Association between Habitual Dietary Iron Intake and Glucose Metabolism in Individuals after Acute Pancreatitis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ascertainment of Dietary Intake
2.3. Markers of Glucose Metabolism
2.4. Definitions of Covariates
2.5. Statistical Analyses
3. Results
3.1. Study Cohort
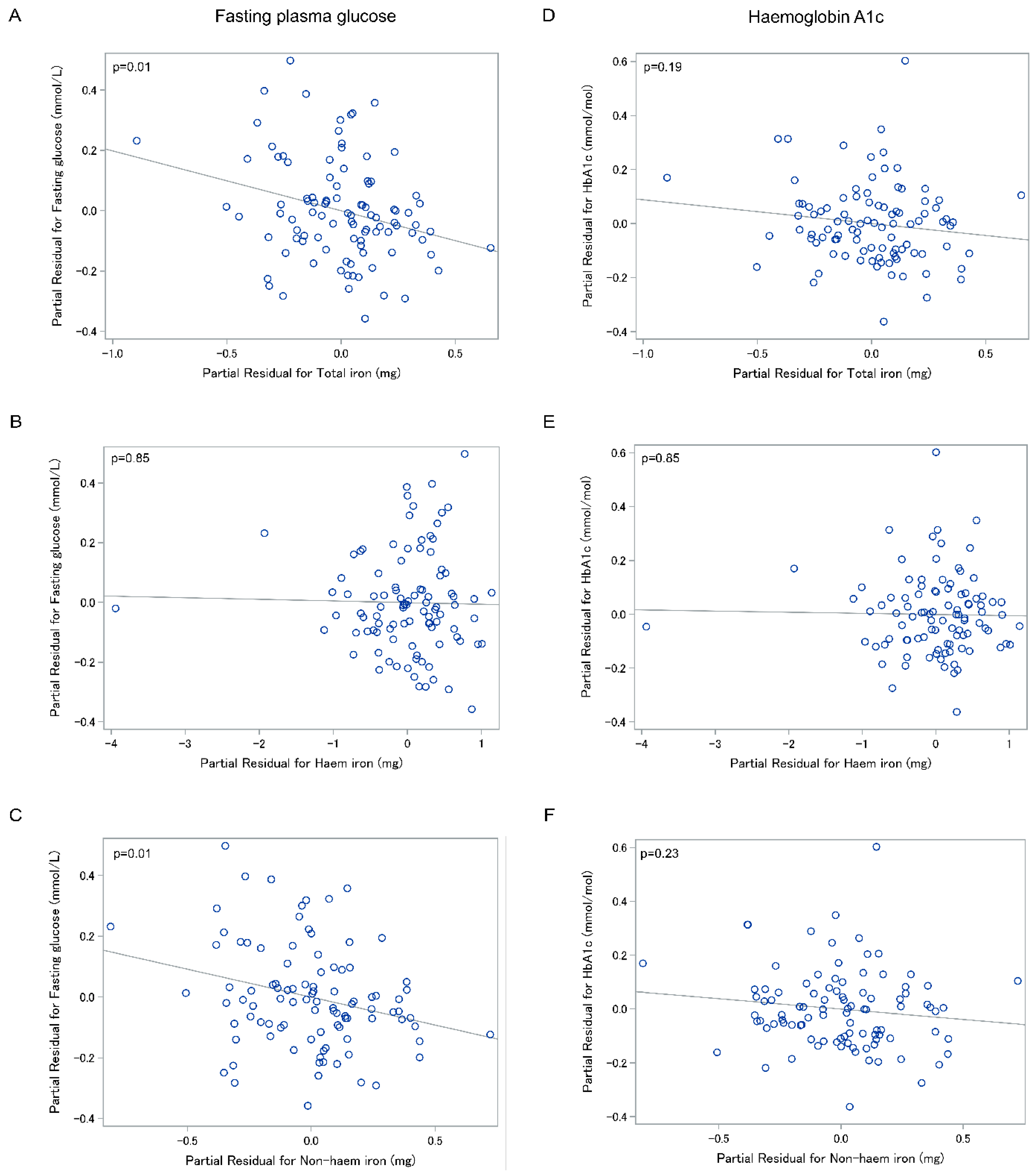
3.2. Association between Fasting Plasma Glucose and Dietary Iron
3.3. Association between Haemoglobin A1c and Dietary Iron
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dos Santos Vieira, D.A.; Hermes Sales, C.; Galvão Cesar, C.L.; Marchioni, D.M.; Fisberg, R.M. Influence of haem, non-haem, and total iron intake on metabolic syndrome and its components: A population-based study. Nutrients 2018, 10, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Z.; Wu, F.; Lu, Y.; Wu, C.; Wang, Z.; Zang, J.; Guo, C.; Jia, X.; Yao, J.; Peng, H.; et al. Total and nonheme dietary iron intake is associated with metabolic syndrome and its components in Chinese men and women. Nutrients 2018, 10, 1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Zhou, M.; Yuan, B.; Qi, L.; Dai, Y.; Luo, Y.; Holmboe-Ottesen, G. Iron intake and body iron stores, anaemia and risk of hyperglycaemia among Chinese adults: The prospective Jiangsu Nutrition Study (JIN). Public Health Nutr. 2010, 13, 1319–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.Y.; Zhong, R.H.; Long, J.A.; Fang, A.; Zhu, H. Dietary iron intake and incident type 2 diabetes in Chinese middle-aged and elderly population: A prospective cohort study. Curr. Dev. Nutr. 2020, 4, 47. [Google Scholar] [CrossRef]
- Jiang, R.; Ma, J.; Ascherio, A.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Dietary iron intake and blood donations in relation to risk of type 2 diabetes in men: A prospective cohort study. Am. J. Clin. Nutr. 2004, 79, 70–75. [Google Scholar] [CrossRef] [Green Version]
- Wlazlo, N.; van Greevenbroek, M.M.; Ferreira, I.; Jansen, E.H.; Feskens, E.J.; van der Kallen, C.J.; Schalkwijk, C.G.; Bravenboer, B.; Stehouwer, C.D. Iron metabolism is prospectively associated with insulin resistance and glucose intolerance over a 7-year follow-up period: The CODAM study. Acta Diabetol. 2014, 52, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Montonen, J.; Boeing, H.; Steffen, A.; Lehmann, R.; Fritsche, A.; Joost, H.G.; Schulze, M.B.; Pischon, T. Body iron stores and risk of type 2 diabetes: Results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam study. Diabetologia 2012, 55, 2613–2621. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Zong, G.; Pan, A.; Ye, X.; Li, H.; Yu, Z.; Zhao, Y.; Zou, S.; Yu, D.; Jin, Q.; et al. Elevated plasma ferritin is associated with increased incidence of type 2 diabetes in middle-aged and elderly Chinese adults. J. Nutr. 2013, 143, 1459–1465. [Google Scholar] [CrossRef]
- Jiang, R.; Manson, J.E.; Meigs, J.B.; Ma, J.; Rifai, N.; Hu, F.B. Body iron stores in relation to risk of type 2 diabetes in apparently healthy women. JAMA 2004, 291, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Forouhi, N.G.; Harding, A.H.; Allison, M.; Sandhu, M.S.; Welch, A.; Luben, R.; Bingham, S.; Khaw, K.T.; Wareham, N.J. Elevated serum ferritin levels predict new-onset type 2 diabetes: Results from the EPIC-Norfolk prospective study. Diabetologia 2007, 50, 949–956. [Google Scholar] [CrossRef] [Green Version]
- Huth, C.; Beuerle, S.; Zierer, A.; Heier, M.; Herder, C.; Kaiser, T.; Koenig, W.; Kronenberg, F.; Oexle, K.; Rathmann, W.; et al. Biomarkers of iron metabolism are independently associated with impaired glucose metabolism and type 2 diabetes: The KORA F4 study. Eur. J. Endocrinol. 2015, 173, 643–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.L.; Singh, P.P.; Phillips, A.R.; Murphy, R.; Windsor, J.A.; Petrov, M.S. Newly diagnosed diabetes mellitus after acute pancreatitis: A systematic review and meta-analysis. Gut 2014, 63, 818–831. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Yadav, D. Global epidemiology and holistic prevention of pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Gillies, N.A.; Pendharkar, S.A.; Singh, R.G.; Asrani, V.M.; Petrov, M.S. Lipid metabolism in patients with chronic hyperglycemia after an episode of acute pancreatitis. Diabetes Metab. Syndr. 2017, 11 (Suppl. S1), S233–S241. [Google Scholar] [CrossRef]
- Xiao, A.Y.; Tan, M.L.; Wu, L.M.; Asrani, V.M.; Windsor, J.A.; Yadav, D.; Petrov, M.S. Global incidence and mortality of pancreatic diseases: A systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol. Hepatol. 2016, 1, 45–55. [Google Scholar] [CrossRef]
- Chand, S.K.; Singh, R.G.; Pendharkar, S.A.; Petrov, M.S. Iron: A strong element in the pathogenesis of chronic hyperglycaemia after acute pancreatitis. Biol. Trace Elem. Res. 2018, 183, 71–79. [Google Scholar] [CrossRef]
- Shen, H.N.; Yang, C.C.; Chang, Y.H.; Lu, C.L.; Li, C.Y. Risk of diabetes mellitus after first-attack acute pancreatitis: A national population-based study. Am. J. Gastroenterol. 2015, 110, 1698–1706. [Google Scholar] [CrossRef]
- Bharmal, S.H.; Cho, J.; Alarcon Ramos, G.C.; Ko, J.; Stuart, C.E.; Modesto, A.E.; Singh, R.G.; Petrov, M.S. Trajectories of glycaemia following acute pancreatitis: A prospective longitudinal cohort study with 24 months follow-up. J. Gastroenterol. 2020, 55, 775–788. [Google Scholar] [CrossRef]
- Petrov, M.S. Panorama of mediators in postpancreatitis diabetes mellitus. Curr. Opin. Gastroenterol. 2020, 36, 443–451. [Google Scholar] [CrossRef]
- Fernández-Real, J.M.; McClain, D.; Manco, M. Mechanisms linking glucose homeostasis and iron metabolism toward the onset and progression of type 2 diabetes. Diabetes Care 2015, 38, 2169–2176. [Google Scholar] [CrossRef] [Green Version]
- Miyamori, A.; Takebe, T.; Yamagata, S. Clinical evaluation of iron metabolism in pancreatic disease. Tohoku J. Exp. Med. 1976, 118, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.; Badenoch, J. Iron absorption in pancreatic disease. Lancet 1962, 280, 6–8. [Google Scholar] [CrossRef]
- Kimita, W.; Petrov, M.S. Iron metabolism and the exocrine pancreas. Clin. Chim. Acta 2020, 511, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Maraví Poma, E.; Zubia Olascoaga, F.; Petrov, M.S.; Navarro Soto, S.; Laplaza Santos, C.; Morales Alava, F.; Darnell Martin, A.; Gorraiz López, B.; Bolado Concejo, F.; Casi Villarroya, M.; et al. SEMICYUC 2012. Recommendations for intensive care management of acute pancreatitis. Med. Intensiva 2013, 37, 163–179. [Google Scholar] [CrossRef]
- Mulligan, A.A.; Luben, R.N.; Bhaniani, A.; Parry-Smith, D.J.; O’Connor, L.; Khawaja, A.P.; Forouhi, N.G.; Khaw, K. A new tool for converting food frequency questionnaire data into nutrient and food group values: FETA research methods and availability. BMJ Open 2014, 4, e004503. [Google Scholar] [CrossRef] [Green Version]
- Stuart, C.E.; Singh, R.G.; Alarcon Ramos, G.C.; Priya, S.; Ko, J.; DeSouza, S.V.; Cho, J.; Petrov, M.S. Relationship of pancreas volume to tobacco smoking and alcohol consumption following pancreatitis. Pancreatology 2020, 20, 60–67. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Luan, D.C.; Li, H.; Li, S.J.; Zhao, Z.; Li, X.; Liu, Z.M. Body iron stores and dietary iron intake in relation to diabetes in adults in North China. Diabetes Care 2008, 31, 285–286. [Google Scholar] [CrossRef] [Green Version]
- Shi, Z.; Hu, X.; Yuan, B.; Pan, X.; Meyer, H.E.; Holmboe-Ottesen, G. Association between serum ferritin, hemoglobin, iron intake, and diabetes in adults in Jiangsu, China. Diabetes Care 2006, 29, 1878–1883. [Google Scholar] [CrossRef] [Green Version]
- Esfandiar, Z.; Hosseini-Esfahani, F.; Mirmiran, P.; Habibi-Moeini, A.S.; Azizi, F. Red meat and dietary iron intakes are associated with some components of metabolic syndrome: Tehran Lipid and Glucose Study. J. Transl. Med. 2019, 17, 313. [Google Scholar] [CrossRef]
- Prynne, C.J.; Mander, A.; Wadsworth, M.E.; Stephen, A.M. Diet and glycosylated haemoglobin in the 1946 British birth cohort. Eur. J. Clin. Nutr. 2009, 63, 1084–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazanfari, Z.; Haghdoost, A.A.; Alizadeh, S.M.; Atapour, J.; Zolala, F. A comparison of HbA1c and fasting blood sugar tests in general population. Int. J. Prev. Med. 2010, 1, 187–194. [Google Scholar] [PubMed]
- Petrov, M.S. Diabetes of the exocrine pancreas: American Diabetes Association-compliant lexicon. Pancreatology 2017, 17, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Kowalkowska, J.; Slowinska, M.A.; Slowinski, D.; Dlugosz, A.; Niedzwiedzka, E.; Wadolowska, L. Comparison of a full food-frequency questionnaire with the three-day unweighted food records in young Polish adult women: Implications for dietary assessment. Nutrients 2013, 5, 2747–2776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.G.; Nguyen, N.N.; DeSouza, S.V.; Pendharkar, S.A.; Petrov, M.S. Comprehensive analysis of body composition and insulin traits associated with intra-pancreatic fat deposition in healthy individuals and people with new-onset prediabetes/diabetes after acute pancreatitis. Diabetes Obes. Metab. 2019, 21, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.K.; Pendharkar, S.A.; Bharmal, S.H.; Bartlett, A.S.; Pandol, S.J.; Petrov, M.S. Frequency and risk factors for liver disease following pancreatitis: A population-based cohort study. Dig. Liver Dis. 2019, 51, 551–558. [Google Scholar] [CrossRef]
- Cho, J.; Dalbeth, N.; Petrov, M.S. Relationship between gout and diabetes mellitus after acute pancreatitis: A nationwide cohort study. J. Rheumatol. 2020, 47, 917–923. [Google Scholar] [CrossRef]
- Pendharkar, S.A.; Mathew, J.; Petrov, M.S. Age- and sex-specific prevalence of diabetes associated with diseases of the exocrine pancreas: A population-based study. Dig. Liver Dis. 2017, 49, 540–544. [Google Scholar] [CrossRef]
- Miret, S.; Simpson, R.J.; McKie, A.T. Physiology and molecular biology of dietary iron absorption. Annu. Rev. Nutr. 2003, 23, 283–301. [Google Scholar] [CrossRef]
- West, A.R.; Oates, P.S. Mechanisms of heme iron absorption: Current questions and controversies. World J. Gastroenterol. 2008, 14, 4101–4110. [Google Scholar] [CrossRef]
- Fuqua, B.K.; Vulpe, C.D.; Anderson, G.J. Intestinal iron absorption. J. Trace Elem. Med. Biol. 2012, 26, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Samaniego-Vaesken, M.; Partearroyo, T.; Olza, J.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G. Iron intake and dietary sources in the Spanish population: Findings from the ANIBES study. Nutrients 2017, 9, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Li, S.; Liu, G.; Yan, F.; Ma, X.; Huang, Z.; Tian, H. Body iron stores and heme-iron intake in relation to risk of type 2 diabetes: A systematic review and meta-analysis. PLoS ONE 2012, 7, e41641. [Google Scholar] [CrossRef] [PubMed]
- Sharp, P.; Srai, S.K. Molecular mechanisms involved in intestinal iron absorption. World J. Gastroenterol. 2007, 13, 4716–4724. [Google Scholar] [CrossRef]
- Chand, S.K.; Singh, R.G.; Pendharkar, S.A.; Bharmal, S.H.; Petrov, M.S. Interplay between innate immunity and iron metabolism after acute pancreatitis. Cytokine 2018, 103, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S. Metabolic trifecta after pancreatitis: Exocrine pancreatic dysfunction, altered gut microbiota, and new-onset diabetes. Clin. Transl. Gastroenterol. 2019, 10, 4–6. [Google Scholar] [CrossRef]
- Cho, J.; Scragg, R.; Petrov, M.S. The influence of cholecystectomy and recurrent biliary events on the risk of post-pancreatitis diabetes mellitus: A nationwide cohort study in patients with first attack of acute pancreatitis. HPB 2020. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, S.; Tian, Y. Cholecystectomy as a risk factor of metabolic syndrome: From epidemiologic clues to biochemical mechanisms. Lab. Investig. 2018, 98, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Zweers, S.J.; Booij, K.A.; Komuta, M.; Roskams, T.; Gouma, D.J.; Jansen, P.L.; Schaap, F.G. The human gallbladder secretes fibroblast growth factor 19 into bile: Towards defining the role of fibroblast growth factor 19 in the enterobiliary tract. Hepatology 2012, 55, 575–5783. [Google Scholar] [CrossRef]
- Barrera, F.; Azocar, L.; Molina, H.; Schalper, K.A.; Ocares, M.; Liberona, J.; Villarroel, L.; Pimentel, F.; Pérez-Ayuso, R.M.; Nervi, F.; et al. Effect of cholecystectomy on bile acid synthesis and circulating levels of fibroblast growth factor 19. Ann. Hepatol. 2015, 14, 710–721. [Google Scholar] [CrossRef]
- Yoon, W.; Kim, H.N.; Park, E.; Ryu, S.; Chang, Y.; Shin, H.; Kim, H.L.; Yi, S. The impact of cholecystectomy on the gut microbiota: A case-control study. J. Clin. Med. 2019, 8, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utzschneider, K.M.; Kratz, M.; Damman, C.J.; Hullar, M. Mechanisms linking the gut microbiome and glucose metabolism. J. Clin. Endocrinol. Metab. 2016, 101, 1445–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, O.C.; Olier, M.; Ellero-Simatos, S.; Naud, N.; Dupuy, J.; Huc, L.; Taché, S.; Graillot, V.; Levêque, M.; Bézirard, V.; et al. Haem iron reshapes colonic luminal environment: Impact on mucosal homeostasis and microbiome through aldehyde formation. Microbiome 2019, 7, 6–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Mean (SD) or n (%) |
|---|---|
| Age (years) | 56.22 (14.82) |
| Men | 73 (70) |
| BMI category | |
| <18.5 kg/m2 | 1 (1) |
| 18.5–25 kg/m2 | 32 (29) |
| 25.1–29.9 kg/m2 | 38 (35) |
| ≥30 kg/m2 | 38 (35) |
| Tobacco smoking | |
| Yes | 45 (43) |
| No | 59 (57) |
| Alcohol consumption (g/day) | 11.41 (18.21) |
| Haemoglobin A1c (mmol/mol) | 40.03 (10.67) |
| Fasting plasma glucose (mmol/L) | 5.86 (1.64) |
| Triglycerides (mmol/L) | 2.16 (3.06) |
| Aetiology | |
| Biliary | 58 (58) |
| Non-biliary | 42 (42) |
| Recurrence | |
| Yes | 31 (30) |
| No | 71 (70) |
| Energy (kcal/day) | 1734.94 (674.43) |
| Total iron (mg/day) | 10.16 (4.14) |
| Haem iron (mg/day) | 0.87 (0.45) |
| Non-haem iron (mg/day) | 9.29 (3.94) |
| (A) Fasting Plasma Glucose | (B) Haemoglobin A1c | ||||||
|---|---|---|---|---|---|---|---|
| Dietary Iron | |||||||
| Model | n | β Coefficient (95% CI) | p | n | β Coefficient (95% CI) | p | |
| Total iron (mg) | 1 | 109 | −0.05 (−0.15, 0.05) | 0.30 | 108 | −0.03 (−0.12, 0.07) | 0.60 |
| 2 | 109 | −0.27 (−0.43, −0.10) | <0.01 | 108 | −0.19 (−0.35, 0.03) | 0.09 | |
| 3 | 109 | −0.25 (−0.41, −0.09) | <0.01 | 108 | −0.17 (−0.33, −0.02) | 0.09 | |
| 4 | 104 | −0.24 (−0.42, −0.07) | 0.01 | 103 | −0.16 (−0.32, 0.01) | 0.12 | |
| 5 | 100 | −0.21 (−0.38, −0.05) | 0.01 | 99 | −0.13(−0.29, 0.03) | 0.17 | |
| 6 | 100 | −0.19 (−0.35, −0.05) | 0.01 | 99 | −0.09 (−0.22, 0.04) | 0.23 | |
| Haem iron (mg) | 1 | 109 | <−0.01 (−0.06, 0.06) | 0.18 | 108 | <−0.01 (−0.06, 0.05) | 0.99 |
| 2 | 109 | −0.01 (−0.08, −0.05) | 0.08 | 108 | −0.02 (−0.08, 0.05) | 0.99 | |
| 3 | 109 | −0.02 (−0.08, −0.04) | 0.08 | 108 | −0.02 (−0.08, 0.04) | 0.99 | |
| 4 | 104 | −0.01 (−0.08, 0.06) | 0.10 | 103 | −0.01 (−0.07, 0.05) | 0.99 | |
| 5 | 100 | −0.01 (−0.07, 0.05) | 0.18 | 99 | −0.01 (−0.07, 0.05) | 0.99 | |
| 6 | 100 | −0.01 (−0.06, 0.05) | 0.34 | 99 | −0.01 (−0.06, 0.04) | 0.99 | |
| Non-haem iron (mg) | 1 | 109 | −0.04 (−0.14, 0.05) | 0.35 | 108 | −0.02 (−0.11, 0.07) | 0.71 |
| 2 | 109 | −0.24 (−0.40, −0.08) | 0.02 | 108 | −0.16 (−0.31, 0.01) | 0.18 | |
| 3 | 109 | −0.22 (−0.37, −0.06) | 0.02 | 108 | −0.14 (−0.29, 0.01) | 0.18 | |
| 4 | 104 | −0.21 (−0.38, −0.05) | 0.03 | 103 | −0.13 (−0.29, 0.03) | 0.21 | |
| 5 | 100 | −0.19 (−0.35, −0.03) | 0.03 | 99 | −0.11 (−0.26, 0.05) | 0.24 | |
| 6 | 100 | −0.19 (−0.33, −0.04) | 0.03 | 99 | −0.08 (−0.20, 0.04) | 0.24 | |
| (A) Fasting Plasma Glucose | (B) Haemoglobin A1c | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dietary Iron | Biliary | Non-Biliary | Biliary | Non-Biliary | |||||||||
| Model | n | β Coefficient (95% CI) | p | n | β Coefficient (95% CI) | p | n | β Coefficient (95% CI) | p | n | β Coefficient (95% CI) | p | |
| Total iron (mg) | 1 | 42 | −0.16 (0.28, −0.05) | 0.01 | 58 | 0.04 (−0.12, 0.20) | 0.68 | 42 | −0.10 (−0.20, −0.01) | 0.06 | 58 | 0.04 (−0.12, 0.20) | 0.65 |
| 2 | 42 | −0.35 (−0.54, −0.17) | <0.01 | 58 | −0.16 (−0.44, 0.12) | 0.68 | 42 | −0.17 (−0.33, 0.01) | 0.06 | 58 | −0.17 (−0.46, 0.12) | 0.65 | |
| 3 | 42 | −0.35 (−0.54, −0.16) | <0.01 | 58 | −0.11 (−0.39, 0.17) | 0.68 | 42 | −0.18 (−0.34, −0.01) | 0.06 | 58 | −0.11 (−0.39, 0.17) | 0.65 | |
| 4 | 41 | −0.35 (−0.53, −0.16) | <0.01 | 57 | −0.08 (−0.38, 0.22) | 0.68 | 41 | −0.17 (−0.34, 0.01) | 0.06 | 57 | −0.08 (−0.38, 0.22) | 0.65 | |
| 5 | 39 | −0.38 (−0.60, −0.15) | <0.01 | 55 | −0.10 (−0.36, 0.17) | 0.68 | 39 | −0.23 (−0.44, −0.03) | 0.06 | 55 | −0.11 (−0.38, 0.16) | 0.65 | |
| 6 | 39 | −0.39 (−0.63, −0.16) | <0.01 | 55 | −0.05 (−0.27, 0.18) | 0.68 | 39 | −0.17 (−0.36, 0.01) | 0.06 | 55 | −0.05 (−0.26, 0.17) | 0.65 | |
| Haem iron (mg) | 1 | 42 | −0.04 (−0.11, 0.04) | 0.60 | 58 | 0.01 (−0.08, 0.10) | 0.91 | 42 | −0.04 (−0.10, 0.02) | 0.28 | 58 | 0.03 (−0.07,0.12) | 0.72 |
| 2 | 42 | −0.03 (−0.12, 0.06) | 0.65 | 58 | −0.02 (−0.11, 0.08) | 0.91 | 42 | −0.03 (−0.10, 0.04) | 0.44 | 58 | <0.01 (−0.10, 0.10) | 0.99 | |
| 3 | 42 | −0.06 (−0.15, 0.03) | 0.60 | 58 | 0.02 (−0.08, 0.13) | 0.91 | 42 | −0.07 (−0.14, 0.01) | 0.13 | 58 | 0.05 (−0.05, 0.15) | 0.72 | |
| 4 | 41 | −0.05 (−0.15, 0.04) | 0.60 | 57 | 0.03 (−0.07, 0.14) | 0.91 | 41 | −0.07 (−0.14, 0.01) | 0.13 | 57 | 0.06 (−0.05, 0.16) | 0.72 | |
| 5 | 39 | −0.03 (−0.13, 0.07) | 0.65 | 55 | 0.02 (−0.07, 0.11) | 0.91 | 39 | −0.08 (−0.16, 0.01) | 0.13 | 55 | 0.04 (−0.05, 0.14) | 0.72 | |
| 6 | 39 | 0.01 (−0.10, 0.12) | 0.92 | 55 | 0.01 (−0.07, 0.08) | 0.91 | 39 | −0.03 (−0.11, 0.05) | 0.44 | 55 | 0.02 (−0.06, 0.09) | 0.72 | |
| Non-haem iron (mg) | 1 | 42 | −0.17 (−0.28, −0.05) | <0.01 | 58 | 0.06 (−0.09, 0.21) | 0.80 | 42 | −0.11 (−0.20, −0.01) | 0.10 | 58 | 0.05 (−0.10, 0.20) | 0.64 |
| 2 | 42 | −0.36 (−0.54, −0.18) | <0.01 | 58 | −0.09 (−0.36, 0.17) | 0.80 | 42 | −0.16 (−0.32, 0.01) | 0.10 | 58 | −0.12 (−0.39, 0.15) | 0.64 | |
| 3 | 42 | −0.34 (−0.53, −0.16) | <0.01 | 58 | −0.07 (−0.33, 0.19) | 0.80 | 42 | −0.16 (0.32, 0.01) | 0.10 | 58 | −0.09 (−0.35, 0.17) | 0.64 | |
| 4 | 41 | −0.34 (−0.53, −0.16) | <0.01 | 57 | −0.04 (−0.32, 0.23) | 0.80 | 41 | −0.14 (−0.31, 0.03) | 0.10 | 57 | −0.07 (−0.34, 0.21) | 0.64 | |
| 5 | 39 | −0.36 (−0.58, −0.15) | <0.01 | 55 | −0.07 (−0.32, 0.17) | 0.80 | 39 | −0.19 (−0.39, 0.02) | 0.10 | 55 | −0.11 (−0.36, 0.14) | 0.64 | |
| 6 | 39 | −0.39 (−0.61, −0.18) | <0.01 | 55 | −0.03 (−0.23, 0.18) | 0.80 | 39 | −0.16 (−0.33, 0.02) | 0.10 | 55 | −0.05 (−0.25, 0.15) | 0.64 | |
| (A) Fasting Plasma Glucose | (B) Haemoglobin A1c | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dietary Iron | FAP | RAP | FAP | RAP | |||||||||
| Model | n | β Coefficient (95% CI) | p-Value | n | β Coefficient (95% CI) | p-Value | n | β Coefficient (95% CI) | p-Value | n | β Coefficient (95% CI) | p-Value | |
| Total iron (mg) | 1 | 71 | −0.03 (−0.13, 0.07) | 0.58 | 31 | −0.09 (−0.33, 0.16) | 0.48 | 72 | 0.02 (−0.08, 0.11) | 0.71 | 30 | −0.10 (−0.35, 0.14) | 0.40 |
| 2 | 71 | −0.26 (−0.44, −0.07) | 0.02 | 31 | −0.30 (−0.69, 0.08) | 0.26 | 72 | −0.09 (−0.26, 0.09) | 0.71 | 30 | −0.30 (−0.68, 0.08) | 0.20 | |
| 3 | 71 | −0.27 (−0.45, −0.08) | 0.02 | 31 | −0.33 (−0.71, 0.05) | 0.26 | 72 | −0.09 (−0.27, 0.08) | 0.71 | 30 | −0.33 (−0.70, 0.05) | 0.20 | |
| 4 | 68 | −0.26 (−0.46, −0.07) | 0.02 | 31 | −0.29 (−0.69, 0.11) | 0.26 | 69 | −0.08 (−0.27, 0.10) | 0.71 | 30 | −0.29 (−0.68, 0.10) | 0.20 | |
| 5 | 65 | −0.25 (−0.46, −0.05) | 0.02 | 30 | −0.25 (−0.62, 0.12) | 0.26 | 66 | −0.06 (−0.25, 0.14) | 0.71 | 29 | −0.28 (−0.64, 0.09) | 0.20 | |
| 6 | 65 | −0.23 (−0.42, −0.05) | 0.02 | 30 | −0.13 (−0.38, 0.13) | 0.39 | 66 | −0.04 (−0.19, 0.12) | 0.71 | 29 | −0.16 (−0.45, 0.13) | 0.30 | |
| Haem iron (mg) | 1 | 71 | −0.01 (−0.07, 0.04) | 0.98 | 31 | 0.03 (−0.14, 0.20) | 0.84 | 72 | <0.01 (−0.05, 0.06) | 0.97 | 30 | 0.01 (−0.16, 0.17) | 0.96 |
| 2 | 71 | −0.03 (−0.09, 0.03) | 0.98 | 31 | 0.02 (−0.20, 0.24) | 0.84 | 72 | <−0.01 (−0.07,0.05) | 0.97 | 30 | −0.01 (−0.23, 0.20) | 0.96 | |
| 3 | 71 | −0.02 (−0.08, 0.04) | 0.98 | 31 | −0.06 (−0.29, 0.18) | 0.84 | 72 | −0.01 (−0.06, 0.06) | 0.97 | 30 | −0.10 (−0.33, 0.14) | 0.79 | |
| 4 | 68 | −0.01 (−0.07, 0.06) | 0.98 | 31 | −0.10 (−0.36, 0.15) | 0.84 | 69 | <0.01 (−0.06, 0.06) | 0.97 | 30 | −0.09 (−0.34, 0.15) | 0.79 | |
| 5 | 65 | −0.01 (−0.07, 0.06) | 0.98 | 30 | −0.12 (−0.35, 0.11) | 0.84 | 66 | 0.01 (−0.05, 0.07) | 0.97 | 29 | −0.12 (−0.36, 0.11) | 0.79 | |
| 6 | 65 | −0.01 (−0.06, 0.06) | 0.98 | 30 | −0.19 (−0.67, 0.29) | 0.84 | 66 | 0.01 (−0.04, 0.05) | 0.97 | 29 | −0.06 (−0.24, 0.13) | 0.79 | |
| Non-haem iron (mg) | 1 | 71 | −0.03 (−0.12, 0.07) | 0.59 | 31 | −0.07 (−0.32, 0.18) | 0.57 | 72 | 0.02 (−0.07,0.11) | 0.70 | 30 | −0.09 (−0.34, 0.16) | 0.47 |
| 2 | 71 | −0.23 (−0.40, −0.06) | 0.02 | 31 | −0.26 (−0.65, 0.13) | 0.41 | 72 | −0.08 (−0.24, 0.09) | 0.67 | 30 | −0.26 (−0.64, 0.12) | 0.30 | |
| 3 | 71 | −0.25 (−0.42, −0.07) | 0.02 | 31 | −0.28 (−0.66, 0.10) | 0.41 | 72 | −0.11 (−0.26, 0.07) | 0.67 | 30 | −0.28 (−0.66, 0.09) | 0.30 | |
| 4 | 68 | −0.25 (−0.43, −0.07) | 0.02 | 31 | −0.23 (−0.64, 0.17) | 0.41 | 69 | −0.08 (−0.26, 0.09) | 0.67 | 30 | −0.25 (−0.65, 0.14) | 0.30 | |
| 5 | 65 | −0.24 (−0.43, −0.05) | 0.02 | 30 | −0.20 (−0.58, 0.17) | 0.41 | 66 | −0.06 (−0.24, 0.12) | 0.67 | 29 | −0.24 (−0.62, 0.13) | 0.30 | |
| 6 | 65 | −0.23 (−0.40, −0.05) | 0.02 | 30 | −0.12 (−0.43, 0.19) | 0.50 | 66 | −0.04 (−0.19, 0.10) | 0.67 | 29 | −0.16 (−0.45, 0.12) | 0.30 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimita, W.; Li, X.; Ko, J.; Bharmal, S.H.; Cameron-Smith, D.; Petrov, M.S. Association between Habitual Dietary Iron Intake and Glucose Metabolism in Individuals after Acute Pancreatitis. Nutrients 2020, 12, 3579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113579
Kimita W, Li X, Ko J, Bharmal SH, Cameron-Smith D, Petrov MS. Association between Habitual Dietary Iron Intake and Glucose Metabolism in Individuals after Acute Pancreatitis. Nutrients. 2020; 12(11):3579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113579
Chicago/Turabian StyleKimita, Wandia, Xinye Li, Juyeon Ko, Sakina H. Bharmal, David Cameron-Smith, and Maxim S. Petrov. 2020. "Association between Habitual Dietary Iron Intake and Glucose Metabolism in Individuals after Acute Pancreatitis" Nutrients 12, no. 11: 3579. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113579