Eating Competence Associated with Food Consumption and Health Outcomes among Brazilian Adult Population


 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
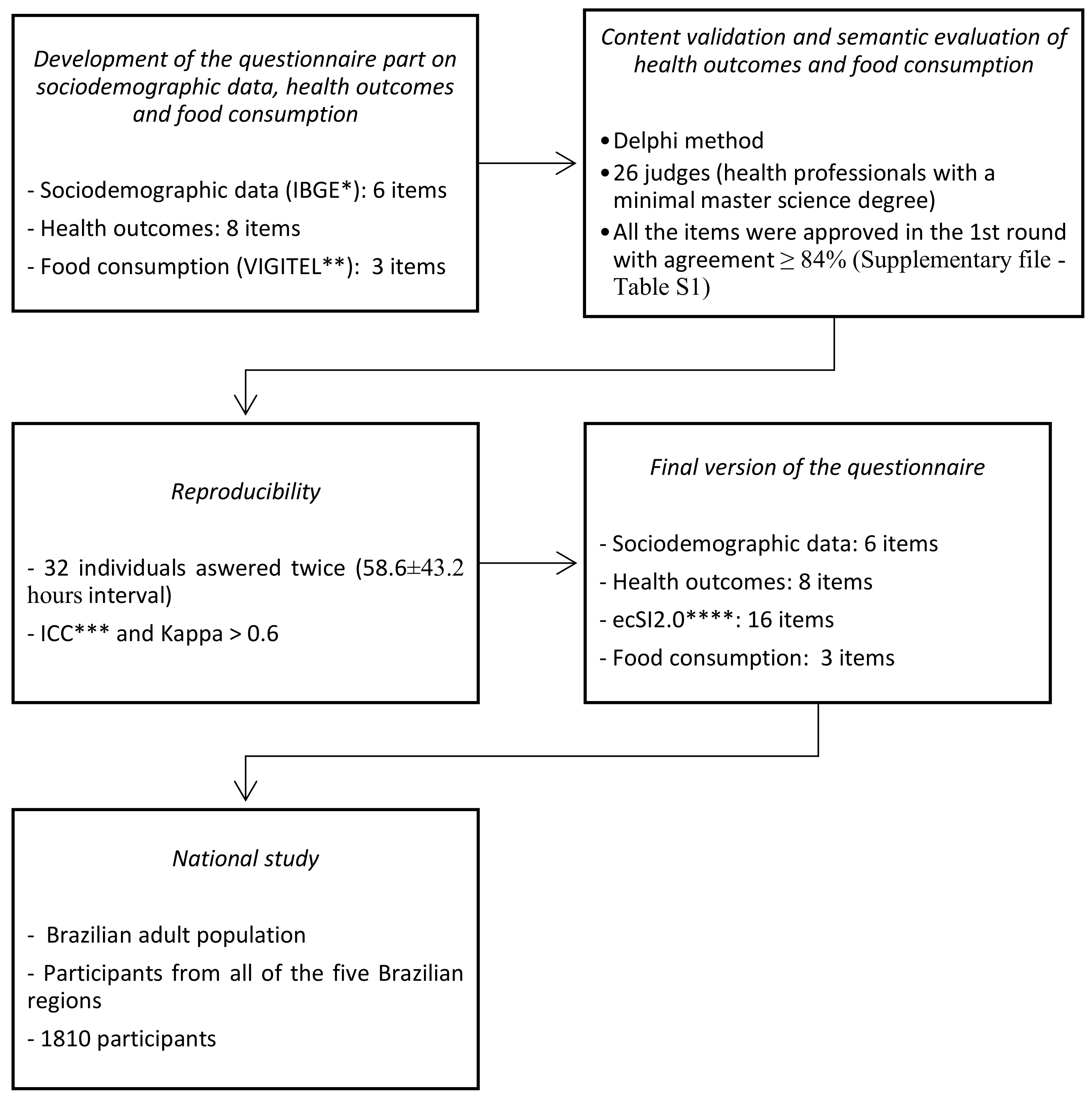
2.1. Development of a Questionnaire Regarding Sociodemographic Data, Health Outcomes, and Food Consumption
2.2. National Study to Associate EC with Food Consumption and Health Outcomes in the Brazilian Population
2.3. Statistical Analysis
3. Results
Questionnaire in the Brazilian Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Brazilian-Portuguese Questionnaire
- Parte 1: Dados sociodemográficos
- Qual o seu gênero?
- ○
- Feminino
- ○
- Masculino
- Qual a sua idade? (em anos)
- Em que estado brasileiro você mora?
- Qual é a sua escolaridade?
- ○
- Sem instrução
- ○
- Fundamental incompleto
- ○
- Fundamental completo
- ○
- Médio incompleto
- ○
- Médio completo
- ○
- Superior incompleto
- ○
- Superior completo
- ○
- Pós graduação
- Qual é a sua renda familiar média mensal? (em reais)
- ○
- 1,00 a 500,00
- ○
- 501,00 a 1.000,00
- ○
- 1.001,00 a 2.000,00
- ○
- 2.001,00 a 3.000,00
- ○
- 3.001,00 a 5.000,00
- ○
- 5.001,00 a 10.000,00
- ○
- 10.001,00 a 20.000,00
- ○
- 20.001,00 a 100.000
- ○
- 100.001 ou mais
- Parte 2: Dados de saúde
- Quantos quilos você pesa? Se você não sabe, por favor coloque um valor aproximado.
- Qual é a sua altura? Se você não sabe, por favor coloque um valor aproximado.
- Em relação ao seu peso você acha que:
- ○
- Está acima do peso
- ○
- Está abaixo do peso
- ○
- Está bem com o peso atual
- Você tem diabetes?
- ○
- Sim
- ○
- Não
- Caso tenha respondido SIM, como você trata a diabetes?
- ○
- Com remédio (comprimidos e/ ou insulina)
- ○
- Com dieta
- ○
- Com remédios (comprimidos e/ ou insulina) E dieta
- Você tem pressão alta (hipertensão)?
- ○
- Sim
- ○
- Não
- Caso tenha respondido SIM, como você trata a pressão alta (hipertensão)?
- ○
- Com remédio
- ○
- Com dieta
- ○
- Com remédio E dieta
- Parte 3: Inventário de Competências Alimentares (ecSI2.0™BR)
- Parte 4: Consumo de Alimentos
- Em quantos dias da semana você costuma comer frutas?
- ○
- 1 a 2 dias por semana
- ○
- 3 a 4 dias por semana
- ○
- 5 a 6 dias por semana
- ○
- Todos os dias incluindo sábado e domingo
- ○
- Quase nunca como frutas
- ○
- Nunca como frutas
- Em quantos dias da semana você costuma comer pelo menos um tipo de verdura ou legume (ex: tomate, alface, couve, cenoura, chuchu, beterraba, abobrinha, berinjela - não vale batata, mandioca ou inhame)?
- ○
- 1 a 2 dias por semana
- ○
- 3 a 4 dias por semana
- ○
- 5 a 6 dias por semana
- ○
- Todos os dias incluindo sábado e domingo
- ○
- Quase nunca como verdura ou legume
- ○
- Nunca como verdura ou legume
- Em quantos dias da semana você costuma beber refrigerante ou suco artificial (caixinha, garrafa ou em pó)?
- ○
- 1 a 2 dias por semana
- ○
- 3 a 4 dias por semana
- ○
- 5 a 6 dias por semana
- ○
- Todos os dias incluindo sábado e domingo
- ○
- Quase nunca bebo refrigerante ou suco artificial
- ○
- Nunca bebo refrigerante ou suco artificial
References
- Satter, E. Eating Competence: Definition and Evidence for the Satter Eating Competence Model. J. Nutr. Educ. Behav. 2007, 39, S142–S153. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Bailey, R.L.; Krall, J.S.; Wall, D.E.; Mitchell, D.C. Diet quality is related to eating competence in cross-sectional sample of low-income females surveyed in Pennsylvania. Appetite 2012, 58, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Psota, T.; Zazpe, I.; Sorli, V.; Salas-salvado, J.; Ros, E. Eating Competence of Elderly Spanish Adults Is Associated with a Healthy Diet and a Favorable Cardiovascular Disease Risk Profile 1–3. J. Nutr. 2010, 140, 1322–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohse, B.; Cunningham-Sabo, L. Eating Competence of Hispanic Parents Is Associated with Attitudes and Behaviors That May Mediate Fruit and Vegetable-Related Behaviors of 4th Grade Youth. J. Nutr. 2012, 142, 1903–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tylka, T.L.; Eneli, I.U.; Kroon Van Diest, A.M.; Lumeng, J.C. Which adaptive maternal eating behaviors predict child feeding practices? An examination with mothers of 2- to 5-year-old children. Eat. Behav. 2013, 14, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohse, B.; Satter, E.; Horacek, T.; Gebreselassie, T.; Oakland, M.J. Measuring Eating Competence: Psychometric Properties and Validity of the ecSatter Inventory. J. Nutr. Educ. Behav. 2007, 39, S154–S166. [Google Scholar] [CrossRef] [PubMed]
- Krall, J.S.; Lohse, B. Validation of a measure of the Satter eating competence model with low-income females. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Brown, L.B.; Larsen, K.J.; Nyland, N.K.; Eggett, D.L. Eating competence of college students in an introductory nutrition course. J. Nutr. Educ. Behav. 2013, 45, 269–273. [Google Scholar] [CrossRef]
- Clifford, D.; Keeler, L.A.; Gray, K.; Steingrube, A.; Morris, M.N. Weight Attitudes Predict Eating Competence among College Students. Fam. Consum. Sci. Res. J. 2010, 39, 184–193. [Google Scholar] [CrossRef]
- Quick, V.; Byrd-Bredbenner, C.; Shoff, S.; White, A.A.; Lohse, B.; Horacek, T.; Colby, S.; Brown, O.; Kidd, T.; Greene, G. Relationships of Sleep Duration With Weight-Related Behaviors of U.S. College Students. Behav. Sleep Med. 2016, 14, 565–580. [Google Scholar] [CrossRef]
- Quick, V.; Shoff, S.; Lohse, B.; White, A.; Horacek, T.; Greene, G. Relationships of eating competence, sleep behaviors and quality, and overweight status among college students. Eat. Behav. 2015, 19, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quick, V.; Byrd-Bredbenner, C.; White, A.A.; Brown, O.; Colby, S.; Shoff, S.; Lohse, B.; Horacek, T.; Kidd, T.; Greene, G. Eat, sleep, work, play: Associations of weight status and health- related behaviors among young adult college students. Am. J. Health Promot. 2014, 29, e54–e72. [Google Scholar] [CrossRef] [PubMed]
- Lohse, B.; Arnold, K.; Wamboldt, P. Evaluation of About Being Active, an online lesson about physical activity shows that perception of being physically active is higher in eating competent low-income women. BMC Women Health 2013, 13, 12. [Google Scholar] [CrossRef] [Green Version]
- Psota, T.L.; Lohse, B.; West, S.G. Associations between Eating Competence and Cardiovascular Disease Biomarkers. J. Nutr. Educ. Behav. 2007, 39, S171–S178. [Google Scholar] [CrossRef] [PubMed]
- Stotts Krall, J.; Lohse, B. Interviews with Low-Income Pennsylvanians Verify a Need to Enhance Eating Competence. J. Am. Diet. Assoc. 2009, 109, 468–473. [Google Scholar] [CrossRef]
- Satter, E. Eating Competence: Nutrition Education with the Satter Eating Competence Model. J. Nutr. Educ. Behav. 2007, 39, S189–S194. [Google Scholar] [CrossRef]
- Stotts, J.L.; Lohse, B. Reliability of the ecSatter Inventory as a Tool to Measure Eating Competence. J. Nutr. Educ. Behav. 2007, 39, S167–S170. [Google Scholar] [CrossRef]
- Lohse, B. The Satter Eating Competence Inventory for Low-income persons is a valid measure of eating competence for persons of higher socioeconomic position. Appetite 2015, 87, 223–228. [Google Scholar] [CrossRef]
- Godleski, S.; Lohse, B.; Krall, J.S. Satter Eating Competence Inventory Subscale Restructure After Confirmatory Factor Analysis. J. Nutr. Educ. Behav. 2019, 51, 1003–1010. [Google Scholar] [CrossRef]
- NEEDs Center Protocol for the Use of the ecSatter Inventory 2.0. Available online: https://www.needscenter.org/wp-content/uploads/2019/09/ecSI-2.0-Usage-Protocol-2-1.pdf (accessed on 9 March 2020).
- De Queiroz, F.L.N.; Nakano, E.Y.; Ginani, V.C.; Botelho, R.B.A.; Araújo, W.M.C.; Zandonadi, R.P. Eating competence among a select sample of Brazilian adults: Translation and reproducibility analyses of the satter eating competence inventory. Nutrients 2020, 12, 2145. [Google Scholar] [CrossRef]
- BRASIL, M. VIGITEL 2019, Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas por Inquerito Telefônico, 1st ed.; da S. Brasil, M., Ed.; Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis: Brasília, Brazil, 2020; ISBN 9788533419568.
- IBGE IBGE—Instituto Brasileiro de Geografia: Pesquisa Nacional por Amostra de Domicílio Contínua (PNAD Contínua). Available online: http://www.ibge.gov.br/estatisticas-novoportal/sociais/educacao/1727-pnad-continua.html (accessed on 22 April 2020).
- World Health Organization WHO. Mean Body Mass Index (BMI); WHO: Geneva, Switzerland. Available online: http://www.who.int/gho/ncd/risk_factors/bmi_text/en/ (accessed on 20 May 2020).
- Da Coqueiro, R.S.; Borges, L.J.; Araújo, V.C.; Pelegrini, A.; Barbosa, A.R. Medidas auto-referidas são válidas para avaliação do estado nutricional na população brasileira? Rev. Bras. Cineantropom. Desempenho Hum. 2009, 11, 113–119. [Google Scholar] [CrossRef]
- Tilles-Tirkkonen, T.; Outi, N.; Sakari, S.; Jarmo, L.; Kaisa, P.; Leila, K. Preliminary Finnish measures of Eating Competence suggest association with health-promoting eating patterns and related Psychobehavioral factors in 10–17 year old adolescents. Nutrients 2015, 7, 3828–3846. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, S.M.; Araújo, W.M.C.; Nakano, E.Y.; Zandonadi, R.P. Brazilian vegetarians diet quality markers and comparison with the general population: A nationwide cross-sectional study. PLoS ONE 2020, 15, e0232954. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Conti, M.A.; Scagliusi, F.; Queiroz, G.K.O.; Hearst, N.; Cordás, T.A. Cross-cultural adaptation: Translation and Portuguese language content validation of the tripartite influence scale for body dissatisfaction|Adaptação transcultural: Tradução e validação de conteúdo para o idioma Português do modelo da Tripartite Influe. Cad. Saude Publica 2010, 26, 503–513. [Google Scholar] [CrossRef] [Green Version]
- Pratesi, C.P.; Häuser, W.; Uenishi, R.H.; Selleski, N.; Nakano, E.Y.; Gandolfi, L.; Pratesi, R.; Zandonadi, R.P. Quality of life of celiac patients in Brazil: Questionnaire translation, cultural adaptation and validation. Nutrients 2018, 10, 1167. [Google Scholar] [CrossRef] [Green Version]
- Farage, P.; Zandonadi, R.P.; Ginani, V.C.; Gandolfi, L.; Pratesi, R.; de Medeiros Nóbrega, Y.K. Content validation and semantic evaluation of a check-list elaborated for the prevention of gluten cross-contamination in food services. Nutrients 2017, 9, 36. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.R.; Mathur, A. The value of online surveys. Internet Res. 2005, 15, 195–219. [Google Scholar] [CrossRef]
- IBGE Instituto Brasileiro de Geografia e Estatistica PNAD Contínua TIC 2017: Internet Chega a três em Cada Quatro Domicílios do País. Available online: http://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia,-de-noticias/releases/23445-pnad-continua-tic-2017-internet-chega-a-tres-em-cada-quatro-domicilios-do-pais (accessed on 21 April 2020).
- Streiner, D.L.; Streiner, D.L. Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- Lohse, B.; Krall, J.S.; Psota, T.; Kris-Etherton, P. Impact of a Weight Management Intervention on Eating Competence: Importance of Measurement Interval in Protocol Design. Am. J. Health Promot. 2018, 32, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Järvelä-Reijonen, E.; Karhunen, L.; Sairanen, E.; Rantala, S.; Laitinen, J.; Puttonen, S.; Peuhkuri, K.; Hallikainen, M.; Juvonen, K.; Myllymäki, T.; et al. High perceived stress is associated with unfavorable eating behavior in overweight and obese Finns of working age. Appetite 2016, 103, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, C.A.; Machado, P.P.; da Costa, M.L.L.; Levy, R.B.; Monteiro, C.A. Parents’ cooking skills confidence reduce children’s consumption of ultra-processed foods. Appetite 2019, 144, 104452. [Google Scholar] [CrossRef]
- Hartmann, C.; Dohle, S.; Siegrist, M. Importance of cooking skills for balanced food choices. Appetite 2013, 65, 125–131. [Google Scholar] [CrossRef]
- Reicks, M.; Trofholz, A.C.; Stang, J.S.; Laska, M.N. Impact of Cooking and Home Food Preparation Interventions Among Adults: Outcomes and Implications forFuture Programs. J. Nutr. Educ. Behav. 2014, 46, 259–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarpe-Ratner, E.; Folkens, S.; Sharma, S.; Daro, D.; Edens, N.K. An Experiential Cooking and Nutrition Education Program Increases Cooking Self-Efficacy and Vegetable Consumption in Children in Grades 3–8. J. Nutr. Educ. Behav. 2016, 48, 697–705.e1. [Google Scholar] [CrossRef] [Green Version]
- McGowan, L.; Caraher, M.; Raats, M.; Lavelle, F.; Hollywood, L.; McDowell, D.; Spence, M.; McCloat, A.; Mooney, E.; Dean, M. Domestic cooking and food skills: A review. Crit. Rev. Food Sci. Nutr. 2017, 57, 2412–2431. [Google Scholar] [CrossRef]
- Burton, E.T.; Smith, W.A. Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention. Nutrients 2020, 12, 1425. [Google Scholar] [CrossRef]
- Kuijer, R.G.; Boyce, J.A. Chocolate cake. Guilt or celebration? Associations with healthy eating attitudes, perceived behavioural control, intentions and weight-loss. Appetite 2014, 74, 48–54. [Google Scholar] [CrossRef]
- Davidson, D.J.; Freudenburg, W.R. Gender and environmental risk concerns: A review and analysis of available research. Environ. Behav. 1996, 28, 302–339. [Google Scholar] [CrossRef]
- Ministério do Planejamento, Orçamento e Gestão Instituto Brasileiro de Geografia e Estatística—IBGE POF—Pesquisa de Orçamentos Familiares. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv50063.pdf (accessed on 22 April 2020).
- Krall, J.S.; Lohse, B. Cognitive testing with female nutrition and education assistance program participants informs validity of the satter eating competence inventory. J. Nutr. Educ. Behav. 2010, 42, 277–283. [Google Scholar] [CrossRef]
- Clifford, D.; Ozier, A.; Bundros, J.; Moore, J.; Kreiser, A.; Morris, M.N. Impact of Non-Diet Approaches on Attitudes, Behaviors, and Health Outcomes: A Systematic Review. J. Nutr. Educ. Behav. 2015, 47, 143–155.e1. [Google Scholar] [CrossRef]
- Tilles-Tirkkonen, T.; Aittola, K.; Männikkö, R.; Absetz, P.; Kolehmainen, M.; Schwab, U.; Lindström, J.; Lakka, T.; Pihlajamäki, J.; Karhunen, L. Eating competence is associated with lower prevalence of obesity and better insulin sensitivity in finnish adults with increased risk for type 2 diabetes: The stopdia study. Nutrients 2020, 12, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Diet, nutrition and the prevention of chronic diseases. World Health Organ. Tech. Rep. Ser. 2003, 916, 1–149. [Google Scholar] [CrossRef] [Green Version]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of Soft Drink Consumption on Nutrition and Health: A Systematic Review and Meta-Analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef]
- Ministério da Saúde. Guia Alimentar Para a População Brasileira; Ministério da Saúde: Brasília, Brazil, 2019; Volume 2.


{kind=link}
| Mean (DP) | Median (Q1–Q3) | Range | Floor Effect (%) | Ceiling Effect (%) | Cronbach’s Alpha | |
|---|---|---|---|---|---|---|
| Eating attitude | 12.06 (3.91) | 13 (9–15) | 0–18 | 0.2% | 6.3% | 0.793 |
| Food acceptance | 5.03 (2.42) | 5 (3–7) | 0–9 | 3.8% | 8.2% | 0.704 |
| Internal regulation | 3.85 (1.53) | 4 (3–5) | 0–6 | 2.9% | 16.6% | 0.543 |
| Contextual skills | 9.26 (3.70) | 10 (7–12) | 0–15 | 0.8% | 6.9% | 0.815 |
| Total | 30.19 (8.90) | 31 (24–37) | 1–48 | 0% | 0.5% | 0.868 |
| Eating Attitude | Food Acceptance | Internal Regulation | Contextual Skills | Total | ecSI2.0™BR ≥ 32 | |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Freq. (%) | |
| Gender * | ||||||
| Female (n = 1353) | 11.87 (4.00) A | 5.15 (2.42) A | 3.80 (1.51) A | 9.45 (3.66) A | 30.26 (9.02) A | 658 (48.6%) A |
| Male (n = 454) | 12.61 (3.61) B | 4.64 (2.39) B | 4.01 (1.55) B | 8.69 (3.75) A | 29.94 (8.52) A | 206 (45.4%) A |
| p | 0.000 | 0.000 | 0.010 | 0.238 | 0.518 | 0.233 *** |
| Age * | ||||||
| Up to 40 years (n = 975) | 11.58 (4.09) A | 5.06 (2.48) A | 3.68 (1.56) A | 8.58 (3.72) A | 28.90 (9.18) A | 413 (42.4%) A |
| More than 40 years (n = 835) | 12.62 (3.62) B | 4.99 (2.35) A | 4.04 (1.47) B | 10.04 (3.52) B | 31.69 (8.31) B | 453 (54.3%) B |
| p | 0.000 | 0.542 | 0.000 | 0.000 | 0.000 | 0.000 *** |
| Schooling level ** | ||||||
| High School (n = 159) | 11.84 (4.33) A | 4.67 (2.51) A | 4.10 (1.69) A | 8.60 (4.06) A | 29.21 (9.52) A | 71 (44.7%) A |
| Undergraduate (n = 769) | 12.05 (3.88) A | 4.85 (2.43) AB | 3.86 (1.54) A | 8.80 (3.79) A | 29.56 (8.96) AB | 344 (44.7%) A |
| Graduate (n = 882) | 12.10 (3.87) A | 5.24 (2.38) B | 3.79 (1.49) A | 9.77 (3.48) B | 30.90 (8.67) B | 451 (51.1%) B |
| p | 0.735 | 0.001 | 0.064 | 0.000 | 0.003 | 0.024 *** |
| Family income +,** | ||||||
| Up to R$ 3000 (n = 325) | 11.90 (4.12) A | 4.90 (2.38) A | 3.85 (1.55) A | 8.63 (3.93) A | 29.27 (9.23) A | 145 (44.6%) A |
| R$ 3001 to R$ 5000 (n = 255) | 11.85 (3.48) A | 4.57 (2.47) A | 3.82 (1.66) A | 8.73 (3.70) A | 28.98 (9.39) A | 112 (43.9%) A |
| R$ 5001 to R$ 10,000 (n = 417) | 11.98 (4.07) A | 5.08 (2.36) B | 3.83 (1.53) A | 9.17 (9.79) AB | 30.06 (9.13) AB | 190 (45.6%) AB |
| R$ 10,001to R$ 20,000 (n = 455) | 12.08 (4.06) A | 5.10 (2.42) B | 3.84 (3.42) A | 9.75 (8.02) B | 30.76 (8.24) AB | 220 (48.4%) AB |
| More than R$ 20,000 (n = 358) | 12.41 (3.91) A | 5.31 (1.32) B | 3.90 (3.48) A | 9.67 (9.21) B | 31.29 (8.61) B | 199 (55.6%) B |
| p | 0.361 | 0.004 | 0.973 | 0.000 | 0.003 | 0.014 *** |
| BMI kg/m2 ** | ||||||
| Low: <18.5 (n = 44) | 12.89 (4.12) A | 5.07 (2.68) A | 4.50 (1.32) A | 8.34 (3.42) AB | 30.80 (9.79) AB | 20 (45.5%) A |
| Normal: 18.5–24.9 (n = 869) | 12.92 (3.48) A | 5.25 (2.38) A | 4.09 (1.41) AB | 9.83 (3.48) C | 32.10 (8.02)B | 490 (56.4%) A |
| Overweight: 25.0–29.9 (n = 591) | 11.57 (4.07) B | 4.88 (2.47) AB | 3.73 (1.55) BC | 9.24 (3.68) AC | 29.42 (9.21)A | 268 (45.3%) A |
| Obesity: ≥ 30 (n = 304) | 10.40 (4.06) B | 4.66 (2.36) B | 3.28 (1.66) C | 7.76 (3.93) A | 26.09 (8.98) C | 86 (28.3%) A |
| p | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 *** |
| Perception of body size ** | ||||||
| Undersize (n = 64) | 13.38 (3.71) A | 4.61 (2.50) A | 4.31 (1.39) A | 7.97 (4.00) A | 30.27 (9.01) A | 32 (50.0%) A |
| Appropriate size (n = 730) | 13.58 (3.19) A | 5.40 (2.35) B | 4.30 (1.31) A | 10.35 (3.29) B | 33.63 (7.46) B | 463 (63.4%) B |
| Oversize (n = 1016) | 10.88 (4.00) B | 4.78 (2.43) AB | 3.49 (1.58) B | 8.55 (3.76) A | 27.70 (9.02) C | 371 (36.5%) C |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 *** |
| Diabetes * | ||||||
| No (n = 1729) | 12.07 (3.91) A | 5.03 (2.42) A | 3.86 (1.51) A | 9.24 (3.70) A | 30.19 (8.91) A | 832 (48.1%) A |
| Yes (n = 81) | 11.79 (3.91) A | 4.98 (2.48) A | 3.67 (1.78) A | 9.6 (3.63) A | 30.04 (8.72) A | 34 (42.0%) A |
| p | 0.529 | 0.849 | 0.350 | 0.384 | 0.878 | 0.307 *** |
| Hypertension * | ||||||
| No (n = 1567) | 12.01 (3.92) A | 5.06 (2.42) A | 3.84 (1.52) A | 9.19 (3.66) A | 30.10 (8.87) A | 740 (47.2%) A |
| Yes (n = 243) | 12.38 (3.83) A | 4.82 (2.40) A | 3.89 (1.59) A | 9.65 (3.92) A | 30.74 (9.05) A | 126 (51.9%) A |
| p | 0.169 | 0.153 | 0.618 | 0.071 | 0.292 | 0.190 *** |
| Fruit´s consumption ** | ||||||
| Never/rarely (n = 168) | 11.14 (4.25) A | 3.42 (2.65) A | 3.65 (1.68) A | 6.20 (3.90) A | 24.40 (9.49) A | 38 (22.6%) A |
| 1 to 4 days/week (n = 731) | 11.55 (4.05) A | 4.69 (2.38) B | 3.68 (1.55) A | 8.26 (3.58) B | 28.18 (8.86) B | 284 (38.9%) B |
| 5 or more days/week (n = 910) | 12.63 (3.64) B | 5.59 (2.22) C | 4.02 (1.46) B | 10.62 (3.12) C | 32.86 (7.83) C | 543 (59.7%) C |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 *** |
| Vegetable´s consumption ** | ||||||
| Never/rarely (n = 86) | 10.38 (4.36) A | 2.67 (2.44) A | 3.59 (1.85) A | 6.20 (3.73) A | 22.85 (9.17) A | 13 (15.1%) A |
| 1 to 4 days/week (n = 527) | 11.06 (3.93) A | 3.92 (2.28) B | 3.68 (1.56) AB | 7.50 (3.59) B | 26.16 (8.49) B | 150 (28.5%) B |
| 5 or more days/week (n = 1196) | 12.61 (3.75) B | 5.68 (2.19) C | 3.94 (1.48) B | 10.25 (3.32) C | 32.48 (8.11) C | 702 (58.7%) C |
| P | 0.000 | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 *** |
| Artificial juice or soda consumption ** | ||||||
| Never/rarely (n = 1032) | 12.52 (3.73) A | 5.46 (2.29) A | 3.98 (1.45) A | 10.40 (3.34) A | 32.37 (8.26) A | 596 (57.8%) A |
| 1 to 4 days/week (n = 613) | 11.39 (4.07) B | 4.53 (2.45) B | 3.66 (1.56) B | 8.11 (3.47) B | 27.69 (8.88) B | 226 (36.9%) B |
| 5 or more days/week (n = 164) | 11.61 (4.05) B | 4.13 (2.52) B | 3.68 (1.76) B | 6.32 (3.74) C | 25.75 (8.81) C | 43 (26.2%) C |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Queiroz, F.L.N.d.; Nakano, E.Y.; Botelho, R.B.A.; Ginani, V.C.; Cançado, A.L.F.; Zandonadi, R.P. Eating Competence Associated with Food Consumption and Health Outcomes among Brazilian Adult Population. Nutrients 2020, 12, 3218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103218
Queiroz FLNd, Nakano EY, Botelho RBA, Ginani VC, Cançado ALF, Zandonadi RP. Eating Competence Associated with Food Consumption and Health Outcomes among Brazilian Adult Population. Nutrients. 2020; 12(10):3218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103218
Chicago/Turabian StyleQueiroz, Fabiana Lopes Nalon de, Eduardo Yoshio Nakano, Raquel Braz Assunção Botelho, Verônica Cortez Ginani, André Luiz Fernandes Cançado, and Renata Puppin Zandonadi. 2020. "Eating Competence Associated with Food Consumption and Health Outcomes among Brazilian Adult Population" Nutrients 12, no. 10: 3218. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103218