Dietary Acrylamide Intake and the Risk of Pancreatic Cancer: The Japan Public Health Center-Based Prospective Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
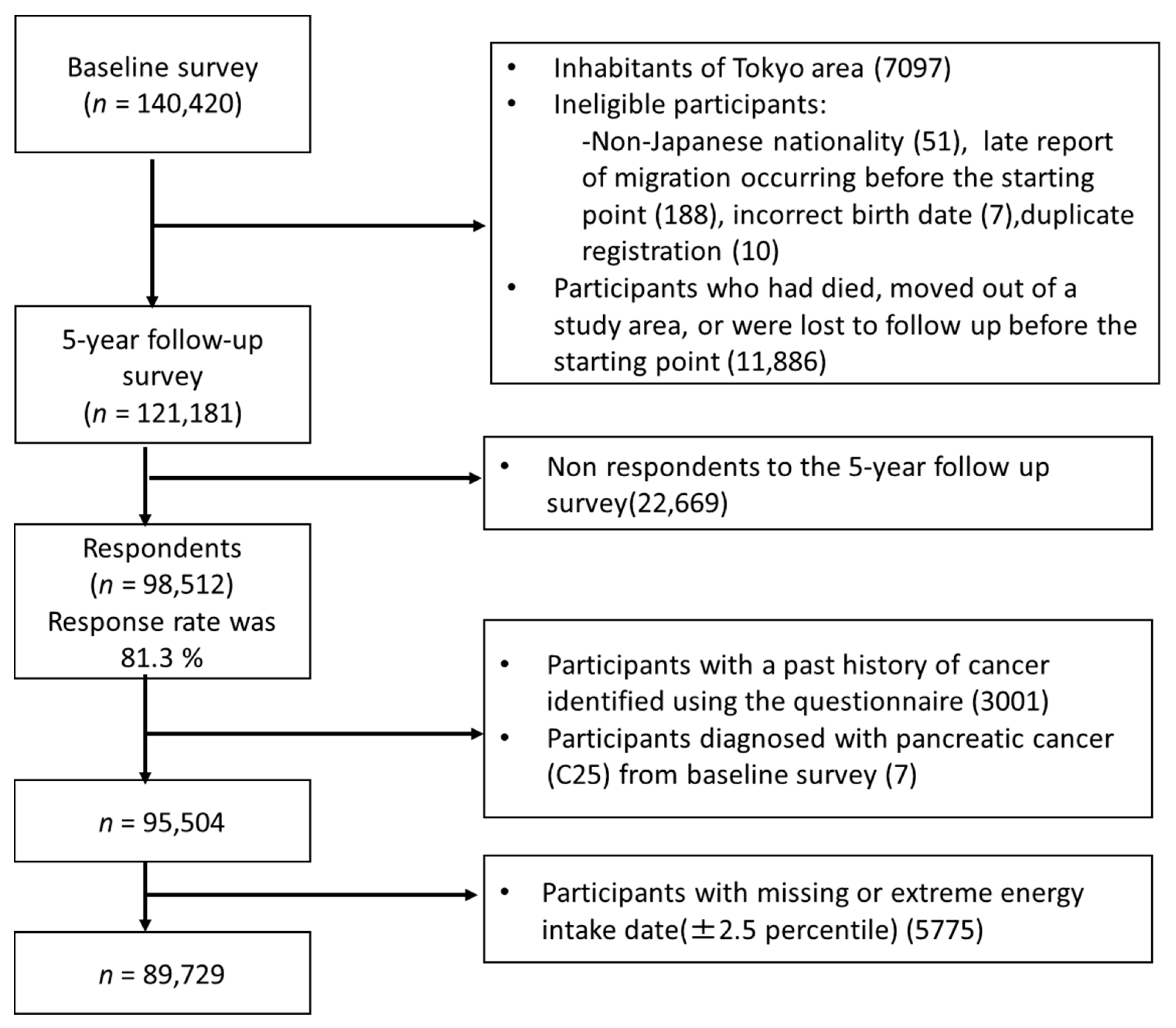
2.1. Study Participants
2.2. Food Frequency Questionnaire
2.3. Assessment of Energy and Acrylamide Intake from the FFQ
2.4. Follow-Up and Identification of Pancreatic Cancer
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- IARC. Working group on the evaluation of carcinogenic risks to humans: Some industrial chemicals. Lyon, 15–22 February 1994. In Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans; World Health Organization: Geneva, Switzerland, 1994; Volume 60, 560p. [Google Scholar]
- Tareke, E.; Rydberg, P.; Karlsson, P.; Eriksson, S.; Törnqvist, M. Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J. Agric. Food Chem. 2002, 50, 4998–5006. [Google Scholar] [CrossRef]
- Smith, C.J.; Perfetti, T.A.; Rumple, M.A.; Rodgman, A.; Doolittle, D.J. “IARC group 2A Carcinogens” reported in cigarette mainstream smoke. Food Chem. Toxicol. 2000, 38, 371–383. [Google Scholar] [CrossRef]
- Besaratinia, A.; Pfeifer, G.P. A review of mechanisms of acrylamide carcinogenicity. Carcinogenesis 2007, 28, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipp, A.; Lawrence, G.; Gentry, R.; McDonald, T.; Bartow, H.; Bounds, J.; Macdonald, N.; Clewell, H.; Allen, B.; Van Landingham, C. Acrylamide: Review of toxicity data and dose-response analyses for cancer and noncancer effects. Crit. Rev. Toxicol. 2006, 36, 481–608. [Google Scholar] [CrossRef] [PubMed]
- Hirvonen, T.; Kontto, J.; Jestoi, M.; Valsta, L.; Peltonen, K.; Pietinen, P.; Virtanen, S.M.; Sinkko, H.; Kronberg-Kippilä, C.; Albanes, D.; et al. Dietary acrylamide intake and the risk of cancer among Finnish male smokers. Cancer Causes Control 2010, 21, 2223–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obón-Santacana, M.; Slimani, N.; Lujan-Barroso, L.; Travier, N.; Hallmans, G.; Freisling, H.; Ferrari, P.; Boutron-Ruault, M.C.; Racine, A.; Clavel, F.; et al. Dietary intake of acrylamide and pancreatic cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Ann. Oncol. 2013, 24, 2645–2651. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake is not associated with gastrointestinal cancer risk. J. Nutr. 2008, 138, 2229–2236. [Google Scholar] [CrossRef] [Green Version]
- Pelucchi, C.; Galeone, C.; Talamini, R.; Negri, E.; Polesel, J.; Serraino, D.; La Vecchia, C. Dietary acrylamide and pancreatic cancer risk in an Italian case-control study. Ann. Oncol. 2011, 22, 1910–1915. [Google Scholar] [CrossRef]
- Pelucchi, C.; Rosato, V.; Bracci, P.M.; Li, D.; Neale, R.E.; Lucenteforte, E.; Serraino, D.; Anderson, K.E.; Fontham, E.; Holly, E.A.; et al. Dietary acrylamide and the risk of pancreatic cancer in the International Pancreatic Cancer Case-Control Consortium (PanC4). Ann. Oncol. 2017, 28, 408–414. [Google Scholar] [CrossRef]
- Pelucchi, C.; Bosetti, C.; Galeone, C.; La Vecchia, C. Dietary acrylamide and cancer risk: An updated meta-analysis. Int. J. Cancer 2015, 136, 2912–2922. [Google Scholar] [CrossRef]
- Kotemori, A.; Ishihara, J.; Nakadate, M.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Validity of a self-administered food frequency questionnaire for the estimation of acrylamide intake in the Japanese population: The JPHC FFQ Validation Study. J. Epidemiol. 2018, 28, 482–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konings, E.J.; Hogervorst, J.G.; van Rooij, L.; Schouten, L.J.; Sizoo, E.A.; van Egmond, H.P.; Goldbohm, R.A.; van den Brandt, P.A. Validation of a database on acrylamide for use in epidemiological studies. Eur. J. Clin. Nutr. 2010, 64, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freisling, H.; Moskal, A.; Ferrari, P.; Nicolas, G.; Knaze, V.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; Nailler, L.; Teucher, B.; Grote, V.A.; et al. Dietary acrylamide intake of adults in the European Prospective Investigation into Cancer and Nutrition differs greatly according to geographical region. Eur. J. Nutr. 2013, 52, 1369–1380. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Tsugane, S.; Sobue, T.; Konishi, M.; Baba, S. Study design and organization of the JPHC study. Japan Public Health Center-Based Prospective Study on Cancer and Cardiovascular Diseases. J. Epidemiol. 2001, 11, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S.; Sawada, N. The JPHC study: Design and some findings on the typical Japanese diet. Jpn. J. Clin. Oncol. 2014, 44, 777–782. [Google Scholar] [CrossRef]
- Resources Council, Science and Technology Agency, Government of Japan. Standard Tables of Food Composition in Japan, 5th ed.; Printing Bureau, Ministry of Finance: Tokyo, Japan, 2002.
- Tsugane, S.; Sasaki, S.; Kobayashi, M.; Tsubono, Y.; Akabane, M. Validity and reproducibility of the self-administered food frequency questionnaire in the JPHC Study Cohort I: Study design, conduct, and participant profiles. J. Epidemiol. 2003, 13, S2–S12. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, J.; Sobue, T.; Yamamoto, S.; Yoshimi, I.; Sasaki, S.; Kobayashi, M.; Takahashi, T.; Iitoi, Y.; Akabane, M.; Tsugane, S. Validity and reproducibility of a self-administered food frequency questionnaire in the JPHC Study Cohort II: Study design, participant profile and results in comparison with Cohort I. J. Epidemiol. 2003, 13, S134–S147. [Google Scholar] [CrossRef]
- Ishihara, J.; Inoue, M.; Kobayashi, M.; Tanaka, S.; Yamamoto, S.; Iso, H.; Tsugane, S. Impact of the revision of a nutrient database on the validity of a self-administered food frequency questionnaire (FFQ). J. Epidemiol. 2006, 16, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Food Safety Commission of Japan Study on Estimate of Acrylamide Intake from Food: Interim Report. 2016. Available online: https://www.fsc.go.jp/fsciis/technicalResearch/show/cho99920151507 (accessed on 28 September 2020).
- National Institute for Environmental Studies, Japan. Study on Statistical Estimate of Acrylamide Intake from Foods. Available online: http://www.fsc.go.jp/fsciis/technicalResearch/show/cho99920141408 (accessed on 28 September 2020).
- Ministry of Agriculture, Forestry, and Fisheries. Risk Profile Sheet Relating to Food Safety; for Acrylamide. Available online: https://www.maff.go.jp/j/syouan/seisaku/risk_analysis/priority/pdf/150807_rp_aa.pdf (accessed on 28 September 2020).
- National Institute of Health Sciences. Acrylamide Analysis in Food. Available online: https://www.mhlw.go.jp/topics/2002/11/tp1101-1a.html (accessed on 28 September 2020).
- Mizukami, Y.; Kohata, K.; Yamaguchi, Y.; Hayashi, N.; Sawai, Y.; Chuda, Y.; Ono, H.; Yada, H.; Yoshida, M. Analysis of acrylamide in green tea by gas chromatography-mass spectrometry. J. Agric. Food Chem. 2006, 54, 7370–7377. [Google Scholar] [CrossRef]
- Takatsuki, S.; Nemoto, S.; Sasaki, K.; Maitani, T. Production of acrylamide in agricultural products by cooking. Shokuhin Eiseigaku Zasshi 2004, 45, 44–48. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Yoshida, M.; Ono, H.; Ohnishi-Kameyama, M.; Chuda, Y.; Yada, H.; Kobayashi, H.; Ishizaka, M. Determination of acrylamide in processed foodstuff in Japan. Nippon Shokuhin Kagaku Kogaku Kaishi 2002, 49, 822–825. (In Japanese) [Google Scholar] [CrossRef]
- Yoshida, M.; Miyoshi, K.; Horibata, K.; Mizukami, Y.; Takenaka, M.; Yasui, A. Estimation of acrylamide intake from cooked rice in Japan. Nippon Shokuhin Kagaku Kogaku Kaishi 2011, 58, 525–530. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Food and Agriculture Organization/World Health Organization. Health Implications of Acrylamide in Food 2002. Available online: http://www.who.int/foodsafety/publications/acrylamide-food/en/ (accessed on 28 September 2020).
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013; pp. 260–286. [Google Scholar]
- World Cancer Research Fund. Nutrition, Physical Activity, and Pancreatic Cancer. Available online: https://www.wcrf.org/sites/default/files/Pancreatic-cancer-report.pdf (accessed on 28 September 2020).
- Kotemori, A.; Ishihara, J.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Dietary acrylamide intake and risk of breast cancer: The Japan Public Health Center-based Prospective Study. Cancer Sci. 2018, 109, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Kotemori, A.; Ishihara, J.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Dietary acrylamide intake and the risk of endometrial or ovarian cancers in Japanese women. Cancer Sci. 2018, 109, 3316–3325. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Sobue, T.; Kitamura, T.; Kitamura, Y.; Ishihara, J.; Kotemori, A.; Zha, L.; Ikeda, S.; Sawada, N.; Iwasaki, M.; et al. Dietary Acrylamide Intake and Risk of Esophageal, Gastric, and Colorectal Cancer: The Japan Public Health Center-Based Prospective Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1461–1468. [Google Scholar] [CrossRef]
- Lucas, D.; Farez, C.; Bardou, L.G.; Vaisse, J.; Attali, J.R.; Valensi, P. Cytochrome P450 2E1 activity in diabetic and obese patients as assessed by chlorzoxazone hydroxylation. Fundam. Clin. Pharmacol. 1998, 12, 553–558. [Google Scholar] [CrossRef]
- Gade, C.; Dalhoff, K.; Petersen, T.S.; Riis, T.; Schmeltz, C.; Chabanova, E.; Christensen, H.R.; Mikus, G.; Burhenne, J.; Holm, J.C.; et al. Higher chlorzoxazone clearance in obese children compared with non-obese peers. Br. J. Clin. Pharmacol. 2018, 84, 1738–1747. [Google Scholar] [CrossRef] [Green Version]
- Peter Guengerich, F.; Avadhani, N.G. Roles of cytochrome P450 in the metabolism of ethanol and carcinogens. Adv. Exp. Med. Biol. 2018, 1032, 15–35. [Google Scholar]
- Obón-Santacana, M.; Lujan-Barroso, L.; Freisling, H.; Cadeau, C.; Fagherazzi, G.; Boutron-Ruault, M.C.; Kaaks, R.; Fortner, R.T.; Boeing, H.; Ramón Quirós, J.; et al. Dietary and lifestyle determinants of acrylamide and glycidamide hemoglobin adducts in non-smoking postmenopausal women from the EPIC cohort. Eur. J. Nutr. 2017, 56, 1157–1168. [Google Scholar] [CrossRef] [Green Version]
- Vikström, A.C.; Wilson, K.M.; Paulsson, B.; Athanassiadis, I.; Grönberg, H.; Adami, H.O.; Adolfsson, J.; Mucci, L.A.; Bälter, K.; Törnqvist, M. Alcohol influence on acrylamide to glycidamide metabolism assessed with hemoglobin-adducts and questionnaire data. Food Chem. Toxicol. 2010, 48, 820–824. [Google Scholar] [CrossRef]
- Vesper, H.W.; Slimani, N.; Hallmans, G.; Tjønneland, A.; Agudo, A.; Benetou, V.; Bingham, S.; Boeing, H.; Boutron-Ruault, M.C.; Bueno-de-Mesquita, H.B.; et al. Cross-sectional study on acrylamide hemoglobin adducts in subpopulations from the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. J. Agric. Food Chem. 2008, 56, 6046–6053. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Liu, Y.; Sun, H.; Ding, X.; Fu, D.; Liu, K.; Du, X.; Jia, G. Inhibition of acrylamide toxicity in mice by three dietary constituents. J. Agric. Food Chem. 2008, 56, 6054–6060. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA), Parma, Italy. Scientific Opinion on acrylamide in food. EFSA Panel on Contaminants in the Food Chain (CONTAM). EFSA J. 2015, 13, 4104. [Google Scholar]
- Huang, M.; Zhuang, P.; Jiao, J.; Wang, J.; Zhang, Y. Association of acrylamide hemoglobin biomarkers with obesity, abdominal obesity, and overweight in the general US population: NHANES 2003–2006. Sci. Total Environ. 2018, 631–632, 589–596. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Quartile of Acrylamide Intake | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | |||||||||||||||||
| Participants, n | 22,432 | 22,432 | 22,433 | 22,432 | ||||||||||||||||
| Male, % | 27.8 | 24.5 | 23.3 | 24.3 | ||||||||||||||||
| Female, % | 22.5 | 25.4 | 26.5 | 25.6 | ||||||||||||||||
| Acrylamide intake | ||||||||||||||||||||
| Mean, µg/day a | 3.1 | ± | 0.9 | 5.2 | ± | 0.5 | 7.3 | ± | 0.7 | 12.1 | ± | 3.5 | ||||||||
| Median, µg/day b | 3.3 | (2.6 | – | 3.8) | 5.2 | (4.7 | – | 5.6) | 7.2 | (6.6 | – | 7.9) | 11.0 | (9.7 | – | 13.3) | ||||
| Mean, µg/kg body weight/day a | 0.06 | ± | 0.04 | 0.10 | ± | 0.09 | 0.13 | ± | 0.09 | 0.22 | ± | 0.26 | ||||||||
| Age at 5-year follow-up survey, years b | 58 | (52 | – | 63) | 57 | (51 | – | 63) | 56 | (50 | – | 62) | 55 | (48 | – | 61) | ||||
| Body mass index, kg/m2 b | 23.4 | (21.6 | – | 25.5) | 23.4 | (21.5 | – | 25.4) | 23.3 | (21.4 | – | 25.3) | 23.1 | (21.3 | – | 25.2) | ||||
| Smoking status, % | ||||||||||||||||||||
| Never smoker | 60.6 | 64.5 | 64.4 | 58.9 | ||||||||||||||||
| Ex-smoker | 9.6 | 9.1 | 8.0 | 8.0 | ||||||||||||||||
| Current smoker | 23.2 | 20.6 | 21.9 | 27.7 | ||||||||||||||||
| Missing | 6.6 | 5.8 | 5.7 | 5.5 | ||||||||||||||||
| History of diabetes mellitus, % | 8.2 | 7.1 | 6.3 | 5.6 | ||||||||||||||||
| Family history of pancreatic cancer, % | 0.3 | 0.4 | 0.4 | 0.3 | ||||||||||||||||
| Dietary intake | ||||||||||||||||||||
| Energy, kcal/d a,c | 1999 | ± | 642 | 1998 | ± | 610 | 2013 | ± | 612 | 1977 | ± | 622 | ||||||||
| Alcohol intake, g/week a | 155 | ± | 250 | 108 | ± | 197 | 90 | ± | 175 | 70 | ± | 146 | ||||||||
| Coffee, g/d a,c | 34 | ± | 50 | 81 | ± | 82 | 144 | ± | 131 | 324 | ± | 313 | ||||||||
| Green tea, g/d a,c | 285 | ± | 314 | 460 | ± | 407 | 559 | ± | 449 | 802 | ± | 732 | ||||||||
| Potato, g/d a,c | 9 | ± | 9 | 16 | ± | 13 | 19 | ± | 17 | 21 | ± | 25 | ||||||||
| Biscuits and cookies, g/d a,c | 1 | ± | 1 | 2 | ± | 2 | 3 | ± | 3 | 5 | ± | 8 | ||||||||
| Vegetables, g/d a,c | 178 | ± | 118 | 208 | ± | 119 | 221 | ± | 128 | 221 | ± | 138 | ||||||||
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p for Trend | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | HR | (95% CI) | HR | (95% CI) | HR | (95% CI) | HR | (95% CI) | ||
| All | ||||||||||
| Participants, n | 89,729 | 22,432 | 22,432 | 22,433 | 22,432 | |||||
| Cases, n | 576 | 180 | 143 | 126 | 127 | |||||
| Person-years | 1,360,237 | 340,654 | 341,672 | 340,712 | 337,198 | |||||
| Age- and area-adjusted a | 1.00 | (Reference) | 0.83 | (0.66–1.03) | 0.77 | (0.61–0.97) | 0.84 | (0.67–1.07) | 0.09 | |
| Multivariate-adjusted b | 1.00 | (Reference) | 0.84 | (0.67–1.05) | 0.77 | (0.61–0.97) | 0.83 | (0.65–1.05) | 0.07 | |
| Multivariate-adjusted (excluding cases <3 y) b | 1.00 | (Reference) | 0.83 | (0.66–1.06) | 0.77 | (0.60–0.99) | 0.82 | (0.63–1.05) | 0.08 | |
| Male | ||||||||||
| Cases, n | 319 | 108 | 70 | 67 | 74 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.74 | (0.55–1.01) | 0.77 | (0.56–1.05) | 0.85 | (0.62–1.17) | 0.29 | |
| Female | ||||||||||
| Cases, n | 257 | 72 | 73 | 59 | 53 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.97 | (0.70–1.35) | 0.79 | (0.56–1.13) | 0.83 | (0.58–1.20) | 0.19 | |
| By smoking status | ||||||||||
| Current or past smokers | ||||||||||
| Cases, n | 235 | 73 | 57 | 47 | 58 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.89 | (0.63–1.26) | 0.75 | (0.52–1.10) | 0.84 | (0.58–1.21) | 0.25 | |
| Never smokers | ||||||||||
| Cases, n | 285 | 89 | 69 | 73 | 54 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.76 | (0.56–1.05) | 0.85 | (0.62–1.17) | 0.78 | (0.55–1.11) | 0.23 | |
| By coffee consumption | ||||||||||
| <1 cup/week | ||||||||||
| Cases, n | 173 | 99 | 36 | 21 | 17 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.72 | (0.49–1.05) | 0.66 | (0.41–1.07) | 0.80 | (0.47–1.35) | 0.11 | |
| ≥1 cup/week | ||||||||||
| Cases, n | 403 | 81 | 107 | 105 | 110 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.88 | (0.66–1.18) | 0.78 | (0.58–1.05) | 0.81 | (0.60–1.10) | 0.15 | |
| By green tea consumption | ||||||||||
| <1 cup/week | ||||||||||
| Cases, n | 44 | 29 | 9 | 4 | 2 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.98 | (0.46–2.10) | 0.69 | (0.24–2.00) | 0.43 | (0.10–1.86) | 0.23 | |
| ≥1 cup/week | ||||||||||
| Cases, n | 532 | 151 | 134 | 122 | 125 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.84 | (0.67–1.07) | 0.79 | (0.62–1.01) | 0.86 | (0.67–1.10) | 0.18 | |
| By alcohol consumption | ||||||||||
| <150 g/wk | ||||||||||
| Cases, n | 416 | 111 | 107 | 95 | 103 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.90 | (0.69–1.18) | 0.79 | (0.60–1.04) | 0.86 | (0.65–1.14) | 0.20 | |
| ≥150 g/wk | ||||||||||
| Cases, n | 160 | 69 | 36 | 31 | 24 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.71 | (0.47–1.06) | 0.75 | (0.49–1.15) | 0.77 | (0.48–1.25) | 0.19 | |
| By BMI | ||||||||||
| <25 kg/m2 | ||||||||||
| Cases, n | 411 | 122 | 104 | 93 | 92 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.88 | (0.67–1.14) | 0.80 | (0.61–1.05) | 0.81 | (0.61–1.08) | 0.11 | |
| ≥25 kg/m2 | ||||||||||
| Cases, n | 141 | 46 | 33 | 31 | 31 | |||||
| Multivariate-adjusted b | 1.00 | (Reference) | 0.78 | (0.50–1.23) | 0.80 | (0.51–1.28) | 0.93 | (0.58–1.50) | 0.71 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kito, K.; Ishihara, J.; Kotemori, A.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Dietary Acrylamide Intake and the Risk of Pancreatic Cancer: The Japan Public Health Center-Based Prospective Study. Nutrients 2020, 12, 3584. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113584
Kito K, Ishihara J, Kotemori A, Zha L, Liu R, Sawada N, Iwasaki M, Sobue T, Tsugane S. Dietary Acrylamide Intake and the Risk of Pancreatic Cancer: The Japan Public Health Center-Based Prospective Study. Nutrients. 2020; 12(11):3584. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113584
Chicago/Turabian StyleKito, Kumiko, Junko Ishihara, Ayaka Kotemori, Ling Zha, Rong Liu, Norie Sawada, Motoki Iwasaki, Tomotaka Sobue, and Shoichiro Tsugane. 2020. "Dietary Acrylamide Intake and the Risk of Pancreatic Cancer: The Japan Public Health Center-Based Prospective Study" Nutrients 12, no. 11: 3584. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113584