The Mediating and Moderating Effects of Physical Fitness of the Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life in University Students

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Size
2.3. Study Variables
2.3.1. Adherence to the Mediterranean Diet
2.3.2. Health-Related Quality of Life
2.3.3. Anthropometric Variables
2.3.4. Physical Fitness
Handgrip Strength
Cardiorespiratory Fitness
2.3.5. Family Socioeconomic Status
2.3.6. Statistical Analysis
3. Results
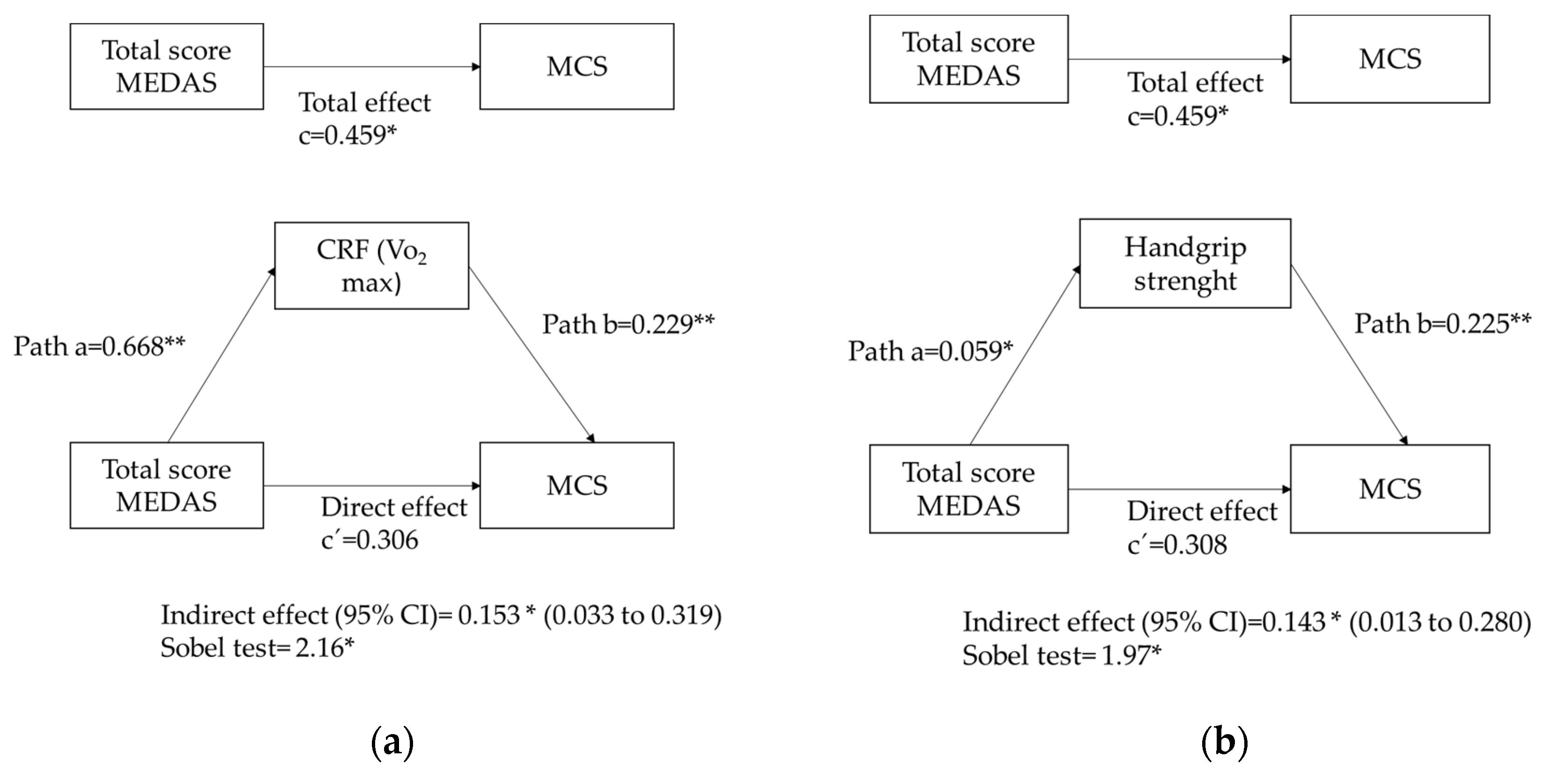
3.1. Mediation Analysis
3.2. Moderation Analysis
3.3. Sensitive Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of Physical Activity, Sedentary Time, and Sleep Duration on the Health-Related Quality of Life of College Students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozuelo-Carrascosa, D.P.; Martínez-Vizcaíno, V.; Sánchez-López, M.; Bartolomé-Gutiérrez, R.; Rodríguez-Martín, B.; Notario-Pacheco, B. Resilience as a mediator between cardiorespiratory fitness and mental health-related quality of life: A cross-sectional study. Nurs. Health Sci. 2017, 19, 316–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franquelo-Morales, P.; Sánchez-López, M.; Notario-Pacheco, B.; Miota-Ibarra, J.; Lahoz-García, N.; Gómez-Marcos, M.Á.; Martínez-Vizcaíno, V. Association between health-related quality of life, obesity, fitness, and sleep quality in young adults: The Cuenca adult study. Behav. Sleep Med. 2018, 16, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Tasigchana, R.F.; León-Muñoz, L.M.; Lopez-Garcia, E.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Mediterranean Diet and Health-Related Quality of Life in Two Cohorts of Community-Dwelling Older Adults. PLoS ONE 2016, 11, e0151596. [Google Scholar]
- Zaragoza-Martí, A.; Ferrer-Cascales, R.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Cabañero-Martínez, M.J. Relationship Between Adherence to the Mediterranean Diet and Health-Related Quality of Life and Life Satisfaction Among Older Adults. J. Nutr. Health Ageing 2018, 22, 89–96. [Google Scholar] [CrossRef]
- Klonizakis, M.; Grammatikopoulou, M.G.; Theodoridis, X.; Milner, M.; Liu, Y.; Chourdakis, M. Effects of Long-Versus Short-Term Exposure to the Mediterranean Diet on Skin Microvascular Function and Quality of Life of Healthy Adults in Greece and the UK. Nutrients 2018, 11, 2487. [Google Scholar] [CrossRef] [Green Version]
- Godos, J.; Castellano, S.; Marranzano, M. Adherence to a Mediterranean Dietary Pattern Is Associated with Higher Quality of Life in a Cohort of Italian Adults. Nutrients 2018, 11, 981. [Google Scholar] [CrossRef] [Green Version]
- Milte, C.M.; Thorpe, M.G.; Crawford, D.; Ball, K.; McNaughton, S.A. Associations of diet quality with health-related quality of life in older Australian men and women. Exp. Gerontol. 2015, 64, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Ravens-Sieberer, U.; Erhart, M.; Wille, N.; Bullinger, M. Health-related Quality of Life in Children and Adolescents in Germany: Results of the BELLA Study. Eur. Child Adolesc. Psychiatry 2008, 17, 148–156. [Google Scholar] [CrossRef]
- Stewart, A.L.; Hays, R.D.; Wells, K.B.; Rogers, W.H.; Spritzer, K.L.; Greenfield, S. Long-term functioning and well-being outcomes associated with physical activity and exercise in patients with chronic conditions in the Medical Outcomes Study. J. Clin. Epidemiol. 1994, 47, 719–730. [Google Scholar] [CrossRef]
- Ware, J. Conceptualization and measurement of health-related quality of life: Comments on an evolving field. Arch. Phys Med. Rehabil. 2003, 84, S43–S51. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C. The Mediterranean diet: Science and practice. Public Health Nutr. 2006, 9, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrer-Cascales, R.; Albaladejo-Blázquez, N.; Ruiz-Robledillo, N.; Clement-Carbonell, V.; Sánchez-SanSegundo, M.; Zaragoza-Martí, A. Higher Adherence to the Mediterranean Diet is Related to More Subjective Happiness in Adolescents: The Role of Health-Related Quality of Life. Nutrients 2019, 11, 698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evaristo, S.; Moreira, C.; Lopes, L.; Oliveira, A.; Abreu, S.; Agostinis-Sobrinho, C.; Oliveira-Santos, J.; Póvoas, S.; Santos, R.; Mota, J. Muscular fitness and cardiorespiratory fitness are associated with health-related quality of life: Results from the LabMed Physical Activity Study. J. Exerc. Sci. Fits 2019, 17, 55–61. [Google Scholar] [CrossRef]
- Al-Mallah, M.H.; Sakr, S.; Al-Quinabet, A. Cardirespiratory fitness and cardiovascular disease prevention: An update. Curr. Atheroscler. Rep. 2018, 20, 1. [Google Scholar] [CrossRef]
- Ozemek, C.; Laddu, D.R.; Lavie, C.; Claeys, H.; Kaminsky, L.A.; Ross, R.; Wisloff, U.; Arena, R.; Blair, S.N. An Update on the Role of Cardiorespiratory Fitness, Structured Exercise and Lifestyle Physical Activity in Preventing Cardiovascular Disease and Health Risk. Prog. Cardiovasc. Dis. 2018, 61, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Kaminsky, L.A.; Arena, R.; Ellingsen, Ø.; Harber, M.P.; Myers, J.; Ozemek, C.; Ross, R. Cardiorespiratory fitness and cardiovascular disease—The past, present, and future. Prog. Cardiovasc. Dis. 2019, 62, 86–93. [Google Scholar] [CrossRef]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.L.; Kaminsky, L.A. Cardiorespiratory Fitness and Mortality in Healthy Men and Women. J. Am. Coll. Cardiol. 2018, 72, 2283–2292. [Google Scholar] [CrossRef]
- Laukkanen, J.A.; Zaccardi, F.; Khan, H.; Kurl, S.; Jae, S.Y.; Rauramaa, R. Long-term Change in Cardiorespiratory Fitness and All-Cause Mortality: A Population-Based Follow-up Study. Mayo Clin. Proc. 2016, 91, 1183–1188. [Google Scholar] [CrossRef]
- Redondo-Tébar, A.; Ruíz-Hermosa, A.; Martínez-Vizcaíno, V.; Cobo-Cuenca, A.I.; Bermejo-Cantarero, A.; Cavero-Redondo, I.; Sánchez-López, M. Associations between health-related quality of life and physical fitness in 4–7-year-old Spanish children: The MOVIKIDS study. Qual. Life Res. 2019, 28, 1751–1759. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond) 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, A.; Mota, J.; Gaspar, T.; de Matos, M.G. Associations between self-reported fitness and self-rated health, life-satisfaction and health-related quality of life among adolescents. J. Exerc. Sci. Fits 2017, 15, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Ojeda-Pardo, M.L.; Sandoval-Cuellar, C.; García-Hermoso, A.; Carrillo, H.A.; González-Ruíz, K.; Prieto-Benavides, D.H.; Tordecilla-Sanders, A.; Martinkėnas, A.; et al. Optimal Adherence to a Mediterranean Diet and High Muscular Fitness Are Associated with a Healthier Cardiometabolic Profile in Collegiate Students. Nutrients 2018, 10, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostinis-Sobrinho, C.; Santos, R.; Rosário, R.; Moreira, C.; Lopes, L.; Mota, J.; Martinkenas, A.; García-Hermoso, A.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Optimal Adherence to a Mediterranean Diet May Not Overcome the Deleterious Effects of Low Physical Fitness on Cardiovascular Disease Risk in Adolescents: A Cross-Sectional Pooled Analysis. Nutrients 2018, 10, 815. [Google Scholar] [CrossRef] [Green Version]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Ries, F.; Gisladottir, T.; Domínguez, R.; Sánchez-Oliver, A.J. Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. Int. J. Environ. Res. Public Health 2018, 15, 2632. [Google Scholar] [CrossRef] [Green Version]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Concomitant Associations between Lifestyle Characteristics and Physical Activity Status in Children and Adolescents. J. Res. Health Sci. 2019, 19, e00439. [Google Scholar]
- Yavari, A.; Javadi, M.; Mirmiran, P.; Bahadoran, Z. Exercise-Induced Oxidative Stress and Dietary Antoxidative. Asian J. Sports Med. 2015, 6, e24898. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Fisac, J.L.; Guallar-Castillón, P.; León-Muñoz, L.M.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: The ENRICA study. Obes. Rev. 2012, 13, 388–392. [Google Scholar] [CrossRef]
- Schroeder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-aventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 41, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Bamia, C.; Martimianaki, G.; Kritikou, M.; Trichopoulou, A. Indexes for assessing adherence to a Mediterranean diet from data measured through brief questionnaires: Issues raised from the analysis of a Greek population study. Curr. Dev. Nutr. 2017, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Cuenca, A.I.; Garrido-Miguel, M.; Soriano-Cano, A.; Ferri-Morales, A.; Martínez-Vizcaíno, V.; Martín-Espinosa, N.M. Adherence to the Mediterranean Diet and Its Association with Body Composition and Physical Fitness in Spanish University Students. Nutrients 2019, 11, 2830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Pérez-Baurer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreiras, O.; Carbajal, A.; Cabrera, L. Tablas De Composicion de Alimentos [Food Composition Tables], 9th ed.; Editorial Piramide: Madrid, Spain, 2005. [Google Scholar]
- Alonso, J.; Regidor, E.; Barrio, G.; Prieto, L.; Rodríguez, C.; Dela Fuente, L. Population reference values of the Spanish version of the Health Questionnaire SF-36. Med. Clin. 1998, 111, 410–416. [Google Scholar]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Organization World Health. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 meters shuttle run test for aerobic fitness. J. Sports Sci. 1998, 6, 93–101. [Google Scholar] [CrossRef]
- Domingo-Salvany, A.; Regidor, E.; Alonso, J.; Alvarez-Dardet, C. Proposal for a social class measure. Working Group of the Spanish Society of Epidemiology and the Spanish Society of Family and Community Medicine. Aten. Prim. 2000, 25, 350–363. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The Moderator–Mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Grao-Cruces, A.; Fernández-Martínez, A.; Nuviala, A. Association of fitness with life satisfaction, health risk behaviors, and adherence to the Mediterranean diet in Spanish adolescents. J. Strength Cond. Res. 2014, 28, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Grao-Cruces, A.; Nuviala, A.; Fernández-Martínez, A.; Porcel-Gálvez, A.M.; Moral-García, J.E.; Martínez-López, E.J. Adherence to the Mediterranean diet in rural and urban adolescents of southern Spain, life satisfaction, anthropometry, and physical and sedentary activities. Nutr. Hosp. 2013, 28, 1129–1135. [Google Scholar]
- Bolton, K.A.; Jacka, F.; Allender, S.; Kremer, P.; Gibbs, L.; Waters, E.; de Silva, A. The association between self-reported diet quality and health-related quality of life in rural and urban Australian adolescents. Aust. J. Rural Health 2016, 24, 317–325. [Google Scholar] [CrossRef]
- Knox, E.; Muros, J.J. Association of lifestyle behaviourellrs with self-esteem through health-related quality of life in Spanish adolescents. Eur. J. Pediatr. 2017, 176, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Zervaki, K.; Yiannakouris, N.; Sdrali, D.; Costarelli, V. Diet quality, disordered eating and health-related quality of life in Greek adolescents. Nutr. Food Sci. 2017, 41, 511–521. [Google Scholar] [CrossRef]
- Wu, X.Y.; Zhuang, L.H.; Li, W.; Guo, H.W.; Zhang, J.H.; Zhao, Y.K.; Hu, J.W.; Gao, Q.Q.; Luo, S.; Ohinmaa, A.; et al. The influence of diet quality and dietary behavior on health-related quality of life in the general population of children and adolescents: A systematic review and meta-analysis. Qual. Life Res. 2019, 28, 1989–2015. [Google Scholar] [CrossRef]
- Ruano, C.; Henriquez, P.; Martínez-González, M.Á.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Sánchez-Villegas, A. Empirically derived dietary patterns and health-related quality of life in the SUN project. PLoS ONE 2013, 8, e61490. [Google Scholar] [CrossRef] [Green Version]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Pounis, G.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Adherence to a Mediterranean Diet Is Associated With a Better Health-Related Quality of Life: A Possible Role of High Dietary Antioxidant Content. BMJ Open 2013, 3, e003003. [Google Scholar] [CrossRef] [Green Version]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship Between Diet and Mental Health in Children and Adolescents: A Systematic Review. Am. J. Public Health 2014, 104, e31–e42. [Google Scholar] [CrossRef] [PubMed]
- Khalid, S.; Williams, C.M.; Reynolds, S.A. Is there an association between diet and depression in children and adolescents? A systematic review. Br. J. Nutr. 2017, 116, 2097–2108. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2013, 99, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Delgado-Rodríguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Majem, L.S.; Martínez-González, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra Follow-up. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef]
- Sanhueza, C.; Ryan, L.; Foxcroft, D.R. Diet and the risk of unipolar depression in adults: Systematic review of cohort studies. J. Hum. Nutr. Diet. 2012, 26, 56–70. [Google Scholar] [CrossRef]
- Gómez-Pinilla, F. Brain foods: The effects of nutrients on brain function. Nat. Rev. Neurosci. 2008, 9, 568–578. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional modulation of cognitive function and mental health. J. Nutr Biochem. 2013, 24, 724–743. [Google Scholar] [CrossRef] [Green Version]
- Evaristo, O.S.; Moreira, C.; Lopes, L.; Abreu, S.; Agostinis-Sobrinho, C.; Oliveira-Santos, J.; Póvoas, S.; Oliveira, A.; Santos, R.; Mota, J. Associations between physical fitness and adherence to the Mediterranean diet with health-related quality of life in adolescents: Results from the LabMed Physical Activity Study. Eur. J. Public Health 2018, 28, 631–635. [Google Scholar] [CrossRef]
- Helseth, S.; Haraldstad, K.; Christophersen, K.-A. A cross-sectional study of Health Related Quality of Life and body mass index in a Norwegian school sample (8–18 years): A comparison of child and parent perspectives. Health Qual. Life Outcomes 2015, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bolton, K.; Kremer, P.; Rossthorn, N.; Moodie, M.; Gibbs, L.; Waters, E.; Swinburn, B.; de Silva, A. The effect of gender and age on the association between weight status and health-related quality of life in Australian adolescents. BMC Public Health 2014, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelqvist-Schmidlechner, K.; Vaara, J.P.; Vasankari, T.; Häkkinen, A.; Mäntysaari, M.; Kyröläinen, H. Muscular and cardiorespiratory fitness are associated with health-related quality of life among young adult men. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.R.; Natvig, G.K.; Aadland, E.; Moe, V.F.; Kolotkin, R.L.; Anderssen, S.A.; Resaland, G.K. Associations between health-related quality of life, cardiorespiratory fitness, muscle strength, physical activity and waist circumference in 10-year-old children: The ASK study. Qual. Life Res. 2017, 26, 3421–3428. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Stubbs, B.; Osborn, D.; Hayes, J. The association between cardiorespiratory fitness and the incidence of common mental health disorders: A systematic review and meta-analysis. J. Affect. Disord. 2019, 257, 748–757. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Debbia, F.; Rodríguez-Muñoz, P.M.; Carmona-Torres, J.M.; Hidalgo-Lopezosa, P.; Cobo-Cuenca, A.I.; López-Soto, P.J.; Rodríguez-Borrego, M.A. Association between Physical Activity, Food Consumption and Depressive Symptoms among Young Adults in Spain: Findings of a National Survey. Issues Mental Health Nurs. 2020, 41, 59–65. [Google Scholar] [CrossRef]
- Jakobsen, L.H.; Rask, I.K.; Kondrup, J. Validation of handgrip strength and endurance as a measure of physical function and quality of life in healthy subjects and patients. Nutrition 2010, 26, 542–550. [Google Scholar] [CrossRef]
- Hart, P.D. Relationship between Muscular Fitness, Health Behaviors, and Health-related Quality of Life in US Women. Am. J. Sports Sci. Med. 2020, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; García-Pinillos, F.; Latorre-Román, P.Á. Handgrip strength is associated with psychological functioning, mood and sleep in women over 65 years. Int. J. Environ. Res. Public Health 2019, 16, 873. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.Y.; Lim, J.; Park, H.S. Relationship between low handgrip strength and quality of life in Korean men and women. Qual. Life Res. 2018, 27, 2571–2580. [Google Scholar] [CrossRef]
- Kwak, Y.; Kim, Y. Quality of life and subjective health status according to handgrip strength in the elderly: Across-sectional study. Aging Ment. Health 2019, 23, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Moratalla-Cecilia, N.; Soriano-Maldonado, A.; Ruiz-Cabello, P.; Fernández, M.; Gregorio-Arenas, E.; Aranda, P.; Aparicio, V. Association of physical fitness with health-related quality of life in early postmenopause. Qual Life Res. 2016, 25, 2675–2681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Sousa, M.A.; Olivares, P.R.; García-Hermoso, A.; Gusi, N. Fitness as a Mediator of the Enhancement of Quality of Life after a 6-Months Exercise Program. Res. Q. Exerc. Sport 2020, 91, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.N.; Deuster, P.A. Biological mechanisms underlying the role of physical fitness in health and resilience. Interface Focus 2014, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuenca-García, M.; Ortega, F.B.; Huybrechts, I.; Ruiz, J.R.; González-Gross, M.; Ottevaere, C.; Sjöström, M.; Dìaz, L.E.; Ciarapica, D.; Molnar, D.; et al. Cardiorespiratory fitness and dietary intake in Europeanadolescents: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 1850–1859. [Google Scholar] [CrossRef] [Green Version]
- Shikany, J.M.; Jacobs, D.R.; Lewis, C.E.; Steen, L.M.; Sternfeld, B.; Carnethon, M.R.; Richman, J.S. Associations between food groups, dietary patterns, and cardiorespiratory fitness in the Coronary Artery Risk Development. Am. J. Clin. Nutr. 2013, 98, 1402–14096. [Google Scholar] [CrossRef] [Green Version]
- Pires-Junior, R.; Coledam, D.; de Aguiar Greca, J.; de Arruda, G.; Teixeira, M.; de Oliveira, A. Physical fitness and health-related quality of life in Brazilian adolescents: A cross-sectional study. Hum. Movement 2018, 19. [Google Scholar] [CrossRef]
- Loprinzi, P.; Addoh, O.; Wong Sarver, N.; Espinoza, I.; Mann, J. Cross-sectional association of exercise, strengthening activities, and cardiorespiratory fitness on generalized anxiety, panic and depressive symptoms. Postgrad Med. J. 2017, 129, 676–685. [Google Scholar] [CrossRef]
- Oliveira, A.; Maranhao Neto, G.; Barros, O.; Pedreiro, R.; Murillo-Rodriguez, E.; Ponce de Leon, A.; Machado, S. Association between physical fitness and psychological distress among Brazilian armed force personnel. Sport Sci. Health 2019, 15, 141–147. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All (n = 310) | Men (n = 108) | Women (n = 202) | p * | |
|---|---|---|---|---|
| Age (years) | 20.9 ± 2.5 | 21.1 ± 2.8 | 20.7 ± 2.3 | 0.146 |
| Weight (Kg) | 65.4 ± 12.3 | 72.6 ± 10.99 | 61.4 ± 11.1 | <0.001 |
| Height (cm) | 167.3 ± 8.6 | 175.3 ± 7.0 | 162.9 ± 5.8 | <0.001 |
| Waist circumference (cm) | 78.9 ± 9.3 | 83.0 ± 7.9 | 76.6 ± 9.2 | <0.001 |
| % Fat mass | 29.3 ± 9.0 | 20.5 ± 6.3 | 33.7 ± 6.7 | <0.001 |
| Total lean mass (Kg) | 43.0 ± 9.3 | 53.5 ± 6.8 | 37.8 ± 4.9 | <0.001 |
| BMI (Kg/m2) | 23.3 ± 3.5 | 23.5 ± 3.03 | 23.1 ± 3.8 | 0.269 |
| Underweight (%) | 3.1 | 0.8 | 4.4 | |
| Normal weight (%) | 70.6 | 70.6 | 70.6 | 0.068 |
| Overweight (%) | 21.8 | 26.2 | 19.3 | |
| Obesity (%) | 4.5 | 2.4 | 5.7 | |
| CRF (stages) | 5.8 ± 2.6 | 7.0 ± 1.9 | 3.8 ± 1.4 | <0.001 |
| CRF (VO2 max estimate, ml/Kg/min) | 37.5 ± 8.0 | 44.4 ± 6.6 | 32.8 ± 4.9 | <0.001 |
| Muscle strength index (cm/Kg) a | 0.013 ± 1.7 | 1.523 ± 1.2 | −1.050 ± 1.2 | <0.001 |
| Handgrip strength (Kg) | 30.4 ± 9.5 | 39.2 ± 7.7 | 24.4 ± 4.7 | <0.001 |
| Standing long jump (cm) | 161.2 ± 43.7 | 195.5 ± 31.9 | 136.8 ± 33.5 | <0.001 |
| EI (Kcal) | 2795.7 ± 1804.7 | 2865.9 ± 1287.0 | 2757.6 ± 2033.2 | 0.590 |
| Carbohydrate (% EI) | 43.0 ± 7.1 | 43.1 ± 6.6 | 42.9 ± 7.3 | 0.852 |
| Protein (% EI) | 17.4 ± 3.4 | 17.4 ± 3.2 | 17.5 ± 3.6 | 0.749 |
| Fat (% EI) | 38.2 ± 6.2 | 37.9 ± 5.9 | 38.3 ± 6.3 | 0.578 |
| Health-related quality of life b (SF-12) | ||||
| PCS | 54.7 ± 5.5 | 54.7 ± 5.3 | 54.6 ± 5.6 | 0.827 |
| MCS | 40.0 ± 6.4 | 42.1 ± 5.9 | 38.6 ± 6.4 | <0.001 |
| Adherence Mediterranean Diet (%) | ||||
| Low adherence | 65.4 | 70.4 | 79.0 | 0.090 |
| Good adherence | 24.0 | 29.6 | 21.0 | |
| Total score MEDAS | 7.0 ± 2.0 | 7.2 ± 1.9 | 6.9 ± 2.0 | 0.214 |
| PCS | MCS | BMI | WC | % Fat Mass | Total Lean Mass | CRF (Steges) | CRF (VO2 Max Estimate) | Handgrip Strength | Total EI | Total Score MEDAS | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PCS | - | −0.446 * | −0.240 ** | −0.223 ** | −0.252 ** | −0.014 | 0.124 | 0.129 * | −0.102 | 0.018 | 0.023 |
| MCS | - | 0.075 | 0.156 ** | −0.030 | 0.272 ** | 0.279 ** | 0.272 ** | 0.335 ** | 0.044 | 0.160 ** | |
| BMI | - | 0.802 ** | 0.493 ** | 0.337 ** | −0.188 ** | −0.190 ** | 0.224 ** | −0.116 * | 0.164 ** | ||
| WC | - | 0.217 * | 0.544 * | −0.007 | −0.010 | 0.383 ** | −0.057 | 0.130 * | |||
| % Fat mass | - | −0.496 ** | −0.548 ** | −0.540 ** | −0.390 ** | −0.166 ** | 0.016 | ||||
| Total lean mass | - | 0.628 ** | 0.621 ** | 0.780 ** | −0.061 | 0.144 * | |||||
| CRF (stages) | - | 0.996 ** | 0.597 ** | 0.188 ** | 0.155 * | ||||||
| CRF (VO2 max estimate) | - | 0.589 ** | 0.176 ** | 0.155 * | |||||||
| Handgrip strength | - | 0.101 | 0.139 * | ||||||||
| Total EI | - | 0.088 |
| CRF (VO2 Max Estimate, mL/Kg/min) | Handgrip Strength (Kg) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Low | Medium | High | p | ES d | Low | Medium | High | p | ES d | |
| n | 60 | 121 | 66 | 65 | 132 | 63 | ||||
| PCS | ||||||||||
| Model 0 | 53.5 ± 6.9 a | 55.7 ± 5.2 | 55.6 ± 4.6 | 0.031 | 0.03 | 56.1 ± 4.7 | 55.1 ± 5.9 | 54.5 ± 5.3 | 0.251 | 0.01 |
| Model 1 | 52.8 ± 6.0 a,c | 55.5 ± 5.2 | 56.6 ± 4.5 | 0.007 | 0.04 | 56.5 ± 4.3 | 55.1 ± 5.9 | 53.9 ± 5.2 | 0.157 | 0.01 |
| MCS | ||||||||||
| Model 0 | 38.1± 7.1 a,c | 38.7 ± 6.3 b | 42.8 ± 6.1 | <0.001 | 0.08 | 37.5 ± 6.8 a | 39.0 ± 6.1 b | 42.9 ± 6.3 | <0.001 | 0.09 |
| Model 1 | 38.57 ± 7.2 | 38.98 ± 6.3 b | 42.0 ± 6.2 | 0.044 | 0.02 | 38.2 ± 6.8 | 39.2 ± 6.2 | 41.8 ± 6.4 | 0.055 | 0.02 |
| Total MEDAS | ||||||||||
| Model 0 | 6.7 ± 2.0 a | 6.9 ± 2.1 | 7.6 ± 2.1 | 0.050 | 0.03 | 6.3 ± 1.9 | 7.0 ± 2.1 | 7.5 ± 2.2 | 0.040 | 0.03 |
| Model 1 | 6.5 ± 2.0 a | 6.8 ± 2.0 | 7.7 ± 2.1 | 0.067 | 0.03 | 6.3 ± 2.0 a | 7.1 ± 2.1 | 7.5 ± 2.2 | 0.052 | 0.02 |
| Adherence to the MD | ||||
|---|---|---|---|---|
| Low Adherence | Good Adherence | p | ES a | |
| n | 232 | 74 | ||
| PCS | ||||
| Model 0 | 54.5 ± 5.4 | 54.4 ± 5.1 | 0.728 | 0.001 |
| Model 1 | 54.7 ± 5.0 | 54.5 ± 5.0 | 0.819 | 0.001 |
| Model 2 | 55.3 ± 5.6 | 55.8 ± 5.1 | 0.573 | 0.001 |
| Model 3 | 55.2 ± 4.9 | 55.4 ± 5.0 | 0.683 | 0.001 |
| MCS | ||||
| Model 0 | 39.6 ± 6.7 | 41.4 ± 5.7 | 0.044 | 0.013 |
| Model 1 | 39.5 ± 6.6 | 41.1 ± 5.8 | 0.095 | 0.009 |
| Model 2 | 39.3 ± 6.8 | 40.9 ± 6.0 | 0.113 | 0.011 |
| Model 3 | 39.2 ± 5.9 | 40.9 ± 6.8 | 0.089 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Espinosa, N.M.; Garrido-Miguel, M.; Martínez-Vizcaíno, V.; González-García, A.; Redondo-Tébar, A.; Cobo-Cuenca, A.I. The Mediating and Moderating Effects of Physical Fitness of the Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life in University Students. Nutrients 2020, 12, 3578. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113578
Martín-Espinosa NM, Garrido-Miguel M, Martínez-Vizcaíno V, González-García A, Redondo-Tébar A, Cobo-Cuenca AI. The Mediating and Moderating Effects of Physical Fitness of the Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life in University Students. Nutrients. 2020; 12(11):3578. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113578
Chicago/Turabian StyleMartín-Espinosa, Noelia María, Miriam Garrido-Miguel, Vicente Martínez-Vizcaíno, Alberto González-García, Andrés Redondo-Tébar, and Ana Isabel Cobo-Cuenca. 2020. "The Mediating and Moderating Effects of Physical Fitness of the Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life in University Students" Nutrients 12, no. 11: 3578. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113578