014.7 | 1886.0 ± 789.2 * | 1456.1 ± 422.8 | 1877.2 ± 866.2 | 1501.4 ± 634.7 |
| Macronutrients (g/day) | ||||||
| Protein | 75.1 ± 24.8 | 85.4 ± 40.2 | 70.5 ± 32.6 | 57.7 ± 18.3 | 71.6 ± 34.3 | 56.6 ± 25.3 * |
| Fat | 68.4 ± 28.1 | 78.2 ± 42.0 | 64.9 ± 33.1 | 53.2 ± 22.9 | 63.3 ± 35.9 | 50.1 ± 26.0 |
| Saturated fat | 20.6 ± 10.0 | 22.9 ± 13.4 | 19.0 ± 10.7 | 16.0 ± 7.7 | 18.4 ± 11.1 | 14.6 ± 8.3 |
| Carbohydrate | 233.4 ± 77.8 | 302.6 ± 134.7 | 244.4 ± 100.2 | 188.0 ± 58.9 | 260.1 ± 125.0 | 209.7 ± 93.1 |
| Dietary fiber | 16.8 ± 9.0 | 25.6 ± 14.3 | 21.0 ± 11.6 | 14.2 ± 6.5 | 24.3 ± 14.0 | 19.4 ± 10.6 |
| Vitamins and minerals (mg/day) | ||||||
| Vitamin A (IU) | 7032.0 ± 6010.3 | 12,343.7 ± 9860.6 | 9222.6 ± 6166.1 | 6885.9 ± 5826.1 | 13,241.7 ± 9933.6 | 9491.9 ± 6154.5 |
| Vitamin D (IU) | 127.2 ± 123.4 | 150.8 ± 114.1 | 129.9 ± 94.8 * | 104.2 ± 102.9 | 137.0 ± 102.1 | 113.2 ± 80.5 |
| Vitamin E | 8.8 ± 4.7 | 12.8 ± 8.2 | 10.9 ± 7.4 | 7.3 ± 3.8 | 10.6 ± 6.6 | 8.8 ± 5.9 |
| Vitamin C | 120.1 ± 86.5 | 181.7 ± 124.3 | 156.6 ± 101.6 | 113.0 ± 75.9 | 188.7 ± 128.7 | 161.3 ± 106.8 |
| Vitamin B6 | 1.8 ± 0.8 | 2.5 ± 1.3 | 2.1 ± 1.1 | 1.4 ± 0.6 | 2.1 ± 1.1 | 1.7 ± 0.9 |
| Vitamin B12 (mcg) | 4.4 ± 5.2 | 5.2 ± 3.8 | 4.6 ± 3.5 * | 3.2 ± 3.3 | 4.1 ± 2.8 | 3.5 ± 2.5 |
| Calcium | 592.3 ± 323.8 | 803.3 ± 426.6 | 674.5 ± 348.0 | 503.9 ± 264.1 | 750.8 ± 420.0 | 608.0 ± 332.7 |
| Phosphorous | 1113.8 ± 396.4 | 1382.6 ± 625.7 | 1145.1 ± 511.9 | 876.2 ± 308.8 | 1198.7 ± 575.8 | 956.0 ± 440.6 |
| Magnesium | 280.3 ± 109.1 | 370.4 ± 167.0 | 308.7 ± 136.4 | 221.9 ± 82.6 | 327.5 ± 156.1 | 264.2 ± 120.8 |
| Iron | 13.2 ± 5.8 | 18.3 ± 9.8 | 15.4 ± 8.6 | 10.3 ± 3.9 | 15.3 ± 8.3 | 12.5 ± 6.9 |
| Nutrient density | ||||||
| % kcal | ||||||
| Protein | 16.0 ± 3.4 | 14.7 ± 2.8 | 14.7 ± 2.7 | 15.9 ± 3.4 | 15.0 ± 2.9 | 14.8 ± 2.7 |
| Fat | 31.6 ± 7.5 | 29.7 ± 7.0 | 30.1 ± 6.9 | 31.3 ± 7.7 | 29.2 ± 7.0 | 29.0 ± 6.8 |
| Saturated fat | 9.5 ± 3.0 | 8.7 ± 2.6 | 8.8 ± 2.6 | 9.4 ± 3.1 | 8.5 ± 2.6 | 8.4 ± 2.5 |
| Carbohydrate | 49.7 ± 9.1 | 52.1 ± 9.3 | 51.5 ± 8.9 | 51.8 ± 8.9 | 54.4 ± 8.8 | 54.7 ± 8.5 |
| mg/1000 kcal | ||||||
| Dietary fiber (g) | 9.0 ± 4.0 | 11.1 ± 4.2 | 11.0 ± 4.0 | 10.0 ± 4.1 | 12.9 ± 4.5 | 12.7 ± 4.2 |
| Vitamin A (IU) | 3896.5 ± 3516.3 | 5482.8 ± 4720.2 | 4889.9 ± 3133.5 | 4969.5 ± 4519.8 | 7056.2 ± 4585.8 | 6273.4 ± 3422 |
| Vitamin D (IU) | 68.7 ± 64.5 | 66.1 ± 42.5 * | 68.5 ± 41.8 * | 72.5 ± 70.4 | 72.1 ± 45.5 * | 73.6 ± 43.3 * |
| Vitamin E | 4.6 ± 2.0 | 5.5 ± 3.1 | 5.8 ± 3.5 | 4.8 ± 2.0 | 5.5 ± 2.3 | 5.7 ± 2.8 |
| Vitamin C | 65.9 ± 44.8 | 80.2 ± 47.3 | 83.1 ± 45.9 | 81.4 ± 56.7 | 101.6 ± 56.2 | 106.7 ± 57.7 |
| Vitamin B6 | 1.0 ± 0.3 | 1.1 ± 0.4 | 1.1 ± 0.4 | 1.0 ± 0.4 | 1.1 ± 0.4 | 1.1 ± 0.4 |
| Vitamin B12 (mcg) | 2.3 ± 2.5 | 2.3 ± 1.4 * | 2.4 ± 1.5 * | 2.2 ± 2.3 | 2.1 ± 1.1 * | 2.3 ± 1.3 * |
| Calcium | 315.6 ± 143.1 | 349.5 ± 128.4 | 354.6 ± 123.4 | 344.9 ± 149.7 | 393.8 ± 139.0 | 395.2 ± 134.1 |
| Phosphorous | 591.7 ± 130.9 | 596.6 ± 120.3 * | 599.6 ± 119.5 | 600.5 ± 139.5 | 628.8 ± 127.8 | 624.0 ± 126.0 |
| Magnesium | 149.8 ± 40.0 | 160.9 ± 37.9 | 162.7 ± 37.7 | 154.9 ± 43.9 | 173.5 ± 39.6 | 174.0 ± 39.3 |
| Iron | 7.1 ± 2.5 | 8.0 ± 3.2 | 8.1 ± 3.5 | 7.2 ± 2.4 | 8.1 ± 2.6 | 8.1 ± 2.8 |
| Daily Intake | Nutrient Density | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Men (n = 1141) | Women (n = 1150) | Men (n = 1141) | Women (n = 1150) | ||||||
| Original-PS | GS-PS | Original-PS | GS-PS | Original-PS | GS-PS | Original-PS | GS-PS | ||
| Energy (kcal) | 0.30 | 0.24 | 0.28 | 0.23 | |||||
| Macronutrients (g/day) | Macronutrients (% energy) | ||||||||
| Protein | 0.29 | 0.23 | 0.29 | 0.26 | Protein | 0.38 | 0.38 | 0.49 | 0.50 |
| Fat | 0.37 | 0.33 | 0.34 | 0.29 | Fat | 0.62 | 0.63 | 0.62 | 0.61 |
| Saturated fat | 0.45 | 0.42 | 0.42 | 0.39 | Saturated fat | 0.68 | 0.69 | 0.70 | 0.69 |
| Carbohydrate | 0.37 | 0.33 | 0.36 | 0.34 | Carbohydrate | 0.66 | 0.68 | 0.66 | 0.65 |
| Dietary fiber | 0.47 | 0.48 | 0.49 | 0.49 | Dietary fiber (g/1000 kcal) | 0.74 | 0.75 | 0.75 | 0.75 |
| Vitamins and Minerals (mg/day) | Vitamins and Minerals (mg/1000 kcal) | ||||||||
| Vitamin A (IU) | 0.45 | 0.43 | 0.47 | 0.46 | Vitamin A (IU) | 0.59 | 0.59 | 0.60 | 0.60 |
| Vitamin D (IU) | 0.52 | 0.52 | 0.56 | 0.55 | Vitamin D (IU) | 0.60 | 0.59 | 0.63 | 0.62 |
| Vitamin E | 0.27 | 0.24 | 0.25 | 0.19 | Vitamin E | 0.42 | 0.40 | 0.37 | 0.34 |
| Vitamin C | 0.55 | 0.56 | 0.56 | 0.58 | Vitamin C | 0.66 | 0.66 | 0.65 | 0.66 |
| Vitamin B6 | 0.41 | 0.39 | 0.41 | 0.40 | Vitamin B6 | 0.64 | 0.63 | 0.58 | 0.58 |
| Vitamin B12 (mcg) | 0.34 | 0.31 | 0.36 | 0.33 | Vitamin B12 (mcg) | 0.41 | 0.40 | 0.43 | 0.41 |
| Calcium | 0.49 | 0.49 | 0.51 | 0.50 | Calcium | 0.73 | 0.72 | 0.74 | 0.74 |
| Phosphorous | 0.36 | 0.34 | 0.39 | 0.37 | Phosphorous | 0.69 | 0.69 | 0.67 | 0.67 |
| Magnesium | 0.40 | 0.39 | 0.40 | 0.39 | Magnesium | 0.71 | 0.71 | 0.66 | 0.67 |
| Iron | 0.40 | 0.38 | 0.34 | 0.31 | Iron | 0.62 | 0.60 | 0.56 | 0.54 |
| Average | 0.40 | 0.38 | 0.40 | 0.38 | Average | 0.61 | 0.61 | 0.61 | 0.60 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.; Park, S.-Y.; Boushey, C.J.; Wilkens, L.R.; Marchand, L.L.; Kolonel, L.N.; Murphy, S.P.; Paik, H.-Y. Considering Gender Differences in Portion Sizes to Improve the Accuracy of Nutrient Intakes from A Food Frequency Questionnaire. Nutrients 2019, 11, 1449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071449
Kang M, Park S-Y, Boushey CJ, Wilkens LR, Marchand LL, Kolonel LN, Murphy SP, Paik H-Y. Considering Gender Differences in Portion Sizes to Improve the Accuracy of Nutrient Intakes from A Food Frequency Questionnaire. Nutrients. 2019; 11(7):1449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071449
Chicago/Turabian StyleKang, Minji, Song-Yi Park, Carol J. Boushey, Lynne R. Wilkens, Loïc Le Marchand, Laurence N. Kolonel, Suzanne P. Murphy, and Hee-Young Paik. 2019. "Considering Gender Differences in Portion Sizes to Improve the Accuracy of Nutrient Intakes from A Food Frequency Questionnaire" Nutrients 11, no. 7: 1449. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11071449