Energy Balance and Active Lifestyle: Potential Mediators of Health and Quality of Life Perception in Aging

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Anthropometric Measurements
2.4. Steps and Total Energy Expenditure
2.5. Energy Intake
2.6. Body Image Dissatisfaction
2.7. Health and Quality of Life Perception
2.8. Statistical Analysis
3. Results
3.1. Preliminary Analysis
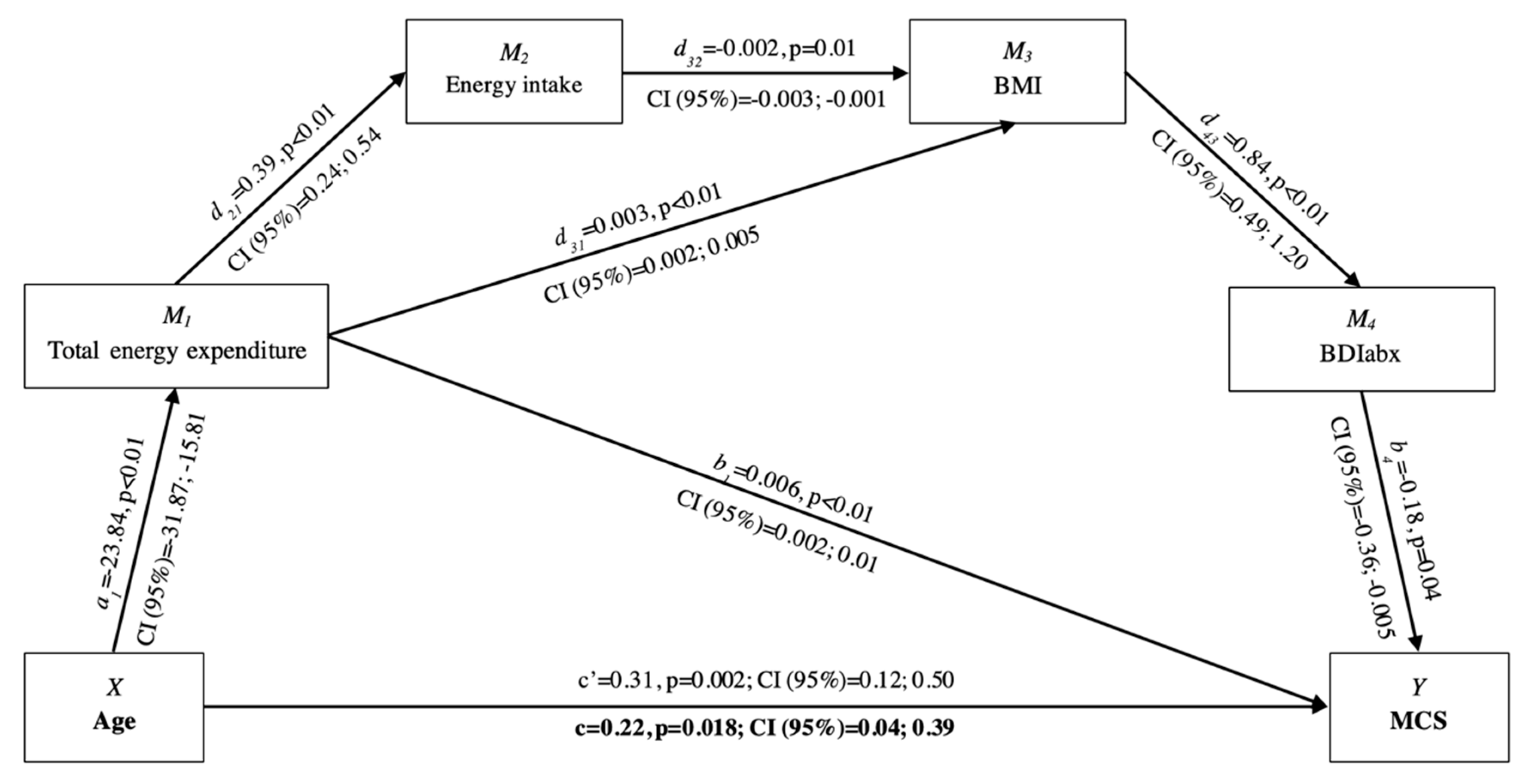
3.2. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 25 January 2019).
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; De Bourdeaudhuij, I.; et al. Determinants of diet and physical activity (DEDIPAC): A summary of findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 150. [Google Scholar] [CrossRef] [PubMed]
- Leone, L.; Pesce, C. From delivery to adoption of physical activity guidelines: Realist synthesis. Int. J. Environ. Res. Public Health 2017, 14, 1193. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://www.who.int/ncds/prevention/physical-activity/global-action-plan-2018-2030/en/ (accessed on 25 January 2019).
- Spirduso, W.W.; Francis, K.L.; MacRae, P.G. Physical Dimensions of Aging, 2nd ed.; Human Kinetics: Champain, IL, USA, 2005. [Google Scholar]
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://www.who.int/ageing/events/world-report-2015-launch/en/ (accessed on 10 August 2019).
- Layte, R.; Sexton, E.; Savva, G. Quality of life in older age: Evidence from an Irish cohort study. J. Am. Geriatr. Soc. 2013, 61, S299–S305. [Google Scholar] [CrossRef] [PubMed]
- Raggi, A.; Corso, B.; Minicuci, N.; Quintas, R.; Sattin, D.; De Torres, L.; Chatterji, S.; Frisoni, G.B.; Haro, J.M.; Koskinen, S.; et al. Determinants of quality of life in ageing populations: Results from a cross-sectional study in Finland, Poland and Spain. PLoS ONE 2016, 11, e0159293. [Google Scholar] [CrossRef] [PubMed]
- Eisele, M.; Kaduszkiewicz, H.; König, H.-H.; Lange, C.; Wiese, B.; Prokein, J.; Weyerer, S.; Werle, J.; Riedel-Heller, S.G.; Luppa, M.; et al. Determinants of health-related quality of life in older primary care patients: Results of the longitudinal observational AgeCoDe study. Br. J. Gen. Pract. 2015, 65, e716–e723. [Google Scholar] [CrossRef]
- Amarantos, E.; Martinez, A.; Dwyer, J. Nutrition and quality of life in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Rejeski, W.J.; Mihalko, S.L. Physical activity and quality of life in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 23–35. [Google Scholar] [CrossRef]
- Manini, T.M. Energy expenditure and aging. Ageing Res. Rev. 2010, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tooze, J.A.; Schoeller, D.A.; Subar, A.F.; Kipnis, V.; Schatzkin, A.; Troiano, R.P. Total daily energy expenditure among middle-aged men and women: The OPEN Study. Am. J. Clin. Nutr. 2007, 86, 382–387. [Google Scholar] [CrossRef]
- Lührmann, P.; Bender, R.; Edelmann-Schäfer, B.; Neuhäuser-Berthold, M. Longitudinal changes in energy expenditure in an elderly German population: A 12-year follow-up. Eur. J. Clin. Nutr. 2009, 63, 986–992. [Google Scholar] [CrossRef]
- Elia, M.; Ritz, P.; Stubbs, R.J. Total energy expenditure in the elderly. Eur. J. Clin. Nutr. 2000, 54, S92–S103. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; et al. Energy intake, profile, and dietary sources in the Spanish population: Findings of the ANIBES study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, R.; Kato, Y.; Nishita, Y.; Tange, C.; Tomida, M.; Nakamoto, M.; Imai, T.; Ando, F.; Shimokata, H. Age-related changes in energy intake and weight in community-dwelling middle-aged and elderly Japanese. J. Nutr. Health Aging 2016, 20, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Giezenaar, C.; Chapman, I.; Luscombe-Marsh, N.; Feinle-Bisset, C.; Horowitz, M.; Soenen, S. Ageing is associated with decreases in appetite and energy intake—a meta-analysis in healthy adults. Nutrients 2016, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Shroff, H.P.; Calogero, R.M.; Thompson, J.K. Assessment of body image. In Handbook of Assessment Methods for Eating Behaviors and Weight-Related Problems: Measures, Theory, and Research; Allison, D.B., Allison, D.B., Baskin, M.L., Eds.; Sage: Thousand Oaks, CA, USA, 2009; pp. 115–136. [Google Scholar]
- Tiggemann, M. Body image across the adult life span: Stability and change. Body Image 2004, 1, 29–41. [Google Scholar] [CrossRef]
- Jankowski, G.S.; Diedrichs, P.C.; Williamson, H.; Christopher, G.; Harcourt, D. Looking age-appropriate while growing old gracefully: A qualitative study of ageing and body image among older adults. J. Health Psychol. 2016, 21, 550–561. [Google Scholar] [CrossRef] [PubMed]
- Hausenblas, H.A.; Fallon, E.A. Exercise and body image: A meta-analysis. Psychol. Health 2006, 21, 33–47. [Google Scholar] [CrossRef]
- Borg, C.; Fagerström, C.; Balducci, C.; Burholt, V.; Ferring, D.; Weber, G.; Wenger, C.; Holst, G.; Hallberg, I.R. Life satisfaction in 6 European countries: The relationship to health, self-esteem, and social and financial resources among people (Aged 65–89) with reduced functional capacity. Geriatr. Nurs. 2008, 29, 48–57. [Google Scholar] [CrossRef]
- Svantesson, U.; Jones, J.; Wolbert, K.; Alricsson, M. Impact of physical activity on the self-perceived quality of life in non-frail older adults. J. Clin. Med. Res. 2015, 7, 585–593. [Google Scholar] [CrossRef]
- Mura, G.; Carta, M.G. Physical activity in depressed elderly. A systematic review. Clin. Pract. Epidemiol. Ment. Health 2013, 9, 125–135. [Google Scholar] [CrossRef]
- Prakash, R.S.; Voss, M.W.; Erickson, K.I.; Kramer, A.F. Physical activity and cognitive vitality. Annu. Rev. Psychol. 2015, 66, 769–797. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Haboubi, N. Assessment and management of nutrition in older people and its importance to health. Clin. Interv. Aging 2010, 5, 207–216. [Google Scholar] [Green Version]
- Condello, G.; Ling, F.C.M.; Bianco, A.; Chastin, S.; Cardon, G.; Ciarapica, D.; Conte, D.; Cortis, C.; De Craemer, M.; Di Blasio, A.; et al. Using concept mapping in the development of the EU-PAD framework (EUropean-Physical Activity Determinants across the life course): A DEDIPAC-study. BMC Public Health 2016, 16, 1145. [Google Scholar] [CrossRef] [PubMed]
- Aleksovska, K.; Puggina, A.; Giraldi, L.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Colotto, M.; et al. Biological determinants of physical activity across the life course: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. Sports Med. Open 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Cortis, C.; Puggina, A.; Pesce, C.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; et al. Psychological determinants of physical activity across the life course: A “DEterminants of DIet and Physical ACtivity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182709. [Google Scholar] [CrossRef] [PubMed]
- Condello, G.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; Coppinger, T.; et al. Behavioral determinants of physical activity across the life course: A “DEterminants of DIet and Physical ACtivity” (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, L.; Steinbrecher, A.; Luzak, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; et al. Socio-cultural determinants of physical activity across the life course: A ‘Determinants of Diet and Physical Activity’(DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 173. [Google Scholar] [CrossRef] [PubMed]
- O’Donoghue, G.; Kennedy, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Ciarapica, D.; Colotto, M.; et al. Socio-economic determinants of physical activity across the life course: A” DEterminants of DIet and Physical ACtivity” (DEDIPAC) umbrella literature review. PLoS ONE 2018, 13, e0190737. [Google Scholar] [CrossRef] [PubMed]
- Carlin, A.; Perchoux, C.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Chantal, S.; Ciarapica, D.; Condello, G.; et al. A life course examination of the physical environmental determinants of physical activity behaviour: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182083. [Google Scholar] [CrossRef]
- Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Condello, G.; Coppinger, T.; et al. Policy determinants of physical activity across the life course: A ‘DEDIPAC’umbrella systematic literature review. Eur. J. Public Health 2017, 28, 105–118. [Google Scholar] [CrossRef]
- Condello, G.; Capranica, L.; Stager, J.; Forte, R.; Falbo, S.; Di Baldassarre, A.; Segura-Garcia, C.; Pesce, C. Physical activity and health perception in aging: Do body mass and satisfaction matter? A three-path mediated link. PLoS ONE 2016, 11, e0160805. [Google Scholar] [CrossRef] [PubMed]
- Pétré, B.; Scheen, A.J.; Ziegler, O.; Donneau, A.-F.; Dardenne, N.; Husson, E.; Albert, A.; Guillaume, M. Body image discrepancy and subjective norm as mediators and moderators of the relationship between body mass index and quality of life. Patient Prefer. Adherence 2016, 10, 2261–2270. [Google Scholar] [CrossRef]
- Osness, W.; Adrian, M.; Clark, B.; Hoeger, W.; Raab, D.; Wiswell, R. Functional Fitness Assessment for Adults Over 60 Years: The American Alliance for Health, Physical Education, Recreation and Dance; Reston: New York, NY, USA, 1990. [Google Scholar]
- World Health Organization. Global strategy on Diet, Physical Activity, and Health. 2011. Available online: http://www.who.int/dietphysicalactivity/factsheet_olderadults/en 2011 (accessed on 25 January 2019).
- Mackey, D.C.; Manini, T.M.; Schoeller, D.A.; Koster, A.; Glynn, N.W.; Goodpaster, B.H.; Satterfield, S.; Newman, A.B.; Harris, T.B.; Cummings, S.R. Validation of an armband to measure daily energy expenditure in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Di Blasio, A.; Napolitano, G.; Di Donato, F.; Izzicupo, P.; Di Baldassarre, A.; Modestini, E.; Bergamin, M.; Bullo, V.; Bucci, I.; Di Pietro, M. Analysis of female physical activity characteristics according to age and ponderal status in a free-living context: A study from a central Italy sample. Sport Sci. Health 2016, 12, 453–462. [Google Scholar] [CrossRef]
- Scheers, T.; Philippaerts, R.; Lefevre, J. Variability in physical activity patterns as measured by the SenseWear Armband: How many days are needed? Eur. J. Appl. Physiol. 2012, 112, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Bingham, S.A.; Gill, C.; Welch, A.; Cassidy, A.; Runswick, S.A.; Oakes, S.; Lubin, R.; Thurnham, D.I.; Key, T.; Roe, L.; et al. Validation of dietary assessment methods in the UK arm of EPIC using weighed records, and 24-h urinary nitrogen and potassium and serum vitamin C and carotenoids as biomarkers. Int. J. Epidemiol. 1997, 26, S137–S151. [Google Scholar] [CrossRef]
- Brunner, E.; Juneja, M.; Marmot, M. Dietary assessment in Whitehall II: Comparison of 7 d diet diary and food-frequency questionnaire and validity against biomarkers. Br. J. Nutr. 2001, 86, 405–414. [Google Scholar] [CrossRef]
- Davey, G.K.; Spencer, E.A.; Appleby, P.N.; Allen, N.E.; Knox, K.H.; Key, T.J. EPIC–Oxford: Lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK. Public Health Nutr. 2003, 6, 259–268. [Google Scholar] [CrossRef]
- Leclercq, C.; Arcella, D.; Piccinelli, R.; Sette, S.; Le Donne, C.; Turrini, A. INRAN-SCAI 2005-06 Study Group. The Italian National Food Consumption Survey INRAN-SCAI 2005-06: Main results in terms of food consumption. Public Health Nutr. 2009, 12, 2504–2532. [Google Scholar] [CrossRef]
- Segura-García, C.; Papaianni, M.; Rizza, P.; Flora, S.; De Fazio, P. The development and validation of the Body Image Dimensional Assessment (BIDA). Eat. Weight Disord. 2012, 17, e219–e225. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Keller, S. How to Score the SF-12 Physical and Mental Health Summary Scales; Quality Metric. Inc.: Lincoln, RI, USA, 1998. [Google Scholar]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- König, H.-H.; Heider, D.; Lehnert, T.; Riedel-Heller, S.G.; Angermeyer, M.C.; Matschinger, H.; Vilagut, G.; Bruffaerts, R.; Haro, J.M.; de Girolamo, G.; et al. Health status of the advanced elderly in six European countries: Results from a representative survey using EQ-5D and SF-12. Health Qual. Life Outcomes 2010, 8, 143. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Pannemans, D.L.; Westerterp, K.R. Energy expenditure, physical activity and basal metabolic rate of elderly subjects. Br. J. Nutr. 1995, 73, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Madden, K.M.; Ashe, M.C.; Chase, J.M. Activity profile and energy expenditure among active older Adults, British Columbia, 2011–2012. Prev. Chronic Dis. 2015, 12, E112. [Google Scholar] [CrossRef] [PubMed]
- Hurree, N.; Jeewon, R. An analysis of contributors to energy intake among middle aged and elderly adults. Curr. Res. Nutr. Food Sci. 2016, 4, 8–18. [Google Scholar] [CrossRef]
- Thomas, M.L.; Kaufmann, C.N.; Palmer, B.W.; Depp, C.A.; Martin, A.S.; Glorioso, D.K.; Thompson, W.K.; Jeste, D.V. Paradoxical trend for improvement in mental health with aging: A community-based study of 1546 adults aged 21–100 years. J. Clin. Psychiatry 2016, 77, e1019–e1025. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Gnardellis, C.; Lagiou, A.; Benetou, V.; Trichopoulos, D. Body mass index in relation to energy intake and expenditure among adults in Greece. Epidemiology 2000, 11, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, A.L.; Heitmann, B.; Kyvik, K.O.; Sørensen, T.I. Associations between dietary intake and body fat independent of genetic and familial environmental background. Int. J. Obes. (Lond.) 2010, 34, 892–898. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [CrossRef]
- Moon, K.; Krems, C.; Heuer, T.; Roth, A.; Hoffmann, I. Predictors of BMI vary along the BMI range of German adults-Results of the German National Nutrition Survey II. Obes. Facts 2017, 10, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, K.; Campbell, M.K.; Choi, Y.-H.; Sarma, S. The relationship between diet quality and adult obesity: Evidence from Canada. J. Am. Coll. Nutr. 2014, 33, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Hollis, J.H. Associations between eating frequency and energy intake, energy density, diet quality and body weight status in adults from the USA. Br. J. Nutr. 2016, 115, 2138–2144. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Body Mass (kg) | Height (m) | BMI (kg·m−2) | Medications (n) | Diseases (n) | |
|---|---|---|---|---|---|
| Physical activity level | |||||
| Senior athletes | 69.4 ± 10.2 | 1.67 ± 0.07 | 24.80 ± 2.75 1 | 1.3 ± 1.2 1,2 | 1.8 ± 2 |
| Physically active | 74.0 ± 12.3 | 1.65 ± 0.09 | 27.19 ± 3.77 | 3.7 ± 2.9 | 2.9 ± 2.3 |
| Sedentary | 76.0 ± 14.6 | 1.64 ± 0.1 | 28.10 ± 3.73 | 3.7 ± 2.9 | 3.1 ± 2.9 |
| Age class | |||||
| 55–65 | 76.6 ± 14.5 3 | 1.68 ± 0.09 3,4 | 26.95 ± 4.2 | 2.1 ± 2 | 1.5 ± 2.2 3,4 |
| 65–74 | 73.7 ± 12.8 | 1.64 ± 0.09 | 27.37 ± 3.61 | 3.2 ± 2.6 | 2.9 ± 2.3 |
| 75–84 | 69.6 ± 9.9 | 1.63 ± 0.09 | 26.26 ± 3.26 | 4.0 ± 3.3 | 3.8 ± 2.6 |
| Gender | |||||
| Female | 65.5 ± 9.8 | 1.59 ± 0.06 | 26.08 ± 3.98 | 3.3 ± 3.3 | 2.8 ± 2.5 |
| Male | 80.0 ± 11.5 5 | 1.70 ± 0.07 5 | 27.56 ± 3.42 | 2.9 ± 2.3 | 2.6 ± 2.5 |
| Steps (n) | Total Energy Expenditure (Kcal·day−1) | Energy Intake (Kcal·day−1) | |
|---|---|---|---|
| Physical activity level | |||
| Senior athletes | 11,941 ± 3739 1 | 2553.3 ± 468.4 1 | 1961.7 ± 368.1 |
| Physical active | 10,819 ± 3601 1 | 2483.5 ± 460 1 | 1884.4 ± 353.4 |
| Sedentary | 8923 ± 3218 | 2318.7 ± 423.9 | 1806.3 ± 489.3 |
| Age class | |||
| 55–65 | 11,1834 ± 3495 2 | 2653.9 ± 492.2 2,3 | 1926.7 ± 384.1 |
| 65–74 | 10,785 ± 3919 2 | 2402.4 ± 370.9 2 | 1818.3 ± 390.3 |
| 75–84 | 8884 ± 3230 | 2215.9 ± 393.5 | 1881.8 ± 483.6 |
| Gender | |||
| Female | 10,915 ± 3747 | 2178.4 ± 337 | 1675.7 ± 342 |
| Male | 9964 ± 3609 | 2645.2 ± 434.4 4 | 2033.2 ± 404.3 4 |
| BD (%) | SxBD (%) | CBD (%) | BDIabx (%) | PCS (pt.) | MCS (pt.) | |
|---|---|---|---|---|---|---|
| Physical activity level | ||||||
| Senior athletes | 9.4 ± 13.9 1 | 4.8 ± 23.7 1 | −18.3 ± 18.9 1 | 17.9 ± 8.6 | 54.5 ± 5.1 | 53.6 ± 7.7 |
| Physically active | 14.9 ± 11.9 | 12.1 ± 17.5 | −11.8 ± 16.0 | 15.8 ± 7.2 1 | 51.8 ± 7.3 | 51.9 ± 8.7 |
| Sedentary | 18.7 ± 13.9 | 20.0 ± 18.4 | −2.7 ± 22.4 | 19.7 ± 9.7 | 50.0 ± 8.3 | 49.5 ± 10.1 |
| Age class | ||||||
| 55–65 | 17.8 ± 13.1 | 17.2 ± 18.4 | −4.8 ± 21.0 2 | 18.9 ± 9.7 | 52.6 ± 6.8 | 48.7 ± 10.7 2 |
| 65–74 | 14.7 ± 14.3 | 14.5 ± 21.2 | −10.9 ± 21.9 | 18.7 ± 8.1 | 50.4 ± 8.1 | 52.0 ± 7.8 |
| 75–84 | 11.6 ± 13.1 | 6.5 ± 20.9 | −15.4 ± 15.8 | 15.5 ± 7.9 | 52.6 ± 7.0 | 53.9 ± 7.8 |
| Gender | ||||||
| Female | 16.3 ± 14.1 | 13.0 ± 19.6 | −8.9 ± 20.5 | 17.6 ± 9.4 | 51.1 ± 7.7 | 49.6 ± 10.6 |
| Male | 13.7 ± 13.3 | 13.3 ± 21.2 | 10.8 ± 20.3 | 18.1 ± 8.2 | 52.4 ± 7.2 | 52.8 ± 7.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Condello, G.; Capranica, L.; Migliaccio, S.; Forte, R.; Di Baldassarre, A.; Pesce, C. Energy Balance and Active Lifestyle: Potential Mediators of Health and Quality of Life Perception in Aging. Nutrients 2019, 11, 2122. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092122
Condello G, Capranica L, Migliaccio S, Forte R, Di Baldassarre A, Pesce C. Energy Balance and Active Lifestyle: Potential Mediators of Health and Quality of Life Perception in Aging. Nutrients. 2019; 11(9):2122. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092122
Chicago/Turabian StyleCondello, Giancarlo, Laura Capranica, Silvia Migliaccio, Roberta Forte, Angela Di Baldassarre, and Caterina Pesce. 2019. "Energy Balance and Active Lifestyle: Potential Mediators of Health and Quality of Life Perception in Aging" Nutrients 11, no. 9: 2122. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11092122