Food Consumption Patterns and Body Composition in Children: Moderating Effects of Prop Taster Status

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
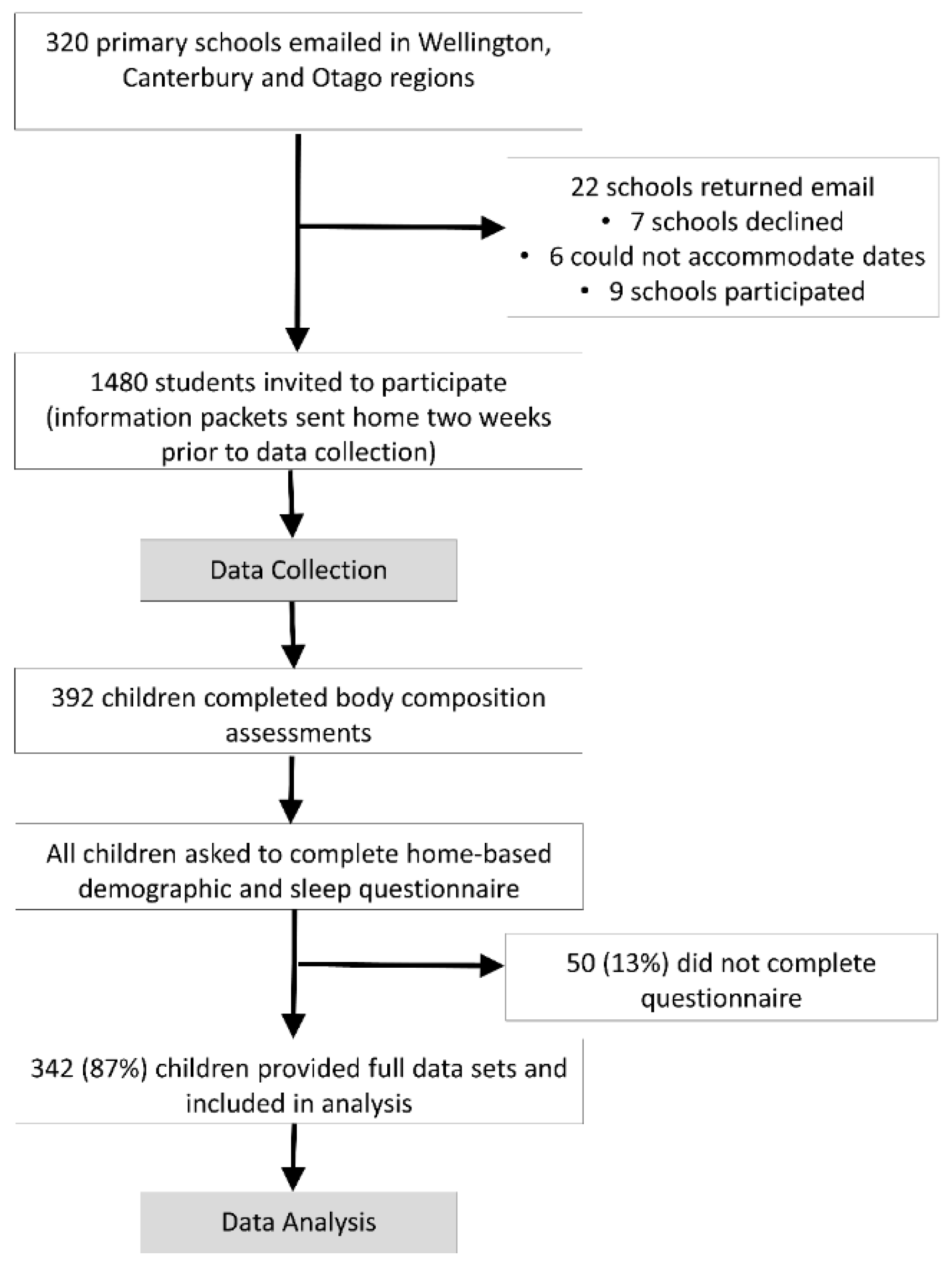
2.1. Participants
2.2. Study Design
2.3. Demographic Data
2.4. Dependent Variables: Body Composition
2.4.1. Body Fat and Fat Mass
2.4.2. Anthropometrics
2.5. Independent Variables: Food Consumption Patterns
2.6. Moderation Variable: Prop Taster Status
2.7. Covariates
Physical Activity
2.8. Statistical Analysis
3. Results
3.1. Participants
3.2. Food Consumption Patterns
3.3. Tasters vs. Non-Tasters
3.4. Associations between Body Composition and Food Types
3.5. Associations between Body Composition and Food Types: Stratified by Prop Taster Status
3.6. Sensitivity Analysis: Sex Interaction
4. Discussion
4.1. Limitations and Strengths
4.2. Associations between Food Patterns and Body Composition
4.3. Moderating Effect of PROP (Taster) Status
4.4. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oftedal, K.N.; Tepper, B.J. Influence of the PROP bitter taste phenotype and eating attitudes on energy intake and weight status in pre-adolescents: A 6-year follow-up study. Physiol. Behav. 2013, 118, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organisation for Economic Cooperation and Development (OCED). Obesity Update 2017. Paris, France. 2017. Available online: http://www.oecd.org/health/obesity-update.htm (accessed on 2 May 2019).
- Minsitry of Health (MOH). Annual Update of Key Results 2017/18. Available online: https://www.health.govt.nz/publication/annual-update-key-results-2017-18-new-zealand-health-survey (accessed on 30 June 2019).
- Livingstone, M.; McCaffrey, T.; Rennie, K.; McCaffrey, T. Childhood obesity prevention studies: Lessons learned and to be learned. Public Health Nutr. 2006, 9, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Specter, S.E. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Mainland, J.D.; Keller, A.; Li, Y.R.; Zhou, T.; Trimmer, C.; Snyder, L.L.; Moberly, A.H.; Adipietro, K.A.; Liu, W.L.; Zhuang, H.; et al. The missense of smell: Functional variability in the human odorant receptor repertoire. Nat. Neurosci. 2014, 17, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Bachmanov, A.A.; Beauchamp, G.K. Taste Receptor Genes. Annu. Rev. Nutr. 2007, 27, 389–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roper, S.D. Signal transduction and information processing in mammalian taste buds. Pflügers Arch. Eur. J. Physiol. 2007, 454, 759–776. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Duffy, V.B.; Miller, I.J. PTC/PROP tasting: Anatomy, psychophysics, and sex effects. Physiol. Behav. 1994, 56, 1165–1171. [Google Scholar] [CrossRef]
- Chang, W.-I.; Chung, J.-W.; Kim, Y.-K.; Chung, S.-C.; Kho, H.-S. The relationship between phenylthiocarbamide (PTC) and 6-n-propylthiouracil (PROP) taster status and taste thresholds for sucrose and quinine. Arch. Oral Biol. 2006, 51, 427–432. [Google Scholar] [CrossRef]
- García-Bailo, B.; Toguri, C.; Eny, K.M.; El-Sohemy, A. Genetic Variation in Taste and Its Influence on Food Selection. OMICS A J. Integr. Biol. 2009, 13, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Anliker, J.A.; Bartoshuk, L.; Ferris, A.M.; Hooks, L.D. Children’s food preferences and genetic sensitivity to the bitter taste of 6-n-propylthiouracil (PROP). Am. J. Clin. Nutr. 1991, 54, 316–320. [Google Scholar] [CrossRef]
- Keller, K.L.; Steinmann, L.; Nurse, R.J.; Tepper, B.J. Genetic taste sensitivity to 6-n-propylthiouracil influences food preference and reported intake in preschool children. Appetite 2002, 38, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.L.; Tepper, B.J. Inherited Taste Sensitivity to 6-n-Propylthiouracil in Diet and Body Weight in Children. Obes. Res. 2004, 12, 904–912. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.A.; Feeney, E.L.; Scannell, A.G.; Markey, A.; Gibney, E.R. Bitter Taste Perception and Dietary Intake Patterns in Irish Children. J. Nutr. Nutr. 2013, 6, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, J.C.; Cardinal, T.M.; Sitto, J.R.; Kannan, S. Ability to taste 6-n-propylthiouracil and BMI in low-income preschool-aged children. Obesity 2008, 16, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.I.; Tepper, B.J. Short-term vegetable intake by young children classified by 6-n-propylthoiuracil bitter-taste phenotype. Am. J. Clin. Nutr. 2006, 84, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Mennella, J.A.; Hughes, S.O.; Liu, Y.; Mendoza, P.M.; Patrick, H. Offering “Dip” Promotes Intake of a Moderately-Liked Raw Vegetable among Preschoolers with Genetic Sensitivity to Bitterness. J. Acad. Nutr. Diet. 2012, 112, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Feeney, E.; O’Brien, S.; Scannell, A.; Markey, A.; Gibney, E.R. Genetic variation in taste perception: Does it have a role in healthy eating? Proc. Nutr. Soc. 2011, 70, 135–143. [Google Scholar] [CrossRef]
- Baranowski, J.C.; Baranowski, T.; Beltran, A.; Watson, K.B.; Jago, R.; Callie, M.; Missaghian, M.; Tepper, B.J. 6-n-Propylthiouracil sensitivity and obesity status among ethnically diverse children. Public Health Nutr. 2010, 13, 1587–1592. [Google Scholar] [CrossRef]
- Burd, C.; Senerat, A.; Chambers, E.; Keller, K.L. PROP taster status interacts with the built environment to influence children’s food acceptance and body weight status. Obesity (Silver Spring) 2013, 21, 786–794. [Google Scholar] [CrossRef]
- Bouthoorn, S.H.; Van Lenthe, F.J.; Kiefte-De Jong, J.C.; Taal, H.R.; Wijtzes, A.I.; Hofman, A.; Jaddoe, V.W.; Glymour, M.M.; Rivadeneira, F.; Raat, H. Genetic taste blindness to bitter and body composition in childhood: A Mendelian randomization design. Int. J. Obes. 2014, 38, 1005–1010. [Google Scholar] [CrossRef]
- Goldstein, G.L.; Daun, H.; Tepper, B.J. Influence of PROP taster status and maternal variables on energy intake and body weight of pre-adolescents. Physiol. Behav. 2007, 90, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Skeaff, S.A.; Wong, J.E.; Skidmore, P.M.L. Reproducibility and Relative Validity of a Short Food Frequency Questionnaire in 9–10 Year-Old Children. Nutrients 2016, 8, 271. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Castro, N.; Faulkner, J.; Skidmore, P.; Williams, M.; Lambrick, D.M.; Signal, L.; Thunders, M.; Muller, D.; Lark, S.; Hamlin, M.; et al. Pre-Adolescent Cardio-Metabolic Associations and Correlates: PACMAC methodology and study protocol. BMJ Open 2014, 4, e005815. [Google Scholar] [CrossRef] [PubMed]
- Zamora Salas, J.D.; Laclé-Murray, A. Predictive validity of body fat percentage by bioimpedance compared with deuterium oxide dilution in Costa Rican schoolchildren. Am. J. Hum. Biol. 2017, 29. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Davison, B.; Saeedi, P.; Black, K.; Harrex, H.; Haszard, J.; Meredith-Jones, K.; Quigg, R.; Skeaff, S.; Stoner, L.; Wong, J.E.; et al. The Association between Parent Diet Quality and Child Dietary Patterns in Nine- to Eleven-Year-Old Children from Dunedin, New Zealand. Nutrients 2017, 9, 483. [Google Scholar] [CrossRef]
- Corder, K.; Van Sluijs, E.M.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef]
- The Jamovi Project. Jamovi (Version 0.9) [Computer Software). 2019. Available online: https://www.jamovi.org (accessed on 2 May 2019).
- Statistics New Zealand. 2013 Census Quickstats about Culture and Identity. 2014. Available online: http://www.stats.govt.nz/Census/2013-census/%0Aprofile-and-summary-reports/quickstats-culture-identity.aspx (accessed on 2 May 2019).
- Pinto, A.; Cristina, A.; Lopes, C.; Oliveira, A. Dietary patterns at 7 year-old and their association with cardiometabolic health at 10 year-old. Clin. Nutr. 2019. [Google Scholar] [CrossRef]
- Costa, C.S.; Rauber, F.; Leffa, P.S.; Sangalli, C.N.; Campagnolo, P.D.B.; Vitolo, M.R. Nutrition, Metabolism & Cardiovascular Diseases Ultra-processed food consumption and its effects on anthropometric and glucose pro fi le: A longitudinal study during childhood. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 177–184. [Google Scholar] [PubMed]
- Nilsen, B.B.; Yngve, A.; Monteagudo, C.; Tellström, R.; Scander, H.; Werner, B. Reported habitual intake of breakfast and selected foods in relation to overweight status among seven-to nine-year-old Swedish children. Scand. J. Public Health 2017, 45, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh-Taskar, P.R.; Nicklas, T.A.; O’Neil, C.E.; Keast, D.R.; Radcliffe, J.D.; Cho, S. The relationship of breakfast skipping and type of breakfast consumption with nutrient intake and weight status in children and adolescents: The National Health and Nutrition Examination Survey 1999–2006. J. Am. Diet. Assoc. 2010, 110, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Traub, M.; Lauer, R.; Kesztyüs, T.; Steinacker, JM. Skipping breakfast is detrimental for primary school children: Cross-sectional analysis of determinants for targeted prevention. BMC Public Health 2017, 17, 258. [Google Scholar] [CrossRef] [PubMed]
- De la Hunty, A.; Gibson, S.; Ashwell, M. Does regular breakfast cereal consumption help children and adolescents stay slimmer? A systematic review and meta-analysis. Obes. Facts 2013, 6, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef]
- Keller, K.L.; Adise, S. Variation in the Ability to Taste Bitter Thiourea Compounds: Implications for Food Acceptance, Dietary Intake, and Obesity Risk in Children. Annu. Rev. Nutr. 2016, 36, 157–182. [Google Scholar] [CrossRef]


{kind=link}
| All | Tasters | Non-Tasters | ||||||
|---|---|---|---|---|---|---|---|---|
| Categorical Variables | n (%) | n (%) | n (%) | P | ||||
| n | 342 | (100) | 140 | (41) | 202 | (144) | ||
| Female | 169 | (49) | 73 | (52) | 96 | (48) | 0.401 | |
| Ethnicity | ||||||||
| New Zealand European | 278 | (81) | 114 | (81) | 164 | (81) | 0.250 | |
| Māori | 37 | (11) | 11 | (8) | 26 | (13) | ||
| Pacific | 22 | (6) | 12 | (9) | 10 | (5) | ||
| Not Recorded | 5 | (2) | 3 | (2) | 2 | (1) | ||
| School Year/Grade | ||||||||
| 4 | 72 | (21) | 24 | (17) | 48 | (24) | 0.521 | |
| 5 | 96 | (28) | 41 | (29) | 55 | (27) | ||
| 6 | 111 | (33) | 47 | (34) | 64 | (32) | ||
| 7 | 63 | (18) | 28 | (20) | 35 | (17) | ||
| School Decile | ||||||||
| Low (≤5) | 174 | (51) | 58 | (41) | 116 | (57) | 0.004 | |
| High (>5) | 168 | (49) | 82 | (59) | 86 | (43) | ||
| Obesity status | ||||||||
| Overweight/Obese | 99 | (29) | 38 | (27) | 61 | (30) | 0.540 | |
| Non-Overweight | 243 | (71) | 102 | (73) | 141 | (70) | ||
| Continuous variables | Mean (SD) | Mean (SD) | Mean (SD) | P | ES | |||
| Age (years) | 9.56 | (1.12) | 9.64 | (1.05) | 9.50 | (1.17) | 0.248 | 0.13 |
| Body Fat (%) | 19.8 | (9.40) | 20.2 | (9.82) | 19.6 | (9.12) | 0.589 | 0.06 |
| Fat Mass (Kg) | 7.18 | (5.08) | 7.43 | (5.57) | 7.01 | (4.71) | 0.445 | 0.08 |
| Fat Mass Index (kg/m2) | 3.68 | (2.37) | 3.75 | (2.53) | 3.63 | (2.26) | 0.653 | 0.05 |
| Body Mass Index (kg/m2) | 0.41 | (1.18) | 0.34 | (1.23) | 0.45 | (1.15) | 0.426 | −0.09 |
| Waist to Height Ratio (W:Ht) | 0.44 | (0.05) | 0.43 | (0.05) | 0.44 | (0.05) | 0.366 | −0.10 |
| Physical Activity (mins) | 165 | (135) | 143 | (116) | 180 | (146) | 0.015 | −0.27 |
| Processed Foods | 0.00 | (1.24) | 0.08 | (2.06) | −0.06 | (1.69) | 0.487 | 0.08 |
| Fruit/Veg | 0.00 | (1.56) | −0.02 | (1.51) | 0.01 | (1.60) | 0.881 | −0.02 |
| Breakfast Foods | 0.00 | (1.85) | 0.09 | (1.21) | −0.06 | (1.26) | 0.266 | 0.12 |
| Factor 1 | Factor 2 | Factor 3 | |
|---|---|---|---|
| Food Items/Group | Processed Food | Fruit/Veg | Breakfast Food |
| Fruits | −0.02 | 0.41 | −0.02 |
| Vegetables | −0.01 | 0.45 | −0.02 |
| Trim milk | 0.01 | 0.22 | −0.45 |
| Milk | 0.11 | 0.07 | 0.54 |
| Cheese | 0.04 | 0.27 | 0.32 |
| Yoghurt | 0.19 | 0.27 | −0.02 |
| Ice cream | 0.24 | −0.07 | −0.06 |
| Processed meat | 0.29 | 0.13 | −0.06 |
| Other meats | 0.25 | 0.21 | −0.06 |
| Fish | 0.27 | 0.04 | −0.16 |
| Nondairy drinks | 0.31 | −0.18 | −0.05 |
| Breakfast cereals | 0.17 | 0.18 | 0.25 |
| White bread | 0.30 | −0.19 | 0.03 |
| Brown/Wholemeal bread | −0.12 | 0.37 | 0.09 |
| Rice, rice-based dishes | 0.25 | 0.02 | −0.29 |
| Pasta, noodles | 0.24 | 0.16 | −0.31 |
| Salty snacks | 0.25 | −0.13 | 0.03 |
| Biscuits, cakes, muffins, doughnuts, fruit pies | 0.12 | 0.15 | 0.25 |
| Lollies (candies/sweets) | 0.24 | −0.19 | 0.16 |
| Sweet snacks | 0.33 | −0.08 | 0.13 |
| Spreads | 0.28 | 0.11 | 0.08 |
| Eigenvalue | 3.5 | 2.4 | 1.5 |
| Variance explained (%) | 17 | 11 | 7 |
| Cumulative Variance (% | 17 | 28 | 35 |
| Univariate | Multivariate | Multivariate (adjusted) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | LCI | UCI | P | ES | β | LCI | UCI | P | ES | β | LCI | UCI | P | ES | |
| Body Fat (%) | |||||||||||||||
| Processed | 0.616 | 0.077 | 1.150 | 0.025 | 0.121 | 0.785 | 0.253 | 1.317 | 0.004 | 0.154 | 0.647 | 0.128 | 1.167 | 0.015 | 0.130 |
| Fruit/Veg | −0.780 | −1.420 | −0.144 | 0.016 | −0.130 | −0.824 | −1.448 | −0.200 | 0.010 | −0.137 | −0.419 | −1.040 | 0.200 | 0.184 | −0.070 |
| Breakfast | −1.220 | −2.020 | −0.422 | 0.003 | −0.161 | −1.352 | −2.143 | −0.561 | <0 .001 | −0.178 | −1.440 | −2.204 | −0.679 | <0.001 | −0.192 |
| Fat Mass (kg) | |||||||||||||||
| Processed | 0.473 | 0.185 | 0.762 | 0.001 | 0.172 | 0.561 | 0.275 | 0.846 | < 0.001 | 0.204 | 0.416 | 0.137 | 0.695 | 0.004 | 0.153 |
| Fruit/Veg | −0.418 | −0.761 | −0.074 | 0.017 | −0.129 | −0.454 | −0.789 | −0.119 | 0.008 | −0.140 | −0.260 | −0.594 | 0.073 | 0.125 | −0.080 |
| Breakfast | −0.581 | −1.010 | −0.149 | 0.009 | −0.142 | −0.679 | −1.104 | −0.255 | 0.002 | −0.166 | −0.729 | −1.138 | −0.319 | <0.001 | −0.178 |
| Fat Mass Index (kg/m2) | |||||||||||||||
| Processed | 0.178 | 0.042 | 0.313 | 0.010 | 0.139 | 0.220 | 0.087 | 0.354 | 0.001 | 0.172 | 0.163 | 0.031 | 0.295 | 0.016 | 0.129 |
| Fruit/Veg | −0.238 | −0.397 | −0.078 | 0.004 | −0.157 | −0.251 | −0.408 | −0.095 | 0.002 | −0.166 | −0.146 | −0.304 | 0.011 | 0.069 | −0.096 |
| Breakfast | −0.274 | −0.475 | −0.072 | 0.008 | −0.143 | −0.310 | −0.509 | −0.112 | 0.002 | −0.162 | −0.333 | −0.527 | −0.140 | <0.001 | −0.175 |
| Body Mass Index (kg/m2) | |||||||||||||||
| Processed | 0.039 | −0.029 | 0.107 | 0.264 | 0.061 | 0.054 | −0.014 | 0.122 | 0.117 | 0.085 | 0.018 | −0.050 | 0.085 | 0.602 | 0.019 |
| Fruit/Veg | −0.114 | −0.194 | −0.034 | 0.005 | −0.151 | −0.117 | −0.197 | −0.037 | 0.004 | −0.155 | −0.067 | −0.147 | 0.014 | 0.105 | −0.098 |
| Breakfast | −0.088 | −0.189 | 0.014 | 0.090 | −0.092 | −0.095 | −0.196 | 0.006 | 0.065 | −0.100 | −0.106 | −0.205 | −0.007 | 0.037 | −0.095 |
| Waist: Height | |||||||||||||||
| Processed | 0.001 | −0.002 | 0.004 | 0.454 | 0.041 | 0.002 | −0.001 | 0.005 | 0.230 | 0.065 | 0.000 | −0.002 | 0.003 | 0.577 | 0.031 |
| Fruit/Veg | −0.006 | −0.009 | −0.002 | 0.001 | −0.177 | −0.006 | −0.009 | −0.002 | < 0.001 | −0.180 | −0.004 | −0.007 | 0.000 | 0.025 | −0.124 |
| Breakfast | −0.003 | −0.007 | 0.001 | 0.137 | −0.081 | −0.003 | −0.008 | 0.001 | 0.113 | −0.085 | −0.004 | −0.009 | 0.000 | 0.035 | −0.114 |
| Tasters (n = 140) | Non-Tasters (n = 202) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | LCI | UCI | P | ES | β | LCI | UCI | P | ES | |
| Body Fat (%) | ||||||||||
| Processed | 0.878 | 0.087 | 1.669 | 0.030 | 0.184 | 0.317 | −0.413 | 1.048 | 0.392 | 0.061 |
| Fruit/Veg | −0.515 | −1.626 | 0.597 | 0.361 | −0.079 | −0.362 | −1.138 | 0.413 | 0.358 | −0.065 |
| Breakfast | −0.999 | −2.293 | 0.295 | 0.129 | −0.123 | −1.503 | −2.488 | −0.518 | 0.003 | −0.211 |
| Fat Mass (kg) | ||||||||||
| Processed | 0.753 | 0.314 | 1.193 | < 0.001 | 0.279 | 0.008 | −0.362 | 0.378 | 0.966 | 0.003 |
| Fruit/Veg | −0.221 | −0.839 | 0.397 | 0.481 | −0.060 | −0.279 | −0.671 | 0.114 | 0.163 | −0.095 |
| Breakfast | −0.433 | −1.152 | 0.287 | 0.236 | −0.094 | −0.783 | −1.282 | −0.285 | 0.002 | −0.209 |
| Fat Mass Index (kg/m2) | ||||||||||
| Processed | 0.258 | 0.052 | 0.464 | 0.014 | 0.211 | 0.042 | −0.139 | 0.223 | 0.647 | 0.032 |
| Fruit/Veg | −0.135 | −0.424 | 0.154 | 0.357 | −0.080 | −0.149 | −0.341 | 0.043 | 0.126 | −0.107 |
| Breakfast | −0.206 | −0.542 | 0.131 | 0.228 | −0.099 | −0.361 | −0.604 | −0.117 | 0.004 | −0.203 |
| Body Mass Index (kg/m2) | ||||||||||
| Processed | 0.069 | −0.035 | 0.173 | 0.193 | 0.116 | −0.035 | −0.130 | 0.060 | 0.473 | −0.052 |
| Fruit/Veg | −0.063 | −0.209 | 0.084 | 0.399 | −0.077 | −0.068 | −0.169 | 0.033 | 0.187 | −0.095 |
| Breakfast | −0.034 | −0.204 | 0.136 | 0.692 | −0.034 | −0.131 | −0.259 | −0.003 | 0.045 | −0.144 |
| Waist: Height | ||||||||||
| Processed | 0.002 | −0.003 | 0.006 | 0.411 | 0.075 | −0.000 | −0.004 | 0.004 | 0.941 | −0.005 |
| Fruit/Veg | −0.003 | −0.009 | 0.003 | 0.333 | −0.090 | −0.004 | −0.008 | 0.000 | 0.056 | −0.139 |
| Breakfast | −0.003 | −0.010 | 0.004 | 0.426 | −0.070 | −0.004 | −0.010 | 0.001 | 0.112 | −0.115 |
| Female (n = 106) - Male (n = 96) | |||||
|---|---|---|---|---|---|
| β | LCI | UCI | P | ES | |
| Body Fat (%) | −2.233 | −4.222 | −0.243 | 0.028 | −0.124 |
| Fat Mass (kg) | −1.105 | −2.119 | −0.098 | 0.032 | −0.376 |
| Fat Mass Index (kg/m2) | −0.553 | −1.045 | −0.062 | 0.028 | −0.395 |
| Body Mass Index (kg/m2) | −0.188 | −0.448 | 0.073 | 0.156 | −0.263 |
| Waist: Height | −0.007 | −0.017 | 0.004 | 0.227 | −0.080 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoner, L.; Castro, N.; Kucharska-Newton, A.; Smith-Ryan, A.E.; Lark, S.; Williams, M.A.; Faulkner, J.; Skidmore, P. Food Consumption Patterns and Body Composition in Children: Moderating Effects of Prop Taster Status. Nutrients 2019, 11, 2037. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092037
Stoner L, Castro N, Kucharska-Newton A, Smith-Ryan AE, Lark S, Williams MA, Faulkner J, Skidmore P. Food Consumption Patterns and Body Composition in Children: Moderating Effects of Prop Taster Status. Nutrients. 2019; 11(9):2037. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092037
Chicago/Turabian StyleStoner, Lee, Nicholas Castro, Anna Kucharska-Newton, Abbie E. Smith-Ryan, Sally Lark, Michelle A. Williams, James Faulkner, and Paula Skidmore. 2019. "Food Consumption Patterns and Body Composition in Children: Moderating Effects of Prop Taster Status" Nutrients 11, no. 9: 2037. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092037