Effect of Exercise Habit on Skeletal Muscle Mass Varies with Protein Intake in Elderly Patients with Type 2 Diabetes: A Retrospective Cohort Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
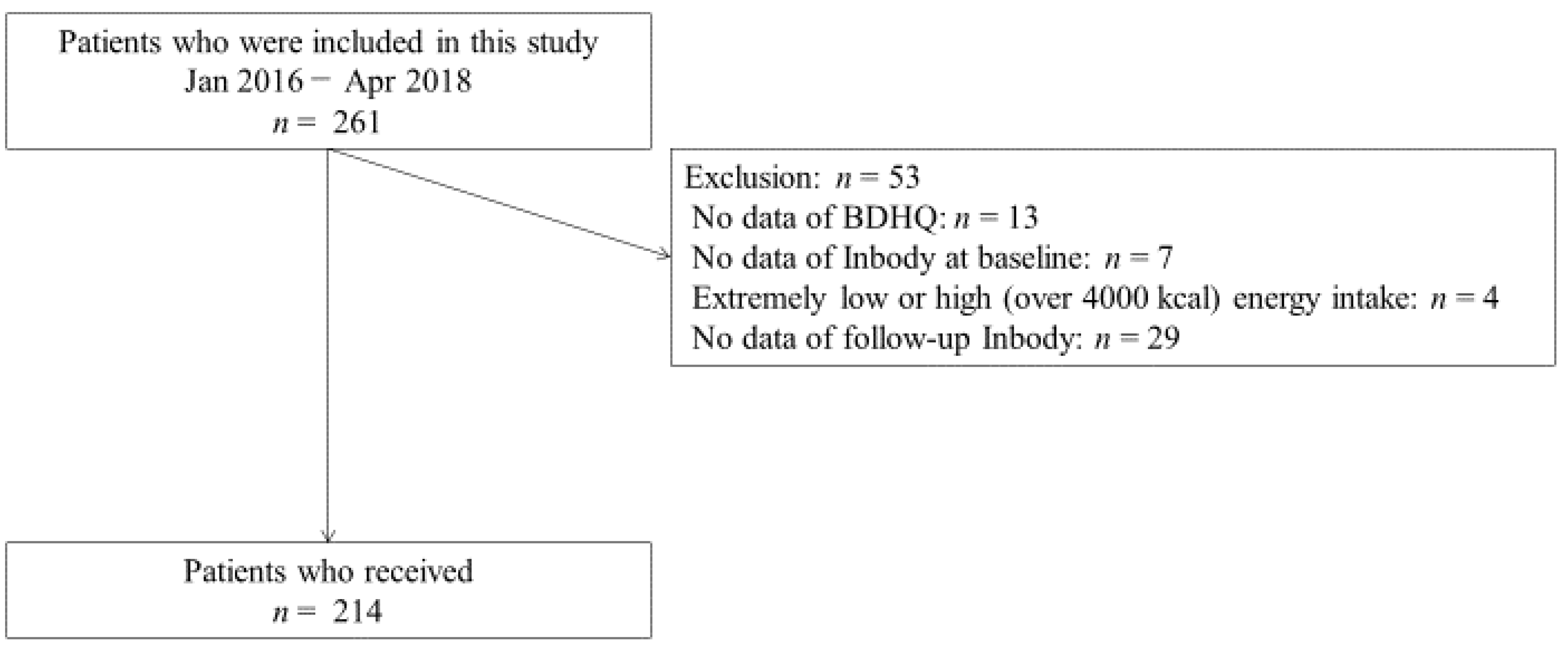
2.1. Study Patients
2.2. Lifestyle, Medications, and Laboratory Data Collection
2.3. Measurement of Body Composition Determined by Bioelectric Impedance
2.4. Estimation and Assessment of Habitual Food and Nutrient Intake
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Availability of Data and Materials
References
- Umegaki, H. Sarcopenia and frailty in older patients with diabetes mellitus. Geriatr. Gerontol. Int. 2016, 16, 293–299. [Google Scholar] [CrossRef]
- Yanase, T.; Yanagita, I.; Muta, K.; Nawata, H. Frailty in elderly diabetes patients. Endocr. J. 2018, 65, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Okamura, T.; Miki, A.; Hashimoto, Y.; Kaji, A.; Sakai, R.; Osaka, T.; Hamaguchi, M.; Yamazaki, M.; Fukui, M. Shortage of energy intake rather than protein intake is associated with sarcopenia in elderly patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort. J. Diabetes 2018, 11, 477–483. [Google Scholar] [CrossRef]
- Nakamura, K.; Yoshida, D.; Honda, T.; Hata, J.; Shibata, M.; Hirakawa, Y.; Furuta, Y.; Kishimoto, H.; Ohara, T.; Kitazono, T.; et al. Prevalence and mortality of sarcopenia in a community-dwelling older Japanese population: The Hisayama Study. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Liu, P.; Hao, Q.; Hai, S.; Wang, H.; Cao, L.; Dong, B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas 2017, 103, 16–22. [Google Scholar] [CrossRef]
- Abbas, H.; Perna, S.; Shah, A.; Al-Mannai, M.; Gasparri, C.; Infantino, V.; Cereda, E.; Peroni, G.; Riva, A.; Petrangolini, G.; et al. Risk factors for 5-year mortality in a cohort of elderly patients with sarcopenia. Exp. Gerontol. 2020, 136. [Google Scholar] [CrossRef]
- Wang, X.; Hu, Z.; Hu, J.; Du, J.; Mitch, W.E. Insulin Resistance Accelerates Muscle Protein Degradation: Activation of the Ubiquitin-Proteasome Pathway by Defects in Muscle Cell Signaling. Endocrinology 2006, 147, 4160–4168. [Google Scholar] [CrossRef] [Green Version]
- Muscariello, E.; Nasti, G.; Siervo, M.; Di Maro, M.; Lapi, D.; D’Addio, G.; Colantuoni, A. Dietary protein intake in sarcopenic obese older women. Clin. Interv. Aging 2016, 11, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kröger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkilä, A.T. Association of protein intake with the change of lean mass among elderly women: The Osteoporosis Risk Factor and Prevention—Fracture Prevention Study (OSTPRE-FPS). J. Nutr. Sci. 2015, 4, e41. [Google Scholar] [CrossRef] [Green Version]
- Shephard, R.J.; Park, H.; Park, S.; Aoyagi, Y. Objectively Measured Physical Activity and Progressive Loss of Lean Tissue in Older Japanese Adults: Longitudinal Data from the Nakanojo Study. J. Am. Geriatr. Soc. 2013, 61, 1887–1893. [Google Scholar] [CrossRef]
- Yu, R.; Wong, M.; Leung, J.; Lee, J.; Auyeung, T.W.; Woo, J. Incidence, reversibility, risk factors and the protective effect of high body mass index against sarcopenia in community-dwelling older Chinese adults. Geriatr. Gerontol. Int. 2014, 14, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med Direct. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Okamura, T.; Iwai, K.; Hashimoto, Y.; Senmaru, T.; Ushigome, E.; Hamaguchi, M.; Asano, M.; Yamazaki, M.; Fukui, M. Japanese radio calisthenics prevents the reduction of skeletal muscle mass volume in people with type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001027. [Google Scholar] [CrossRef] [Green Version]
- Sakai, R.; Hashimoto, Y.; Ushigome, E.; Miki, A.; Okamura, T.; Matsugasumi, M.; Fukuda, T.; Majima, S.; Matsumoto, S.; Senmaru, T.; et al. Late-night-dinner is associated with poor glycemic control in people with type 2 diabetes: The KAMOGAWA-DM cohort study. Endocr. J. 2018, 65, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Kaji, A.; Hashimoto, Y.; Kobayashi, Y.; Sakai, R.; Okamura, T.; Miki, A.; Hamaguchi, M.; Kuwahata, M.; Yamazaki, M.; Fukui, M. Sarcopenia is associated with tongue pressure in older patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort study. Geriatr. Gerontol. Int. 2018, 19, 153–158. [Google Scholar] [CrossRef]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Okubo, H.; Hosoi, Y.; Horiguchi, H.; Oguma, E.; Kayama, F. Dietary glycemic index and load in relation to metabolic risk factors in Japanese female farmers with traditional dietary habits. Am. J. Clin. Nutr. 2006, 83, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Kimura, T.; Hashimoto, Y.; Tanaka, M.; Asano, M.; Yamazaki, M.; Oda, Y.; Toda, H.; Marunaka, Y.; Nakamura, N.; Fukui, M. Sodium-chloride Difference and Metabolic Syndrome: A Population-based Large-scale Cohort Study. Intern. Med. 2016, 55, 3085–3090. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised Equations for Estimated GFR From Serum Creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2014, 15, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med Direct. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Mitchell, W.K.; Williams, J.; Atherton, P.J.; Larvin, M.; Lund, J.N.; Narici, M. Sarcopenia, Dynapenia, and the Impact of Advancing Age on Human Skeletal Muscle Size and Strength; a Quantitative Review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemmens, H.J.M.; Brodsky, J.B.; Bernstein, D.P. Estimating Ideal Body Weight—A New Formula. Obes. Surg. 2005, 15, 1082–1083. [Google Scholar] [CrossRef]
- Standard Tables of Food Composition in Japan; Ministry of Education, Culture, Sports, Science and Technology: Tokyo, Japan, 2010. (In Japanese). Available online: https://www.mext.go.jp/b_menu/shingi/gijyutu/gijyutu3/houkoku/1298713.htm (accessed on 20 October 2020).
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef]
- Kaji, A.; Hashimoto, Y.; Kobayashi, Y.; Wada, S.; Kuwahata, M.; Yamazaki, M.; Fukui, M. Protein intake is not associated with progression of diabetic kidney disease in patients without macroalbuminuria. Diabetes Metab. Res. Rev. 2019, 35, e3150. [Google Scholar] [CrossRef]
- Chitturi, S.; Farrell, G.C.; Hashimoto, E.; Saibara, T.; Lau, G.K.K.; Sollano, J.D.; Nafld, A.-P.W.P.O. Non-alcoholic fatty liver disease in the Asia-Pacific region: Definitions and overview of proposed guidelines. J. Gastroenterol. Hepatol. 2007, 22, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Franzke, B.; Neubauer, O.; Cameron-Smith, D.; Wagner, K.-H. Dietary Protein, Muscle and Physical Function in the Very Old. Nutrients 2018, 10, 935. [Google Scholar] [CrossRef] [Green Version]
- English, K.L.; A Mettler, J.; Ellison, J.B.; Mamerow, M.M.; Arentson-Lantz, E.J.; Pattarini, J.M.; Ploutz-Snyder, R.; Sheffield-Moore, M.; Paddon-Jones, D. Leucine partially protects muscle mass and function during bed rest in middle-aged adults. Am. J. Clin. Nutr. 2015, 103, 465–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Atherton, P.; Smith, K.; Rennie, M.J. Human muscle protein synthesis and breakdown during and after exercise. J. Appl. Physiol. 2009, 106, 2026–2039. [Google Scholar] [CrossRef] [Green Version]
- Tipton, K.D.; Borsheim, E.; Wolf, S.E.; Sanford, A.P.; Wolfe, R.R. Acute response of net muscle protein balance reflects 24-h balance after exercise and amino acid ingestion. Am. J. Physiol. Metab. 2003, 284, E76–E89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.X.; Liu, X.D.; Li, K.; Liu, W.Z.; Ren, Y.S.; Zhang, J.X. Different dietary energy intake affects skeletal muscle development through an Akt-dependent pathway in Dorper × small thin-tailed crossbred ewe lambs. Domest. Anim. Endocrinol. 2016, 57, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.X.; Liu, X.D.; Zhang, J.X.; Y, W.; Li, H.Q. Effect of different dietary energy on collagen accumulation in skeletal muscle of ram lambs1. J. Anim. Sci. 2015, 93, 4200–4210. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Junior, H.J.; Marzetti, E.; Picca, A.; Cesari, M.; Uchida, M.; Calvani, R. Protein Intake and Frailty: A Matter of Quantity, Quality, and Timing. Nutrients 2020, 12, 2915. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All n = 214 | Exercise (−)/Adequate Protein Intake (−) n = 52 | Exercise (+)/Adequate Protein Intake (−) n = 56 | Exercise (−)/Adequate Protein Intake (+) n = 40 | Exercise (+)/Adequate Protein Intake (+) n = 66 | p | |
|---|---|---|---|---|---|---|
| Men/Women | 120 94 | 27/25 | 34/22 | 21/19 | 38/28 | 0.772 |
| Age, years | 72.2 (5.1) | 72.9 (5.7) | 71.5 (4.9) | 72.3 (4.6) | 72.2 (5.2) | 0.612 |
| Duration of diabetes, years | 15.6 (10.2) | 17.2 (11.5) | 15.1 (9.5) | 14.5 (11.5) | 15.6 (8.7) | 0.602 |
| Height, cm | 159.9 (8.7) | 159.7 (8.1) | 161.6 (8.5) | 158.5 (9.9) | 159.4 (8.5) | 0.320 |
| Body weight, kg | 60.5 (10.8) | 61.5 (10.7) | 60.6 (11.0) | 59.6 (10.7) | 60.1 (11.0) | 0.857 |
| Body mass index, kg/m2 | 23.7 (3.9) | 24.1 (4.1) | 23.2 (4.1) | 23.8 (4.2) | 23.6 (3.3) | 0.662 |
| Insulin (−/+) | 154/60 | 36/16 | 40/16 | 27/13 | 51/15 | 0.678 |
| Antihypertension medication (−/+) | 84/130 | 19/33 | 20/36 | 15/25 | 30/36 | 0.666 |
| Antilipidemic medication (−/+) | 102/112 | 21/31 | 26/30 | 23/17 | 32/34 | 0.439 |
| Smoking (−/+) | 184/30 | 44/8 | 52/4 | 34/6 | 54/12 | 0.354 |
| Habitual alcohol intake (−/+) | 195/19 | 49/3 | 51/5 | 34/6 | 61/5 | 0.455 |
| Habit of exercise (−/+) | 92/112 | 52/0 | 0/56 | 40/0 | 0/66 | <0.001 |
| Hemoglobin A1c, % | 7.2 (1.0) | 7.0 (0.9) | 7.1 (0.8) | 7.3 (1.2) | 7.2 (1.0) | 0.642 |
| Hemoglobin A1c, mmol/mol | 54.8 (10.7) | 53.4 (10.0) | 54.5 (9.1) | 56.0 (13.1) | 55.4 (10.8) | 0.642 |
| Plasma glucose, mmol/l | 8.1 (2.8) | 8.0(3.1) | 8.1 (2.6) | 8.6 (3.8) | 7.9 (2.0) | 0.627 |
| Creatinine, umol/l | 73.8 (25.5) | 77.2 (22.5) | 74.5 (26.2) | 72.2 (24.9) | 71.7 (27.8) | 0.672 |
| eGFR, ml/min/1.73 m2 | 66.4 (17.8) | 61.4 (17.1) | 66.8 (17.2) | 67.2 (18.7) | 69.5 (17.7) | 0.098 |
| Total energy intake, kcal/day | 1736 (591) | 1421 (374) | 1375 (352) | 2067 (573) * † | 2089 (589) * † | <0.001 |
| Energy intake, kcal/IBW/day | 30.7 (9.8) | 25.1 (5.3) | 23.8 (5.2) | 37.2 (9.0) * † | 37.2 (9.4) * † | <0.001 |
| Total protein intake, g/day | 74.7 (29.9) | 53.6 (11.2) | 53.0 (11.3) | 95.8 (28.6) * † | 96.8 (26.6) * † | <0.001 |
| Animal protein intake, g/day | 46.5 (23.5) | 31.4 (9.5) | 29.4 (10.4) | 61.8 (22.2) * † | 63.8 (21.8) * † | <0.001 |
| Animal protein intake, g/IBW/day | 6.02 (3.05) | 4.05 (1.20) | 3.76 (1.30) | 8.04 (2.79) * † | 8.27 (2.85) * † | <0.001 |
| Vegetable protein intake, g/day | 28.2 (9.8) | 22.3 (7.1) | 23.6 (6.0) | 34.1 (10.8) * † | 33.1 (9.0) * † | <0.001 |
| Vegetable protein intake, g/IBW/day | 3.63 (1.21) | 2.86 (0.84) | 3.01 (0.73) | 4.43 (1.31) * † | 4.27 (1.08) * † | <0.001 |
| Protein intake, g/IBW/day | 1.33 (0.54) | 0.95 (0.17) | 0.92 (0.19) | 1.73 (0.49) * † | 1.73 (0.48) * † | <0.001 |
| Adequate protein intake (−/+) | 108/106 | 45/0 | 46/0 | 0/34 | 0/61 | <0.001 |
| Total fat intake, g/day | 55.1 (21.9) | 43.3 (12.6) | 40.6 (11.2) | 65.2 (17.6) * † | 70.5 (23.7) * † | <0.001 |
| Fat intake, g/IBW/day | 0.98 (0.39) | 0.77 (0.20) | 0.70 (0.18) | 1.18 (0.31) * † | 1.26 (0.42) * † | <0.001 |
| Total carbohydrate intake, g/day | 218.2 (81.7) | 191.1 (67.2) | 182.8 (59.4) | 251.5 (97.6) * † | 249.4 (79.3) * † | <0.001 |
| Carbohydrate intake, g/IBW/day | 3.9 (1.3) | 3.4 (1.1) | 3.2 (1.0) | 4.5 (1.6) * † | 4.4 (1.3) * † | <0.001 |
| Appendicular muscle mass, kg | 17.6 (3.8) | 17.4 (3.8) | 18.1 (3.6) | 17.2 (3.7) | 17.8 (4.1) | 0.673 |
| Body fat mass, kg | 17.6 (7.4) | 19.0 (7.7) | 17.3 (7.8) | 17.6 (7.5) | 16.7 (6.6) | 0.431 |
| Percent body fat mass, % | 28.4 (8.8) | 30.3 (9.0) | 27.8 (8.6) | 28.7 (9.0) | 27.4 (8.5) | 0.313 |
| SMI, kg/m2 | 6.8 (0.9) | 6.8 (0.9) | 6.9 (0.9) | 6.8 (0.8) | 6.9 (1.1) | 0.767 |
| Change in SMI, kg/m2/month | −0.007 (0.023) | −0.007 (0.020) | −0.013 (0.019) | −0.011 (0.027) | 0.001 (0.023) † ‡ | 0.002 |
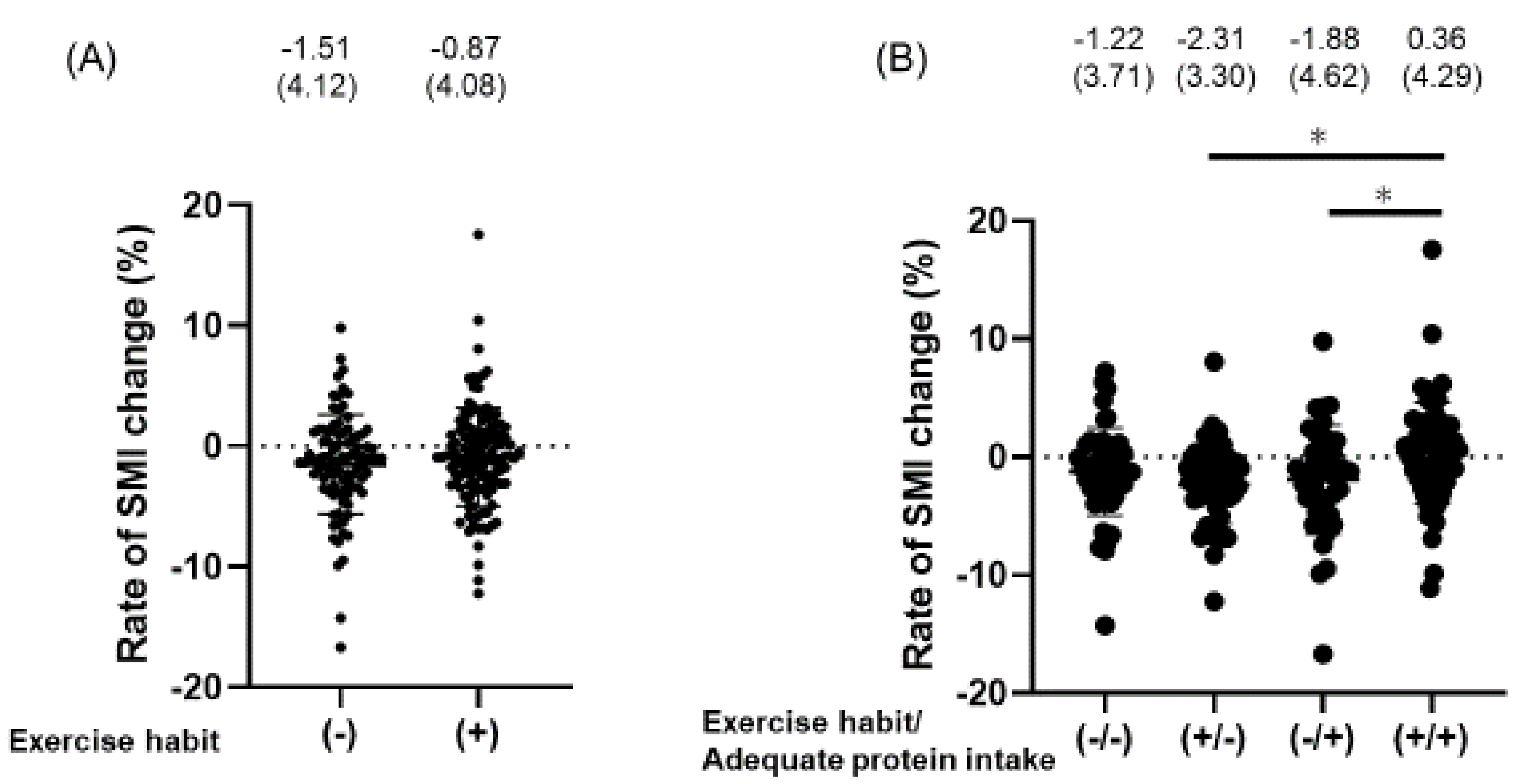
| Rate of SMI change, % | −1.14 (4.10) | −1.22 (3.71) | −2.31 (3.30) | −1.88 (4.62) | 0.36 (4.29) † ‡ | 0.002 |
| Decreasing SMI (−/+) | 87/127 | 19/33 | 15/41 | 14/26 | 39/27 | 0.002 |
| Model 1 | Mode 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Men | 1.22 (0.66–2.25) | 0.520 | 0.40 (0.15–1.09) | 0.072 | 0.43 (0.16–1.18) | 0.095 |
| Age, years | 0.98 (0.92–1.03) | 0.386 | 0.99 (0.93–1.05) | 0.739 | 0.99 (0.93–1.05) | 0.740 |
| Smoking, yes | 0.76 (0.32–1.79) | 0.533 | 0.75 (0.31–1.80) | 0.519 | 0.72 (0.30–1.76) | 0.476 |
| Alcohol consumption, yes | 1.04 (0.36–3.05) | 0.930 | 1.15 (0.38–3.47) | 0.805 | 2.38 (0.25–22.6) | 0.449 |
| Duration of diabetes, years | ― | ― | 1.01 (0.97–1.04) | 0.730 | 1.01 (0.98–1.04) | 0.695 |
| SMI at baseline examination, kg/m2 | ― | ― | 2.49 (1.37–4.55) | 0.002 | 2.40 (1.29–4.47) | 0.004 |
| BMI, kg/m2 | ― | ― | 0.92 (0.83–1.03) | 0.159 | 0.93 (0.82–1.04) | 0.194 |
| Energy intake, kcal/IBW/day | ― | ― | 0.98 (0.94–1.02) | 0.342 | 0.86 (0.62–1.20) | 0.388 |
| Animal proteins intake, kcal/IBW/day | ― | ― | ― | ― | 1.17 (0.87–1.56) | 0.302 |
| Vegetable proteins intake, kcal/IBW/day | ― | ― | ― | ― | 1.03 (0.61–1.74) | 0.915 |
| Carbohydrate intake, kcal/IBW/day | ― | ― | ― | ― | 1.85 (0.42–8.21) | 0.419 |
| Fat intake, kcal/IBW/day | ― | ― | ― | ― | 1.62 (0.06–41.9) | 0.773 |
| Exercise (−)/Adequate protein intake (−) | 2.58 (1.21–5.48) | 0.014 | 1.21 (0.22–6.74) | 0.829 | 2.50 (0.90–6.90) | 0.078 |
| Exercise (+)/Adequate protein intake (−) | 3.77 (1.73–8.19) | <0.001 | 3.37 (1.28–8.85) | 0.014 | 3.58 (1.24–10.4) | 0.019 |
| Exercise (−)/Adequate protein intake (+) | 2.70 (1.19–6.15) | 0.018 | 1.60 (0.73–3.51) | 0.245 | 3.03 (1.27–7.22) | 0.012 |
| Exercise (+)/Adequate protein intake (+) | Ref | ― | Ref | ― | Ref | ― |
| Adequate Protein Intake (−) n = 108 | Standardized β | p |
|---|---|---|
| Men | 0.06 | 0.679 |
| Age, years | −0.001 | 0.990 |
| Duration of diabetes, years | −0.010 | 0.929 |
| Smoking, yes | −0.145 | 0.201 |
| Alcohol consumption, yes | −0.005 | 0.978 |
| SMI at baseline examination, kg/m2 | −0.014 | 0.940 |
| Body mass index, kg/m2 | −0.207 | 0.205 |
| Energy intake, kcal/IBW/day | 0.236 | 0.672 |
| Animal protein intake, kcal/IBW/day | −0.129 | 0.435 |
| Vegetable protein intake, kcal/IBW/day | −0.124 | 0.547 |
| Carbohydrate intake, kcal/IBW/day | −0.102 | 0.835 |
| Fat intake, kcal/IBW/day | 0.036 | 0.860 |
| Exercise habit, yes | −0.182 | 0.094 |
| Adequate protein intake (+) n = 106 | Standardized β | p |
| Men | 0.298 | 0.073 |
| Age, years | 0.039 | 0.704 |
| Duration of diabetes, years | −0.021 | 0.845 |
| Smoking, yes | 0.134 | 0.189 |
| Alcohol consumption, yes | −0.011 | 0.969 |
| SMI at baseline examination, kg/m2 | −0.427 | 0.022 |
| Body mass index, kg/m2 | 0.011 | 0.969 |
| Energy intake, kcal/IBW/day | 0.207 | 0.862 |
| Animal protein intake, kcal/IBW/day | 0.022 | 0.934 |
| Vegetable protein intake, kcal/IBW/day | 0.028 | 0.871 |
| Carbohydrate intake, kcal/IBW/day | −0.140 | 0.860 |
| Fat intake, kcal/IBW/day | −0.028 | 0.953 |
| Exercise habit, yes | 0.255 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashimoto, Y.; Kaji, A.; Sakai, R.; Takahashi, F.; Kawano, R.; Hamaguchi, M.; Fukui, M. Effect of Exercise Habit on Skeletal Muscle Mass Varies with Protein Intake in Elderly Patients with Type 2 Diabetes: A Retrospective Cohort Study. Nutrients 2020, 12, 3220. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103220
Hashimoto Y, Kaji A, Sakai R, Takahashi F, Kawano R, Hamaguchi M, Fukui M. Effect of Exercise Habit on Skeletal Muscle Mass Varies with Protein Intake in Elderly Patients with Type 2 Diabetes: A Retrospective Cohort Study. Nutrients. 2020; 12(10):3220. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103220
Chicago/Turabian StyleHashimoto, Yoshitaka, Ayumi Kaji, Ryosuke Sakai, Fuyuko Takahashi, Rena Kawano, Masahide Hamaguchi, and Michiaki Fukui. 2020. "Effect of Exercise Habit on Skeletal Muscle Mass Varies with Protein Intake in Elderly Patients with Type 2 Diabetes: A Retrospective Cohort Study" Nutrients 12, no. 10: 3220. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103220