Can a Simple Dietary Screening in Early Pregnancy Identify Dietary Habits Associated with Gestational Diabetes?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Cohort Study
2.1.1. The Outcome Variable
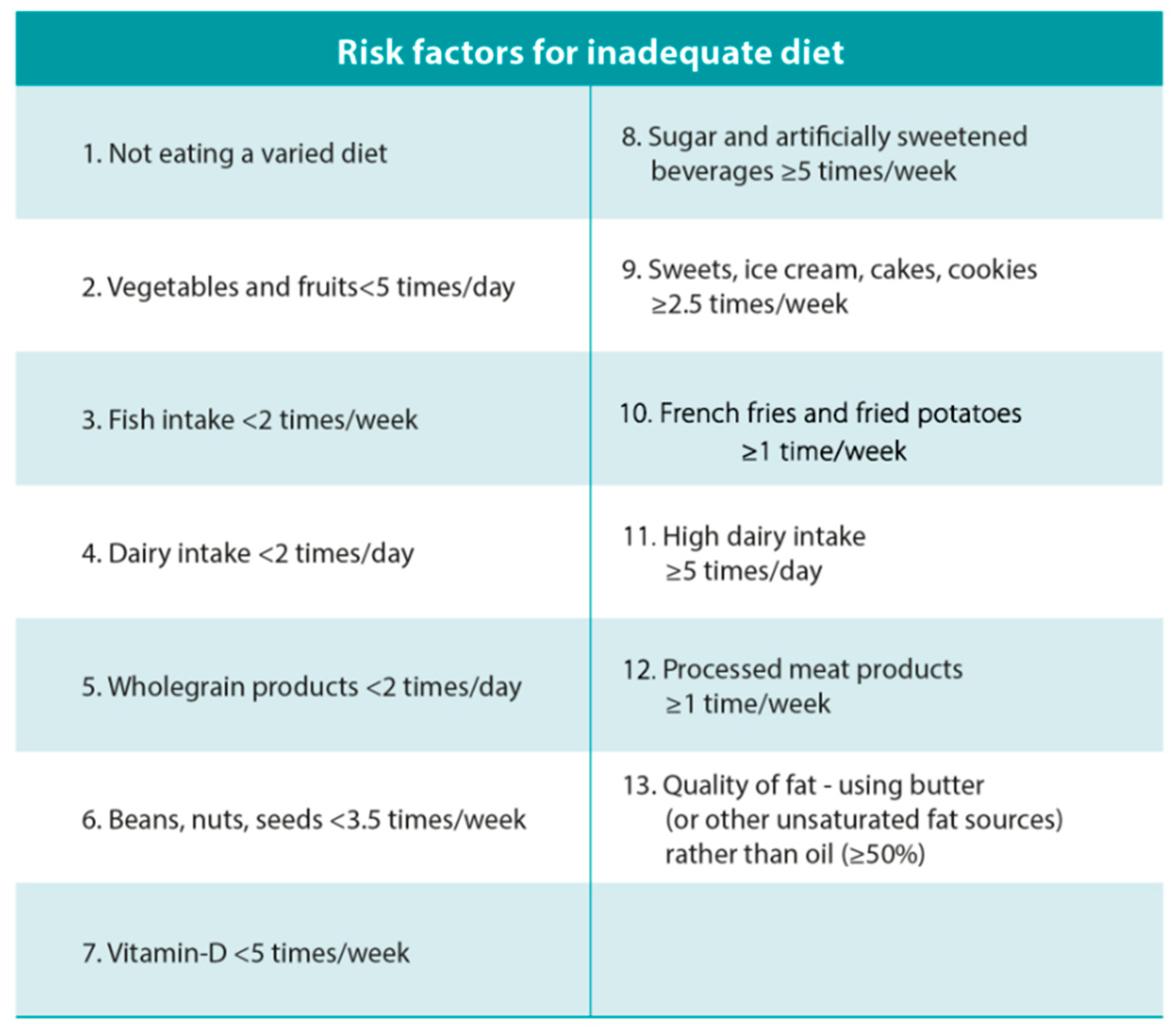
2.1.2. The Dietary Assessment and the Dietary Risk Score
2.2. The Pilot Intervention Study
2.3. Statistical Analyses
2.4. Ethics
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Crude b RR (95%CI) | Adjusted b,c RR (95%CI) | |
|---|---|---|
| SCORE-1 | 1.23 (1.10, 1.36) | 1.11 (1.00, 1.22) |
| SCORE-2 | 1.26 (1.13, 1.40) | 1.13 (1.02, 1.25) |
| SCORE-3 | 1.22 (1.09, 1.36) | 1.10 (0.99, 1.22) |
| 5 | Control (n = 41) a | Intervention (n = 47) a | p Value b |
|---|---|---|---|
| Milk | 5.3 (2.2–7.6) | 5.4 (2.1–14.4) | 0.289 |
| Cultured milk | 5.0 (1.0–5.0) | 2.5 (1.0–5.0) | 0.876 |
| Beans, nuts and/or seeds | 0.5 (0.1–1.0) | 0.5 (0.1–2.5) | 0.244 |
| Vegetables | 7.0 (3.8–7.0) | 7.0 (2.5–14) | 0.202 |
| Fruits and berries | 14.0 (7.0–14) | 7.0 (5.0–14) | 0.655 |
| Fish | 1.1 (1.0–2.8) | 1.5 (0.8–2.8) | 0.803 |
| Processed meat | 0.5 (0.3–0.8) | 0.5 (0.3–1.0) | 0.158 |
| Soft drinks | 2.0 (0.6–5.0) | 2.0 (0.6–3.5) | 0.556 |
| French fries or chips | 0.5 (0.5–1.0) | 0.5 (0.5–1.0) | 0.554 |
| Cakes, biscuits, ice and sweets | 3.5 (1.5–6.0) | 2.7 (1.5–5.0) | 0.058 |
References
- Zhu, Y.; Zhang, C. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: A Global Perspective. Curr. Diabetes Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Wendland, E.M.; Torloni, M.R.; Falavigna, M.; Trujillo, J.; Dode, M.A.; Campos, M.A.; Duncan, B.B.; Schmidt, M.I. Gestational diabetes and pregnancy outcomes—A systematic review of the World Health Organization (WHO) and the International Association of Diabetes in Pregnancy Study Groups (IADPSG) diagnostic criteria. BMC Pregnancy Childbirth 2012, 12, 23. [Google Scholar] [CrossRef] [PubMed]
- Alberico, S.; Montico, M.; Barresi, V.; Monasta, L.; Businelli, C.; Soini, V.; Erenbourg, A.; Ronfani, L.; Maso, G. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: Results from a prospective multicentre study. BMC Pregnancy Childbirth 2014, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Vohr, B.R.; Boney, C.M. Gestational diabetes: The forerunner for the development of maternal and childhood obesity and metabolic syndrome? J. Matern. Fetal Neonatal Med. 2008, 21, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.; Hod, M.; Kitzmiler, J.L.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Donazar-Ezcurra, M.; Lopez-Del Burgo, C.; Martinez-Gonzalez, M.A.; Basterra-Gortari, F.J.; de Irala, J.; Bes-Rastrollo, M. Pre-pregnancy adherences to empirically derived dietary patterns and gestational diabetes risk in a Mediterranean cohort: The Seguimiento Universidad de Navarra (SUN) project. Br. J. Nutr. 2017, 118, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Schulze, M.B.; Solomon, C.G.; Hu, F.B. A prospective study of dietary patterns, meat intake and the risk of gestational diabetes mellitus. Diabetologia 2006, 49, 2604–2613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tryggvadottir, E.A.; Medek, H.; Birgisdottir, B.E.; Geirsson, R.T.; Gunnarsdottir, I. Association between healthy maternal dietary pattern and risk for gestational diabetes mellitus. Eur. J. Clin. Nutr. 2016, 70, 237–242. [Google Scholar] [CrossRef] [PubMed]
- He, J.R.; Yuan, M.Y.; Chen, N.N.; Lu, J.H.; Hu, C.Y.; Mai, W.B.; Zhang, R.F.; Pan, Y.H.; Qiu, L.; Wu, Y.F.; et al. Maternal dietary patterns and gestational diabetes mellitus: A large prospective cohort study in China. Br. J. Nutr. 2015, 113, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns during Pregnancy Are Associated with Risk of Gestational Diabetes Mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenaker, D.A.; Mishra, G.D.; Callaway, L.K.; Soedamah-Muthu, S.S. The Role of Energy, Nutrients, Foods, and Dietary Patterns in the Development of Gestational Diabetes Mellitus: A Systematic Review of Observational Studies. Diabetes Care 2016, 39, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.M.; McGowan, C.A.; Mahony, R.; Foley, M.E.; McAuliffe, F.M. Low glycaemic index diet in pregnancy to prevent macrosomia (ROLO study): Randomised control trial. BMJ 2012, 345, e5605. [Google Scholar] [CrossRef]
- Khoury, J.; Henriksen, T.; Christophersen, B.; Tonstad, S. Effect of a cholesterol-lowering diet on maternal, cord, and neonatal lipids, and pregnancy outcome: A randomized clinical trial. Am. J. Obstet. Gynecol. 2005, 193, 1292–1301. [Google Scholar] [CrossRef] [PubMed]
- Briley, A.L.; Barr, S.; Badger, S.; Bell, R.; Croker, H.; Godfrey, K.M.; Holmes, B.; Kinnunen, T.I.; Nelson, S.M.; Oteng-Ntim, E.; et al. A complex intervention to improve pregnancy outcome in obese women; the UPBEAT randomised controlled trial. BMC Pregnancy Childbirth 2014, 14, 74. [Google Scholar] [CrossRef]
- Hrolfsdottir, L.; Halldorsson, T.I.; Birgisdottir, B.E.; Hreidarsdottir, I.T.; Hardardottir, H.; Gunnarsdottir, I. Development of a dietary screening questionnaire to predict excessive weight gain in pregnancy. Matern. Child Nutr. 2018, e12639. [Google Scholar] [CrossRef]
- Nordic Nutrition Recommendations. Integrating Nutrition and Physical Activity; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Embætti Landlæknis. Grundvöllur Ráðlegginga um Mataræði og Ráðlagðir Dagskammtar Næringarefna; Embætti Landlæknis: Reykjavík, Iceland, 2016. [Google Scholar]
- Gunnarsdottir, I.; Tryggvadottir, E.A.; Birgisdottir, B.E.; Halldorsson, T.I.; Medek, H.; Geirsson, R.T. Diet and nutrient intake of pregnant women in the capital area in Iceland. Laeknabladid 2016, 102, 378–384. [Google Scholar]
- Olsen, S.F.; Halldorsson, T.I.; Willett, W.C.; Knudsen, V.K.; Gillman, M.W.; Mikkelsen, T.B.; Olsen, J. Milk consumption during pregnancy is associated with increased infant size at birth: Prospective cohort study. Am. J. Clin. Nutr. 2007, 86, 1104–1110. [Google Scholar] [CrossRef]
- Renault, K.M.; Carlsen, E.M.; Norgaard, K.; Nilas, L.; Pryds, O.; Secher, N.J.; Olsen, S.F.; Halldorsson, T.I. Intake of Sweets, Snacks and Soft Drinks Predicts Weight Gain in Obese Pregnant Women: Detailed Analysis of the Results of a Randomised Controlled Trial. PLoS ONE 2015, 10, e0133041. [Google Scholar] [CrossRef]
- Englund-Ogge, L.; Brantsaeter, A.L.; Haugen, M.; Sengpiel, V.; Khatibi, A.; Myhre, R.; Myking, S.; Meltzer, H.M.; Kacerovsky, M.; Nilsen, R.M.; et al. Association between intake of artificially sweetened and sugar-sweetened beverages and preterm delivery: A large prospective cohort study. Am. J. Clin. Nutr. 2012, 96, 552–559. [Google Scholar] [CrossRef]
- Zhu, Y.; Olsen, S.F.; Mendola, P.; Halldorsson, T.I.; Rawal, S.; Hinkle, S.N.; Yeung, E.H.; Chavarro, J.E.; Grunnet, L.G.; Granstrom, C.; et al. Maternal consumption of artificially sweetened beverages during pregnancy, and offspring growth through 7 years of age: A prospective cohort study. Int. J. Epidemiol. 2017, 46, 1499–1508. [Google Scholar] [CrossRef]
- Nutrition Mother and Baby; In Icelandic Næring Móðir og Barn. Available online: https://nmb.is/ (accessed on 1 April 2019).
- White, S.L.; Lawlor, D.A.; Briley, A.L.; Godfrey, K.M.; Nelson, S.M.; Oteng-Ntim, E.; Robson, S.C.; Sattar, N.; Seed, P.T.; Vieira, M.C.; et al. Early Antenatal Prediction of Gestational Diabetes in Obese Women: Development of Prediction Tools for Targeted Intervention. PLoS ONE 2016, 11, e0167846. [Google Scholar] [CrossRef]
- Torloni, M.R.; Betran, A.P.; Horta, B.L.; Nakamura, M.U.; Atallah, A.N.; Moron, A.F.; Valente, O. Prepregnancy BMI and the risk of gestational diabetes: A systematic review of the literature with meta-analysis. Obes. Rev. 2009, 10, 194–203. [Google Scholar] [CrossRef]
- Bouthoorn, S.H.; Silva, L.M.; Murray, S.E.; Steegers, E.A.; Jaddoe, V.W.; Moll, H.; Hofman, A.; Mackenbach, J.P.; Raat, H. Low-educated women have an increased risk of gestational diabetes mellitus: The Generation R Study. Acta Diabetol. 2015, 52, 445–452. [Google Scholar] [CrossRef]
- England, L.J.; Levine, R.J.; Qian, C.; Soule, L.M.; Schisterman, E.F.; Yu, K.F.; Catalano, P.M. Glucose tolerance and risk of gestational diabetes mellitus in nulliparous women who smoke during pregnancy. Am. J. Epidemiol. 2004, 160, 1205–1213. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Emberson, J.R.; Ebrahim, S.; Whincup, P.H.; Wannamethee, S.G.; Walker, M.; Smith, G.D. Is the association between parity and coronary heart disease due to biological effects of pregnancy or adverse lifestyle risk factors associated with child-rearing? Findings from the British Women’s Heart and Health Study and the British Regional Heart Study. Circulation 2003, 107, 1260–1264. [Google Scholar]
- Donazar-Ezcurra, M.; Lopez-Del Burgo, C.; Martinez-Gonzalez, M.A.; Basterra-Gortari, F.J.; de Irala, J.; Bes-Rastrollo, M. Soft drink consumption and gestational diabetes risk in the SUN project. Clin. Nutr. 2018, 37, 638–645. [Google Scholar] [CrossRef]
- Ruiz-Gracia, T.; Duran, A.; Fuentes, M.; Rubio, M.A.; Runkle, I.; Carrera, E.F.; Torrejon, M.J.; Bordiu, E.; Valle, L.D.; Garcia de la Torre, N.; et al. Lifestyle patterns in early pregnancy linked to gestational diabetes mellitus diagnoses when using IADPSG criteria. The St Carlos gestational study. Clin. Nutr. 2016, 35, 699–705. [Google Scholar] [CrossRef]
- Battaglia Richi, E.; Baumer, B.; Conrad, B.; Darioli, R.; Schmid, A.; Keller, U. Health Risks Associated with Meat Consumption: A Review of Epidemiological Studies. Int. J. Vitam. Nutr. Res. 2015, 85, 70–78. [Google Scholar] [CrossRef]
- Boada, L.D.; Henriquez-Hernandez, L.A.; Luzardo, O.P. The impact of red and processed meat consumption on cancer and other health outcomes: Epidemiological evidences. Food Chem. Toxicol. 2016, 92, 236–244. [Google Scholar] [CrossRef]
- Zhang, Y.; Gong, Y.; Xue, H.; Xiong, J.; Cheng, G. Vitamin D and gestational diabetes mellitus: A systematic review based on data free of Hawthorne effect. BJOG 2018, 125, 784–793. [Google Scholar] [CrossRef]
- Koivusalo, S.B.; Rono, K.; Klemetti, M.M.; Roine, R.P.; Lindstrom, J.; Erkkola, M.; Kaaja, R.J.; Poyhonen Alho, M.; Tiitinen, A.; Huvinen, E.; et al. Gestational Diabetes Mellitus Can Be Prevented by Lifestyle Intervention: The Finnish Gestational Diabetes Prevention Study (RADIEL): A Randomized Controlled Trial. Diabetes Care 2016, 39, 24–30. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- Assaf-Balut, C.; Garcia de la Torre, N.; Duran, A.; Fuentes, M.; Bordiu, E.; Del Valle, L.; Familiar, C.; Valerio, J.; Jimenez, I.; Herraiz, M.A.; et al. A Mediterranean Diet with an Enhanced Consumption of Extra Virgin Olive Oil and Pistachios Improves Pregnancy Outcomes in Women Without Gestational Diabetes Mellitus: A Sub-Analysis of the St. Carlos Gestational Diabetes Mellitus Prevention Study. Ann. Nutr. Metab. 2019, 74, 69–79. [Google Scholar] [CrossRef]
- Chen, L.W.; Aris, I.M.; Bernard, J.Y.; Tint, M.T.; Chia, A.; Colega, M.; Gluckman, P.D.; Shek, L.P.; Saw, S.M.; Chong, Y.S.; et al. Associations of Maternal Dietary Patterns during Pregnancy with Offspring Adiposity from Birth Until 54 Months of Age. Nutrients 2016, 9, 2. [Google Scholar] [CrossRef]
- Brantsaeter, A.L.; Haugen, M.; Samuelsen, S.O.; Torjusen, H.; Trogstad, L.; Alexander, J.; Magnus, P.; Meltzer, H.M. A dietary pattern characterized by high intake of vegetables, fruits, and vegetable oils is associated with reduced risk of preeclampsia in nulliparous pregnant Norwegian women. J. Nutr. 2009, 139, 1162–1168. [Google Scholar] [CrossRef]
- Hillesund, E.R.; Bere, E.; Haugen, M.; Overby, N.C. Development of a New Nordic Diet score and its association with gestational weight gain and fetal growth—A study performed in the Norwegian Mother and Child Cohort Study (MoBa). Public Health Nutr. 2014, 17, 1909–1918. [Google Scholar] [CrossRef]
- Martin, C.L.; Sotres-Alvarez, D.; Siega-Riz, A.M. Maternal Dietary Patterns during the Second Trimester Are Associated with Preterm Birth. J. Nutr. 2015, 145, 1857–1864. [Google Scholar] [CrossRef]
- Wolff, S.; Legarth, J.; Vangsgaard, K.; Toubro, S.; Astrup, A. A randomized trial of the effects of dietary counseling on gestational weight gain and glucose metabolism in obese pregnant women. Int. J. Obes. (Lond.) 2008, 32, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Haby, K.; Glantz, A.; Hanas, R.; Premberg, A. Mighty Mums—An antenatal health care intervention can reduce gestational weight gain in women with obesity. Midwifery 2015, 31, 685–692. [Google Scholar] [CrossRef]
- Rogozinska, E.; Marlin, N.; Jackson, L.; Rayanagoudar, G.; Ruifrok, A.E.; Dodds, J.; Molyneaux, E.; van Poppel, M.N.; Poston, L.; Vinter, C.A.; et al. Effects of antenatal diet and physical activity on maternal and fetal outcomes: Individual patient data meta-analysis and health economic evaluation. Health Technol. Assess. (Winch. Engl.) 2017, 21, 1–158. [Google Scholar] [CrossRef]
- Guo, X.Y.; Shu, J.; Fu, X.H.; Chen, X.P.; Zhang, L.; Ji, M.X.; Liu, X.M.; Yu, T.T.; Sheng, J.Z.; Huang, H.F. Improving the effectiveness of lifestyle interventions for gestational diabetes prevention: A meta-analysis and meta-regression. BJOG 2019, 126, 311–320. [Google Scholar] [CrossRef]

| All a | GDM a,b | No GDM a | p Value c | |
|---|---|---|---|---|
| (n = 1651) | (16%) | (84%) | ||
| Maternal age (year) | 30.3 ± 5.2 | 31.8 ± 5.4 | 30.0 ± 5.1 | <0.01 d |
| Height (cm) | 167.5 ± 6.1 | 166.5 ± 6.3 | 167.7 ± 6.1 | <0.01 d |
| Birth weight (g) | 3670 ± 552 | 3686 ± 587 | 3667± 545 | 0.64 d |
| Gestational age (weeks) | 40.0 (1.0) | 39.0 ± 2.0 | 40.0 ± 2.0 | <0.01 e |
| Pre-pregnancy weight (kg) | 68.0 (20.0) | 85.0 (19.5) | 66.0 (16.0) | <0.01 e |
| Pre-pregnancy BMI (kg/m2) | 24.2 (6.7) | 30.5 (7.6) | 23.5 (5.3) | <0.01 e |
| Pre-pregnancy BMI (groups) | <0.01 f | |||
| <18.5 kg/m2 (%) | 3 | 1 | 4 | |
| 18.5–24.99 kg/m2 (%) | 54 | 17 | 61 | |
| 25–29.99 kg/m2 (%) | 24 | 24 | 23 | |
| ≥30 kg/m2 (%) | 19 | 59 | 11 | |
| Exc. GWG (%) | 36 | 33 | 36 | 0.38 f |
| Parity (%) | <0.01 f | |||
| Nulliparous | 39 | 31 | 41 | |
| Primi/multiparous | 61 | 69 | 59 | |
| Single (%) | 6 | 7 | 5 | 0.34 f |
| Smoking during pregnancy (%) | 6 | 7 | 6 | 0.74 f |
| Family history of type 2 diabetes (%) | 18 | 15 | 39 | <0.01 f |
| Education (%) | <0.01 f | |||
| Elementary schooling | 13 | 18 | 12 | |
| High sch. and technical sch. | 30 | 32 | 29 | |
| University education | 34 | 37 | 34 | |
| Higher academic | 24 | 14 | 26 |
| Risk factors | All (n = 1651) | GDM a (16%) | No GDM (84%) | pb |
|---|---|---|---|---|
| Not eating a varied diet | 21% | 23% | 21% | 0.43 |
| Sugar and artificially sweetened beverages ≥5 times/week | 28% | 37% | 27% | <0.01 |
| Sweet, ice cream, cakes, cookies ≥2.5 times/week | 59% | 63% | 58% | 0.14 |
| Processed meat products ≥1 time/week | 31% | 37% | 30% | 0.04 |
| Whole grain products <2 times/day | 91% | 93% | 91% | 0.26 |
| Dairy <2 times/day | 78% | 81% | 77% | 0.18 |
| Vitamin D intake <5 times/week | 30% | 34% | 29% | 0.12 |
| RR (95% CI) b | |||
|---|---|---|---|
| Cases (%)/n | Crude | Adjusted c | |
| Dichotomized score | |||
| ≤2 scores | 49 (12%)/407 | ref | ref |
| 3 scores | 76 (15%)/503 | 1.26 (0.90, 1.75) | 0.96 (0.72, 1.30) |
| 4 scores | 69 (16%)/439 | 1.31 (0.93, 1.83) | 1.00 (0.74, 1.37) |
| ≥5 scores | 71 (24%)/302 | 1.95 (1.40, 2.72) | 1.38 (1.03, 1.85) |
| p for trend | <0.01 | 0.02 | |
| Stratified analyses, continuous score | |||
| All women | 265 (16%)/1651 | 1.20 (1.10, 1.32) | 1.10 (1.02, 1.20) |
| BMI < 25 kg/m2 d | 51 (5%)/947 | 1.20 (0.96, 1.52) | 1.11 (0.90, 1.36) |
| BMI ≥ 25 kg/m2 d | 214 (30%)/704 | 1.12 (1.02, 1.23) | 1.09 (1.002, 1.19) |
| Control (n = 41) a | Intervention (n = 47) a | p-Value b | |
|---|---|---|---|
| Baseline Characteristics | |||
| Pre-pregnancy BMI (kg/m2) | 28.7 (27.1–31.5) | 29.4 (27.5–35.2) | 0.40 |
| Gestational length at baseline (weeks) | 15.0 ± 2.5 | 14.8 ± 2.7 | 0.83 |
| Age | 0.27 | ||
| 18–24, n (%) | 10 (24) | 10 (21) | |
| 25–34, n (%) | 28 (68) | 28 (60) | |
| ≥35, n (%) | 3 (7) | 9 (19) | |
| Parity | 0.27 | ||
| Nulliparous, n (%) | 13 (32) | 10 (21) | |
| Primi/multiparous, n (%) | 28 (68) | 37 (79) | |
| Smoking during pregnancy, n (%) | 5 (12) | 5 (11) | 0.82 |
| Dietary habits at endpoint c | |||
| Milk and cultured milk products (g/d) | 217 (138–396) | 247 (102–376) | 0.91 |
| Vegetables (g/d) | 91 (23–148) | 101 (57–135) | 0.18 |
| Fruits and berries (g/d) | 105 (73–220) | 150 (70–215) | 0.67 |
| Fish ≥300g/week (%) | 22% | 32% | 0.30 |
| Processed meat (g/d) | 14 (0–42) | 10 (0–25) | 0.69 |
| Soft drinks (g/d) | 125 (25–365) | 75 (0–200) | 0.03 |
| French fries or chips ≥100g/week (%) | 27% | 19% | 0.38 |
| Cakes, biscuits, and/or sweets (g/d) | 62 (19–114) | 37 (18–88) | 0.25 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrolfsdottir, L.; Gunnarsdottir, I.; Birgisdottir, B.E.; Hreidarsdottir, I.T.; Smarason, A.K.; Hardardottir, H.; Halldorsson, T.I. Can a Simple Dietary Screening in Early Pregnancy Identify Dietary Habits Associated with Gestational Diabetes? Nutrients 2019, 11, 1868. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081868
Hrolfsdottir L, Gunnarsdottir I, Birgisdottir BE, Hreidarsdottir IT, Smarason AK, Hardardottir H, Halldorsson TI. Can a Simple Dietary Screening in Early Pregnancy Identify Dietary Habits Associated with Gestational Diabetes? Nutrients. 2019; 11(8):1868. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081868
Chicago/Turabian StyleHrolfsdottir, Laufey, Ingibjorg Gunnarsdottir, Bryndis Eva Birgisdottir, Ingibjorg Th Hreidarsdottir, Alexander Kr. Smarason, Hildur Hardardottir, and Thorhallur I. Halldorsson. 2019. "Can a Simple Dietary Screening in Early Pregnancy Identify Dietary Habits Associated with Gestational Diabetes?" Nutrients 11, no. 8: 1868. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11081868