Obesity Risk Assessment Tool for Low-Income Spanish Speaking Immigrant Parents with Young Children: Validity with BMI and Biomarkers of Obesity

 ,
,
Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Participants
2.2. Study Design, Timeline & Data Collection
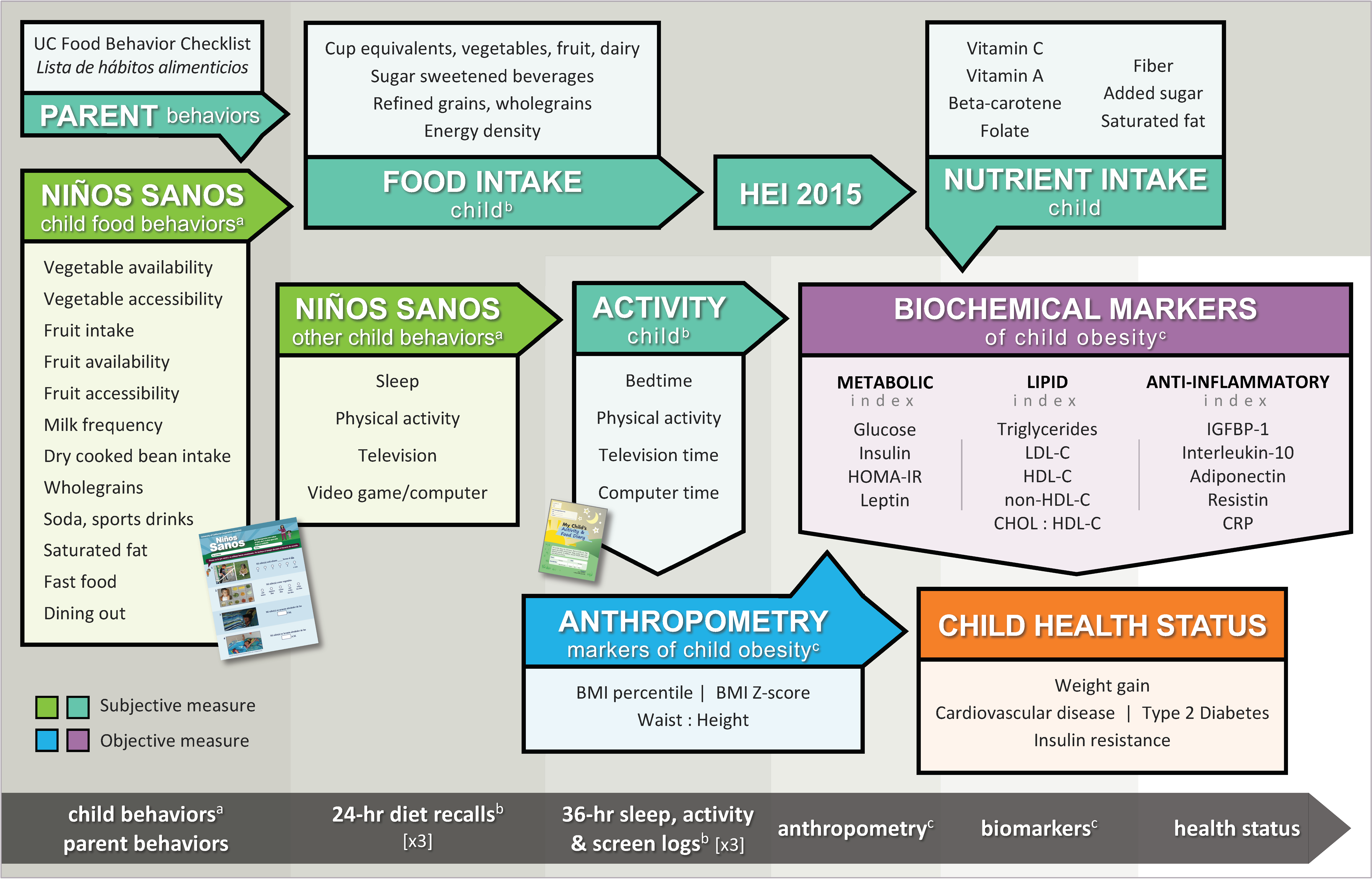
2.3. Biopsychosocial Framework
2.4. Child Anthropometry
2.5. Child Blood Biomarkers
2.6. Calculated Biomarkers
2.7. Blood Collection, Storage, Analysis
2.8. Biomarker Indices
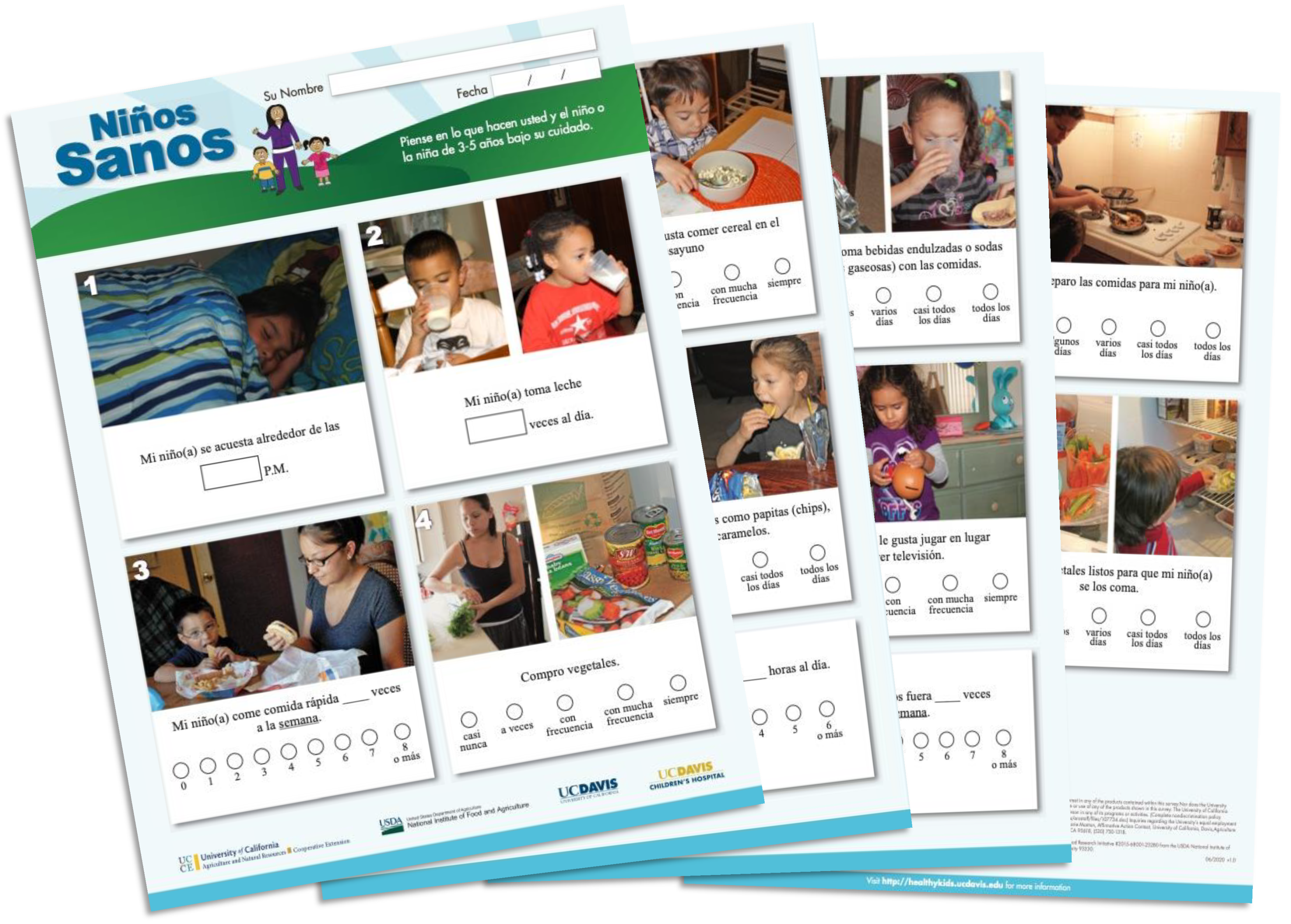
2.9. Niños Sanos Cultural Adaptation and Face Validation
2.10. Item Reduction for Niños Sanos
2.11. Sample and Attrition
2.12. Statistics
3. Results
3.1. Demographics
3.2. Item Reduction for Niños Sanos
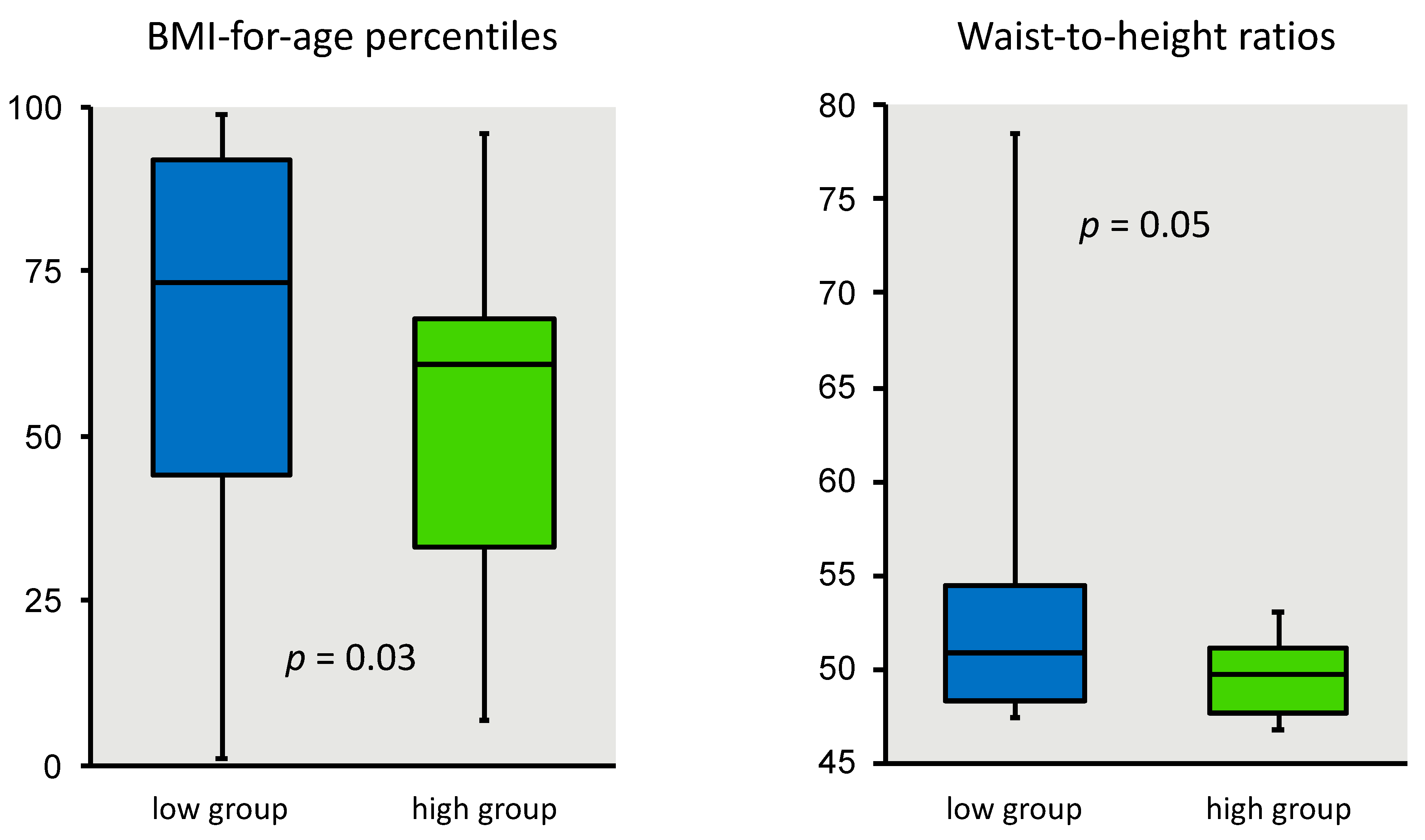
3.3. Niños Sanos and Child Anthropometry
3.4. Child Biomarkers and Anthropometry
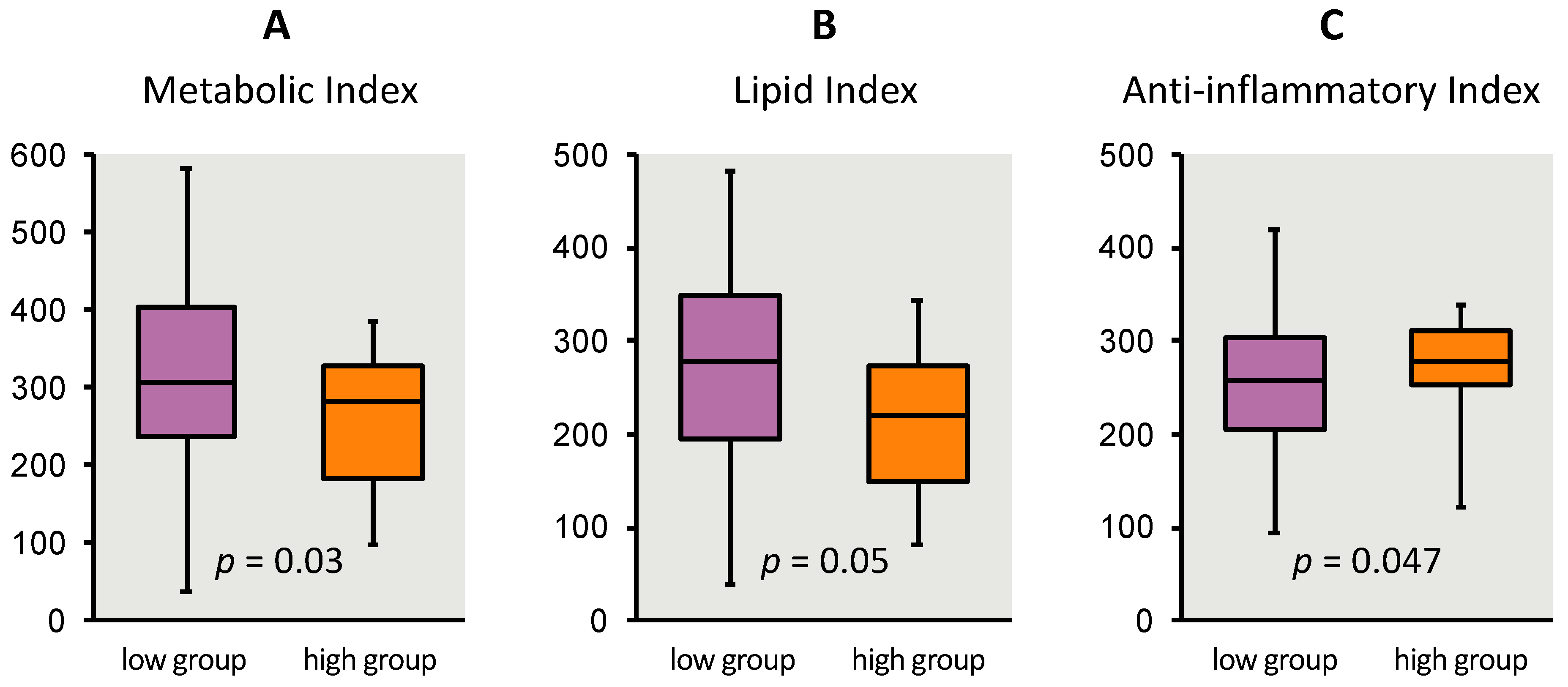
3.5. Niños Sanos and Child Biomarker Indices
4. Discussion
4.1. Anthropometric and Blood Biomarkers in Children
4.2. Advancing Obesity Risk Assessment
4.3. Comparison to Other Validation Studies for This Audience
4.4. Beyond Translation
4.5. Comparison to Other Biomarker Literature
4.6. Using Niños Sanos
4.7. Limitations and Strengths
5. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Fryar, C.D.; Hales, C.M.; Carroll, M.D.; Aoki, Y.; Freedman, D.S. Differences in Obesity Prevalence by Demographics and Urbanization in US Children and Adolescents, 2013–2016. JAMA 2018, 319, 2410–2418. [Google Scholar] [CrossRef] [PubMed]
- Ward, Z.J.; Long, M.W.; Resch, S.C.; Giles, C.M.; Cradock, A.L.; Gortmaker, S.L. Simulation of Growth Trajectories of Childhood Obesity into Adulthood. N. Engl. J. Med. 2017, 377, 2145–2153. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US). Committee on Prevention of Obesity in Children and Youth. In Preventing Childhood Obesity: Health in the Balance; Koplan, J.P., Liverman, C.T., Kraak, V.I., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2005; ISBN 978-0-309-09196-1. [Google Scholar]
- Krebs, N.F.; Jacobson, M.S. American Academy of Pediatrics Committee on Nutrition Prevention of pediatric overweight and obesity. Pediatrics 2003, 112, 424–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanovski, S.Z.; Yanovski, J.A. Viewpoint: Toward Precision Approaches for the Prevention and Treatment of Obesity. JAMA 2018, 319, 223–224. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.P.; Anstee, Q.M. PNPLA3 and obesity: A synergistic relationship in NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 506–507. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.N.; Lê, K.A.; Walker, R.W.; Vikman, S.; Spruijt-Metz, D.; Weigensberg, M.J.; Allayee, H.; Goran, M.I. Increased hepatic fat in overweight Hispanic youth influenced by interaction between genetic variation in PNPLA3 and high dietary carbohydrate and sugar consumption. Am. J. Clin. Nutr. 2010, 92, 1522–1527. [Google Scholar] [CrossRef] [Green Version]
- Leoni, M.C.; Valsecchi, C.; Mantelli, M.; Marastoni, L.; Tinelli, C.; Marchi, A.; Castellazzi, A. Impact of child obesity on adipose tissue physiology: Assessment of adipocytokines and inflammatory cytokines as biomarkers of obesity. Pediatr. Rep. 2010, 2. [Google Scholar] [CrossRef] [Green Version]
- Körner, A.; Kiess, W.; Landgraf, K. White Adipose Tissue Accumulation and Dysfunction in Children with Obesity. In Pediatric Obesity: Etiology, Pathogenesis and Treatment; Freemark, M.S., Ed.; Springer International Publishing: Cham, Germany, 2018; pp. 95–115. ISBN 978-3-319-68192-4. [Google Scholar]
- Aguilar-Morales, I.; Colin-Ramirez, E.; Rivera-Mancía, S.; Vallejo, M.; Vázquez-Antona, C. Performance of Waist-To-Height Ratio, Waist Circumference, and Body Mass Index in Discriminating Cardio-Metabolic Risk Factors in a Sample of School-Aged Mexican Children. Nutrients 2018, 10, 1850. [Google Scholar] [CrossRef] [Green Version]
- Frithioff-Bøjsøe, C.; Lund, M.A.V.; Lausten-Thomsen, U.; Hedley, P.L.; Pedersen, O.; Christiansen, M.; Baker, J.L.; Hansen, T.; Holm, J.-C. Leptin, adiponectin, and their ratio as markers of insulin resistance and cardiometabolic risk in childhood obesity. Pediatr. Diabetes 2020, 21, 194–202. [Google Scholar] [CrossRef]
- Jung, M.K.; Yoo, E.-G. Hypertriglyceridemia in Obese Children and Adolescents. J. Obes. Metab. Syndr. 2018, 27, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Gil, A.M.; Peschard-Franco, M.; Castillo, E.C.; Gutierrez-DelBosque, G.; Treviño, V.; Silva-Platas, C.; Perez-Villarreal, L.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Myokine–adipokine cross-talk: Potential mechanisms for the association between plasma irisin and adipokines and cardiometabolic risk factors in Mexican children with obesity and the metabolic syndrome. Diabetol. Metab. Syndr. 2019, 11, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlando, A.; Nava, E.; Giussani, M.; Genovesi, S. Adiponectin and Cardiovascular Risk. From Pathophysiology to Clinic: Focus on Children and Adolescents. Int. J. Mol. Sci. 2019, 20, 3228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brand, C.; Gaya, A.C.A.; Dias, A.F.; Agostinis-Sobrinho, C.; Farinha, J.B.; Boeno, F.P.; Mota, J.; de Oliveira, A.R.; Gaya, A.R. Relationship between insulin resistance and adipocytokines: The mediator role of adiposity in children. Ann. Hum. Biol. 2020, 47, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, D.; Kant, S.; Pandey, S.; Ehtesham, N.Z. Resistin in metabolism, inflammation, and disease. FEBS J. 2020, 287, 3141–3149. [Google Scholar] [CrossRef]
- Chang, J.-S.; Bai, C.-H.; Huang, Z.-C.; Owaga, E.; Chao, K.-C.; Chang, C.-C.; Chiou, H.-Y. Interleukin 10 and clustering of metabolic syndrome components in pediatrics. Eur. J. Clin. Investig. 2014, 44, 384–394. [Google Scholar] [CrossRef]
- Flores-Ramírez, A.G.; Ibarra-Reynoso, L.D.R.; López-Lemus, H.L.; Olvera-Juárez, M.; Luevano-Contreras, C.; Garay-Sevilla, M.E. Insulin-like growth factor binding protein-1, non-alcoholic fatty liver disease, and its relationship with fructose consumption in children with obesity. Rev. Investig. Clin. 2019, 71, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Mattos, R.T.; Medeiros, N.I.; Menezes, C.A.; Fares, R.C.G.; Franco, E.P.; Dutra, W.O.; Rios-Santos, F.; Correa-Oliveira, R.; Gomes, J.A.S. Chronic Low-Grade Inflammation in Childhood Obesity Is Associated with Decreased IL-10 Expression by Monocyte Subsets. PLoS ONE 2016, 11, e0168610. [Google Scholar] [CrossRef]
- Medeiros, N.I.; Mattos, R.T.; Menezes, C.A.; Fares, R.C.G.; Talvani, A.; Dutra, W.O.; Rios-Santos, F.; Correa-Oliveira, R.; Gomes, J.A.S. IL-10 and TGF-β unbalanced levels in neutrophils contribute to increase inflammatory cytokine expression in childhood obesity. Eur. J. Nutr. 2018, 57, 2421–2430. [Google Scholar] [CrossRef]
- Barkin, S.; Rao, Y.; Smith, P.; Po’e, E. A Novel Approach to the Study of Pediatric Obesity: A Biomarker Model. Pediatr. Ann. 2012, 41, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Rowicka, G.; Dyląg, H.; Chełchowska, M.; Weker, H.; Ambroszkiewicz, J. Serum Calprotectin and Chemerin Concentrations as Markers of Low-Grade Inflammation in Prepubertal Children with Obesity. Int. J. Environ. Res. Public Health 2020, 17, 7575. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Parati, G. Cardiovascular Risk in Children: Focus on Pathophysiological Aspects. Int. J. Mol. Sci. 2020, 21, 6612. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Anzman-Frasca, S.; Ventura, A.K.; Ehrenberg, S.; Myers, K.P. Promoting healthy food preferences from the start: A narrative review of food preference learning from the prenatal period through early childhood. Obes. Rev. 2018, 19, 576–604. [Google Scholar] [CrossRef] [PubMed]
- Rossen, L.M.; Talih, M. Social determinants of disparities in weight among US children and adolescents. Ann. Epidemiol. 2014, 24, 705–713.e2. [Google Scholar] [CrossRef] [Green Version]
- Grummon, A.H.; Taillie, L.S. Supplemental Nutrition Assistance Program participation and racial/ethnic disparities in food and beverage purchases. Public Health Nutr. 2018, 21, 3377–3385. [Google Scholar] [CrossRef] [Green Version]
- Rabbitt, M.P.; Smith, M.D.; Coleman-Jensen, A. Food Security Among Hispanic Adults in the United States, 2011–2014; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2016; p. 42.
- U.S. Department of Health and Human Services Head Start Website. Available online: https://www.acf.hhs.gov/ohs (accessed on 30 September 2020).
- U.S. Department of Agriculture. Food and Nutrition Service WIC Website. Available online: https://www.fns.usda.gov/wic (accessed on 30 September 2020).
- U.S. Department of Agriculture. Food and Nutrition Service SNAP-Ed Website. Available online: https://snaped.fns.usda.gov/program-administration/guidance-and-templates (accessed on 30 September 2020).
- U.S. Department of Agriculture. National Institute of Food and Agriculture EFNEP Website. Available online: https://nifa.usda.gov/program/expanded-food-and-nutrition-education-program-efnep (accessed on 30 September 2020).
- Townsend, M.S. Obesity in low-income communities: Prevalence, effects, a place to begin. J. Am. Diet. Assoc. 2006, 106, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Townsend, M.S.; Sylva, K.; Martin, A.; Metz, D.; Wooten-Swanson, P. Improving readability of an evaluation tool for low-income clients using visual information processing theories. J. Nutr. Educ. Behav. 2008, 40, 181–186. [Google Scholar] [CrossRef]
- Ontai, L.; Ritchie, L.; Williams, S.; Young, T.; Townsend, M.S. Guiding family-based obesity prevention efforts in low-income children in the US, Part 1: What determinants do we target? Int. J. Child. Adolesc. Health 2009, 2, 19–30. [Google Scholar]
- Townsend, M.S.; Ontai, L.; Young, T.; Ritchie, L.; Williams, S. Guiding family-based obesity prevention efforts in low-income children in the US, Part 2: What behaviors do we measure? Int. J. Child. Adolesc. Health 2009, 2, 31–48. [Google Scholar]
- Townsend, M.S.; Shilts, M.K.; Ontai, L.; Leavens, L.L.; Davidson, C.; Sitnick, S. Obesity Risk for Young Children: Development and Initial Validation of an Assessment Tool for Participants of Federal Nutrition Programs. Forum Family Consum. Issues 2014, 19, 1–20. [Google Scholar]
- Townsend, M.S.; Shilts, M.K.; Styne, D.; Lanoue, L.; Ontai, L. Healthy Kids, a 19-Item Pictorial Assessment of Child Obesity Prevention Behaviors: Eating, Physical Activity, Screen, Sleep and Parenting 2017. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/ (accessed on 30 September 2020).
- Townsend, M.S.; Shilts, M.K.; Lanoue, L.; Drake, C.; Styne, D.M.; Woodhouse, L.; Ontai, L. Obesity Risk Assessment Tool among 3–5 Year Olds: Validation with Biomarkers of Low-Grade Chronic Inflammation. Child. Obes. 2020, 16, S23–S32. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.S.; Shilts, M.K.; Styne, D.M.; Drake, C.; Lanoue, L.; Ontai, L. An Obesity Risk Assessment Tool for Young Children: Validity With BMI and Nutrient Values. J. Nutr. Educ. Behav. 2018, 50, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.S.; Kaiser, L.L.; Allen, L.H.; Joy, A.B.; Murphy, S.P. Selecting items for a food behavior checklist for a limited-resource audience. J. Nutr. Educ. Behav. 2003, 35, 69–77. [Google Scholar] [CrossRef]
- Townsend, M.S.; Shilts, M.K.; Davidson, C.; Leavens, L.L. My Child’s Activity & Food Diary (Log for Recording Physical Activity, Television and Computer Times, Bedtime, Wake Up Time, School, Other Activities). 2010. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/ (accessed on 30 September 2020).
- Townsend, M.S.; Shilts, M.K.; Sylva, K.; Davidson, C.; Leavens, L.L. Niños Sanos, a 45-Item Spanish Language Pictorial Assessment of Child Obesity Prevention Behaviors: Eating, Physical Activity, Screen, Sleep and Parenting. 2016. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/ (accessed on 30 September 2020).
- Banna, J.C.; Vera Becerra, L.E.; Kaiser, L.L.; Townsend, M.S. Using qualitative methods to improve questionnaires for Spanish speakers: Assessing face validity of a food behavior checklist. J. Am. Diet. Assoc. 2010, 110, 80–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banna, J.C.; Townsend, M.S. Assessing factorial and convergent validity and reliability of a food behaviour checklist for Spanish-speaking participants in US Department of Agriculture nutrition education programmes. Public Health Nutr. 2011, 14, 1165–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banna, J.C.; Townsend, M.S.; Sylva, K. Lista de Habitos Alimenticios (Food Behavior Checklist) for Spanish Speakers. 2010. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/ (accessed on 30 September 2020).
- Galea, S.; Riddle, M.; Kaplan, G.A. Causal thinking and complex system approaches in epidemiology. Int. J. Epidemiol. 2010, 39, 97–106. [Google Scholar] [CrossRef]
- Engel, G.L. The clinical application of the biopsychosocial model. Am. J. Psychiatry 1980, 137, 535–544. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. Food and Nutrition Service the Supplemental Nutrition Assistance Program Education (SNAP-Ed) Strategies and Interventions. Available online: https://snaped.fns.usda.gov/program-administration/snap-ed-toolkit-strategies-interventions (accessed on 30 September 2020).
- U.S. Department of Health and Human Services. National Cancer Institute Automated Self-Administered 24-Hour (ASA24®) Dietary Assessment Tool. Available online: https://epi.grants.cancer.gov/asa24/ (accessed on 30 September 2020).
- Centers for Disease Control and Prevention, N.C. for H.S. 2000 CDC Growth Charts for the United States: Methods and Development. Available online: https://www.cdc.gov/growthcharts/cdc_charts.htm (accessed on 30 September 2020).
- Centers for Disease Control and Prevention A SAS Program for the 2000 CDC Growth Charts (ages 0 to <20 y). Available online: http://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm (accessed on 14 July 2014).
- Klünder-Klünder, M.; Flores-Huerta, S.; García-Macedo, R.; Peralta-Romero, J.; Cruz, M. Adiponectin in eutrophic and obese children as a biomarker to predict metabolic syndrome and each of its components. BMC Public Health 2013, 13, 88. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Cheng, H.; Zhao, X.; Hou, D.; Yan, Y.; Cianflone, K.; Li, M.; Mi, J. Leptin and Leptin-to-Adiponectin Ratio Predict Adiposity Gain in Nonobese Children over a Six-Year Period. Child. Obes. 2017, 13, 213–221. [Google Scholar] [CrossRef]
- Behiry, E.G.; El Nady, N.M.; AbdEl Haie, O.M.; Mattar, M.K.; Magdy, A. Evaluation of TG-HDL Ratio Instead of HOMA Ratio as Insulin Resistance Marker in Overweight and Children with Obesity. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Motaghedi, R.; Gujral, S.; Sinha, S.; Sison, C.; Ten, S.; Maclaren, N.K. Insulin-like growth factor binding protein-1 to screen for insulin resistance in children. Diabetes Technol. Ther. 2007, 9, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodside, J.V.; Draper, J.; Lloyd, A.; McKinley, M.C. Use of biomarkers to assess fruit and vegetable intake. Proc. Nutr. Soc. 2017, 76, 308–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, M.S.; Shilts, M.K.; Sylva, K.; Davidson, C.; Leavens, L.L. Healthy Kids a 45-Item Pictorial Assessment of Child Obesity Prevention Behaviors: Eating, Physical Activity, Screen, Sleep and Parenting. 2011. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/. (accessed on 30 September 2020).
- Townsend, M.S.; Shilts, M.K.; Diaz Rios, L.K.; Lanoue, L. Ninos Sanos, a 18-Item Pictorial Assessment of Obesity Prevention Behaviors in the Family Environment for Spanish Speakers. 2020. Available online: https://townsendlab.ucdavis.edu/evaluation-research-tools/validation-research/ (accessed on 30 September 2020).
- Confiac, N.; Turk, M.T.; Zoucha, R.; McFarland, M. Mexican American Parental Knowledge and Perceptions of Childhood Obesity: An Integrative Review. Hisp. Health Care Int. 2020, 18, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Katzmarzyk, P.T.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Relation of body mass index and skinfold thicknesses to cardiovascular disease risk factors in children: The Bogalusa Heart Study. Am. J. Clin. Nutr. 2009, 90, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Butte, N.F.; Comuzzie, A.G.; Cai, G.; Cole, S.A.; Mehta, N.R.; Bacino, C.A. Genetic and environmental factors influencing fasting serum adiponectin in Hispanic children. J. Clin. Endocrinol. Metab. 2005, 90, 4170–4176. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Ríos, L.K.; Chapman-Novakofski, K.; Malacara, J.M.; Bollero, G.; Aradillas-García, C.; Garay-Sevilla, E. Metabolic and nutritional profile differences among Mexican, Mexican-American and Non-Hispanic White children. Rev. Investg. Clin. 2014, 66, 31–44. [Google Scholar]
- Volberg, V.; Harley, K.G.; Aguilar, R.S.; Rosas, L.G.; Huen, K.; Yousefi, P.; Davé, V.; Phan, N.; Lustig, R.H.; Eskenazi, B.; et al. Associations between perinatal factors and adiponectin and leptin in 9-year-old Mexican-American children. Pediatr. Obes. 2013, 8, 454–463. [Google Scholar] [CrossRef] [Green Version]
- Ruan, W.; Lai, M. Insulin-like growth factor binding protein: A possible marker for the metabolic syndrome? Acta Diabetol. 2010, 47, 5–14. [Google Scholar] [CrossRef]
- Ibarra-Reynoso, L.d.R.; Pisarchyk, L.; Pérez-Luque, E.L.; Garay-Sevilla, M.E.; Malacara, J.M. Whole-Body and Hepatic Insulin Resistance in Obese Children. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beets, M.W.; Brazendale, K.; Weaver, R.G.; Armstrong, B. Rethinking Behavioral Approaches to Compliment Biological Advances to Understand the Etiology, Prevention, and Treatment of Childhood Obesity. Child. Obes. 2019, 15, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, S.I.; Baranowski, T.; Subar, A.F.; Tooze, J.A.; Frongillo, E.A. Best Practices for Conducting and Interpreting Studies to Validate Self-Report Dietary Assessment Methods. J. Acad. Nutr. Diet. 2019, 119, 1801–1816. [Google Scholar] [CrossRef] [PubMed]
- Ontai, L.L.; Sutter, C.; Sitnick, S.; Shilts, M.K.; Townsend, M.S. Parent Food-Related Behaviors and Family-Based Dietary and Activity Environments: Associations with BMI z-Scores in Low-Income Preschoolers. Child. Obes. 2020, 16, S55–S63. [Google Scholar] [CrossRef] [PubMed]
- Ontai, L.L.; Sutter, C.; Sitnick, S.; Shilts, M.K.; Townsend, M.S. My Child at mealtime parent self-assessment of food related behaviors: Validation with mealtime behaviors. Appetite 2019, 136, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Bekelman, T.A.; Bellows, L.L.; McCloskey, M.L.; Martin, C.K.; Johnson, S.L. Assessing dinner meals offered at home among preschoolers from low-income families with the Remote Food Photography Method. Pediatr. Obes. 2019, 14, e12558. [Google Scholar] [CrossRef]
- Ihmels, M.A.; Welk, G.J.; Eisenmann, J.C.; Nusser, S.M.; Myers, E.F. Prediction of BMI change in young children with the family nutrition and physical activity (FNPA) screening tool. Ann. Behav. Med. 2009, 38, 60–68. [Google Scholar] [CrossRef]
- Yee, K.E.; Pfeiffer, K.A.; Turek, K.; Bakhoya, M.; Carlson, J.J.; Sharman, M.; Lamb, E.; Eisenmann, J.C. Association of the Family Nutrition and Physical Activity Screening Tool with Weight Status, Percent Body Fat, and Acanthosis Nigricans in Children from a Low Socioeconomic, Urban Community. Ethn. Dis. 2015, 25, 399–404. [Google Scholar] [CrossRef]
- Dickin, K.L.; Larios, F.; Parra, P.A. Cognitive Interviewing to Enhance Comprehension and Accuracy of Responses to a Spanish-Language Nutrition Program Evaluation Tool. J. Nutr. Educ. Behav. 2015, 47, 465–471. [Google Scholar] [CrossRef]
- Davis, R.E.; Johnson, T.P.; Lee, S.; Werner, C. Why Do Latino Survey Respondents Acquiesce? Respondent and Interviewer Characteristics as Determinants of Cultural Patterns of Acquiescence Among Latino Survey Respondents. Sage J. 2018, 53, 87–115. [Google Scholar] [CrossRef]
- Hendrickson, S.G. Beyond translation … cultural fit. West. J. Nurs. Res. 2003, 25, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Shilts, M.K.; Sitnick, S.L.; Ontai, L.; Townsend, M.S. Guided Goal Setting: A Feasible Obesity Prevention Behavior Change Strategy for Low-Income Parents with Young Children. J. Hum. Sci. Ext. 2018, 6, 161–179. [Google Scholar]
- Shilts, M.K.; Townsend, M.S.; Leavens, L.; Reed, M. Healthy Kids. Available online: http://healthykids.ucdavis.edu/ (accessed on 30 September 2020).
- Shilts, M.K.; Townsend, M.S.; Ontai, L.; Reed, M. Niños Sanos iPad Kiosk for a Medical Clinic Setting. Available online: http://healthykids.ucdavis.edu/ (accessed on 30 September 2020).
- Shilts, M.K.; Leavens, L.L.; Trujano, J.; Lanoue, L.; Ontai, L.; Townsend, M.S. Setup a Heathy Kids iPad Kiosk Guidebook 2018. Available online: http://healthykids.ucdavis.edu/ (accessed on 30 September 2020).
- Levie, W.H.; Lentz, R. Effects of text illustrations: A review of research. ECTJ 1982, 30, 195–232. [Google Scholar] [CrossRef]
- Van de Vijver, F.J.R.; Leung, K. Methods and Data Analysis for Cross-Cultural Research; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1997; pp. xiii, 186. ISBN 978-0-7619-0106-8. [Google Scholar]
- Townsend, M.S.; Ganthavorn, C.; Neelon, M.; Donohue, S.; Johns, M.C. Improving the Quality of Data From EFNEP Participants With Low Literacy Skills: A Participant-driven Model. J. Nutr. Educ. Behav. 2014, 46, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.D.; Campbell, D.T. Quasi-Experimentation: Design & Analysis Issues for Field Settings; Houghton Mifflin: Boston, MA, USA, 1979; ISBN 978-0-395-30790-8. [Google Scholar]
- Ontai, L.L.; Sitnick, S.L.; Shilts, M.K.; Townsend, M.S. My child at mealtime: A visually enhanced self-assessment of feeding styles for low-income parents of preschoolers. Appetite 2016, 99, 76–81. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sources | Targets | Biological Actions | Relationship to BMI in Children | |
|---|---|---|---|---|
| Metabolic index | ||||
| Glucose | Diet, Liver, Muscle | Cells | Energy | Positive [22] |
| Insulin | Pancreas | Muscle, AT | Glycemia homeostasis, lipolysis inhibition | Positive [22,54] |
| HOMA-IR | n/a | n/a | Insulin sensitivity index | Positive [22,54] |
| Leptin | AT | Brain (hypothalamus), Muscle, AT, liver | Regulation of food intake, satiety and energy expenditure | Positive [22] |
| Leptin: Adiponectin | n/a | n/a | Adipose tissue dysfunction index | Positive [55] |
| TG: HDL-C | n/a | n/a | Insulin resistance index | Positive [56] |
| Lipid index | ||||
| Triglycerides | (Diet), Liver, AT | AT | Energy | Positive [22,54] |
| LDL-C | Plasma | Cells, Liver | Cholesterol transport (influx) | Positive [22] |
| HDL-C | Plasma | Liver | Cholesterol transport (effux) | Negative [22,54] |
| Non-HDL-C | Gut, Liver | Cells, Liver | Cholesterol transport (influx) | Positive [22] |
| CHOL:HDL-C | n/a | n/a | Pro-atherogenic index | Positive [22] |
| Anti-inflammatory index | ||||
| IGFBP-1 | Liver | Muscle, AT | Insulin sensitivity, anti-inflammatory | Negative [57] |
| Interleukin-10 | AT, Spleen | Liver | Anti-inflammatory | Negative [18] |
| Adiponectin | AT | Pancreas, Muscle, Liver, AT | Anti-inflammatory, insulin sensitivity | Negative [22,54] |
| CRP | Liver | Muscle, AT | Pro-inflammatory, insulin resistance | Positive [22] |
| Resistin | AT | AT | Insulin resistance, food intake | Positive [14] |
| Demographic Characteristics | |||||
| Parent/Guardian a,b | Child a,b | Family/Household a,b | |||
| Gender (Female) | 206 (100) | Gender (Female) | 113 (54.3) | Household Income (monthly) | |
| Age (years) | 33.6 ± 6.0 | Age (months) | 51.8 ± 8.0 | <$2000 | 118 (56.7) |
| Marital status | $3000–3500 | 13 (6.3) | |||
| Married | 136 (65.4) | $3500–4000 | 5 (2.4) | ||
| BMI | BMI-for-age-percentile | >$4000 | 5 (2.4) | ||
| Normal <25 | 40 (19.5) | Underweight <5th %ile | 8 (4.0) | ||
| Overweight (25–30) | 75 (36.6) | Normal weight <85th %ile | 130 (65.0) | Assistance programs c | |
| Obesity (30–40) | 77 (37.6) | Overweight > 85th %ile | 24 (12.0) | Head Start | 166 (79.8) |
| Severe obesity >40 | 13 (6.3) | Obesity >95th %ile | 38 (19.0) | WIC | 172 (82.7) |
| Education | SNAP | 84 (40.4) | |||
| College degree | 13 (6.4) | TANF | 18 (8.6) | ||
| Some college | 30 (14.7) | NSLP | 62 (29.8) | ||
| High school diploma | 59 (28.9) | Head Start | 166 (79.8) | ||
| Employment | WIC | 172 (82.7) | |||
| Unemployed | 148 (71.1) | ||||
| Seasonal | 35 (16.8) | ||||
| Full time | 25 (12.0) | ||||
| Acculturation Components a,b | |||||
| Parent/guardian a,b | Child a,b | Family/household a,b | |||
| Living in U.S. (years) | Language spoken at home | ||||
| <3 | 7(3.4) | English | 13 (6.3) | ||
| 3–9 | 33 (16.2) | Spanish | 179 (86.1) | ||
| 10–20 | 116 (56.9) | English or | 16 (7.7) | ||
| >20 | 48 (23.5) | Spanish | |||
| Country of Birth | Country of Birth | ||||
| U.S. | 0 (0) | U.S. | 198 (95.2) | ||
| Mexico | 168 (80.8) | Mexico | 7 (3.4) | ||
| Other | 40 (19.2) | Other | 3 (1.4) | ||
| Ethnicity | Ethnicity | ||||
| Hispanic/Latino | 100 | Hispanic/Latino | 98.6 | ||
| Behavioral Domain & Construct | Item Text | Item Visual | Response a |
|---|---|---|---|
| Vegetables | |||
| Vegetable availability | Compro vegetales. I buy vegetables. | Left: woman getting ready to buy broccoli with her daughter. Right: bag of frozen mixed vegetables, box of frozen green beans, can of diced tomatoes, can of corn and can of mixed vegetables. | 4.2 ± 1.0 |
| Vegetable accessibility | Tengo vegetales listos para que mi niño (a) se los coma. I keep vegetables ready for my child to eat. | Left: refrigerator shelf with bowl of washed cherry tomatoes, carrot and celery sticks in a glass, carrot sticks/celery sticks/cherry tomato in snack bag. Right: child reaching for vegetable snack on refrigerator shelf. | 3.2 ± 1.3 |
| Fruit | |||
| Fruit intake | Yo como frutas __ veces al dia. I eat fruit ____times a day. | Left: mother biting into an apple. Right: another mother eating a banana. | 3.3 ± 0.9 |
| Fruit availability | Compro frutas. I buy fruit. | Left: mother biting into an apple. Right: another mother eating a banana. | 4.4 ± 0.8 |
| Beans | |||
| Dry cooked bean intake | Mi niño (a) come frijoles ___ veces por semana. My child eats beans ____times a week. | Left: dry beans as purchased, cooked dry beans in cans. Right: mother and daughter who is serving prepared beans. | 2.4 ± 1.0 |
| Dairy | |||
| Milk frequency | Mi niño(a) toma leche __ veces al dia. My child drinks milk ___ times a day. | Left: parent pouring milk on cereal. Center: Boy drinking milk in glass with snack/meal. Right: boy drinking chocolate milk via a straw. | 3.3 ± 0.8 |
| Milk frequency | Yo tomo leche __ veces al dia. I drink milk ___ times a day. | Left: mother drinking milk from a glass. Right: another mother drinking milk from a glass. | 2.3 ± 0.8 |
| Whole Grains | |||
| Milk with cereal | A mi nino(a) le gusta comer cereal en el desayuno. My child enjoys cereal for breakfast. | Child with cereal and empty glass of milk. | 3.0 ± 1.2 |
| Sugar Sweetened Beverages | |||
| Soda frequency | Mi niño(a) toma sodas __ veces al día. My child drinks soda ____times a day. | Left: girl drinking Mexican soda from a bottle. Right: selection of carbonated beverages in cans, bottles and paper cup from Mexico and U.S. | 4.7 ± 0.4 |
| Sports drinks, punch frequency | Mi niño(a) toma bebidas deportivas o endulzadas __ veces al día. My child drinks sport drinks or sugared drinks ___ times a day. | Left: boy drinking Kool-Aid© from disposible pouch. Right: SunnyD©, Hawaiian Punch©, Propel Fitness Water©, Gatorade©, Kool-Aid©. | 4.5 ± 0.6 |
| Fat/Saturated Fat | |||
| Energy density | Mi niño(a) come comida rápida __ veces a la semana. My child eats fast food _____times a week. | Child eating hamburger from fast food outlet. Also shown are French fries and soda in paper cup with straw from a Happy Meal box. | 4.4 ± 0.4 |
| Fat, energy density, saturated fat | Le quito la grasa a la carne antes de comerla. I trim fat before eating. | Parent’s hand with knife trimming fat from raw meat on cutting board. Parent’s hand with fork and knife trimming fat from cooked meat as served on dinner plate. | 4.3 ± 1.1 |
| Snack Foods | |||
| Energy dense foods for snack | Mi nino(a) come snacks como papitas (chips), galletas y dulces. My child eats snack foods like cookies, chips and candy. | Left: boy eating cookie. Center: girl eating Mexican pastry Right: girl eating chips. | 4.0 ± 0.7 |
| Eating Out | |||
| Energy density | Nosotros comemos fuera __ veces a la semana. We eat out ____times a week. | Two parents with young child sitting at table in restaurant eating burritos and soda. | 4.1 ± 0.8 |
| Cooking at Home | |||
| Energy density | Preparo las comidas para mi niño(a). I cook my child’s dinner from scratch. | Parent at stove cooking meat in skillet with young child watching. | 4.6 ± 0.7 |
| Screen Time | |||
| Television | Mi niño(a) mira la televisión __ horas al dia. My child watches TV ___ hours a day. | Girl watching TV in living room/front room. | 3.7 ± 0.6 |
| Physical Activity | |||
| Play, sedentary time | A mi niño(a) le gusta jugar en lugar de ver televisión. My child likes playing instead of watching TV. | Girl playing with toy in her bedroom. | 3.4 ± 1.1 |
| Sleep | |||
| Bedtime | Mi niño(a) se acuesta alrededor de las __ PM. My child goes to bed around ___ p.m. | Young girl asleep in her bed in child’s dark bedroom. | 3.0 ± 0.8 |
| Niños Sanos | p-Value a | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Scoring Children | High Scoring Children | ||||||||||
| n | Median | IQR | Q1 | Q3 | n | Median | IQR | Q1 | Q3 | ||
| Anthropometric | |||||||||||
| BMI percentiles-for-age | 176 | 73.50 | 48.00 | 44.00 | 92.00 | 20 | 61.00 | 35.00 | 33.00 | 68.00 | 0.024 |
| BMI Z-scores | 176 | 0.65 | 1.51 | −0.12 | 1.39 | 20 | 0.29 | 1.01 | −0.45 | 0.56 | 0.028 |
| Waist-to-height ratios | 176 | 50.85 | 6.08 | 48.35 | 54.43 | 20 | 49.65 | 3.45 | 47.71 | 51.16 | 0.053 |
| Metabolic | |||||||||||
| Metabolic index | 141 | 307.07 | 166.86 | 237.11 | 403.96 | 18 | 281.08 | 145.27 | 180.90 | 326.17 | 0.028 |
| Lipid index | 149 | 263.96 | 152.66 | 195.27 | 347.93 | 18 | 219.23 | 121.89 | 150.30 | 272.19 | 0.050 |
| Anti-inflammatory index | 140 | 258.39 | 96.25 | 206.05 | 302.31 | 18 | 277.20 | 55.83 | 253.99 | 309.82 | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Townsend, M.S.; Shilts, M.K.; Lanoue, L.; Drake, C.; Díaz Rios, L.K.; Styne, D.M.; Keim, N.L.; Ontai, L. Obesity Risk Assessment Tool for Low-Income Spanish Speaking Immigrant Parents with Young Children: Validity with BMI and Biomarkers of Obesity. Nutrients 2020, 12, 3582. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113582
Townsend MS, Shilts MK, Lanoue L, Drake C, Díaz Rios LK, Styne DM, Keim NL, Ontai L. Obesity Risk Assessment Tool for Low-Income Spanish Speaking Immigrant Parents with Young Children: Validity with BMI and Biomarkers of Obesity. Nutrients. 2020; 12(11):3582. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113582
Chicago/Turabian StyleTownsend, Marilyn S., Mical K. Shilts, Louise Lanoue, Christiana Drake, L. Karina Díaz Rios, Dennis M. Styne, Nancy L. Keim, and Lenna Ontai. 2020. "Obesity Risk Assessment Tool for Low-Income Spanish Speaking Immigrant Parents with Young Children: Validity with BMI and Biomarkers of Obesity" Nutrients 12, no. 11: 3582. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113582