The Effects of a 12-Month Weight Loss Intervention on Cognitive Outcomes in Adults with Overweight and Obesity

 , ,
, ,
Abstract
:1. Introduction
2. Materials & Methods
2.1. Participants
2.2. Physiological Outcomes Testing
2.2.1. Weight Assessment
2.2.2. Cognitive Assessment
N-Back
Task Switch
Stroop Color-Word Task
Iowa Gambling Task (IGT)
2.2.3. Intervention Groups
Diet-Only (DIET)
Diet + Moderate Exercise (DIET + MODEX)
Diet + High Exercise (DIET + HIGHEX)
2.3. Statistical Analyses
2.3.1. Intervention Effects
2.3.2. Cognitive Effects
3. Results
3.1. Participants
3.2. Missing Data
3.3. Intervention Effects
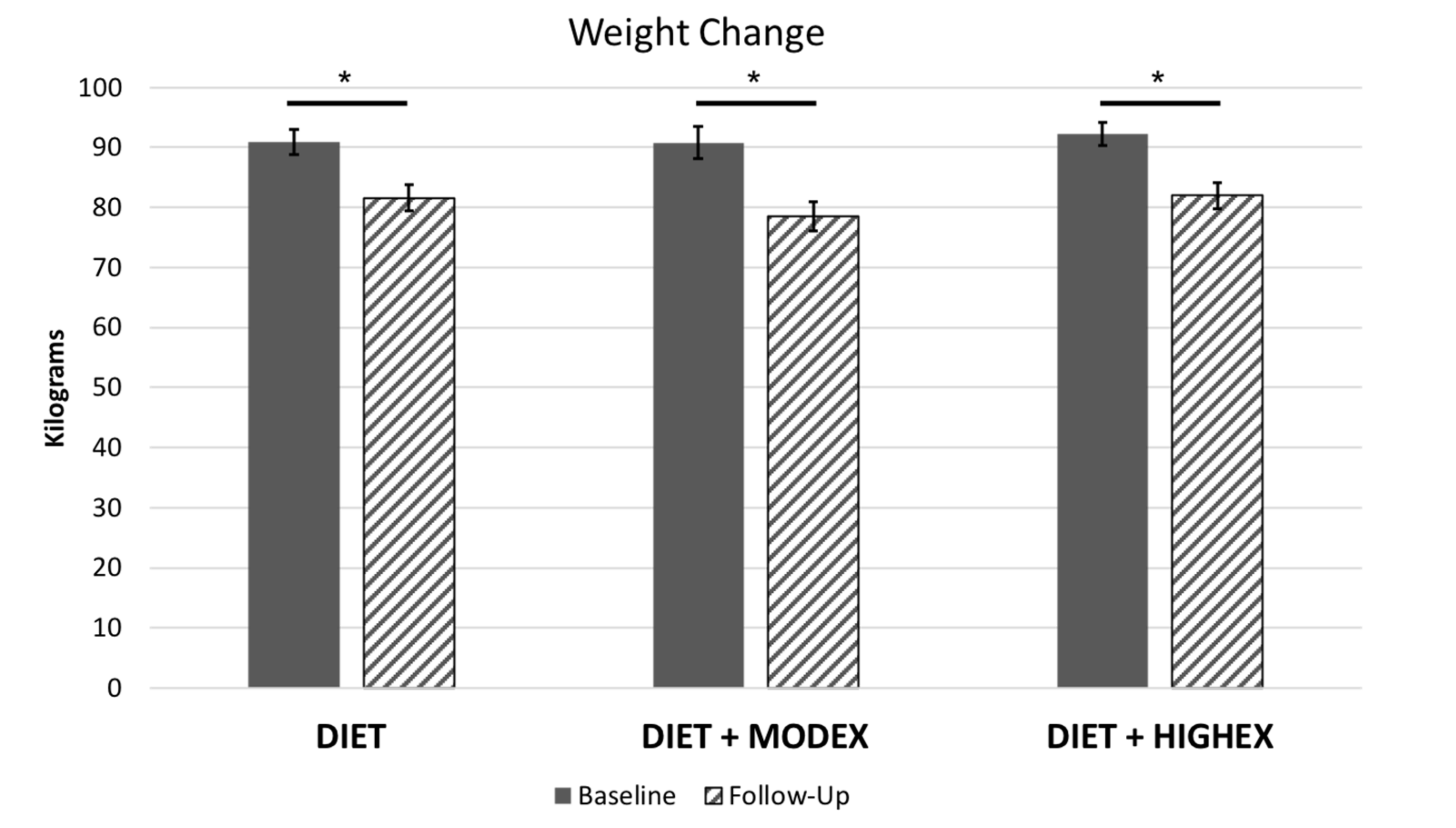
3.3.1. Weight Loss
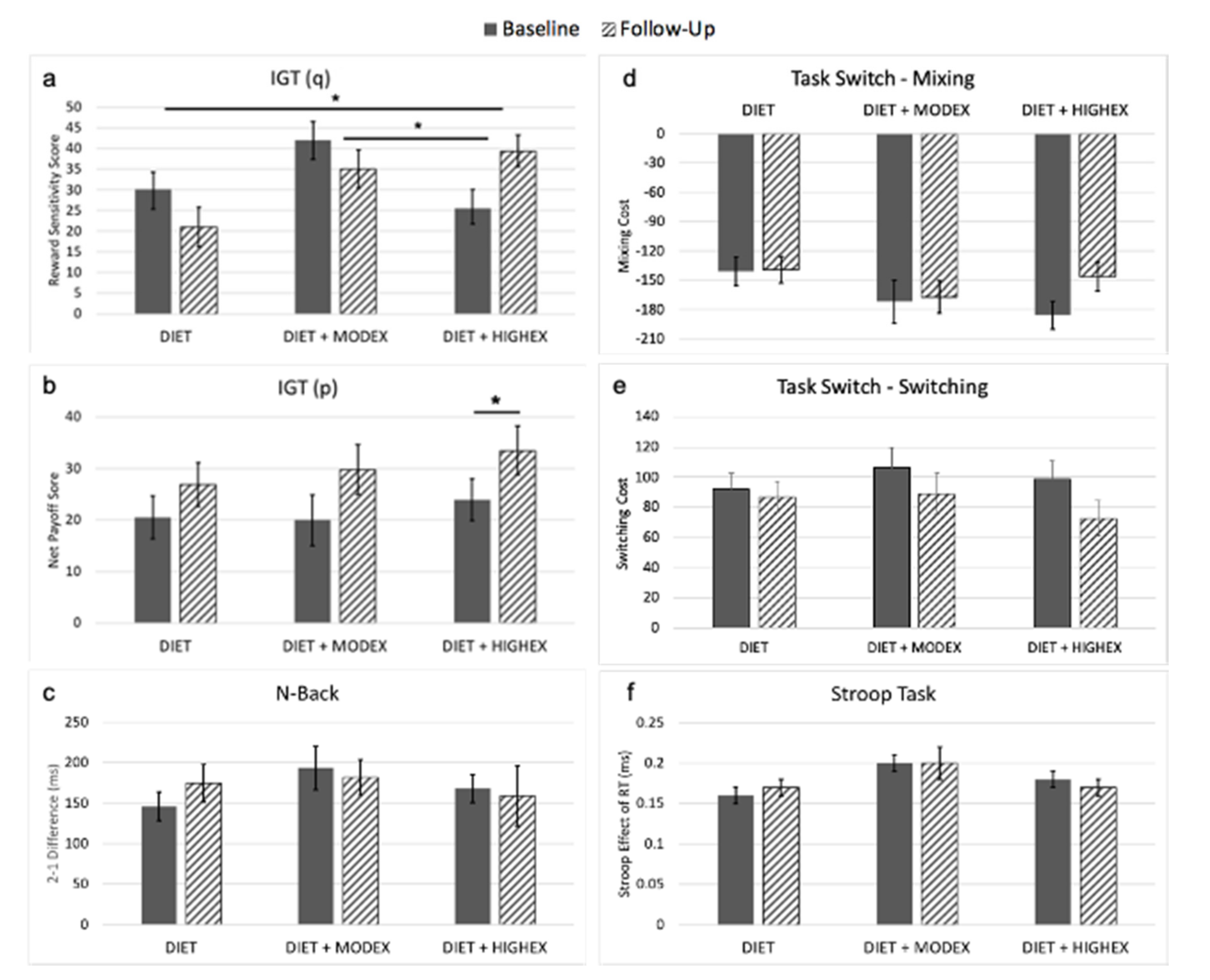
3.3.2. Executive Functioning
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in obesity among adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, M.K.; Joshi, A.V.; Madhavan, S.S.; Amonkar, M.M. Obesity and health-related quality of life: A cross-sectional analysis of the US population. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1227–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schafer, M.H.; Ferraro, K.F. The stigma of obesity: Does perceived weight discrimination affect identity and physical health? Soc. Psychol. Q. 2011, 74, 76–97. [Google Scholar] [CrossRef] [Green Version]
- Prasad, S.; Sajja, R.K.; Naik, P.; Cucullo, L. Diabetes mellitus and blood-brain barrier dysfunction: An Overview. J. Pharmacovigil. 2014, 2, 125. [Google Scholar]
- Smith, E.; Hay, P.; Campbell, L.; Trollor, J.N. A review of the association between obesity and cognitive function across the lifespan: Implications for novel approaches to prevention and treatment. Obes. Rev. 2011, 12, 740–755. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.J.; Telang, F.; Fowler, J.S.; Goldstein, R.Z.; Alia-Klein, N.; Logan, J.; Wong, C.; Thanos, P.K.; Ma, Y.; et al. Inverse association between BMI and prefrontal metabolic activity in healthy adults. Obesity (Silver Spring) 2009, 17, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, S.; Gilbert, S.; Serpell, L. Systematic review: Are overweight and obese individuals impaired on behavioural tasks of executive functioning? Neuropsychol. Rev. 2013, 23, 138–156. [Google Scholar] [CrossRef]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2018, 14, 591–604. [Google Scholar] [CrossRef]
- Dye, L.; Boyle, N.B.; Champ, C.; Lawton, C. The relationship between obesity and cognitive health and decline. Proc. Nutr. Soc. 2017, 76, 443–454. [Google Scholar] [CrossRef] [Green Version]
- Solas, M.; Milagro, F.I.; Ramírez, M.J.; Martínez, A. Inflammation and gut-brain axis link obesity to cognitive dysfunction: Plausible pharmacological interventions. Curr. Opin. Pharmacol. 2017, 37, 87–92. [Google Scholar] [CrossRef]
- Bocarsly, M.E.; Fasolino, M.; Kane, G.A.; LaMarca, E.A.; Kirschen, G.W.; Karatsoreos, I.N.; McEwen, B.S.; Gould, E. Obesity diminishes synaptic markers, alters microglial morphology, and impairs cognitive function. Proc. Natl. Acad. Sci. USA 2015, 112, 15731–15736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellbom, K.S.; Gunstad, J. Cognitive function and decline in obesity. J. Alzheimers Dis. 2012, 30, S89–S95. [Google Scholar] [CrossRef]
- Stice, E.; Yokum, S.; Burger, K.S.; Epstein, L.H.; Small, D.M. Youth at risk for obesity show greater activation of striatal and somatosensory regions to food. J. Neurosci. 2011, 31, 4360–4366. [Google Scholar] [CrossRef] [Green Version]
- Stillman, C.M.; Weinstein, A.M.; Marsland, A.L.; Gianaros, P.J.; Erickson, K.I. Body-brain connections: The effects of obesity and behavioral interventions on neurocognitive aging. Front. Aging Neurosci. 2017, 9, 115. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, E.H.; Charboneau, E.; Dietrich, M.S.; Park, S.; Bradley, B.P.; Mogg, K.; Cowan, R.L. Obese adults have visual attention bias for food cue images: Evidence for altered reward system function. Int. J. Obes. (Lond.) 2009, 33, 1063–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokum, S.; Ng, J.; Stice, E. Attentional bias to food images associated with elevated weight and future weight gain: An fMRI study. Obesity (Silver Spring) 2011, 19, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Ferriday, D.; Brunstrom, J.M. ‘I just can’t help myself’: Effects of food-cue exposure in overweight and lean individuals. Int. J. Obes. (Lond.) 2011, 35, 142–149. [Google Scholar] [CrossRef] [Green Version]
- Opel, N.; Redlich, R.; Grotegerd, D.; Dohm, K.; Haupenthal, C.; Heindel, W.; Kugel, H.; Arolt, V.; Dannlowski, U. Enhanced neural responsiveness to reward associated with obesity in the absence of food-related stimuli. Hum. Brain Mapp. 2015, 36, 2330–2337. [Google Scholar] [CrossRef]
- Stice, E.; Yokum, S. Neural vulnerability factors that increase risk for future weight gain. Psychol. Bull. 2016, 142, 447–471. [Google Scholar] [CrossRef]
- Siervo, M.; Arnold, R.; Wells, J.C.K.; Tagliabue, A.; Colantuoni, A.; Albanese, E.; Brayne, C.; Stephan, B.C.M. Intentional weight loss in overweight and obese individuals and cognitive function: A systematic review and meta-analysis. Obes. Rev. 2011, 12, 968–983. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N.; Sherwood, A. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Facchini, S.; Stubbs, B.; Luchini, C.; Solmi, M.; Manzato, E.; Sergi, G.; Maggi, S.; Cosco, T.; Fontana, L. Weight loss is associated with improvements in cognitive function among overweight and obese people: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 72, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Witbracht, M.G.; Laugero, K.D.; Van Loan, M.D.; Adams, S.H.; Keim, N.L. Performance on the Iowa Gambling Task is related to magnitude of weight loss and salivary cortisol in a diet-induced weight loss intervention in overweight women. Physiol. Behav. 2012, 106, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, R.A.; Roberts, S.B.; Das, S.K.; Gilhooly, C.H.; Golden, J.K.; Hyatt, R.; Lerner, D.; Saltzman, E.; Lieberman, H.R. Long-term effects of provided low and high glycemic load low energy diets on mood and cognition. Physiol. Behav. 2009, 98, 374–379. [Google Scholar] [CrossRef] [Green Version]
- Horie, N.C.; Serrao, V.T.; Simon, S.S.; Gascon, M.R.P.; dos Santos, A.X.; Zambone, M.A.; del Bigio de Freitas, M.M.; Cunha-Neto, E.; Marques, E.L.; Halpern, A.; et al. Cognitive effects of intentional weight loss in elderly obese individuals with mild cognitive impairment. J. Clin. Endocrinol. Metab. 2016, 101, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Baillot, A.; Romain, A.J.; Boisvert-Vigneault, K.; Audet, M.; Baillargeon, J.P.; Dionne, I.J.; Valiquette, L.; Chakra, C.N.A.; Avignon, A.; Langlois, M.F. Effects of lifestyle interventions that include a physical activity component in class II and III obese individuals: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0119017. [Google Scholar] [CrossRef] [Green Version]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Stern, Y.; MacKay-Brandt, A.; Lee, S.; McKinley, P.; McIntyre, K.; Razlighi, Q.; Agarunov, E.; Bartels, M.; Sloan, R.P. Effect of aerobic exercise on cognition in younger adults: A randomized clinical trial. Neurology 2019, 92, e905–e916. [Google Scholar] [CrossRef]
- Wu, T.; Gao, X.; Chen, M.; Van Dam, R.M. Long-term effectiveness of diet-plus-exercise interventions vs. diet-only interventions for weight loss: A meta-analysis. Obes. Rev. 2009, 10, 313–323. [Google Scholar] [CrossRef]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Stillman, C.M.; Jakicic, J.; Rogers, R.; Alfini, A.J.; Smith, J.C.; Watt, J.; Kang, C.; Erickson, K.I. Changes in cerebral perfusion following a 12-month exercise and diet intervention. Psychophysiology 2020, e13589. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.J.; Schelbert, E.B.; Lang, W.; Fridman, Y.; Yuan, N.; Jakicic, J.M. Association of fitness and body fatness with left ventricular mass: The heart health study. Obes. Sci. Pract. 2019, 6, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kray, J.; Lindenberger, U. Adult age differences in task switching. Psychol. Aging 2000, 15, 126–147. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Stocco, A.; Fum, D.; Napoli, A. Dissociable processes underlying decisions in the Iowa Gambling Task: A new integrative framework. Behav. Brain Funct. 2009, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- The 2018 Physical Activity Guidelines Advisory Committee. The Physical Activity Guidelines for Americans, 2nd ed.; The U.S. Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Espeland, M.A.; Rapp, S.R.; Bray, G.A.; Houston, D.K.; Johnson, K.C.; Kitabchi, A.E.; Hergenroeder, A.L.; Williamson, J.; Jakicic, J.M.; van Dorsten, B.; et al. Long-term impact of behavioral weight loss intervention on cognitive function. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1101–1108. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Babyak, M.A.; Craighead, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Strauman, T.A.; Sherwood, A. Effects of the dietary approaches to stop hypertension diet, exercise, and caloric restriction on neurocognition in overweight adults with high blood pressure. Hypertension 2010, 55, 1331–1338. [Google Scholar] [CrossRef]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 2008, 300, 1027–1037. [Google Scholar] [CrossRef] [Green Version]
- Pursey, K.M.; Stanwell, P.; Callister, R.J.; Brain, K.; Collins, C.E.; Burrows, T.L. Neural responses to visual food cues according to weight status: A systematic review of functional magnetic resonance imaging studies. Front. Nutr. 2014, 1, 7. [Google Scholar] [CrossRef]
- Bothe, N. Acute Exercise Influences Reward Processing in Highly Trained and Untrained Men. Ph.D. Thesis, Charité-Universitätsmedizin Berlin, Berlin, Germany, 2013. [Google Scholar]
- Lynch, W.J.; Robinson, A.M.; Abel, J.; Smith, M.A. Exercise as a Prevention for Substance Use Disorder: A Review of Sex Differences and Neurobiological Mechanisms. Curr. Addict. Rep. 2017, 4, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Saanijoki, T.; Nummenmaa, L.; Tuulari, J.J.; Tuominen, L.; Arponen, E.; Kalliokoski, K.K.; Hirvonen, J. Aerobic exercise modulates anticipatory reward processing via the mu-opioid receptor system. Hum. Brain Mapp. 2018, 39, 3972–3983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Rico, E.; Río-Valle, J.S.; Albein-Urios, N.; Caracuel, A.; González-Jiménez, E.; Piqueras, M.J.; Brandi, P.; Ruiz-López, I.M.; García-Rodríguez, I.; Martín-Matillas, M.; et al. Effects of a multicomponent behavioral intervention on impulsivity and cognitive deficits in adolescents with excess weight. Behav. Pharmacol. 2012, 23, 609–615. [Google Scholar] [CrossRef]
- Koritzky, G.; Dieterle, C.; Rice, C.; Jordan, K.; Bechara, A. Decision-making, sensitivity to reward and attrition in weight management. Obesity 2014, 22, 1904–1909. [Google Scholar] [CrossRef]
- Koritzky, G.; Rice, C.; Dieterle, C.; Bechara, A. The biggest loser thinks long-term: Recency as a predictor of success in weight management. Front. Psychol. 2015, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, L.E.; Barnes, D.E.; Lui, L.Y.; Yaffe, K. Physical activity over the life course and its association with cognitive performance and impairment in old age. J. Am. Geriatr. Soc. 2010, 58, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Weuve, J.; Kang, J.H.; Manson, J.E.; Breteler, M.M.B.; Ware, J.H.; Grodstein, F. Physical activity, including walking, and cognitive function in older women. JAMA 2004, 292, 1454–1461. [Google Scholar] [CrossRef] [Green Version]
- Willey, J.Z.; Gardener, H.; Caunca, M.R.; Moon, Y.P.; Dong, C.; Cheung, Y.K.; Sacco, R.L.; Elkind, M.S.V.; Wright, C.B. Leisure-time physical activity associates with cognitive decline: The Northern Manhattan Study. Neurology 2016, 86, 1897–1903. [Google Scholar] [CrossRef] [Green Version]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The aerobic and cognitive exercise study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef]
- Jonasson, L.S.; Nyberg, L.; Kramer, A.F.; Lundquist, A.; Riklund, K.; Boraxbekk, C.J. Aerobic exercise intervention, cognitive performance, and brain structure: Results from the physical influences on brain in aging (PHIBRA) study. Front. Aging Neurosci. 2016, 8, 336. [Google Scholar] [CrossRef]
- Scherder, E.; Scherder, R.; Verburgh, L.; Königs, M.; Blom, M.; Kramer, A.F.; Eggermont, L. Executive functions of sedentary elderly may benefit from walking: A systematic review and meta-analysis. Am. J. Geriatr. Psychiatry 2014, 22, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinilla, F.; Hillman, C. The influence of exercise on cognitive abilities. Compr. Physiol. 2013, 3, 403–428. [Google Scholar] [PubMed] [Green Version]



{kind=link}
{kind=link}
| DIET M (SD) | DIET + MODEX M (SD) | DIET + HIGHEX M (SD) | SIGNIF. | |
|---|---|---|---|---|
| n | 50 | 30 | 45 | |
| Age | 43.26 (8.91) | 45.70 (7.57) | 44.76 (8.88) | 0.443 |
| % Female | 80.0% | 73.3% | 80.0% | 0.746 |
| % White | 72.0% | 70.0% | 75.56% | 0.860 |
| BMI (kg/m2) | 32.55 (3.51) | 32.32 (4.35) | 32.39 (4.15) | 0.965 |
| Weight (kg) | 90.85 (14.74) | 90.82 (14.49) | 92.27 (13.10) | 0.863 |
| Education (years) | 16.22 (2.71) | 16.45 (2.88) | 16.48 (2.78) | 0.882 |
| DIET M (SD) | DIET + MODEX M (SD) | DIET + HIGHEX M (SD) | |
|---|---|---|---|
| IGT Reward Sensitivity (q) * | −9.87 (36.97) | −9.61 (24.56) | 13.98 (31.43) |
| IGT Payoff (p) | 4.61 (31.38) | 8.46 (29.87) | 10.07 (35.17) |
| Task Switch Mixing Cost (RT, ms) | 6.35 (115.39) | 0.76 (114.78) | 33.21 (107.35) |
| Task Switch Switching Cost (RT, ms) | −6.39 (93.90) | −26.71 (91.91) | −35.82 (94.79) |
| N-Back 2-1 (RT, ms) | 27.49 (180.70) | −21.86 (141.92) | −21.51 (225.83) |
| Stroop Effect (RT, ms) | 0.008 (.06) | −0.007 (0.10) | −0.02 (0.08) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peven, J.C.; Jakicic, J.M.; Rogers, R.J.; Lesnovskaya, A.; Erickson, K.I.; Kang, C.; Zhou, X.; Porter, A.; Donofry, S.D.; Watt, J.C.; et al. The Effects of a 12-Month Weight Loss Intervention on Cognitive Outcomes in Adults with Overweight and Obesity. Nutrients 2020, 12, 2988. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102988
Peven JC, Jakicic JM, Rogers RJ, Lesnovskaya A, Erickson KI, Kang C, Zhou X, Porter A, Donofry SD, Watt JC, et al. The Effects of a 12-Month Weight Loss Intervention on Cognitive Outcomes in Adults with Overweight and Obesity. Nutrients. 2020; 12(10):2988. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102988
Chicago/Turabian StylePeven, Jamie C., John M. Jakicic, Renee J. Rogers, Alina Lesnovskaya, Kirk I. Erickson, Chaeryon Kang, Xueping Zhou, Alexis Porter, Shannon D. Donofry, Jennifer C. Watt, and et al. 2020. "The Effects of a 12-Month Weight Loss Intervention on Cognitive Outcomes in Adults with Overweight and Obesity" Nutrients 12, no. 10: 2988. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102988