Effectiveness of Mediterranean Diet’s Adherence in Children with Inflammatory Bowel Diseases

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Anthropometric Data
2.3. Dietary Intake
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Subjects
3.2. Comparison between CD and UC
3.3. Association between Dietary Habits and Markers of Diseaseactivity
3.4. Comparison between IBD Patients and RDA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IBD | Inflammatory Bowel Disease |
| CD | Crohn’s disease |
| UC | Ulcerative colitis |
| HCs | Healthy controls |
| PCDAI | paediatric Crohn’s disease activity index |
| PUCAI | Pediatric Ulcerative Colitis Activity Index |
| MD | Mediterranean Diet |
| RDA | Recommended Daily Allowances |
| ESPGHAN | European Society for Paediatric Gastroenterology, Hepatology and Nutrition |
References
- Lucendo, A.J.; De Rezende, L.C. Importance of nutrition in inflammatory bowel disease. World J. Gastroenterol. 2009, 17, 2081–2088. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakahigashi, M.; Saniabadi, A.R. Review article: Diet and inflammatory bowel disease epidemiology and treatment. Aliment. Pharmacol. Ther. 2009, 2, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Jowett, S.L.; Seal, C.J.; Phillips, E.; Gregory, W.; Barton, J.; Welfare, M.R. Dietary beliefs of people with ulcerative colitis and their effect on relapse and nutrient intake. Clin. Nutr. 2004, 2, 161–170. [Google Scholar] [CrossRef]
- Guerreiro, C.S.; Cravo, M.; Costa, A.R.; Miranda, A.; Tavares, L.; Moura-Santos, P.; MarquesVidal, P.; Leitao, C.N. A comprehensive approach to evaluate nutritionalstatus in Crohn’s patients in the era of biologic therapy: A case-control study. Am. J. Gastroenterol. 2007, 11, 2551–2556. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Martinez-Gonzalez, M.A.; Tong, T.Y.N.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; De Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med 2014, 12, 112. [Google Scholar] [CrossRef] [Green Version]
- Shamir, R.; Phillip, M.; Levine, A. Growth retardation in pediatric Crohn’s disease: Pathogenesis and interventions. Inflamm. Bowel Dis. 2007, 5, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.; Ross, V.; Mahadevan, U. Micronutrient deficiencies in inflammatory bowel disease: From A to zinc. Inflamm. Bowel. Dis. 2012, 10, 1961–1981. [Google Scholar] [CrossRef]
- Mamula, P.; Markowitz, J.; Baldassano, R. Growth Impairment in Pediatric Inflammatory Bowel Disease Title. Pediatric Inflammatory Bowel Diseases; Springer: New York, NY, USA, 2008. [Google Scholar]
- Koletzko, B.; Shamir, R.; Broekaert, I.; Troncone, R. Nutrition in Pediatric Inflammatory Bowel Disease: A Position Paper on Behalf of the Porto Inflammatory Bowel Disease Group of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. 2018, 66, 687–708. [Google Scholar]
- Pons, R.; Whitten, K.E.; Woodhead, H.; Leach, S.T.; Lemberg, D.A.; Day, A.S. Dietary intakes of children with Crohn’s disease. Br. J. Nutr. 2009, 102, 1052–1057. [Google Scholar] [CrossRef] [Green Version]
- Thomas, A.G.; Taylor, F.; Miller, V. Dietary intake and nutritional treatment in childhood Crohn’s disease. J. Pediatr. Gastroenterol. Nutr. 1993, 17, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Marderfeld, L.; Davidson, K.; Mozer-Glassberg, Y.; Poraz, I.; Silbermintz, A.; Zevit, N.; Shamir, R. Food intake adequacy in children and adolescents with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Hagin, S.; Lobato, D.J.; Sands, B.E.; Korzenik, J.; Merrick, M.; Shah, S.; Bancroft, B.; Bright, R.; Law, M.; Moniz, H.; et al. Dietary behaviors in newly diagnosed youth with inflammatory bowel disease. Child Health Care 2017, 46, 408–420. [Google Scholar] [CrossRef]
- Geerling, B.J.; Badart-Smook, A.; Stockbrügger, R.W.; Brummer, R.J. Comprehensive nutritional status in recently diagnosed patients with inflammatory bowel disease compared with population controls. Eur. J. Clin. Nutr. 2000, 54, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappa, H. Health of children and adolescents with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2012, 4, 571. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; De Ridder, L.; Kolho, K.L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. European Society of Pediatric Gastroenterology, Hepatology, and Nutrition. ESPGHAN revised portocriteriafor the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef]
- Kugathasan, S.; Nebel, J.; Skelton, J.A.; Markowitz, J.; Keljo, D.; Rosh, J.; Leleiko, N.; Mack, D.; Griffiths, A.; Bousvaros, A.; et al. Body mass index in children with newly diagnosed inflammatory bowel disease: Observations from two multicenter North American inception cohorts. J. Pediatr. 2007, 151, 523–527. [Google Scholar] [CrossRef]
- Long, M.D.; Crandall, W.V.; Leibowitz, I.H.; Duffy, L.; Del Rosario, F.; Kim, S.C.; Integlia, M.J.; Berman, J.; Grunow, J.; Colletti, R.B.; et al. Prevalence and epidemiology of overweight and obesity in children with inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 2162–2168. [Google Scholar] [CrossRef] [Green Version]
- Farmer, R.G.; Hawk, W.A.; Turnbull, R.B. Clinical patterns in Crohn’s disease: A statistical study of 615 cases. Gastroenterology 1975, 68, 627–635. [Google Scholar] [CrossRef]
- Mekhjian, H.S.; Switz, D.M.; Melnyk, C.S.; Rankin, G.B.; Brooks, R.K. Clinical features and natural history of Crohn’s disease. Gastroenterology 1979, 77, 898–906. [Google Scholar] [CrossRef]
- Filippi, J.; Al-Jaouni, R.; Wiroth, J.B.; Hébuterne, X.; Schneider, S.M. Nutritional Deficiencies in Patients WithCrohn’s Disease in Remission. Inflamm. Bowel Dis. 2006, 3, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Diederen, K.; Krom, H.; Koole, J.C.; Benninga, M.A.; Kindermann, A. Diet and Anthropometrics of Children with Inflammatory Bowel Disease: A Comparison with the General Population. Inflamm. Bowel Dis. 2018, 8, 1632–1640. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.; Paerregaard, A.; Faerk, J.; Kramer, I.; Czernia-Mazurkiewicz, J.; Wewer, V.; Munkholm, P.; Lange, A.; Andersen, J.; Jakobsen, M. Pediatric inflammatory bowel disease: Increasing incidence, decreasing surgery rate, and compromised nutritional status: A prospective population-based cohort study 2007–2009. Inflamm. Bowel. Dis. 2011, 17, 2541–2550. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease, 2nd ed.; Coulston, A.M., Boushey, C., Eds.; Academic Press: San Diego, CA, USA, 2008. [Google Scholar]
- Shatenstein, B.; Amre, D.; Jabbour, M. Examining there lativevalidity of an adult food frequency questionnaire in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2010, 5, 645–652. [Google Scholar] [CrossRef]
- Bertoli, S.; Petroni, M.L.; Pagliato, E.; Mora, S.; Weber, G.; Chiumello, G.; Testolin, G. Validation of food frequency questionnaire for assessing dietary macronutrients and calcium intake in Italian children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.B.; Obarzanek, E.; Morrison, J.; Sabry, Z. Comparative advantage of 3-day food records over 24-hour recall and 5-day food frequency validated by observation of 9- and 10-year-old girls. J. Am. Diet. Assoc. 1994, 6, 626–630. [Google Scholar] [CrossRef]
- Calder, P.C.; Albers, R.; Antoine, J.-M.; Blum, S.; Bourdet-Sicard, R.; Ferns, G.A.; Folkerts, G.; Friedmann, P.S.; Frost, G.S.; Guarner, F.; et al. Inflammatory disease processes and interactions with nutrition. Br. J. Nutr. 2009, 101, S1–S45. [Google Scholar] [CrossRef] [Green Version]
- Holt, E.M.; Steffen, L.M.; Moran, A.; Basu, S.; Steinberger, J.; Ross, J.A.; Hong, C.-P.; Sinaiko, A.R. Fruit and vegetable consumption and its relation to markers of inflammation and oxidative stress in adolescents. J. Am. Diet. Assoc. 2009, 3, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Qureshi, M.M.; Singer, M.R.; Moore, L.L. A cross-sectional study of food group intake and Creactive protein among children. Nutr. Metab. 2009, 6, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R. Anti-inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Hébert, J.R.; Shivappa, N.; Tabung, F.K.; Steck, S.E.; Wirth, M.D.; Hurley, T.G. The dietary inflammatory index: A new tool for assessing diet quality based on inflammatory potential. Digest 2014, 49, 1–9. [Google Scholar]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.K.; Abraham, B.; El-Serag, H. Dietary intake and risk of developing inflammatory bowel disease: A systematic review of the literature. Am. J. Gastroenterol. 2011, 106, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Strisciuglio, C.; Giugliano, F.P.; Martinelli, M.; Cenni, S.; Greco, L.; Staiano, A.; Miele, E. Impact of Environmental and Familial Factors in a Cohort of Pediatric Patients with Inflammatory Bowel Disease. J Pediatr. Gastroenterol. Nutr. 2017, 4, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Chicco, F.; Magrì, S.; Cingolani, A.; Paduano, D.; Pesenti, M.; Zara, F.; Tumbarello, F.; Urru, E.; Melis, A.; Casula, L.; et al. Multidimensional Impact of Mediterranean Diet on IBD Patients. Inflamm. Bowel Dis. 2020, 22, 97. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.; Almutairdi, A.; Shommu, N.; Fedorak, R.N.; Ghosh, S.; Reimer, R.A.; Panaccione, R.; Raman, M. Cross-Sectional Analysis of Overall Dietary Intake and Mediterranean Dietary Pattern in Patients WithCrohn’s Disease. Nutrients 2018, 11, 1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, C.; Eliakim, R.; Shamir, R. Nutritional status and nutritional therapy in inflammatory bowel diseases. World J. Gastroenterol. 2009, 21, 2570–2578. [Google Scholar] [CrossRef]
- Boot, A.M.; Bouquet, J.; Krenning, E.P.; Keizer-Schrama, S.M.P.F.D. Bone mineral density and nutritional status in children with chronic inflammatory bowel disease. Gute 1998, 2, 188–194. [Google Scholar] [CrossRef]
- Conklin, L.S.; Oliva-Hemker, M. Nutritional considerations in pediatric inflammatory bowel disease. Expert Rev. Gastroenterol. Hepatol. 2010, 3, 305–317. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | IBD | HCs | p |
|---|---|---|---|
| n = 125 | n = 125 | ||
| Age in years, Median (range) | 15 (5–17) | 14 (5–17) | 0.312 |
| Gender, n (%) | 1 | ||
| Male | 68 (54.4) | 67 (53.6) | |
| Female | 57 (45.6) | 58 (46.4) | |
| Disease, n (%) | NA | ||
| CD | 53 (42.4) | ||
| UC | 72 (57.6) | ||
| PCDAI/PUCAI (median, range) | 0 (0–15) | NA | |
| Paris classification at diagnosis, n (%) | NA | ||
| CD | |||
| Ileum only (L1) | |||
| Colon only (L2) | 13 (24.5) | ||
| Ileum and colon (L3) | 5 (9.4) | ||
| Upper gastrointestinal tract (L4) | 31 (58.5) | ||
| 3 (5.6) | |||
| UC | |||
| Ulcerative proctitis (E1) | |||
| Left-sided UC (E2) | 9(12.5) | ||
| Extensive UC (E3) | 12(16.6) | ||
| Pancolitis (E4) | 13(18) | ||
| 38(52.7) | |||
| Therapy, n (%) | NA | ||
| 5-ASA | 60(48) | ||
| Immunomodulators (AZA, MTX) | 47(37.6) | ||
| Anti-TNFα (IFX, ADA) | 14(11.2) | ||
| Vedolizumab | 1(0.8) | ||
| None | 3(2.4) | ||
| Weight zscores, mean (±SEM) | 0.15 ± 0.11 | 0.15 ± 0.09 | 0.9865 |
| Height z scores, mean (±SEM) | −0.12 ± 0.10 | −0.14 ± 0.12 | 0.9344 |
| BMI z scores, mean (±SEM) | 0.18 ± 0.11 | 0.35 ± 0.09 | 0.2427 |
| Characteristics | IBD | HCs | p |
|---|---|---|---|
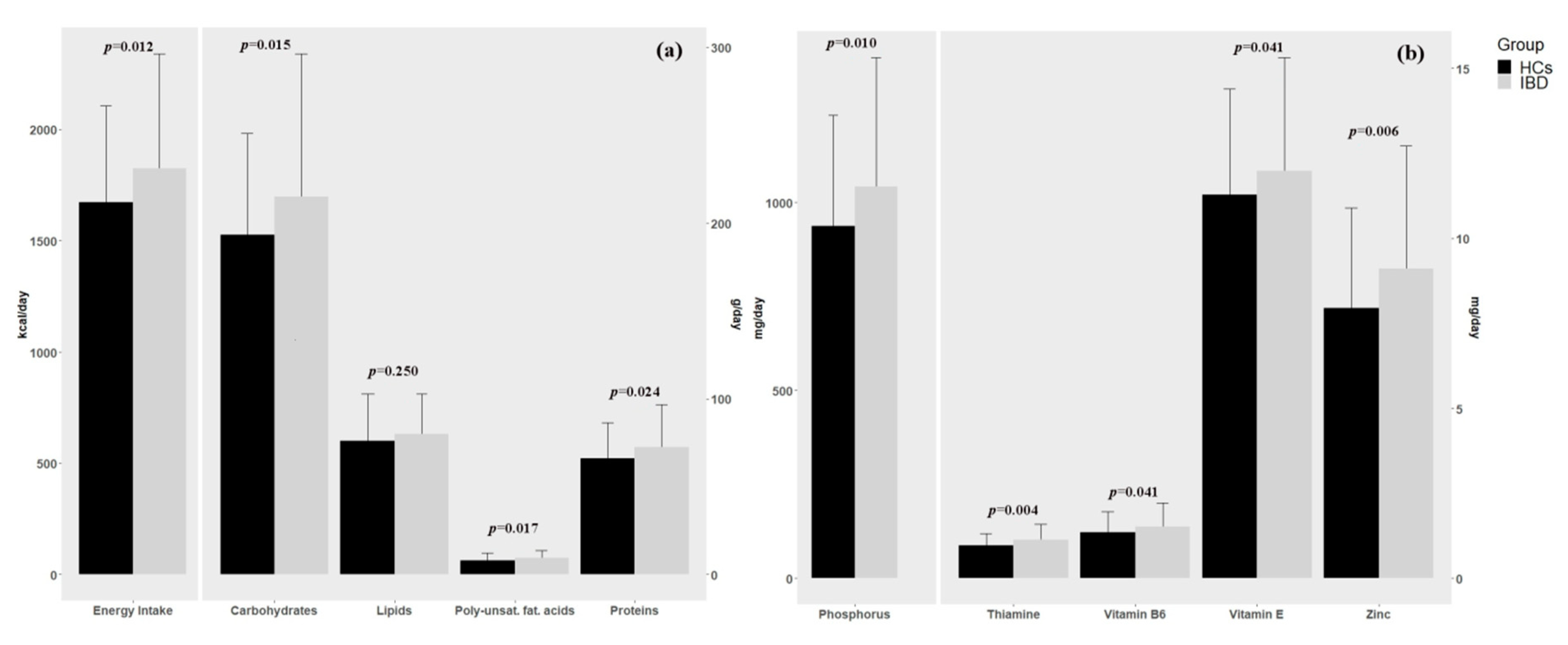
| Energy Intake (kcal/day), mean (±SEM) | 1825.25 ± 46.12 | 1673.15 ± 38.74 | 0.0122 |
| Macronutrients, mean (±SEM) | |||
| Total protein (g/day) | 72.52 ± 2.17 | 66.09 ± 1.82 | 0.024 |
| Lipids (g/day) | 79.83 ± 2.05 | 76.22 ± 2.37 | 0.25 |
| Carbohydrates (g/day) | 215.00 ± 7.29 | 193.17 ± 5.19 | 0.0154 |
| Starch (g/day) | 137.47 ± 5.14 | 127.48 ± 3.95 | 0.1248 |
| Oligosaccharides (g/day) | 42.12 ± 2.14 | 42.23 ± 1.61 | 0.9692 |
| Cholesterol (mg/day) | 205.62 ± 10.41 | 194.03 ± 10.40 | 0.4317 |
| Saturated fatty acids (g/day) | 20.5 ± 0.77 | 20.34 ± 0.84 | 0.909 |
| Poly-unsaturated fatty acids (g/day) | 9.36 ± 0.38 | 8.09 ± 0.36 | 0.0167 |
| Fiber (g/die) | 13.61 ± 0.55 | 13.46 ± 0.43 | 0.8324 |
| Micronutrients, mean (±SEM) | |||
| Calcium (mg/day) | 446.05 ± 20.43 | 414.71 ± 17.05 | 0.24 |
| Sodium (mg/day) | 1633.40 ± 105.47 | 1390.46 ± 88.53 | 0.789 |
| Potassium (mg/day) | 2012.89 ± 58.56 | 1882.94 ± 51.02 | 0.0956 |
| Phosphorus (mg/day) | 1041,65 ± 30.78 | 936.69 ± 26.40 | 0.0102 |
| Iron (mg/day) | 9.4 ± 0.31 | 8.65 ± 0.25 | 0.067 |
| Zinc (mg/day) | 9.10 ± 0.32 | 7.94 ± 0.26 | 0.0058 |
| Folic Acid (mcg/dy) | 183.15 ± 8.27 | 186.21 ± 8.04 | 0.791 |
| Niacin (mg/day) | 15.8 ± 0.67 | 14.24 ± 0.57 | 0.07 |
| Riboflavin (mg/day) | 1.67 ± 0.18 | 1.27 ± 0.12 | 0.052 |
| Thiamine (mg/day) | 1.12 ± 0.04 | 0.97 ± 0.03 | 0.0041 |
| Vitamin A (mcg/day) | 438.5 ± 31.97 | 451.15 ± 33.84 | 0.787 |
| Vitamin B6(mg/day) | 1.5 ± 0.06 | 1.4 ± 0.05 | 0.041 |
| Vitamin C (mg/day) | 71.89 ± 6.05 | 66.75 ± 5.80 | 0.5398 |
| Vitamin D (mcg/day) | 6.49 ± 1.39 | 2.78 ± 0.30 | 0.132 |
| Vitamin E (mg/day) | 11.99 ± 0.30 | 11.28 ± 0.28 | 0.041 |
| KIDMED score, n (%) | 0.7664 | ||
| Optimal | 20 (16.1%) | 17 (15.6%) | |
| Intermediate | 71 (56.9%) | 67 (61.5%) | |
| Low | 33 (26.6%) | 25 (22.9%) | |
| Characteristics | CD | UC | p |
|---|---|---|---|
| (n = 53) | (n = 72) | ||
| Sex | 0.0037 | ||
| Male n, (%) | 37 (69.8%) | 31 (43.1%) | |
| Femalen, (%) | 16 (30.2%) | 41 (56.9%) | |
| Age mean (sd) | 14.77 ± 0.30 | 14.17 ± 0.37 | 0.2263 |
| Weight z-score, mean (±SEM) | 0.07 ± 0.13 | 0.21 ± 0.16 | 0.276 |
| Height z-score, mean (±SEM) | −0.21 ± 0.14 | -0.06 ± 0.15 | 0.342 |
| BMI z-score, mean (±SEM) | 0.11 ± 0.15 | 0.23 ± 0.16 | 0.367 |
| KIDMED score, n (%) | 0.5183 | ||
| Low | 15 (28.3%) | 18 (25.4%) | |
| Intermediate | 32 (60.4%) | 39 (54.9%) | |
| Optimal | 6 (11.3%) | 14 (19.7%) | |
| KIDMED, mean (±SEM) | 4.87 ± 0.30 | 5.35 ± 0.27 | 0.384 |
| Dietary intake, mean (±SEM) | |||
| Energy Intake (kcal/day) | 1942.14 ± 65.80 | 1739.20 ± 62.20 | 0.225 |
| Protein (g/day) | 80.10 ± 3.20 | 66.93 ± 2.78 | 0.047 |
| Lipids (g/day) | 83.42 ± 3.29 | 77.20 ± 2.58 | 0.428 |
| Carbohydrates (g/day) | 230.60 ± 10.29 | 203.52 ± 9.98 | 0.283 |
| Starch (g/day) | 144.57 ± 6.60 | 132.24 ± 7.46 | 0.702 |
| Oligosaccharides (g/day) | 40.94 ± 3.46 | 42.99 ± 2.72 | 0.534 |
| Fiber (g/die) | 13.70 ± 0.81 | 13.54 ± 0.75 | 0.658 |
| Cholesterol (mg/day) | 221.11 ± 12.22 | 194.21 ± 15.62 | 0.436 |
| Saturated fatty acids (g/day) | 21.54 ± 1.13 | 19.68 ± 1.03 | 0.599 |
| Poly-unsaturated fatty acids (g/day) | 10.03 ± 0.63 | 8.86 ± 0.47 | 0.602 |
| Calcium (mg/day) | 465.91 ± 32.61 | 431.42 ± 26.16 | 0.677 |
| Sodium (mg/day) | 1744.70 ± 164.15 | 1551.47 ± 137.77 | 0.733 |
| Potassium (mg/day) | 2109.42 ± 64.70 | 1941.84 ± 79.77 | 0.584 |
| Phosphorus (mg/day) | 1108.34 ± 47.66 | 992.56 ± 39.89 | 0.47 |
| Iron (mg/day) | 10.52 ± 0.49 | 8.54 ± 0.37 | 0.023 |
| Zinc (mg/day) | 9.83 ± 0.54 | 8.56 ± 0.38 | 0.37 |
| Folic Acid (mcg/day) | 194.42 ± 12.35 | 174.86 ± 11.10 | 0.554 |
| Niacin (mg/day) | 17.80 ± 1.04 | 14.38 ± 0.84 | 0.103 |
| Riboflavin (mg/day) | 1.83 ± 0.25 | 1.54 ± 0.24 | 0.834 |
| Thiamine (mg/day) | 1.23 ± 0.07 | 1.04 ± 0.05 | 0.15 |
| Vitamin A (mcg/day) | 439.99 ± 54.74 | 437.42 ± 38.45 | 0.949 |
| Vitamin B6 (mg/day) | 1.72 ± 0.11 | 1.38 ± 0.07 | 0.084 |
| Vitamin C (mg/day) | 73.89 ± 9.97 | 70.42 ± 7.57 | 0.906 |
| Vitamin D (mcg/day) | 10.80 ± 2.96 | 3.32 ± 0.92 | 0.044 |
| Vitamin E (mg/day) | 12.55 ± 0.52 | 11.57 ± 0.34 | 0.243 |
| Nutrient | Sex | Age (y) | Median (Q1;Q2) | Reference Value | p-Value |
|---|---|---|---|---|---|
| Energy intake (kcal/day) | M | 13 | 2061 (1562;2106) | 2780 | 0.031 |
| M | 14 | 2043 (1550;2200) | 2960 | 0.002 | |
| M | 15 | 1939 (1469;2317) | 3110 | 0.004 | |
| M | 16 | 2005 (1700;2598) | 3210 | <0.001 | |
| M | 17 | 1870 (1602;2172) | 3260 | <0.001 | |
| F | 13 | 1621 (1120;1731) | 2780 | 0.062 | |
| F | 14 | 1724 (1137;1957) | 2960 | 0.004 | |
| F | 15 | 1470 (1216;1681) | 3110 | 0.008 | |
| F | 16 | 1321 (1289;1484) | 3210 | 0.004 | |
| F | 17 | 1645 (1430;1779) | 3260 | <0.001 | |
| Mean (±SEM) | |||||
| Lipids (%kcal) | / | / | 39.75 (±6.52) | 40 | 0.670 |
| Carbohydrates (%kcal) | / | / | 46.49 (±7.77) | 52.5 | <0.001 |
| Fiber (g/day) | / | / | 7.56 (±3.19) | 8.4 | 0.004 |
| Proteins (g/day) | M | 11–14 | 84.67 (±26.94) | 48 | <0.001 |
| M | 15–17 | 82.99 (±25.48) | 62 | <0.001 | |
| F | 11–14 | 62.09 (±17.57) | 48 | 0.003 | |
| F | 15–17 | 60.18 (±16.51) | 50 | 0.001 | |
| Calcium (mg/day) | M | 11–17 | 480.66 (±225.74) | 1300 | <0.001 |
| F | 11–14 | 428.38 (±152.07) | 1300 | <0.001 | |
| F | 15–17 | 375.25 (±214.89) | 1200 | <0.001 | |
| Sodium (mg/day) | M | 11–17 | 1762.59 (±1243.83) | 1500 | 0.104 |
| F | 11–17 | 1390.91 (±1023.79) | 1500 | 0.450 | |
| Potassium (mg/day) | M | 11–17 | 2217.43 (±617.67) | 3900 | <0.001 |
| F | 11–17 | 1804.27 (±638.41) | 3900 | <0.001 | |
| Phosphorus (mg/day) | M | 11–17 | 1201.52 (±367.08) | 1250 | 0.306 |
| F | 11–17 | 872.99 (±233.07) | 1250 | <0.001 | |
| Iron (mg/day) | M | 11–14 | 10.19 (±3.91) | 10 | 0.829 |
| M | 15–17 | 34.68 (±151.22) | 13 | 0.364 | |
| F | 11–17 | 7.96 (±2.66) | 18 | <0.001 | |
| Zinc (mg/day) | M | 11–17 | 10.45 (±3.65) | 12 | 0.002 |
| F | 11–17 | 7.59 (±2.90) | 9 | 0.001 | |
| Folic Acid (mcg/day) | M | 11–14 | 211.58 (±114.62) | 350 | <0.001 |
| M | 15–17 | 194.69 (±81.68) | 400 | <0.001 | |
| F | 11–14 | 192.03 (±90.83) | 350 | <0.001 | |
| F | 15–17 | 148.61 (±70.33) | 400 | <0.001 | |
| Niacin (mg/day) | M | 11–14 | 18.54 (±8.48) | 17 | 0.426 |
| M | 15–17 | 23.30 (±30.61) | 18 | 0.274 | |
| F | 11–14 | 14.26 (±5.50) | 17 | 0.044 | |
| F | 15–17 | 12.64 (±5.33) | 18 | <0.001 | |
| Riboflavin (mg/day) | M | 11–14 | 1.52 (±0.69) | 1.3 | 0.167 |
| M | 15–17 | 2.26 (±2.77) | 1.6 | 0.134 | |
| F | 11–14 | 1.30 (±1.21) | 1.2 | 0.733 | |
| F | 15–17 | 1.21 (±1.40) | 1.3 | 0.731 | |
| Thiamine (mg/day) | M | 11–14 | 1.17 (±0.37) | 1.1 | 0.424 |
| M | 15–17 | 1.32 (±0.54) | 1.2 | 0.177 | |
| F | 11–14 | 1.04 (±0.33) | 1 | 0.618 | |
| F | 15–17 | 0.92 (±0.36) | 1.1 | 0.007 | |
| Vitamin A (mcg/day) | M | 11–14 | 432.75 (±268.55) | 600 | 0.012 |
| M | 15–17 | 429.08 (±369.89) | 700 | <0.001 | |
| F | 11–17 | 531 (±838.91) | 600 | 0.561 | |
| Vitamin B6 (mg/day) | M | 11–14 | 1.78 (±0.87) | 1.2 | 0.008 |
| M | 15–17 | 11.42 (±61.54) | 1.3 | 0.299 | |
| F | 11–14 | 1.32 (±0.42) | 1.2 | 0.218 | |
| F | 15–17 | 1.20 (±0.43) | 1.3 | 0.210 | |
| Vitamin C (mg/day) | M | 11–14 | 87.53 (±97.42) | 90 | 0.911 |
| M | 15–17 | 62.09 (±47.79) | 105 | <0.001 | |
| F | 11–14 | 88.17 (±83.41) | 80 | 0.674 | |
| F | 15–17 | 59.79 (±54.11) | 85 | 0.013 | |
| Vitamin D (mcg/day) | / | / | 6.49 (±15.59) | 15 | <0.001 |
| Vitamin E (mg/day) | M | 11–14 | 12.90 (±3.59) | 11 | 0.028 |
| M | 15–17 | 12.19 (±3.40) | 13 | 0.134 | |
| F | 11–14 | 11.96 (±2.73) | 11 | 0.143 | |
| F | 15–17 | 10.83 (±2.00) | 12 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strisciuglio, C.; Cenni, S.; Serra, M.R.; Dolce, P.; Martinelli, M.; Staiano, A.; Miele, E. Effectiveness of Mediterranean Diet’s Adherence in Children with Inflammatory Bowel Diseases. Nutrients 2020, 12, 3206. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103206
Strisciuglio C, Cenni S, Serra MR, Dolce P, Martinelli M, Staiano A, Miele E. Effectiveness of Mediterranean Diet’s Adherence in Children with Inflammatory Bowel Diseases. Nutrients. 2020; 12(10):3206. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103206
Chicago/Turabian StyleStrisciuglio, Caterina, Sabrina Cenni, Maria Rosaria Serra, Pasquale Dolce, Massimo Martinelli, Annamaria Staiano, and Erasmo Miele. 2020. "Effectiveness of Mediterranean Diet’s Adherence in Children with Inflammatory Bowel Diseases" Nutrients 12, no. 10: 3206. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103206