Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Subjects
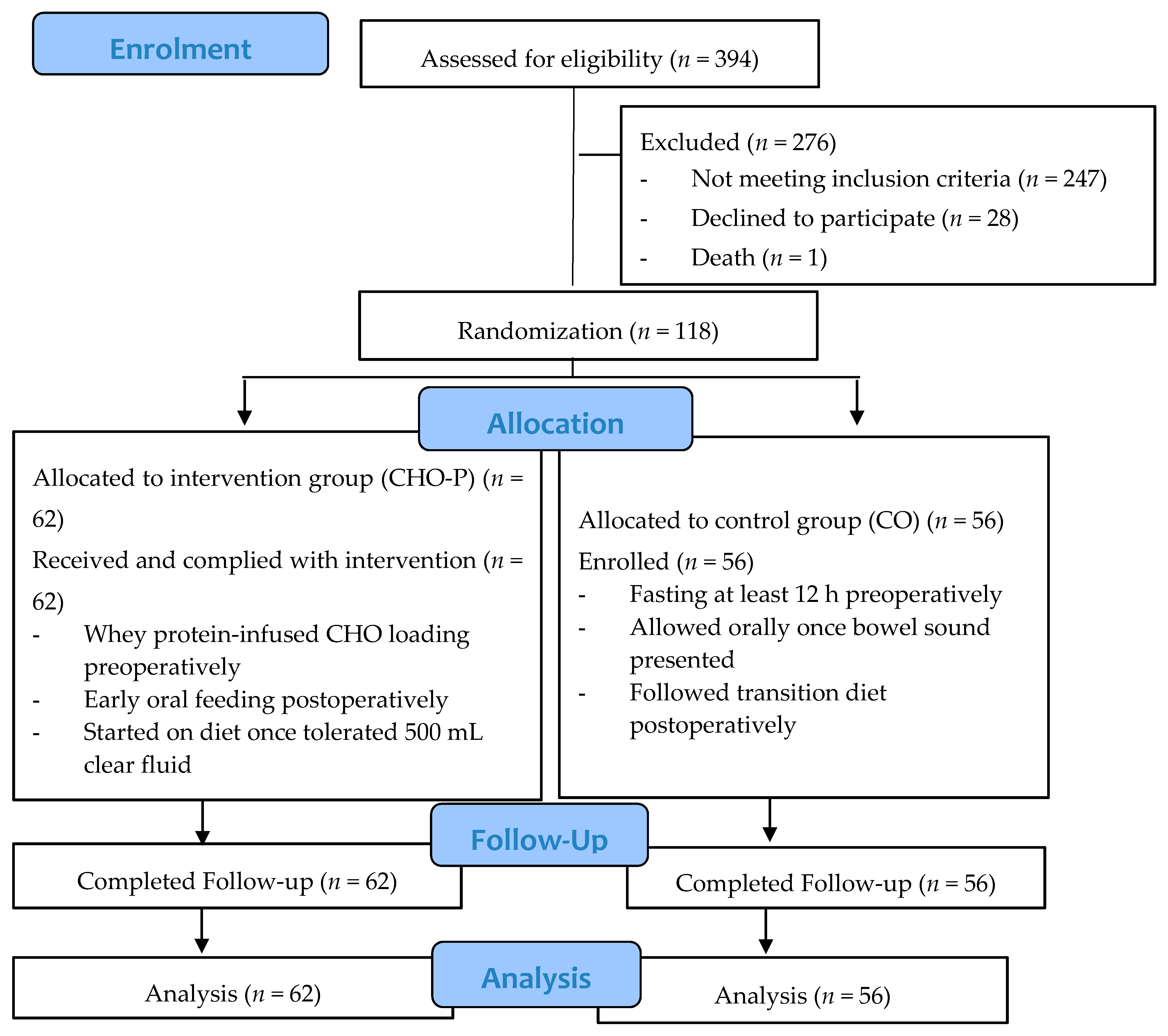
2.3. Study Design and Randomization
2.4. Intervention Group (CHO-P)
2.5. Control Group (CO)
2.6. Discharge Criteria
2.7. Data Collection Procedure
2.8. Outcomes Measurement
2.9. Adverse Events and Data Safety Monitoring
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Ljungqvist, O.; Nygren, J.; Hausel, J.; Thorell, A. Preoperative nutrition therapy-novel developments. Näringsforskning 2000, 44, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Nygren, J. The metabolic effects of fasting and surgery. Best Pract. Res. Clin. Anaesthesiol. 2006, 20, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Balayla, J.; Bujold, E.; Lapensée, L.; Mayrand, M.-H.; Sansregret, A. Early Versus Delayed Postoperative Feeding After Major Gynaecological Surgery and its Effects on Clinical Outcomes, Patient Satisfaction, and Length of Stay: A Randomized Controlled Trial. J. Obstet. Gynaecol. Can. 2015, 37, 1079–1085. [Google Scholar] [CrossRef] [Green Version]
- Kehlet, H.; Wilmore, D.W. Multimodal strategies to improve surgical outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar] [CrossRef]
- Henriksen, M.G.; Hessov, I.; Dela, F.; Vind Hansen, H.; Haraldsted, V.; Rodt, S.Å. Effects of preoperative oral carbohydrates and peptides on postoperative endocrine response, mobilization, nutrition and muscle function in abdominal surgery. Acta Anaesthesiol. Scand. 2003, 47, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Knott, A.; Pathak, S.; McGrath, J.S.; Kennedy, R.; Horgan, A.; Mythen, M.; Carter, F.; Francis, N.K. Consensus views on implementation and measurement of enhanced recovery after surgery in England: Delphi study. BMJ Open 2012, 2, e001878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pexe-Machado, P.A.; de Oliveira, B.D.; Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E. Shrinking preoperative fast time with maltodextrin and protein hydrolysate in gastrointestinal resections due to cancer. Nutrition 2013, 29, 1054–1059. [Google Scholar] [CrossRef] [Green Version]
- Perrone, F.; da-Silva-Filho, A.C.; Adôrno, I.F.; Anabuki, N.T.; Leal, F.S.; Colombo, T.; da Silva, B.D.; Dock-Nascimento, D.B.; Damião, A.; de Aguilar-Nascimento, J.E. Effects of preoperative feeding with a whey protein plus carbohydrate drink on the acute phase response and insulin resistance. A randomized trial. Nutr. J. 2011, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Dock-Nascimento, D.; Aguilar-Nascimento, J.; Faria, M.; Caporossi, C.; Slhessarenko, N.; Waitzberg, D. Evaluation of the Effects of a Preoperative 2-Hour Fast with Maltodextrine and Glutamine on Insulin Resistance, Acute-Phase Response, Nitrogen Balance, and Serum Glutathione After Laparoscopic Cholecystectomy: A Controlled Randomized Trial. J. Parenter. Enter. Nutr. 2012, 36, 43–52. [Google Scholar] [CrossRef]
- Singh, M.; Chaudhary, M.; Vashistha, A.; Kaur, G. Evaluation of effects of a preoperative 2-hour fast with glutamine and carbohydrate rich drink on insulin resistance in maxillofacial surgery. J. Oral Biol. Craniofacial Res. 2015, 5, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalogera, E.; Bakkum-Gamez, J.N.; Jankowski, C.J.; Trabuco, E.; Lovely, J.K.; Dhanorker, S.; Grubbs, P.L.; Weaver, A.L.; Haas, L.R.; Borah, B.J.; et al. Enhanced recovery in gynecologic surgery. Obstet. Gynecol. 2013, 122, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Modesitt, S.C.; Sarosiek, B.M.; Trowbridge, E.R.; Redick, D.L.; Shah, P.M.; Thiele, R.H.; Tiouririne, M.; Hedrick, T.L. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Obstet. Gynecol. 2016, 128, 457–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, C.Y. Is enhanced recovery after surgery safe and beneficial for the elderly? Nutr. Status Dietary Intake Body Compos. 2018, 24, 149. [Google Scholar]
- Ariffin, A.C.; Ahmad, A.W.; Zuhdi, Z.; Mohamad, I.S.; Azman, A.; Othman, H.A.; Jarmin, R. Enhanced recovery after surgery (ERAS) post liver resection: safety and feasibility study. HPB 2016, 18, e539. [Google Scholar] [CrossRef] [Green Version]
- Ariffin, A.C.; Mohammad, A.T.; Zuhdi, Z.; Azman, A.; Othman, H.A.; Jarmin, R. Enhanced Recovery after Surgery (ERAS) Implementation after Pancreaticoduodenectomy: Interim Result. Middle East. J. Sci. Res. 2014, 21, 2072–2079. [Google Scholar]
- Kiela, P.R.; Ghishan, F.K. Physiology of Intestinal Absorption and Secretion. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 145–159. [Google Scholar] [CrossRef] [Green Version]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Lewis, S.J.; Egger, M.; Sylvester, P.A.; Thomas, S. Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials. BMJ 2001, 323, 773. [Google Scholar] [CrossRef] [Green Version]
- Mathur, S.; Plank, L.D.; McCall, J.L.; Shapkov, P.; McIlroy, K.; Gillanders, L.K.; Merrie, A.E.H.; Torrie, J.J.; Pugh, F.; Koea, J.B.; et al. Randomized controlled trial of preoperative oral carbohydrate treatment in major abdominal surgery. BJS 2010, 97, 485–494. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodward, M. Formulae for Sample Size, Power and Minimum Detectable Relative Risk in Medical Studies. J. R. Stat. Soc. 1992, 41, 185–196. [Google Scholar] [CrossRef]
- Elias, K.M.; Stone, A.B.; McGinigle, K.; Jo’An, I.T.; Scott, M.J.; Fawcett, W.J.; Demartines, N.; Lobo, D.N.; Ljungqvist, O.; Urman, R.D. The reporting on eras compliance, outcomes, and elements research (recover) checklist: A joint statement by the ERAS® and ERAS® USA societies. World J. Surg. 2019, 43, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiore, J.F., Jr.; Bialocerkowski, A.; Browning, L.; Faragher, I.G.; Denehy, L. Criteria to determine readiness for hospital discharge following colorectal surgery: An international consensus using the Delphi technique. Dis. Colon Rectum 2012, 55, 416–423. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Makuuchi, R.; Sugisawa, N.; Kaji, S.; Hikage, M.; Tokunaga, M.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Terashima, M. Enhanced recovery after surgery for gastric cancer and an assessment of preoperative carbohydrate loading. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 210–217. [Google Scholar] [CrossRef]
- Anderson, A.D.G.; McNaught, C.E.; MacFie, J.; Tring, I.; Barker, P.; Mitchell, C.J. Randomized clinical trial of multimodal optimization and standard perioperative surgical care. BJS 2003, 90, 1497–1504. [Google Scholar] [CrossRef]
- Minig, L.; Biffi, R.; Zanagnolo, V.; Attanasio, A.; Beltrami, C.; Bocciolone, L.; Botteri, E.; Colombo, N.; Iodice, S.; Landoni, F.; et al. Early Oral Versus “Traditional” Postoperative Feeding in Gynecologic Oncology Patients Undergoing Intestinal Resection: a Randomized Controlled Trial. Ann. Surg. Oncol. 2009, 16, 1660–1668. [Google Scholar] [CrossRef]
- Charoenkwan, K.; Phillipson, G.; Vutyavanich, T. Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Database Syst. Rev. 2007, 17, CD004508. [Google Scholar] [CrossRef]
- Miller, L.; Roland, B.C.; Whitson, M.; Passi, M.; Cheung, M.; Vegesna, A. Chapter 22-Clinical and Translational Aspects of Normal and Abnormal Motility in the Esophagus, Small Intestine and Colon. In Physiology of the Gastrointestinal Tract, 6th ed.; Said, H.M., Ed.; Academic Press: Cambridge, UK, 2018. [Google Scholar]
- Liu, V.X.; Rosas, E.; Hwang, J.; Cain, E.; Foss-Durant, A.; Clopp, M.; Huang, M.; Lee, D.C.; Mustille, A.; Kipnis, P.; et al. Enhanced Recovery After Surgery Program Implementation in 2 Surgical Populations in an Integrated Health Care Delivery SystemEnhanced Recovery After Surgery Program ImplementationEnhanced Recovery After Surgery Program Implementation. JAMA Surg. 2017, 152, e171032. [Google Scholar] [CrossRef] [PubMed]
- Marx, C.; Rasmussen, T.; Jakobsen, D.H.; Ottosen, C.; Lundvall, L.; Ottesen, B.; Callesen, T.; Kehlet, H. The effect of accelerated rehabilitation on recovery after surgery for ovarian malignancy. Acta Obstet. Et Gynecol. Scand. 2006, 85, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Riley, K.A.; Baer, J.A.; Harkins, G.J.; Rao, S.L. Preoperative Oral Hydration in Gynecologic Laparoscopy. J. Gynecolo. Surg. 2015, 31, 135–138. [Google Scholar] [CrossRef]
- Watanabe, J.; Ota, M.; Suwa, Y.; Suzuki, S.; Suwa, H.; Momiyama, M.; Ishibe, A.; Watanabe, K.; Akiyama, H.; Endo, I. The safety of preoperative amino acid (Elental®) loading in colon cancer surgery: prospective cohort study. Int. Surg. 2017. [Google Scholar] [CrossRef] [Green Version]
- Kimball, S.R.; Farrell, P.A.; Jefferson, L.S. Invited Review: Role of insulin in translational control of protein synthesis in skeletal muscle by amino acids or exercise. J. Appl. Physiol. 2002, 93, 1168–1180. [Google Scholar] [CrossRef]
- Noblett, S.E.; Watson, D.S.; Huong, H.; Davison, B.; Hainsworth, P.J.; Horgan, A.F. Pre-operative oral carbohydrate loading in colorectal surgery: A randomized controlled trial. Colorectal Dis. 2006, 8, 563–569. [Google Scholar] [CrossRef]
- Svanfeldt, M.; Thorell, A.; Hausel, J.; Soop, M.; Rooyackers, O.; Nygren, J.; Ljungqvist, O. Randomized clinical trial of the effect of preoperative oral carbohydrate treatment on postoperative whole-body protein and glucose kinetics. BJS 2007, 94, 1342–1350. [Google Scholar] [CrossRef]


{kind=link}
| Items | CHO-P | CO |
|---|---|---|
| (a) preadmission patient education regarding the protocol | Subjects were counselled and had the ERAS protocol explained by a surgeon, anesthetist, and dietitian | Preoperative counselling by surgeon and anesthetist |
| (b) preadmission screening and optimization as indicated for nutritional deficiency, anemia, HbA1c, tobacco cessation, and ethanol use | Preadmission screening: nutritional deficiency via scored PG-SGA, anemia, tobacco cessation, and ethanol counselling | Preadmission screening: anemia, tobacco cessation, and ethanol counselling |
| (c) fasting and carbohydrate loading | Normal diet until 6 h before operation; in the evening before operation the drink comprised 500 kcal, 100 g carbohydrate, and 18 g whey protein (total 474 mL), whilst the drink provided 3 h before operation comprised 237 mL with 250 kcal, 50 g carbohydrate, and 9 g whey protein | Last meal was dinner, which was minimal 12 h before operation. Subjects started fasting from midnight on the day of operation |
| (d) Pre-emptive analgesia (dose, route, timing) | No routine | |
| (e) Antiemetic prophylaxis (dose, route, timing) | 8 mg Dexamethasone given intravenously prior to operation | |
| (f) Intraoperative fluid management strategy | Fluid maintenance given according to total body fluid loss | |
| (g) types, doses, and routes of anesthetics administrated | Continuous intravenous Rocuronium | |
| (h) patient warming strategy | Warm blanket and intravenous warmer | |
| (i) Management of postoperative fluids | 0.5 mL/kg/h for 6 h | |
| (j) Postoperative analgesic and antiemetic plans | Paracetamol 1 g every 6 h orally, Maxalon 10 mg every 8 h intravenously | |
| (k) plan for opioid minimization | Multimodal oral medicine: paracetamol 1 g every 6 h and Celebrex 200 mg every 12 h | |
| (l) drain and line management | No routine—wound drains | |
| (m) Early mobilization strategy | Enforced to stay out of the bed by postoperative day 1 | |
| (n) postoperative diet and bowel regimen management | Subjects were allowed to consume specially formulated clear fluid (474 mL, 500 kcal, 100 g carbohydrate, and 18 g whey protein) 4 h post-operation (without presence of bowel sound). When they could tolerate at least 500 mL of specially formulated clear fluids with additional other clear fluid, solid diet was permitted. | Subjects were allowed clear fluid once there were bowel sounds. After tolerating clear fluid, they proceeded with nourishing fluid, then soft diet, and they only received a regular solid diet after tolerating the soft diet. |
| (o) criteria for discharge | Optimal pain management orally, able to ambulate independently, adequate nutrition intake, gastrointestinal function return, and without suspicion of complications | |
| (p) tracking of post-discharge outcomes | Follow up in multidisciplinary clinic within 7 days post-discharge. If any emergency before follow up, subjects attended emergency department NCI. | |
| Items | CHO-P | CO |
|---|---|---|
| (a) preadmission patient education regarding the protocol | 100% | 0% |
| (b) preadmission screening and optimization as indicated by nutritional deficiency, anemia, HbA1c, tobacco cessation, and ethanol use | 100% | 50% |
| (c) fasting and carbohydrate loading | 100% | 0% |
| (d) Pre-emptive analgesia (dose, route, timing) | Not applicable | Not applicable |
| (e) Antiemetic prophylaxis (dose, route, timing) | 100% | 100% |
| (f) Intraoperative fluid management strategy | 100% | 100% |
| (g) types, doses and routes of anesthetics administrated | 100% | 100% |
| (h) patient warming strategy | 100% | 100% |
| (i) Management of postoperative fluids | 100% | 100% |
| (j) Postoperative analgesic and antiemetic plans | 100% | 100% |
| (k) plan for opioid minimization | 100% | 100% |
| (l) drain and line management | 100% | 100% |
| (m) Early mobilization strategy | 96.7% | 76.8% |
| (n) postoperative diet and bowel regimen management | 100% | 0% |
| (o) criteria for discharge | 100% | 100% |
| (p) tracking of post-discharge outcomes | 100% | 100% |
| Characteristics | CHO-P (n = 62) | CO (n = 56) |
|---|---|---|
| n (%) | n (%) | |
| Ethnic | ||
| Malay | 46 (55) | 47 (45) |
| Chinese | 10 (45) | 12 (55) |
| Indian | 6 (46) | 7 (54) |
| Diagnosis | ||
| Ovarian cancer | 24 (48) | 26 (52) |
| Endometrial cancer | 22 (55) | 18 (45) |
| Cervical cancer | 13 (62) | 8 (38) |
| Uterine cancer | 3 (43) | 4 (57) |
| Stage | ||
| 1 | 55 (53) | 48 (47) |
| 2 | 3 (50) | 3 (50) |
| 3 | 1 (33) | 2 (67) |
| Advanced | 3 (50) | 3 (50) |
| Family history | ||
| Yes | 21 (48) | 23 (52) |
| No | 41 (55) | 33 (45) |
| ASA score | ||
| 1 (Normal healthy) | 28 (61) | 18 (39) |
| 2 (Mild systemic disease) | 33 (48) | 36 (52) |
| 3 (Severe systemic disease) | 1 (33) | 2 (67) |
| Procedure | ||
| TAHBSO | 37 (48) | 40 (52) |
| Salpingoophrectomy | 16 (67) | 8 (33) |
| Radical Hysterectomy | 6 (55) | 5 (45) |
| Debulking Tumor | 3 (50) | 3 (50) |
| Characteristics | CHO-P (n = 62) Mean ± SD | CO (n = 56) Mean ± SD | p-Value |
|---|---|---|---|
| Age | 49.5 ± 12.2 | 51.2± 11.9 | 0.447 |
| Biochemical Profile | |||
| Serum albumin (g/L) | 39.1 ± 5.3 | 37.3 ± 6.3 | 0.097 |
| CRP (mg/L) | 14.2 ± 26.9 | 24.2 ± 57.5 | 0.238 |
| CAR | 0.4 ± 1.0 | 0.9 ± 2.6 | 0.169 |
| Hemoglobin (g/L) | 11.9 ± 1.5 | 11.6 ± 1.9 | 0.061 |
| Body composition | |||
| Weight (kg) | 63.8 ± 13.3 | 66.4 ± 16.7 | 0.361 |
| BMI (kg/m2) | 26.0 ± 6.0 | 27.2 ± 6.4 | 0.310 |
| Muscle mass (kg) | 37.2 ± 4.1 | 37.4 ± 4.7 | 0.765 |
| Fat mass (kg) | 24.4 ± 9.4 | 26.2 ± 12.9 | 0.383 |
| Fat Free Mass (kg) | 39.5 ± 7.5 | 40.1 ± 5.1 | 0.499 |
| MUAC (cm) | 28.0 ± 4.1 | 28.8 ± 6.0 | 0.403 |
| Weight changes in past 1 month (kg) | −3.1 ± 4.4 | −3.7 ± 5.1 | 0.474 |
| Percentage weight changes in past 1 month (%) | −4.5 ± 6.8 | −5.3 ± 7.2 | 0.472 |
| Nutritional assessment | |||
| PG-SGA score | 6.7 ± 5.2 | 7.0 ± 5.5 | 0.758 |
| Functional status | |||
| Handgrip strength (kg) | 16.7 ± 6.1 | 15.0 ± 6.2 | 0.123 |
| Post-Operative Outcomes | CHO-P (n = 62) Mean ± SD | CO (n = 56) Mean ± SD | t-Value | p-Value |
|---|---|---|---|---|
| LPOHS (h) | 78.13 ± 33.05 | 99.49 ± 22.54 | −4.056 | 0.000 ** |
| LOCF (h) | 10.23 ± 3.42 | 21.89 ± 8.77 | −9.329 | 0.000 ** |
| LOSDT (h) | 22.05 ± 11.70 | 52.90 ± 16.43 | −11.633 | 0.000 ** |
| LOBFR (h) | 28.32 ± 19.06 | 53.10 ± 17.29 | −7.368 | 0.000 ** |
| LOBO (h) | 36.04 ± 21.71 | 68.84 ± 19.09 | −8.678 | 0.000 ** |
| Postoperative Complication | CHO-P (n = 62) | CO (n = 56) | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Postoperative nausea | |||
| Yes | 16 (27) | 44 (73) | 0.000 *** |
| No | 46 (79) | 12 (21) | |
| Postoperative vomiting | |||
| Yes | 11 (24) | 34 (76) | 0.000 *** |
| No | 51 (70) | 22 (30) | |
| Pneumonia | |||
| Yes | 0 (0) | 1 (100) | |
| No | 62 (53) | 55 (47) | |
| Postoperative Ileus | |||
| Yes | 0 (0) | 1 (100) | |
| No | 62 (53) | 55 (47) | |
| Infection | |||
| Yes | 1 (17) | 5 (83) | |
| No | 61 (54) | 51 (46) | |
| Readmission within 30 days post discharged | |||
| Yes | |||
| No | 4 (6) | 9 (16) | 0.031 * |
| 58 (94) | 47 (84) |
| Characteristics | Changes Post-Operation | p-Value | |
|---|---|---|---|
| CHO-P (n = 62) (mean ± SD) | CO (n = 56) (mean ± SD) | ||
| Body composition | |||
| Weight (kg) | −0.3 ± 2.3 | −2.1 ± 2.3 | <0.001 *** |
| BMI (kg/m2) | −0.1 ± 3.5 | −1.2 ± 2.8 | 0.034 * |
| Muscle mass (kg) | 0.4 ± 1.7 | −0.7 ± 2.6 | 0.007 ** |
| FM (kg) | −0.8 ± 2.2 | −1.8 ± 2.0 | 0.010 ** |
| FFM (kg) | −0.3 ± 19.2 | −0.6 ± 2.6 | 0.035 * |
| MUAC (cm) | −1.5 ± 1.2 | −1.9 ± 1.3 | 0.698 |
| Biochemical profile | |||
| Albumin (g/L) | −7.6 ± 4.9 | −9.3 ± 6.1 | 0.110 |
| C-reactive protein (mg/L) | 5.0 ± 33.7 | 22.3 ± 59.8 | 0.050 * |
| CAR | 0.3 ± 1.2 | 1.1 ± 2.6 | 0.030 * |
| Hemoglobin (g/L) | −1.0 ± 1.3 | −0.3 ± 1.9 | 0.018 * |
| Functional status | |||
| Handgrip strength (kg) | 0.6 ± 4.3 | −1.9 ± 4.7 | 0.004 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, H.C.; Ibrahim, Z.; Abu Zaid, Z.; Mat Daud, Z.‘A.; Md. Yusop, N.B.; Omar, J.; Mohd Abas, M.N.; Abdul Rahman, Z.; Jamhuri, N. Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial. Nutrients 2020, 12, 264. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010264
Yi HC, Ibrahim Z, Abu Zaid Z, Mat Daud Z‘A, Md. Yusop NB, Omar J, Mohd Abas MN, Abdul Rahman Z, Jamhuri N. Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial. Nutrients. 2020; 12(1):264. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010264
Chicago/Turabian StyleYi, Ho Chiou, Zuriati Ibrahim, Zalina Abu Zaid, Zulfitri ‘Azuan Mat Daud, Nor Baizura Md. Yusop, Jamil Omar, Mohd Norazam Mohd Abas, Zuwariah Abdul Rahman, and Norshariza Jamhuri. 2020. "Impact of Enhanced Recovery after Surgery with Preoperative Whey Protein-Infused Carbohydrate Loading and Postoperative Early Oral Feeding among Surgical Gynecologic Cancer Patients: An Open-Labelled Randomized Controlled Trial" Nutrients 12, no. 1: 264. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12010264