Circulating Ionized Magnesium: Comparisons with Circulating Total Magnesium and the Response to Magnesium Supplementation in a Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Biomarker Measures
2.3. Statistical Analysis
3. Results
3.1. Study Participants
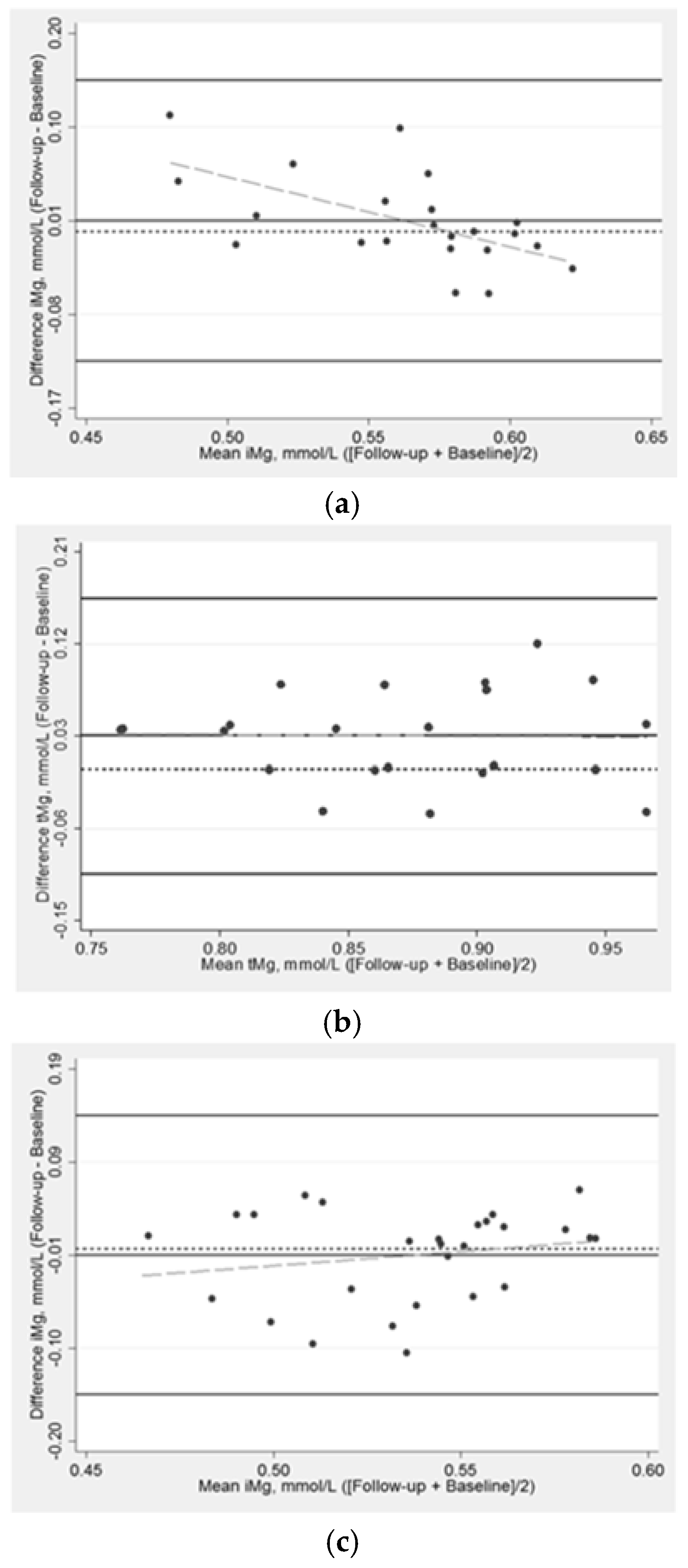
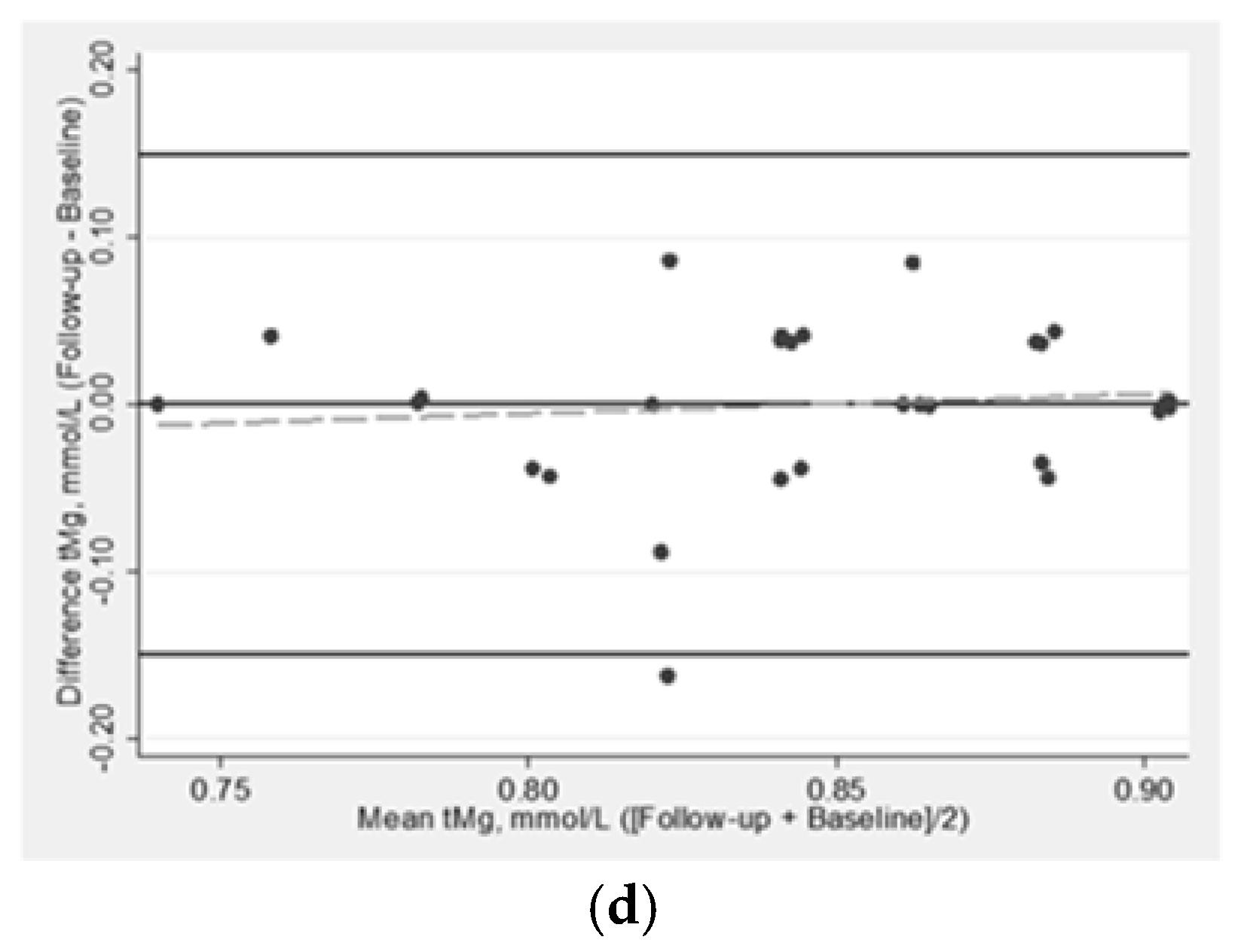
3.2. Effect of Magnesium Supplementation on Magnesium Biomarkers
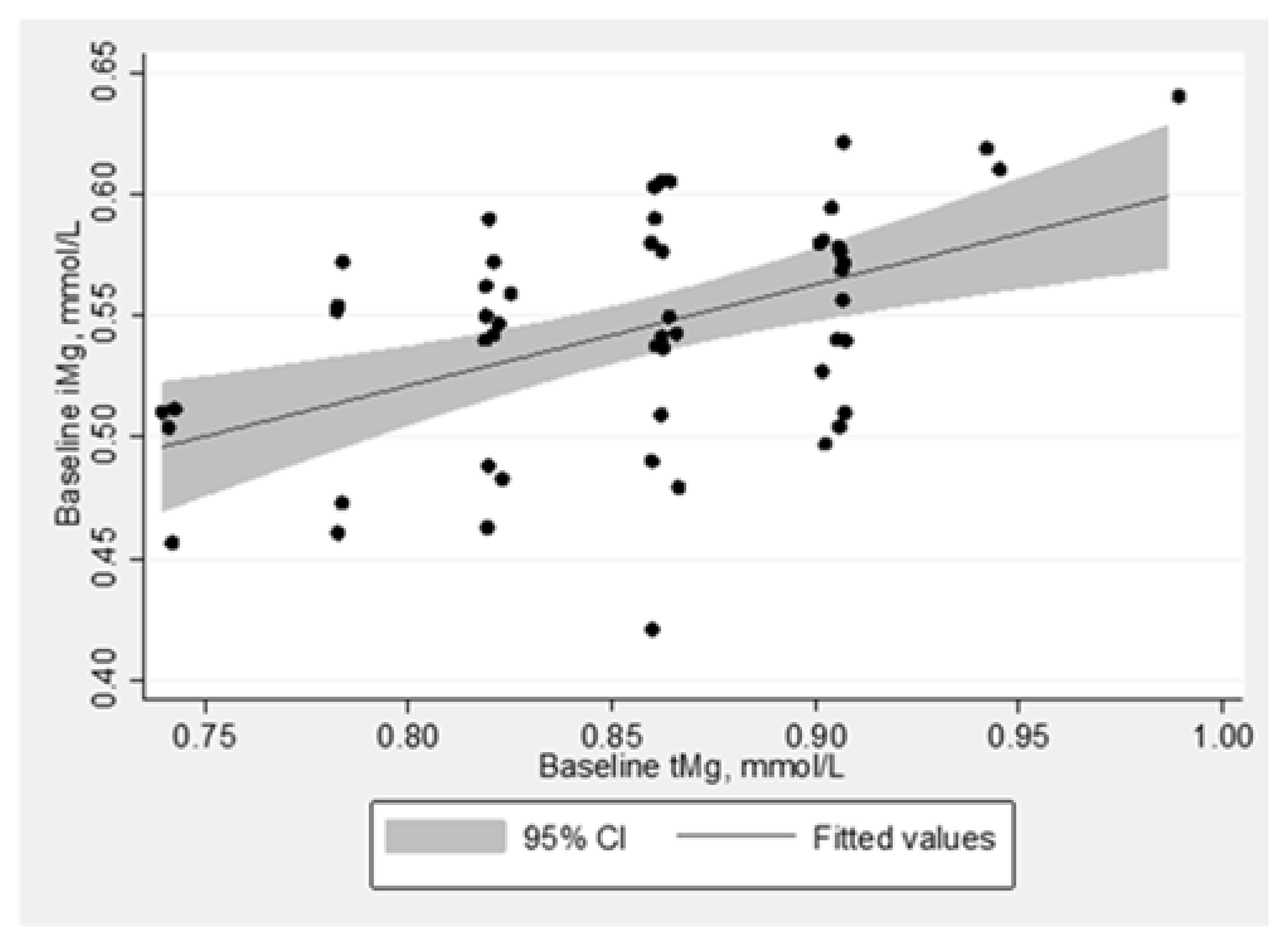
3.3. Relationship between Magnesium Biomarkers
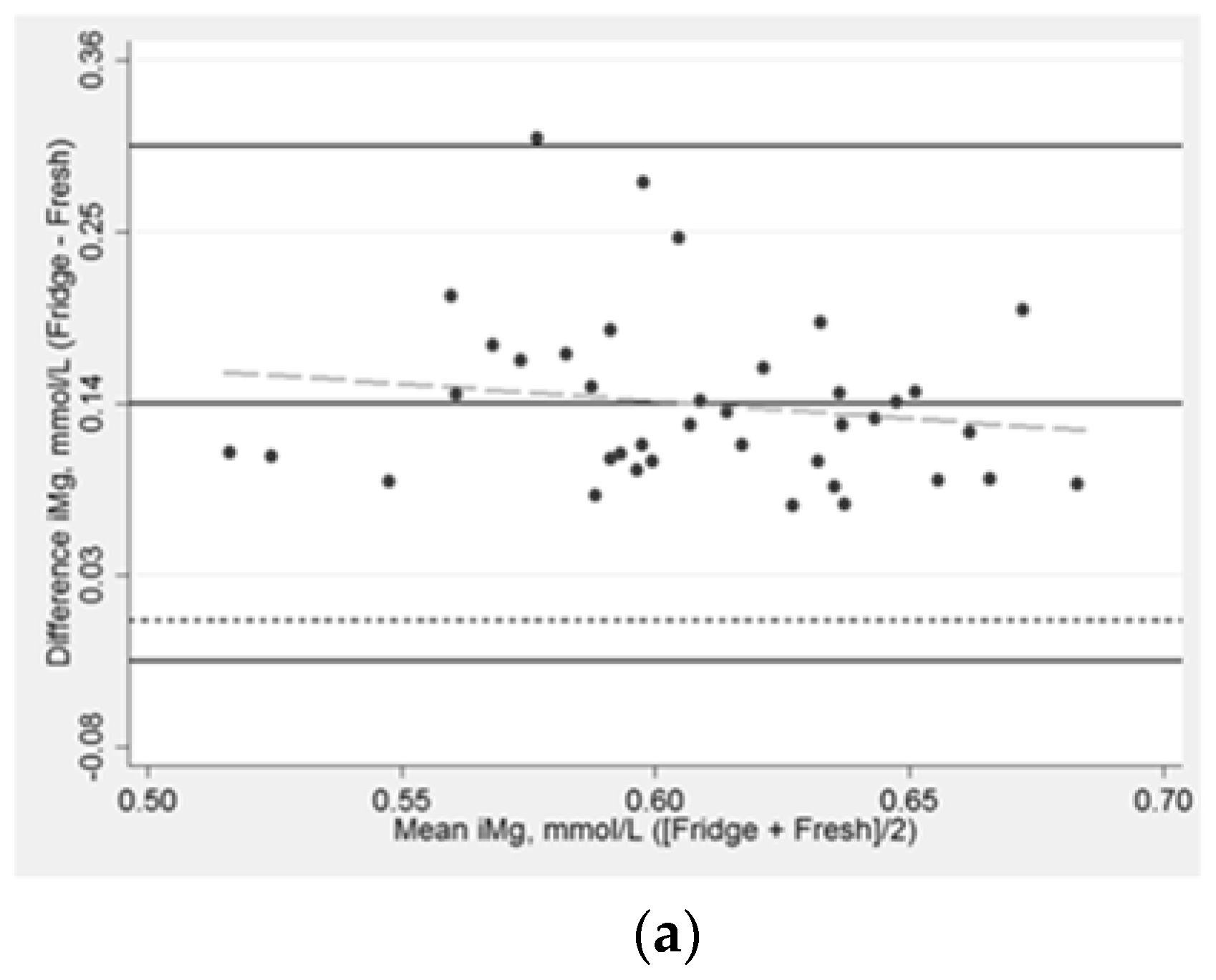
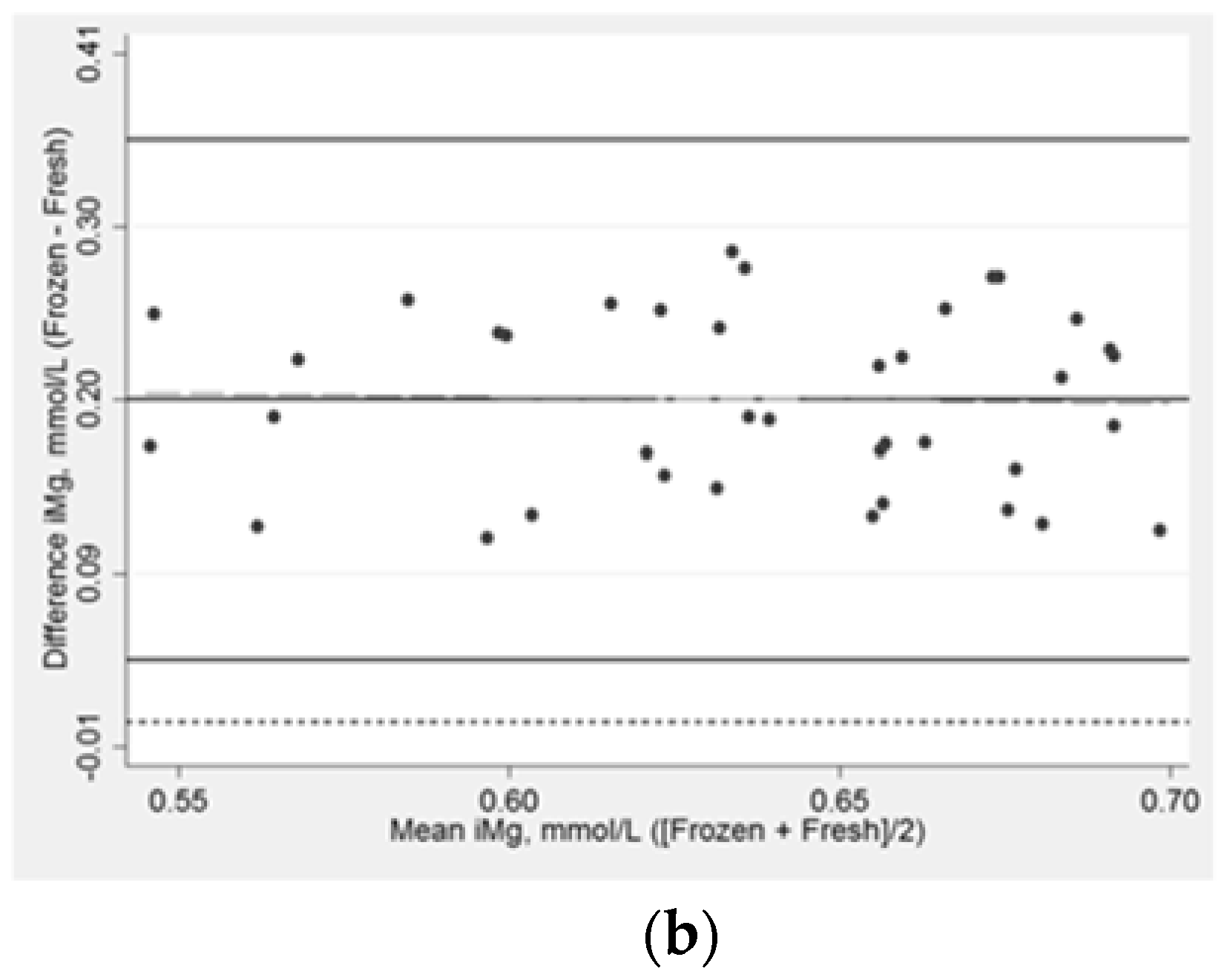
3.4. Comparisons of Ionized Magnesium in Fresh, Refrigerated, and Frozen Blood Specimens
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bryrd-Bredbenner, C.; Moe, G.; Berning, J.; Kelley, D. Wardlaws Perspectives in Nutrition Updated with 2015 2020 Dietary Guidelines for Americans, 10th ed.; McGraw-Hill Education: New York, NY, USA, 2016. [Google Scholar]
- Institute of Medicine Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin, D., and Fluoride; National Academy of Sciences: Washington, DC, USA, 1997. [Google Scholar]
- Costello, R.B.; Nielsen, F. Interpreting magnesium status to enhance clinical care: Key indicators. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Glasdam, S.M.; Glasdam, S.; Peters, G.H. The Importance of Magnesium in the Human Body: A Systematic Literature Review. Adv. Clin. Chem. 2016, 73, 169–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grober, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altura, B.M.; Altura, B.T. Role of magnesium in patho-physiological processes and the clinical utility of magnesium ion selective electrodes. Scand. J. Clin. Lab. Investig. Suppl. 1996, 224, 211–234. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Dominguez, L.J.; Galioto, A.; Pineo, A.; Belvedere, M. Oral magnesium supplementation improves vascular function in elderly diabetic patients. Magnes. Res. 2010, 23, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Kazaks, A.G.; Uriu-Adams, J.Y.; Albertson, T.E.; Shenoy, S.F.; Stern, J.S. Effect of oral magnesium supplementation on measures of airway resistance and subjective assessment of asthma control and quality of life in men and women with mild to moderate asthma: A randomized placebo controlled trial. J. Asthma 2010, 47, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Zavaczki, Z.; Szollosi, J.; Kiss, S.A.; Koloszar, S.; Fejes, I.; Kovacs, L.; Pal, A. Magnesium-orotate supplementation for idiopathic infertile male patients: A randomized, placebo-controlled clinical pilot study. Magnes. Res. 2003, 16, 131–136. [Google Scholar] [PubMed]
- Wary, C.; Brillault-Salvat, C.; Bloch, G.; Leroy-Willig, A.; Roumenov, D.; Grognet, J.M.; Leclerc, J.H.; Carlier, P.G. Effect of chronic magnesium supplementation on magnesium distribution in healthy volunteers evaluated by 31P-NMRS and ion selective electrodes. Br. J. Clin. Pharm. 1999, 48, 655–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutsey, P.L.; Chen, L.Y.; Eaton, A.; Jaeb, M.; Rudser, K.D.; Neaton, J.D.; Alonso, A. A Pilot Randomized Trial of Oral Magnesium Supplementation on Supraventricular Arrhythmias. Nutrients 2018, 10, 884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senn, S. Change from baseline and analysis of covariance revisited. Stat. Med. 2006, 25, 4334–4344. [Google Scholar] [CrossRef] [PubMed]
- Frison, L.; Pocock, S.J. Repeated measures in clinical trials: Analysis using mean summary statistics and its implications for design. Stat. Med. 1992, 11, 1685–1704. [Google Scholar] [CrossRef] [PubMed]
- Greenway, D.C.; Hindmarsh, J.T.; Wang, J.; Khodadeen, J.A.; Hebert, P.C. Reference interval for whole blood ionized magnesium in a healthy population and the stability of ionized magnesium under varied laboratory conditions. Clin. Biochem. 1996, 29, 515–520. [Google Scholar] [CrossRef]
- Altura, B.T.; Shirey, T.L.; Young, C.C.; Dell’Orfano, K.; Hiti, J.; Welsh, R.; Yeh, Q.; Barbour, R.L.; Altura, B.M. Characterization of a new ion selective electrode for ionized magnesium in whole blood, plasma, serum, and aqueous samples. Scand. J. Clin. Lab. Investig. Suppl. 1994, 217, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Yeh, D.D.; Chokengarmwong, N.; Chang, Y.; Yu, L.; Arsenault, C.; Rudolf, J.; Lee-Lewandrowski, E.; Lewandrowski, K. Total and ionized magnesium testing in the surgical intensive care unit—Opportunities for improved laboratory and pharmacy utilization. J. Crit. Care 2017, 42, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.T.; Altura, B.M. Measurement of ionized magnesium in whole blood, plasma and serum with a new ion-selective electrode in healthy and diseased human subjects. Magnes. Trace Elem. 1991, 10, 90–98. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Status | Baseline iMg Concentration | |||
|---|---|---|---|---|
| Magnesium (400 mg Daily) | Placebo | ≥Median 1 | <Median | |
| N | 29 | 30 | 28 | 26 |
| Age, years 2 | 61.3 ± 5.3 | 61.6 ± 5.2 | 61.0 ± 4.3 | 62.2 ± 6.0 |
| Age category | ||||
| ≥65 years | 6 (20.7) | 8 (26.7) | 5 (17.9) | 8 (30.8) |
| <65 years | 23 (79.3) | 22 (73.3) | 23 (82.1) | 18 (69.2) |
| Sex | ||||
| Female | 25 (86.2) | 18 (60.0) | 23 (82.1) | 16 (61.5) |
| Male | 4 (13.8) | 12 (40.0) | 5 (17.9) | 10 (38.5) |
| Race | ||||
| White | 27 (93.1) | 29 (96.7) | 26 (92.9) | 25 (96.2) |
| Non-white | 2 (6.9) | 1(3.3) | 2 (7.1) | 1(3.8) |
| Education | ||||
| High school graduate or GED | 0 (0.0) | 1 (3.3) | 0 (0.0) | 0 (0.0) |
| Some college | 6 (20.7) | 4 (13.3) | 4 (14.3) | 5 (19.2) |
| College graduate | 10 (34.5) | 16 (53.3) | 10 (35.7) | 14 (53.9) |
| Graduate or professional school | 13 (44.8) | 9 (30.0) | 13 (46.4) | 7 (26.9) |
| BMI, kg/m2 | 27.7 ± 4.9 | 28.0 ± 4.5 | 26.9 ± 3.2 | 28.4 ± 5.4 |
| Systolic blood pressure, mmHg | 118.4 ± 14.9 | 119.3 ± 18.4 | 116.8 ± 12.1 | 122.0 ± 20.4 |
| Diastolic blood pressure, mmHg | 71.9 ± 8.7 | 71.2 ± 10.2 | 71.0 ± 7.0 | 72.46 ± 11.2 |
| Glucose, mg/dL | 94.2 ± 10.6 | 103.2 ± 40.2 | 94.1 ± 9.4 | 104.9 ± 43.1 |
| Sensitivity analysis 3 | 94.2 ± 10.6 | 96.2 ± 11.64 | 94.1 ± 9.4 | 96.8 ± 12.7 |
| pH | 7.38 ± 0.02 | 7.38 ± 0.03 | 7.38 ± 0.02 | 7.38 ± 0.03 |
| Total magnesium, mmol/L | 0.86 ± 0.06 | 0.85 ± 0.05 | 0.87 ± 0.05 | 0.84 ± 0.06 |
| Ionized magnesium, mmol/L 4 | 0.56 ± 0.06 | 0.55 ± 0.04 | 0.59 ± 0.03 | 0.51 ± 0.04 |
| Total calcium, mmol/L | 2.35 ± 0.09 | 2.34 ± 0.09 | 2.34 ± 0.09 | 2.35 ± 0.08 |
| Ionized calcium, mmol/L 4 | 1.19 ± 0.03 | 1.18 ± 0.03 | 1.19 ± 0.03 | 1.18 ± 0.03 |
| Intervention Status | Mean Intervention Effect (95% CI) 1 | p-Value | ||
|---|---|---|---|---|
| Magnesium (400 mg Daily) Mean (SD) | Placebo Mean (SD) | |||
| N | 29 | 30 | ||
| iMg, mmol/L 2 | 22 | 27 | 0.03 (0.01, 0.05) | 0.009 |
| Baseline | 0.56 (0.06) | 0.54 (0.04) | ||
| Follow-up 3 | 0.57 (0.03) | 0.53 (0.04) | ||
| Change | 0.01 (0.05) | −0.01 (0.05) | ||
| tMg, mmol/L | 24 | 30 | 0.04 (0.01, 0.06) | 0.004 |
| Baseline | 0.86 (0.06) | 0.85 (0.05) | ||
| Follow-up 3 | 0.89 (0.06) | 0.85 (0.05) | ||
| Change | 0.03 (0.05) | 0.00 (0.05) | ||
| Time from Draw to Analysis 1 | pH 1 | Concentrations, 1 mmol/L | Mean Difference (95% CI), mmol/L | Percentiles of Difference from Fresh iMg, mmol/L 2 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Min | 25th | 50th | 75th | Max | |||||
| iMg (normalized) | |||||||||
| Fresh 3 | 4.8 min (3.4) | 7.38 (0.03) | 0.54 (0.05) | Reference | - | - | - | - | - |
| Refrigerated | 69.6 min (25.3) | 7.45 (0.04) | 0.68 (0.04) | 0.14 (0.12,0.16) | 0.07 | 0.10 | 0.13 | 0.17 | 0.31 |
| Frozen | 82.2 days (15.4) | 7.51 (0.04) | 0.73 (0.05) | 0.19 (0.18,0.21) | 0.11 | 0.15 | 0.19 | 0.25 | 0.29 |
| iMg (not normalized) | |||||||||
| Fresh | 4.8 min (3.4) | 7.38 (0.03) | 0.54 (0.05) | Reference | - | - | - | - | - |
| Refrigerated | 69.6 min (25.3) | 7.45 (0.04) | 0.65 (0.04) | 0.11 (0.10,0.13) | 0.04 | 0.07 | 0.09 | 0.13 | 0.25 |
| Frozen | 82.2 days (15.4) | 7.51 (0.04) | 0.68 (0.05) | 0.14 (0.12,0.15) | 0.05 | 0.09 | 0.13 | 0.18 | 0.20 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rooney, M.R.; Rudser, K.D.; Alonso, A.; Harnack, L.; Saenger, A.K.; Lutsey, P.L. Circulating Ionized Magnesium: Comparisons with Circulating Total Magnesium and the Response to Magnesium Supplementation in a Randomized Controlled Trial. Nutrients 2020, 12, 263. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010263
Rooney MR, Rudser KD, Alonso A, Harnack L, Saenger AK, Lutsey PL. Circulating Ionized Magnesium: Comparisons with Circulating Total Magnesium and the Response to Magnesium Supplementation in a Randomized Controlled Trial. Nutrients. 2020; 12(1):263. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010263
Chicago/Turabian StyleRooney, Mary R., Kyle D. Rudser, Alvaro Alonso, Lisa Harnack, Amy K. Saenger, and Pamela L. Lutsey. 2020. "Circulating Ionized Magnesium: Comparisons with Circulating Total Magnesium and the Response to Magnesium Supplementation in a Randomized Controlled Trial" Nutrients 12, no. 1: 263. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010263