Change in Diet Quality over 12 Years in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Australian Longitudinal Study on Women’s Health
2.2. Participants: The 1946–1951 Cohort
2.3. Sociodemographic Characteristics
2.4. Health Characteristics
2.5. Assessment of Dietary Intake
2.6. Australian Recommended Food Score
2.7. Statistical Analysis
3. Results
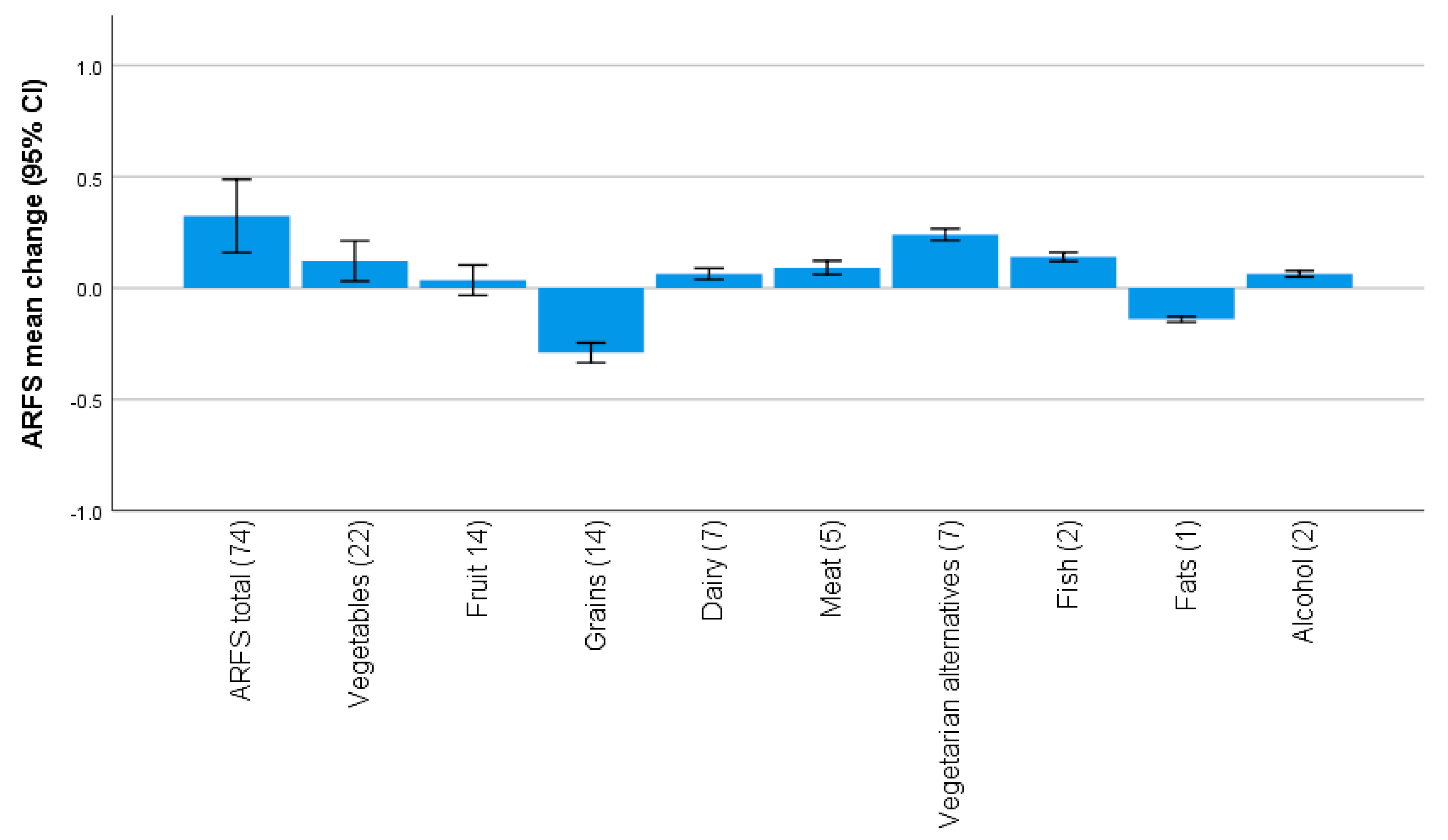
3.1. Australian Recommended Food Score
3.2. Characteristics of Women Whose Diet Quality Changed
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kant, A.K. Dietary patterns health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Wirt, A.; Collins, C.E. Diet quality—What is it does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Diet quality as assessed by the Healthy Eating Index the Alternate Healthy Eating Index the Dietary Approaches to Stop Hypertension score, health outcomes: A systematic review meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2015, 115, 780–800. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef]
- Patterson, A.; Hure, A.; Burrows, T.; Jackson, J.; Collins, C. Diet quality 10-year healthcare costs by BMI categories in the mid-age cohort of the Australian Longitudinal Study on Women’s Health. J. Hum. Nutr. Diet. 2018, 31, 463–472. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Changes in Diet Quality Scores Risk of Cardiovascular Disease among US Men Women. Circulation 2015, 132, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- Baden, M.Y.; Liu, G.; Satija, A.; Li, Y.; Sun, Q.; Fung, T.T.; Rimm, E.B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Changes in Plant-Based Diet Quality Total Cause-Specific Mortality. Circulation 2019, 140, 979–991. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Association of Changes in Diet Quality with Total Cause-Specific Mortality. N. Engl. J. Med 2017, 377, 143–153. [Google Scholar] [CrossRef]
- Brown, W.J.; Bryson, L.; Byles, J.E.; Dobson, A.J.; Lee, C.; Mishra, G.; Schofield, M. Women’s Health Australia: Recruitment for a national longitudinal cohort study. Women Health 1999, 28, 23–40. [Google Scholar] [CrossRef]
- Brown, W.J.; Young, A.F.; Byles, J.E. Tyranny of distance? The health of mid-age women living in five geographical areas of Australia. Aust. J. Rural Health 1999, 7, 148–154. [Google Scholar] [CrossRef]
- Lee, C.; Dobson, A.J.; Brown, W.J.; Bryson, L.; Byles, J.; Warner-Smith, P.; Young, A.F. Cohort profile: The Australian longitudinal study on women’s health. Int. J. Epidemiol. 2005, 34, 987–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Women’s Health Australia. Australian Longitudinal Study on Women’s Health: Sample. 2019. Available online: https://wwwalswhorgau/about/sample (accessed on 10 December 2019).
- Trewin, D. Socio-Economic Indexes for Areas (SEIFA). Canberra Australia; Australian Bureau of Statistics: Canberra, Australia, 2001.
- Burton, N.W.; Brown, W.; Dobson, A. Accuracy of body mass index estimated from self-reported height weight in mid-aged Australian women. Aust. N. Z. J. Public Health 2010, 34, 620–623. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing Managing the Global Epidemic, WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000; p. 252. [Google Scholar]
- Giles, G.; Ireland, P. Dietary Questionnaire for Epidemiological Studies (Version 2) Melbourne; The Cancer Council Victoria: Melbourne, Australia, 1996. [Google Scholar]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health. 2000, 24, 576–583. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines 2013; National Health and Medical Research Council: Canberra, Australia, 2013.
- Williams, R.L.; Rollo, M.E.; Schumacher, T.; Collins, C.E. Diet quality scores of Australian adults who have completed the Healthy Eating Quiz. Nutrients 2017, 9, 880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef]
- Orr, C.J.; Keyserling, T.C.; Ammerman, A.S.; Berkowitz, S.A. Diet quality trends among adults with diabetes by socioeconomic status in the US: 1999–2014. BMC Endocr. Disord. 2019, 19, 54. [Google Scholar] [CrossRef]
- Rollo, M.E.; Aguiar, E.J.; Pursey, K.M.; Morgan, P.J.; Plotnikoff, R.C.; Young, M.D.; Collins, C.E.; Callister, R. Impact on dietary intake of a self-directed gender-tailored diabetes prevention program in men. World J. Diabetes 2017, 8, 414–421. [Google Scholar] [CrossRef]
- Miller, C.K.; Weinhold, K.R.; Nagaraja, H.N. Impact of a Worksite Diabetes Prevention Intervention on Diet Quality Social Cognitive Influences of Health Behavior: A Randomized Controlled Trial. J. Nutr. Educ. Behav. 2016, 48, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [Green Version]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate a practical guide to its calculation use limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Freedman, L.S.; Schatzkin, A.; Midthune, D.; Kipnis, V. Dealing with dietary measurement error in nutritional cohort studies. J. Natl. Cancer Inst. 2011, 103, 1086–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, A.G.; Van Der Pols, J.C.; Dobson, A.J. Regression to the mean: What it is how to deal with it. Int. J. Epidemiol. 2004, 34, 215–220. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Survey 3 (2001) n = 11,226 | Survey 7 (2013) n = 9151 | |
|---|---|---|
| Sociodemographic Characteristics, % (n) | ||
| Age (years), Mean (SD) | 52.1 (1.5) | 64.3 (1.5) |
| SEIFA Index of Disadvantage, Mean (SD) | 995.5 (57.5) | 998.2 (85.5) |
| ARIA Classification | ||
| Major Cities | 34.1 (3807) | 38.3 (3508) |
| Inner/Outer Regional | 61.5 (6861) | 58.5 (5354) |
| Remote/Very Remote | 4.4 (485) | 2.8 (261) |
| Ability to Manage on Current Income | ||
| Difficult/Impossible | 38.6 (4277) | 32.2 (2903) |
| Not Too Bad | 43.5 (4820) | 47.9 (4322) |
| Easy | 18.0 (1993) | 20.0 (1801) |
| Health characteristics, % (n) | ||
| BMI (kg/m2), Mean (SD) | 26.9 (5.5) | 27.8 (5.7) |
| BMI Classification | ||
| Underweight <18.5 kg/m2 | 1.4 (147) | 1.2 (103) |
| Healthy Weight 18.5–24.99 kg/m2 | 42.5 (4457) | 35.0 (3083) |
| Overweight, 25–29.99 kg/m2 | 32.3 (3388) | 33.7 (2971) |
| Obese, ≥30 kg/m2 | 23.7 (2483) | 30.2 (2660) |
| Smoking Status | ||
| Never Smoked | 61.3 (6852) | 63.0 (5716) |
| Ex-Smoker | 24.2 (2709) | 30.3 (2752) |
| Current Smoker | 14.4 (1618) | 6.7 (604) |
| Physical Activity Level | ||
| Sedentary | 18.1 (1936) | 17.4 (1530) |
| Low | 37.1 (3968) | 24.2 (2127) |
| Moderate | 20.3 (2168) | 21.1 (1858) |
| High | 24.5 (2622) | 37.3 (3277) |
| General Health | ||
| Poor | 1.6 (175) | 1.6 (148) |
| Fair | 12.4 (1380) | 12.0 (1099) |
| Good | 39.0 (4347) | 39.5 (3605) |
| Excellent/Very good | 47.1 (5250) | 46.9 (4279) |
| Diet Quality, ARFS Mean Score (SD) | n = 10,629 | n = 9115 |
| Total Score /74 | 32.6 (8.8) | 33.1 (8.6) |
| Vegetables /22 | 13.6 (4.4) | 13.8 (4.5) |
| Fruit /14 | 5.6 (3.2) | 5.7 (3.0) |
| Dairy /7 | 2.1 (1.0) | 2.2 (1.0) |
| Grains /14 | 4.0 (1.8) | 3.8 (1.8) |
| Meat /5 | 2.4 (1.3) | 2.5 (1.3) |
| Vegetarian Alternatives /7 | 2.0 (1.1) | 2.3 (1.1) |
| Fish /2 | 0.9 (0.8) | 1.0 (0.8) |
| Fats /1 | 0.7 (0.5) | 0.5 (0.5) |
| Alcohol /2 | 1.4 (0.6) | 1.5 (0.6) |
| 2001 ARFS Tertile | |||
|---|---|---|---|
| Tertile 1 (Lowest) n = 3357 | Tertile 2 n = 3697 | Tertile 3 (Highest) n = 3575 | |
| 2001 ARFS Total, Mean (SD) | 22.5 (4.7) | 32.5 (2.2) | 42.2 (4.3) |
| 2013 ARFS Total, Mean (SD) | 26.8 (7.6) | 33.3 (6.9) * | 38.7 (7.0) * |
| Change in ARFS Total 2001 to 2013, Mean (SD) | 4.2 (7.1) | 0.7 (6.8) * | −3.4 (6.9) * |
| Sociodemographic Characteristics (Survey 3 2001), % (n) | |||
| SEIFA Index of Disadvantage, Mean (SD) | 990.6 (56.0) | 996.9 (58.5) * | 999.5 (57.8) * |
| Living in Major Cities | 33.0 (1100) | 34.9 (1282) | 34.4 (1223) |
| Managing on Current Income Easy/Not Too Bad | 56.2 (1863) | 62.8 (2291) * | 65.7 (2320) * |
| Health Characteristics (Survey 3 2001), % (n) | |||
| BMI (kg/m2), Mean (SD) | 27.0 (5.8) | 26.8 (5.4) | 26.8 (5.2) |
| Healthy Weight Range for BMI | 41.9 (1297) | 42.8 (1491) | 42.8 (1491) |
| Never Smoker | 56.9 (1903) | 61.4 (2253) * | 64.7 (2299) * |
| High Physical Activity | 19.3 (614) | 23.4 (826) * | 30.9 (1066) |
| Excellent/Very Good General Health | 41.4 (1380) | 47.5 (1739) * | 53.1 (1883) * |
| Diet Quality Got Worse a (n = 2361) | Diet Stayed the Same b (n = 3077) | Diet Quality Improved c (n = 2723) | |
|---|---|---|---|
| Change in ARFS Total 2001 to 2013, Mean (SD) | −8.6 (4.4) | −0.01 (2.0) | 8.4 (2.0) |
| 2001 ARFS Total, Mean (SD) | 37.4 (8.0) ** | 33.2 (8.0) ** | 28.6 (7.7) |
| 2013 ARFS Total, Mean (SD) | 28.9 (8.4) ** | 33.2 (8.0) ** | 37.0 (7.5) |
| Sociodemographic Characteristics (2001), % (n) | |||
| SEIFA Index of Disadvantage, Mean (SD) | 997.5 (56.8) | 997.9 (58.4) | 995.3 (58.1) |
| Living in Major Cities | 33.7 (793) | 33.9 (1041) | 35.3 (957) |
| Managing on Current Income Easy/Not Too Bad | 63.4 (1485) | 65.6 (1997) | 62.8 (1698) |
| Health Characteristics (Survey 3, 2001), % (n) | |||
| BMI (kg/m2), Mean (SD) | 26.9 (5.4) | 26.5 (5.2) | 26.7 (5.4) |
| Healthy Weight Range for BMI | 40.2 (947) | 44.2 (1281) | 44.2 (1135) |
| Never Smoker | 61.7 (1454) | 62.9 (1928) | 63.3 (1721) |
| High Physical Activity | 29.7 (676) ** | 24.3 (727) * | 22.8 (593) |
| Excellent/Very Good General Health | 50.9 (1192) | 50.8 (1556) | 50.1 (1356) |
| Change in ARFS for Women in the Lowest Baseline ARFS Tertile (n = 2451) | ||
|---|---|---|
| Diet Quality Remained Poor/Worsened a (n = 1148) | Diet Quality Improved b (n = 1303) | |
| 2001 ARFS Total, Mean (SD) | 23.4 (4.1) | 22.0 (4.8) |
| 2013 ARFS Total, Mean (SD) | 21.6 (5.6) | 31.5 (5.9) |
| Change in ARFS Total, Mean (SD) | −1.8 (4.1) | 9.4 (4.6) |
| Sociodemographic Characteristics (Survey 3 2001) % (n) | ||
| SEIFA Index of Disadvantage, Mean (SD) | 993.9 (57.5) | 991.9 (56.0) |
| Living in Major Cities | 35.1 (401) | 33.2 (430) |
| Managing on Current Income Easy/Not Too Bad | 58.3 (660) | 58.3 (754) |
| Health Characteristics (Survey 3 2001) % (n) | ||
| BMI (kg/m2), Mean (SD) | 26.9 (5.8) | 26.9 (5.7) |
| Healthy Weight Range for BMI | 41.1 (434) * | 44.2 (540) |
| Never Smoker | 55.6 (637) * | 61.5 (800) |
| High Physical Activity | 19.7 (218) | 19.3 (241) |
| Excellent/Very Good General Health | 42.9 (489) | 46.8 (607) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldwin, J.N.; Forder, P.M.; Haslam, R.L.; Hure, A.J.; Loxton, D.J.; Patterson, A.J.; Collins, C.E. Change in Diet Quality over 12 Years in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. Nutrients 2020, 12, 147. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010147
Baldwin JN, Forder PM, Haslam RL, Hure AJ, Loxton DJ, Patterson AJ, Collins CE. Change in Diet Quality over 12 Years in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health. Nutrients. 2020; 12(1):147. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010147
Chicago/Turabian StyleBaldwin, Jennifer N., Peta M. Forder, Rebecca L. Haslam, Alexis J. Hure, Deborah J. Loxton, Amanda J. Patterson, and Clare E. Collins. 2020. "Change in Diet Quality over 12 Years in the 1946–1951 Cohort of the Australian Longitudinal Study on Women’s Health" Nutrients 12, no. 1: 147. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010147