Adherence to Prudent and Mediterranean Dietary Patterns Is Inversely Associated with Lung Cancer in Moderate But Not Heavy Male Polish Smokers: A Case-Control Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
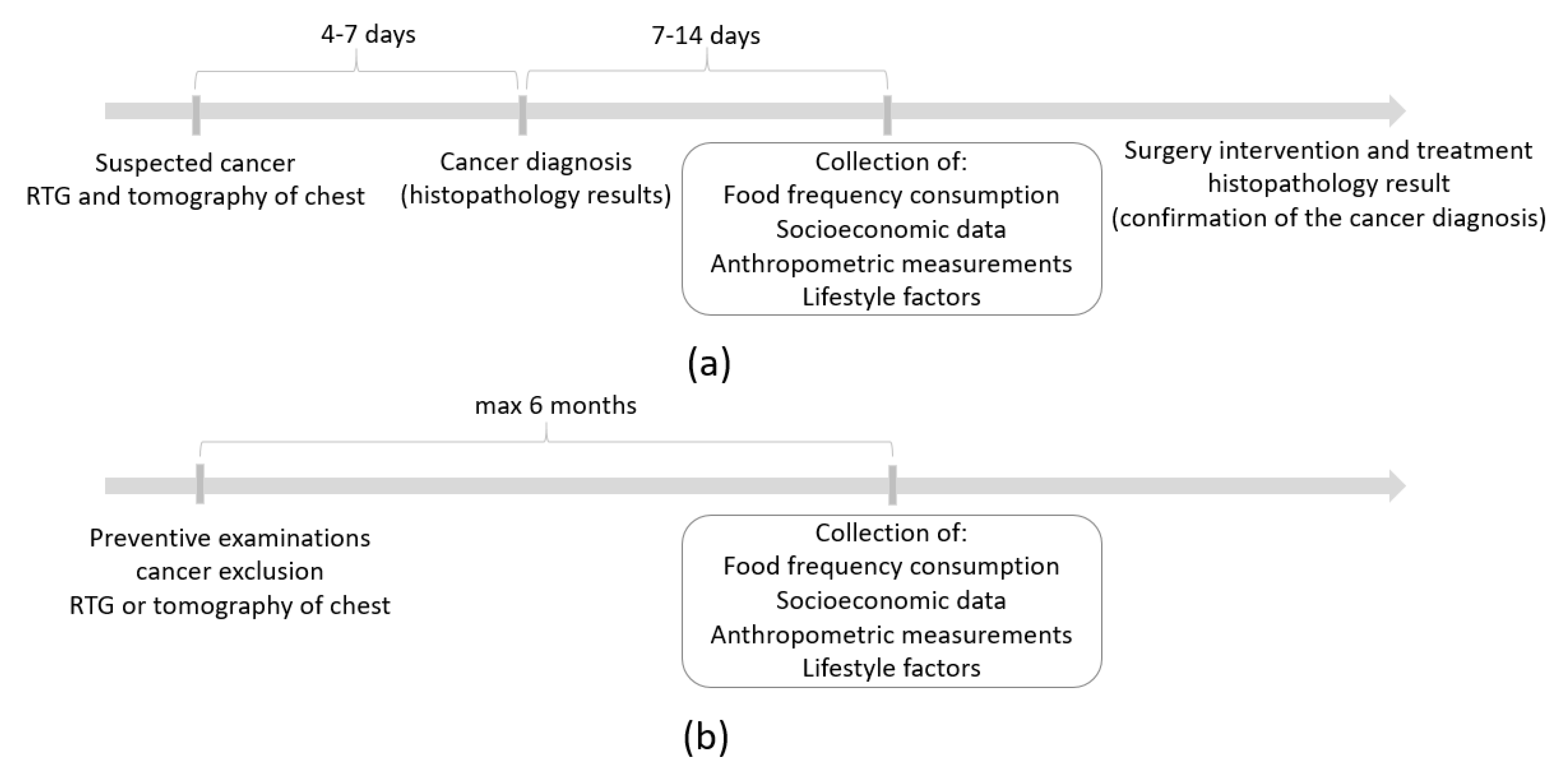
2.2. Study Design and Sample Characteristics
2.3. Dietary Data Collection and Dietary Pattern Identification
2.4. Smoking
- A man reported smoking 30 cigarettes a day for 10 years.
- The calculated number of pack-years is: 10 × 30/20 = 15 pack-years
- 10—years of smoking
- 30—number of cigarettes per day
- 20—number of cigarettes in one pack
2.5. Confounders
2.6. Statistical Analysis
3. Results
3.1. Food Consumption Frequency and Dietary Patterns
3.2. Dietary Patterns and Lung Cancer
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. Editors 2020. World Cancer Report: Cancer Research for Cancer Prevention; International Agency for Research on Cancer: Lyon, France, 2020; Available online: http://publications.iarc.fr/586 (accessed on 22 March 2020).
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef]
- Wojciechowska, U.; Didkowska, J. Zachorowania i zgony na Nowotwory Złośliwe w Polsce; Krajowy Rejestr Nowotworów, Narodowy Instytut Onkologii im. Marii Skłodowskiej-Curie Państwowy Instytut Badawczy: Warszawa, Poland, 2014; Available online: http://onkologia.org.pl/raporty/ (accessed on 4 February 2020).
- OECD. Health at a Glance 2019: OECD Indicators; OECD: Paris, Frace, 2019; Available online: https://0-doi-org.brum.beds.ac.uk/10.1787/4dd50c09-en (accessed on 4 February 2020).
- Kathuria, H.; Neptune, E. Primary and Secondary Prevention of Lung Cancer. Clin. Chest Med. 2020, 41, 39–51. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition, Physical Activity and Lung Cancer. Available online: https://www.wcrf.org/sites/default/files/Lung-cancer-report.pdf (accessed on 4 February 2020).
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentley, A.R.; Kritchevsky, S.B.; Harris, T.B.; Holvoet, P.; Jensen, R.L.; Newman, A.B.; Lee, J.S.; Yende, S.; Bauer, D. Health ABC Study. Dietary antioxidants and forced expiratory volume in 1 s decline: The Health, Aging and Body Composition study. Eur. Respir. J. 2012, 39, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.P.; Niti, M.; Yap, K.B.; Tan, W.C. Dietary and supplemental antioxidant and anti-inflammatory nutrient intakes and pulmonary function. Public Health Nutr. 2014, 17, 2081–2086. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Larsen, V.; Amigo, H.; Bustos, P.; Bakolis, I.; Rona, R.J. Ventilatory function in young adults and dietary antioxidant intake. Nutrients 2015, 7, 2879–2896. [Google Scholar] [CrossRef] [Green Version]
- de Alencar, V.T.L.; Formiga, M.N.; de Lima, V.C.C. Inherited lung cancer: A review. E Cancer Med. Sci. 2020, 29, 1008. [Google Scholar] [CrossRef]
- Sun, S.; Schiller, J.; Gazdar, A. Lung cancer in never smokers—A different disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef]
- Gorlova, O.Y.; Weng, S.F.; Hernandez, L.; Spitz, M.R.; Forman, M.R. Dietary patterns affect lung cancer risk in never smokers. Nutr. Cancer 2011, 63, 842–849. [Google Scholar] [CrossRef]
- Elisia, I.; Cho, B.; Hay, M.; Li, M.Y.; Hofs, E.; Lam, V.; Dyer, R.A.; Lum, J.; Krystal, G. The effect of diet and exercise on tobacco carcinogen-induced lung cancer. Carcinogenesis 2019, 14, 448–460. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. Available online: https://www.wcrf.org/sites/default/files/Summary-of-Third-Expert-Report-2018.pdf (accessed on 4 February 2020).
- Vieira, A.R.; Abar, L.; Vingeliene, S.; Chan, D.S.; Aune, D.; Navarro-Rosenblatt, D.; Stevens, C.; Greenwood, D.; Norat, T. Fruits, vegetables and lung cancer risk: A systematic review and meta-analysis. Ann. Oncol. 2016, 27, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Abar, L.; Vieira, A.R.; Aune, D.; Stevens, C.; Vingeliene, S.; Rosenblatt, D.A.N.; Chan, D.; Greenwood, D.C.; Norat, T. Blood concentrations of carotenoids and retinol and lung cancer risk: An update of the WCRF-AICR systematic review of published prospective studies. Cancer Med. 2016, 5, 2069–2083. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Mattiuzzi, C.; Cervellin, G. Meat consumption and cancer risk: A critical review of published meta-analyses. Crit. Rev. Oncol. Hematol. 2016, 97, 1–14. [Google Scholar] [CrossRef]
- Sharma, P.; McClees, S.F.; Afaq, F. Pomegranate for prevention and treatment of cancer: An update. Molecules 2017, 22, 177. [Google Scholar] [CrossRef] [Green Version]
- Wakai, K.; Sugawara, Y.; Tsuji, I.; Tamakoshi, A.; Shimazu, T.; Matsuo, K.; Nagata, C.; Mizoue, T.; Tanaka, K.; Inoue, M.; et al. Risk of lung cancer and consumption of vegetables and fruit in Japanese: A pooled analysis of cohort studies in Japan. Cancer Sci. 2015, 106, 1057–1065. [Google Scholar] [CrossRef] [Green Version]
- Gilsing, A.M.; Weijenberg, M.P.; Goldbohm, R.A.; Dagnelie, P.C.; van den Brandt, P.A.; Schouten, L.J. Vegetarianism, low meat consumption and the risk of lung, postmenopausal breast and prostate cancer in a population-based cohort study. Eur. J. Clin. Nutr. 2016, 70, 723–729. [Google Scholar] [CrossRef]
- Luqman, M.; Javed, M.M.; Daud, S.; Raheem, N.; Ahmad, J.; Khan, A.U. Risk factors for lung cancer in the Pakistani population. Asian Pac. J. Cancer Prev. 2014, 15, 3035–3039. [Google Scholar] [CrossRef] [Green Version]
- Linseisen, J.; Rohrmann, S.; Bueno-de-Mesquita, B.; Büchner, F.L.; Boshuizen, H.C.; Agudo, A.; Gram, I.T.; Dahm, C.C.; Overvad, K.; Egeberg, R.; et al. Consumption of meat and fish and risk of lung cancer: Results from the European Prospective Investigation into Cancer and Nutrition. Cancer Causes Control. 2011, 22, 909–918. [Google Scholar] [CrossRef]
- Theodoratou, E.; Timofeeva, M.; Li, X.; Meng, X.; Ioannidis, J.P.A. Nature, Nurture, and Cancer Risks: Genetic and Nutritional Contributions to Cancer. Annu. Rev. Nutr. 2017, 37, 293–320. [Google Scholar] [CrossRef]
- Narita, S.; Saito, E.; Sawada, N.; Shimazu, T.; Yamaji, T.; Iwasaki, M.; Ishihara, J.; Takachi, R.; Shibuya, K.; Inoue, M.; et al. Dietary consumption of antioxidant vitamins and subsequent lung cancer risk: The Japan Public Health center-based prospective study. Int. J. Cancer 2018, 142, 2441–2460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, K.L. Dietary patterns, approaches, and multicultural perspective. Appl. Physiol. Nutr. Metab. 2010, 35, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Wirfält, E.; Flood, A.; Mitrou, P.N.; Krebs-Smith, S.M.; Kipnis, V.; Midthune, D.; Leitzmann, M.; Hollenbeck, A.; Schatzkin, A.; et al. Comparing 3 dietary pattern methods—Cluster analysis, factor analysis, and index analysis—With colorectal cancer risk: The NIH–AARP Diet and Health Study. Am. J. Epidemiol. 2010, 171, 479–487. [Google Scholar] [CrossRef]
- Tu, H.; Heymach, J.V.; Wen, C.P.; Ye, Y.; Pierzynski, J.A.; Roth, J.A.; Wu, X. Different dietary patterns and reduction of lung cancer risk: A large cases-control study in the U.S. Sci. Rep. 2016, 6, 26760. [Google Scholar] [CrossRef]
- Sun, Y.; Li, Z.; Li, J.; Li, Z.; Han, J. A Healthy Dietary Pattern Reduces Lung Cancer Risk: A Systematic Review and Meta-Analysis. Nutrients 2016, 8, 134. [Google Scholar] [CrossRef] [Green Version]
- Balder, H.F.; Goldbohm, R.A.; van den Brandt, P.A. Dietary patterns associated with male lung cancer risk in the Netherlands Cohort Study. Cancer Epidemiol. Biomark. Prev. 2005, 14, 483–490. [Google Scholar] [CrossRef] [Green Version]
- He, F.; Xiao, R.D.; Lin, T.; Xiong, W.M.; Xu, Q.P.; Li, X.; Liu, Z.G.; He, B.C.; Hu, Z.J.; Cai, L. Dietary patterns, BCMO1 polymorphisms, and primary lung cancer risk in a Han Chinese population: A case-control study in Southeast China. BMC Cancer 2018, 18, 445. [Google Scholar] [CrossRef]
- Krusinska, B.; Hawrysz, I.; Slowinska, M.A.; Wadolowska, L.; Biernacki, M.; Czerwinska, A.; Golota, J.J. Dietary patterns and breast or lung cancer risk: A pooled analysis of two case-control studies in northern-eastern Poland. Adv. Clin. Exp. Med. 2017, 9, 1367–1375. [Google Scholar] [CrossRef] [Green Version]
- Krusinska, B.; Hawrysz, I.; Wadolowska, L.; Slowinska, M.A.; Biernacki, M.; Czerwinska, A.; Golota, J.J. Associations of Mediterranean Diet and a Posteriori Derived Dietary Patterns with Breast and Lung Cancer Risk: A Case-Control Study. Nutrients 2018, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- Anic, G.M.; Park, Y.; Subar, A.F.; Schap, T.E.; Reedy, J. Index-based dietary patterns and risk of lung cancer in the NIH-AARP diet and health study. Eur. J. Clin. Nutr. 2016, 70, 123–129. [Google Scholar] [CrossRef]
- De Stefani, E.; Boffetta, P.; Ronco, A.L.; Deneo-Pellegrini, H.; Acosta, G.; Gutiérrez, L.P.; Mendilaharsu, M. Nutrient patterns and risk of lung cancer: A factor analysis in Uruguayan men. Lung Cancer 2008, 61, 283–291. [Google Scholar] [CrossRef] [PubMed]
- De Stefani, E.; Deneo-Pellegrini, H.; Boffetta, P.; Ronco, A.L.; Aune, D.; Acosta, G.; Mendilaharsu, M.; Brennan, P.; Ferro, G. Dietary patterns and risk of cancer: A factor analysis in Uruguay. Int. J. Cancer 2009, 124, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, A.; Gibney, M.J.; Brennan, L. Dietary intake patterns are reflected in metabolomics profiles: Potential role in dietary assessment studies. Am. J. Clin. Nutr. 2011, 93, 314–321. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Does a Mediterranean-type diet reduce cancer risk? Curr. Nutr. Rep. 2016, 5, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Schulpen, M.; van den Brandt, P.A. Adherence to the Mediterranean diet and risk of lung cancer in the Netherlands Cohort Study. Br. J. Nutr. 2018, 119, 674–684. [Google Scholar] [CrossRef] [Green Version]
- Hodge, A.M.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; English, D.R.; Giles, G.G.; Severi, G. Dietary inflammatory index, Mediterranean diet score, and lung cancer: A prospective study. Cancer Causes Control 2016, 27, 907–917. [Google Scholar] [CrossRef] [Green Version]
- Gnagnarella, P.; Maisonneuve, P.; Bellomi, M.; Rampinelli, C.; Bertolotti, R.; Spaggiari, L.; Palli, D.; Veronesi, G. Red meat, Mediterranean diet and lung cancer risk among heavy smokers in the COSMOS screening study. Ann. Oncol. 2013, 24, 2606–2611. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean diet: A review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosetti, C.; Gallus, S.; Trichopoulou, A.; Talamini, R.; Franceschi, S.; Nergi, E.; La Vecchia, C. Influence of the Mediterranean diet on the risk of cancers of the upper aerodigestive tract. Cancer Epidemiol. Biomark. Prev. 2003, 12, 1091–1094. [Google Scholar]
- Noah, A.; Truswell, A.S. There are many Mediterranean diets. Asia Pac. J. Clin. Nutr. 2001, 10, 2–9. [Google Scholar] [CrossRef]
- Mohtadi, K.; Msaad, R.; Benalioua, N.; Jafri, A.; Meftah, H.; Elkardi, Y.; Lebrazi, H.; Kettani, A.; Derouiche, A.; Taki, H.; et al. Sociodemographic and Lifestyle Factors Associated with Adherence to Mediterranean Diet in Representative Adult Population in Casablanca City, Morocco: A Cross-Sectional Study. J. Nutr. Metab. 2020, 3, 20. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Lamuela-Raventós, R.; Doménech, M.; Estruch, R. Relationship between polyphenol intake in the Mediterranean diet and obesity. Nutrients 2018, 10, 1523. [Google Scholar] [CrossRef] [Green Version]
- Kwan, H.Y.; Chao, X.; Su, T.; Fu, X.; Tse, A.K.; Fong, W.F.; Yu, Z.L. The anticancer and antiobesity effects of Mediterranean diet. Crit. Rev. Food Sci. Nutr. 2017, 57, 82–94. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Moustaid-Moussa, N. Health benefits of n-3 polyunsaturated fatty acids: Eicosapentaenoic acid and docosahexaenoic acid. Adv. Food Nutr. Res. 2012, 65, 211–222. [Google Scholar] [CrossRef]
- Lee, J.T.; Lai, G.Y.; Liao, L.M.; Subar, A.F.; Bertazzi, P.A.; Pesatori, A.C.; Freedman, N.D.; Landi, M.T.; Lam, T.K. Nut Consumption and Lung Cancer Risk: Results from Two Large Observational Studies. Cancer Epidemiol. Biomark. Prev. 2017, 26, 826–836. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Niedzwiedzka, E.; Wadolowska, L.; Kowalkowska, J. Reproducibility of a Non-Quantitative Food Frequency Questionnaire (62-Item FFQ-6) and PCA-Driven Dietary Pattern Identification in 13–21-Year-Old Females. Nutrients 2019, 11, 2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidia Wadolowska Website. Available online: http://www.uwm.edu.pl/edu/lidiawadolowska/ (accessed on 7 September 2020).
- Previdelli, Á.N.; de Andrade, S.C.; Fisberg, R.M.; Marchioni, D.M. Using two different approaches to assess dietary patterns: Hypothesis-driven and data-driven analysis. Nutrients 2016, 8, 593. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Bartlett, M.S. Test of significance in factor analysis. Br. J. Math Stat. Psychol. 1950, 3, 77–85. [Google Scholar] [CrossRef]
- Osborne, J.W.; Costello, A.B. Sample size and subject to item ratio in principal components analysis. Pract. Assess. Res. Eval. 2004, 9, 1–9. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage Publications: London, UK, 2009. [Google Scholar]
- Fung, T.T.; McCullough, M.L.; Newby, P.K.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef] [PubMed]
- NIAAA. What Is a Standard Drink? 2018. Available online: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/what-standard-drink (accessed on 10 April 2020).
- Barragán, R.; Coltell, O.; Asensio, E.M.; Francés, F.; Sorlí, J.V.; Estruch, R.; Salas-Huetos, A.; Ordovas, J.M.; Corella, D. MicroRNAs and Drinking: Association between the Pre-miR-27a rs895819 Polymorphism and Alcohol Consumption in a Mediterranean Population. Int. J. Mol. Sci. 2016, 17, 1338. [Google Scholar] [CrossRef] [Green Version]
- Bernaards, C.M.; Twisk, J.W.; Snel, J.; Van Mechelen, W.; Kemper, H.C. Is calculating pack-years retrospectively a valid method to estimate life-time tobacco smoking? A comparison between prospectively calculated pack-years and retrospectively calculated pack-years. Addiction 2001, 96, 1653–1661. [Google Scholar] [CrossRef]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell Science: Oxford, UK, 2001. [Google Scholar]
- Jarosz, M.; Taraszewska, A. Nadwaga i otyłość oraz wybrane elementy stylu życia jako czynniki ryzyka GERD. (Overweight and obesity and selected lifestyle elements as risk factors for GERD). Postępy Nauk Med. 2011, 9, 749–759. [Google Scholar]
- Wadolowska, L.; Krusinska, B. The manual for developing nutritional data from the KomPAN questionnaire. In Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing of Nutritional Data; Gawecki, J., Ed.; The Committee of Human Nutrition, Polish Academy of Sciences: Warsaw, Poland, 2014; pp. 34–51. ISBN 978-83-63305-19-2. Available online: http://www.knozc.pan.pl/ (accessed on 22 March 2020).
- De Stefani, E.; Ronco, A.L.; Deneo-Pellegrini, H.; Correa, P.; Boffetta, P.; Acosta, G.; Mendilaharsu, M. Dietary patterns and risk of adenocarcinoma of the lung in males: A factor analysis in Uruguay. Nutr. Cancer 2011, 63, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Bodén, S.; Myte, R.; Wennberg, M.; Harlid, S.; Johansson, I.; Shivappa, N.; Hébert, J.R.; Van Guelpen, B.; Nilsson, L.M. The inflammatory potential of diet in determining cancer risk; A prospective investigation of two dietary pattern scores. PLoS ONE 2019, 14, e0214551. [Google Scholar] [CrossRef] [PubMed]
- Maisonneuve, P.; Shivappa, N.; Hébert, R.; Bellomi, M.; Rampinelli, C.; Bertolotti, R.; Spaggiari, L.; Palli, D.; Veronesi, G.; Gnagnarella, P. Dietary inflammatory index and risk of lung cancer and other respiratory conditions among heavy smokers in the COSMOS screening study. Eur. J. Nutr. 2016, 55, 1069–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2020, 8, 1–26. [Google Scholar] [CrossRef]
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.C.; Tjonneland, A.; O Olsen, A.; Clavelchapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef] [Green Version]
- Gnagnarella, P.; Maisonneuve, P.; Bellomi, M.; Raffaella, B.; Bertolotti, R.; Spaggiari, L.; Palli, D.; Veronesi, G. Nutrient intake and nutrient patterns and risk of lung cancer among heavy smokers: Results from the COSMOS screening study with annual low-dose CT. Eur. J. Epidemiol. 2013, 28, 503–511. [Google Scholar] [CrossRef]
- Dlugosz, A. Dietary Patterns, Adverse Health Outcomes, Socioeconomic Situation and Lifestyle of Adolescents from Less Urbanised Regions of Poland [Dissertations and Monographs]; Wydawnictwo UWM: Olsztyn, Poland, 2017; ISBN 978-83-8100-076-5. [Google Scholar]
- De Stefani, E.; Deneo-Pellegrini, H.; Mendilaharsu, M.; Ronco, A.; Carzoglio, J.C. Dietary sugar and lung cancer: A case-control study in Uruguay. Nutr. Cancer 1998, 31, 132–137. [Google Scholar] [CrossRef]
- Osadnik, T.; Pawlas, N.; Lonnie, M.; Osadnik, K.; Lejawa, M.; Wadolowska, L.; Bujak, K.; Fronczek, M.; Reguła, R.; Gawlita, M.; et al. Family History of Premature Coronary Artery Disease (P-CAD)-A Non-Modifiable Risk Factor? Dietary Patterns of Young Healthy Offspring of P-CAD Patients: A Case-Control Study (MAGNETIC Project). Nutrients 2018, 10, 1488. [Google Scholar] [CrossRef] [Green Version]
- Ceci, C.; Lacal, P.M.; Tentori, L.; De Martino, M.G.; Miano, R.; Graziani, G. Experimental Evidence of the Antitumor, Antimetastatic and Antiangiogenic Activity of Ellagic Acid. Nutrients 2018, 10, 1756. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, M.; Naghan, P.A.; Jafari, A.M.; Yousefifard, M.; Taslimi, S.; Khodadad, K.; Mohammadi, F.; Sadr, M.; Rezaei, M.; Mortaz, E.; et al. Nutrition and lung cancer: A case control study in Iran. BMC Cancer 2014, 14, 860. [Google Scholar] [CrossRef] [Green Version]
- Pala, V.; Sieri, S.; Masala, G.; Palli, D.; Panico, S.; Vineis, P.; Sacerdote, C.; Mattiello, A.; Galasso, R.; Salvini, S.; et al. Associations between dietary pattern and lifestyle, anthropometry and other health indicators in the elderly participants of the EPIC-Italy cohort. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 186–201. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Agriculture Organization (FAO). Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings. Rome, Italy. 2018. Available online: http://www.fao.org/3/i9940en/I9940EN (accessed on 20 November 2020).
- Duncan, C.T. Invited Commentary: Is It Time to Retire the “Pack-Years” Variable? Maybe Not! Am. J. Epidemiol. 2014, 179, 299–302. [Google Scholar]
- Kant, A.K. Dietary patterns: Biomarkers and chronic disease risk. Appl. Physiol. Nutr. Metab. 2010, 4, 7. [Google Scholar]
- Nguyen, H.H.; Wu, F.; Oddy, W.H.; Wills, K.; Winzenberg, T.; Jones, G. Associations between dietary patterns and osteoporosis-related outcomes in older adults: A longitudinal study. Eur. J. Clin. Nutr. 2020, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Ruano, C.; Henriquez, P.; Martínez-González, M.Á.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Sanchez-Villegas, A. Empirically derived dietary patterns and health-related quality of life in the SUN project. PLoS ONE 2013, 8, e61490. [Google Scholar] [CrossRef] [Green Version]
- Trudeau, K.; Rousseau, M.-C.; Barul, C.; Csizmadi, I.; Parent, M.-É. Dietary Patterns Are Associated with Risk of Prostate Cancer in a Population-Based Case-Control Study in Montreal, Canada. Nutrients 2020, 12, 1907. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. Exploratory factor analysis: A five-step guide for novices. J. Emerg. Prim. Health Care 2010, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wirfält, E.; Drake, I.; Wallström, P. What do review papers conclude about food and dietary patterns? Food Nutr. Res. 2013, 57, 20523. [Google Scholar] [CrossRef] [Green Version]
- Kowalkowska, J.; Wadolowska, L.; Czarnocinska, J.; Czlapka-Matyasik, M.; Galinski, G.; Jezewska-Zychowicz, M.; Bronkowska, M.; Długosz, A.; Loboda, D.; Wyka, J. Reproducibility of a Questionnaire for Dietary Habits, Lifestyle and Nutrition Knowledge Assessment (KomPAN) in Polish Adolescents and Adults. Nutrients 2018, 10, 1845. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Cancer Control Sample | Cancer Sample | Control Sample | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sample size | 439 | 100.0 | 187 | 100.0 | 252 | 100.0 | |
| Age (years *) | 62.6 (7.2) | 63.0 (7.1) | 62.3 (7.3) | 0.2586 | |||
| 45.0–49.9 | 12 | 2.8 | 3 | 1.6 | 9 | 3.6 | <0.0001 |
| 50.0–54.9 | 41 | 9.3 | 12 | 6.4 | 29 | 11.5 | |
| 55.0–59.9 | 76 | 17.3 | 24 | 12.8 | 52 | 20.6 | |
| 60.0–64.9 | 133 | 30.3 | 51 | 27.3 | 82 | 32.5 | |
| 65.0–69.9 | 97 | 22.1 | 42 | 22.5 | 55 | 21.8 | |
| 70.0–74.9 | 47 | 10.7 | 29 | 15.5 | 18 | 7.1 | |
| 75.0–80.0 | 33 | 7.5 | 26 | 13.9 | 7 | 2.8 | |
| BMI (kg/m2 *) | 27.7 (4.8) | 27.3 (4.9) | 28.0 (4.7) | 0.1354 | |||
| <18.5 | 10 | 2.3 | 10 | 5.4 | 0 | 0.0 | <0.0001 |
| 18.5–24.9 | 125 | 28.5 | 86 | 46.0 | 39 | 15.5 | |
| 25.0–29.9 | 160 | 36.4 | 55 | 29.4 | 105 | 41.7 | |
| ≥30 | 144 | 32.8 | 36 | 19.2 | 108 | 42.8 | |
| Place of residence | |||||||
| rural | 152 | 34.6 | 67 | 35.8 | 85 | 33.7 | 0.5981 |
| sub-urban | 202 | 46.0 | 81 | 43.3 | 121 | 48.0 | |
| urban | 85 | 19.4 | 39 | 20.9 | 46 | 18.3 | |
| Education level | |||||||
| primary | 104 | 23.7 | 72 | 38.5 | 32 | 12.7 | <0.0001 |
| secondary | 258 | 58.8 | 104 | 55.6 | 154 | 61.1 | |
| higher | 77 | 17.5 | 11 | 5.9 | 66 | 26.2 | |
| Economic situation | |||||||
| below average | 91 | 20.7 | 53 | 28.3 | 38 | 15.1 | <0.0001 |
| average | 278 | 63.3 | 118 | 63.1 | 160 | 63.5 | |
| above average | 70 | 16.0 | 16 | 8.6 | 54 | 21.4 | |
| Socioeconomic status (SES index) a | |||||||
| low | 235 | 53.5 | 121 | 64.7 | 114 | 45.2 | 0.0002 |
| average | 87 | 19.,8 | 25 | 13.4 | 62 | 24.6 | |
| high | 117 | 26.6 | 41 | 21.9 | 76 | 30.2 | |
| Physical activity at work b | |||||||
| low | 223 | 50.8 | 115 | 61.5 | 108 | 42.9 | 0.0003 |
| moderate | 154 | 35.1 | 48 | 25.7 | 106 | 42.0 | |
| high | 62 | 14.1 | 24 | 12.8 | 38 | 15.1 | |
| Physical activity in leisure time c | |||||||
| low | 148 | 33.7 | 71 | 38.0 | 77 | 30.6 | 0.2570 |
| moderate | 236 | 53.8 | 95 | 50.8 | 141 | 55.9 | |
| high | 55 | 12.5 | 21 | 11.2 | 34 | 13.5 | |
| Overall physical activity d | |||||||
| low | 227 | 51.7 | 113 | 60.4 | 114 | 45.2 | 0.0069 |
| moderate | 165 | 37.6 | 57 | 30.5 | 108 | 42.9 | |
| high | 47 | 10.7 | 17 | 9.1 | 30 | 11.9 | |
| Current smoking status | |||||||
| never smokers | 50 | 12.5 | 1 | 0.5 | 49 | 19.5 | <0.0001 |
| current smokers | 157 | 34.6 | 69 | 36.9 | 88 | 45.6 | |
| former smokers | 232 | 52.9 | 117 | 62.6 | 115 | 34.9 | |
| Smoking period | |||||||
| never smokers | 55 | 12.5 | 1 | 0.5 | 54 | 21.4 | <0.0001 |
| <5 years | 27 | 6.1 | 5 | 2.7 | 22 | 8.7 | |
| 5–10 years | 13 | 3.0 | 2 | 1.1 | 11 | 4.4 | |
| >10 years | 344 | 78.4 | 179 | 95.7 | 165 | 65.5 | |
| Number of cigarettes smoked | |||||||
| 0 pcs | 55 | 12.5 | 1 | 0.5 | 54 | 21.4 | <0.0001 |
| <10 pcs | 28 | 6.4 | 6 | 3.2 | 22 | 8.7 | |
| 11–20 pcs | 217 | 49.4 | 104 | 55.6 | 113 | 44.9 | |
| 21–40 pcs | 104 | 23.7 | 50 | 26.8 | 54 | 21.4 | |
| >40 pcs | 35 | 8.0 | 26 | 13.9 | 9 | 3.6 | |
| Smoking (pack-years) | |||||||
| 0 pack-years (never smoker) | 55 | 12.5 | 1 | 0.5 | 54 | 21.4 | <0.0001 |
| 2.5–11 pack-years (moderate smoker) | 252 | 57.4 | 112 | 59.9 | 140 | 55.6 | |
| >11 pack-years (heavy smoker) | 132 | 30.1 | 74 | 39.6 | 58 | 23.0 | |
| Family history of lung cancer among relatives | |||||||
| yes | 91 | 20.7 | 39 | 20.9 | 52 | 20.6 | 0.9945 |
| no | 324 | 73.8 | 138 | 73.8 | 186 | 73.8 | |
| I do not know | 28 | 5.5 | 10 | 5.3 | 14 | 5.6 | |
| Occupational exposure in the workplace | |||||||
| yes | 137 | 31.2 | 64 | 34.2 | 73 | 28.9 | 0.2399 |
| no | 302 | 68.8 | 123 | 65.8 | 179 | 71.1 | |
| Food Groups | PCA-Derived Dietary Patterns | Polish-aMED Score | ||
|---|---|---|---|---|
| Prudent | Westernized Traditional | Sweet Dairy | ||
| Whole grain products | 0.65 | −0.04 | −0.03 | 0.49 * |
| Fruits | 0.64 | 0.16 | 0.24 | 0.25 * |
| Nuts and seeds | 0.57 | 0.05 | 0.12 | 0.54 * |
| Vegetables | 0.49 | 0.43 | 0.20 | 0.50 * |
| Fish | 0.48 | 0.23 | 0.08 | 0.41 |
| Legumes | 0.47 | 0.04 | 0.26 | 0.41 * |
| Fruit, vegetable, vegetable-fruit juices | 0.32 | 0.20 | 0.26 | 0.21 * |
| Refined grains products | −0.54 | 0.39 | 0.35 | −0.21 * |
| Sugar, honey, and sweets | −0.45 | 0.37 | 0.37 | −0.09 |
| Red and processed meats | 0.08 | 0.63 | 0.07 | −0.00 |
| White meat | 0.19 | 0.56 | −0.01 | 0.13 * |
| Potatoes | −0.13 | 0.51 | 0.13 | −0.02 |
| Other fats | −0.18 | 0.45 | −0.39 | −0.13 * |
| Sweetened beverages and energy drinks | 0.10 | 0.38 | 0.23 | 0.14 * |
| Animal fats | −0.11 | 0.01 | 0.66 | 0.06 |
| Milk, fermented milk drinks, and curd cheese | 0.13 | 0.12 | 0.49 | 0.17 * |
| Sweetened milk drinks and flavored homogenized cheese | −0.02 | 0.01 | 0.45 | 0.07 |
| Eggs | 0.12 | 0.17 | 0.43 | 0.14 * |
| Cheese | 0.12 | 0.15 | 0.38 | 0.19 * |
| Breakfast cereals | 0.10 | −0.25 | 0.37 | 0.10 * |
| Vegetable oils | 0.11 | 0.24 | 0.33 | 0.11 * |
| Dried fruit and preserves | 0.23 | 0.02 | 0.32 | 0.15 * |
| Alcohol | 0.05 | 0.12 | 0.01 | 0.21 * |
| Ratio of vegetable oils to animal fat | NA | NA | NA | 0.11 * |
| Share in explaining the variance (%) | 15 | 10 | 6 | NA |
| Adherence to the Dietary Pattern | Cancer Control Sample (n = 439) | Smoking Status | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Never Smoker (n = 55) | Moderate Smoker (n = 252) | Heavy Smoker (n = 132) | ||||||||||||||
| Sample Size | Cancer Cases | p | Sample Size | Cancer Cases | p | Sample Size | Cancer Cases | p | Sample Size | Cancer Cases | p | |||||
| n | % | n | % | n | % | n | % | |||||||||
| Prudent | <0.0001 | 0.6742 | 0.0046 | 0.6541 | ||||||||||||
| lower | 146 | 81 | 55.5 | 7 | 0 | 0.0 | 90 | 51 | 56.7 | 49 | 30 | 61.2 | ||||
| moderate | 146 | 64 | 43.8 | 17 | 0 | 0.0 | 85 | 41 | 48.3 | 44 | 23 | 52.3 | ||||
| higher | 147 | 42 | 28.6 | 30 | 1 | 3.3 | 77 | 20 | 25.9 | 40 | 21 | 52.5 | ||||
| Westernized Traditional | 0.8912 | 0.4102 | 0.9861 | 0.1221 | ||||||||||||
| lower | 147 | 63 | 42.9 | 20 | 1 | 5.0 | 84 | 37 | 44.0 | 43 | 25 | 58.1 | ||||
| moderate | 146 | 64 | 43.8 | 19 | 0 | 0.0 | 82 | 37 | 45.1 | 45 | 27 | 60.0 | ||||
| higher | 146 | 60 | 41.1 | 16 | 0 | 0.0 | 86 | 38 | 44.2 | 44 | 22 | 50.0 | ||||
| Sweet Dairy | 0.4017 | 0.4101 | 0.9054 | 0.8343 | ||||||||||||
| lower | 146 | 62 | 42.5 | 17 | 0 | 0.0 | 85 | 37 | 43.5 | 44 | 25 | 56.8 | ||||
| moderate | 147 | 57 | 38.8 | 20 | 1 | 5.0 | 89 | 37 | 41.6 | 38 | 19 | 50.0 | ||||
| higher | 146 | 68 | 46.6 | 18 | 0 | 0.0 | 78 | 38 | 48.7 | 50 | 30 | 60.0 | ||||
| Polish–aMED score | <0.0001 | 0.4102 | 0.0003 | 0.8254 | ||||||||||||
| low (0–3 points) | 177 | 97 | 51.9 | 15 | 0 | 0.0 | 106 | 63 | 59.4 | 56 | 34 | 60.7 | ||||
| moderate (4–6 points) | 221 | 83 | 44.4 | 27 | 1 | 3.7 | 127 | 47 | 37.1 | 67 | 35 | 52.2 | ||||
| high (7–9 points) | 41 | 7 | 3.7 | 13 | 0 | 0.0 | 19 | 2 | 10.5 | 9 | 5 | 55.6 | ||||
| Adherence to the Dietary Pattern | Cancer-Control Sample (n = 439) | |||
|---|---|---|---|---|
| Crude Model | p | Adjusted Model | p | |
| Prudent | ||||
| lower (ref.) | Ref. | Ref. | ||
| moderate | 0.63 (0.39; 1.00) | 0.0472 | 0.63 (0.37; 1.08) | 0.1394 |
| higher | 0.57 (0.44; 0.72) | <0.0001 | 0.72 (0.53; 0.96) | 0.0432 |
| Westernized Traditional | ||||
| lower (ref.) | Ref. | Ref. | ||
| moderate | 1.04 (0.65; 1.66) | 0.8667 | 0.79 (0.45; 1.37) | 0.5123 |
| higher | 0.96 (0.76;1.22) | 0.7601 | 0.81 (0.60; 1.08) | 0.1495 |
| Sweet Dairy | ||||
| lower (ref.) | Ref. | Ref. | ||
| moderate | 0.86 (0.54; 1.37) | 0.5203 | 0.68 (0.39; 1.20) | 0.1495 |
| higher | 1.09 (0.86; 1.37) | 0.4803 | 0.99 (0.75; 1.30) | 0.7999 |
| Polish–aMED score | ||||
| low (0–3 points; ref.) | Ref. | Ref. | ||
| moderate (4–6 points) | 0.50 (0.33; 0.74) | 0.0004 | 0.51 (0.31; 0.81) | 0.0048 |
| high (7–9 points) | 0.41 (0.27; 0.64) | <0.0001 | 0.51 (0.32; 0.81) | 0.0046 |
| Adherence to the Dietary Pattern | Moderate Smoker (n = 252) | Heavy Smoker (n = 132) | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude Model | p | Adjusted Model | p | Crude Model | p | Adjusted Model | p | |
| Prudent | ||||||||
| lower (ref.) | Ref. | Ref. | Ref. | Ref. | ||||
| moderate | 0.67 (0.37; 1.21) | 0.2579 | 0.68 (0.34; 1.34) | 0.2579 | 0.80 (0.34; 1.90) | 0.6226 | 0.82 (0.30; 2.26) | 0.6958 |
| higher | 0.51 (0.37; 0.71) | < 0.0001 | 0.59 (0.39; 0.90) | 0.0154 | 0.88 (0.57; 1.37) | 0.5758 | 1.10 (0.64; 1.88) | 0.7187 |
| Westernized Traditional | ||||||||
| lower (ref.) | Ref. | Ref. | Ref. | Ref. | ||||
| moderate | 1.09 (0.59; 2.00) | 0.8320 | 0.92 (0.43; 1.96) | 0.8320 | 0.95 (0.40; 2.33) | 0.9147 | 0.79 (0.28; 2.27) | 0.6574 |
| higher | 1.03 (0.76; 1.40) | 0.8131 | 0.95 (0.65; 1.40) | 0.8131 | 0.77 (050; 1.21) | 0.2505 | 0.69 (0.40; 1.19) | 0.1495 |
| Sweet Dairy | ||||||||
| lower (ref.) | Ref. | Ref. | Ref. | Ref. | ||||
| moderate | 0.96 (0.53; 1.76) | 0.5139 | 0.78 (0.38; 1.64) | 0.5139 | 0.68 (0.27; 1.69) | 0.3944 | 0.49 (0.16; 1.46) | 0.1496 |
| higher | 1.14 (0.84;1.56) | 0.8109 | 1.05 (0.72; 1.51) | 0.8109 | 0.98 (0.64; 1.50) | 0.9244 | 0.92 (0.56; 1.50) | 0.7999 |
| Polish–aMED score | ||||||||
| low (0–3 points; ref.) | Ref. | Ref. | Ref. | Ref. | ||||
| moderate (4–6 points) | 0.40 (0.23; 0.68) | 0.0007 | 0.35 (0.18; 0.65) | 0.0010 | 0.71 (0.34; 1.46) | 0.3462 | 0.64 (0.27; 1.55) | 0.2485 |
| high (7–9 points) | 0.28 (0.13; 0.61) | 0.0010 | 0.34 (0.15; 0.76) | 0.0079 | 0.77 (0.90; 0.44) | 0.7692 | 1.17 (0.53; 2.61) | 0.3462 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawrysz, I.; Wadolowska, L.; Slowinska, M.A.; Czerwinska, A.; Golota, J.J. Adherence to Prudent and Mediterranean Dietary Patterns Is Inversely Associated with Lung Cancer in Moderate But Not Heavy Male Polish Smokers: A Case-Control Study. Nutrients 2020, 12, 3788. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123788
Hawrysz I, Wadolowska L, Slowinska MA, Czerwinska A, Golota JJ. Adherence to Prudent and Mediterranean Dietary Patterns Is Inversely Associated with Lung Cancer in Moderate But Not Heavy Male Polish Smokers: A Case-Control Study. Nutrients. 2020; 12(12):3788. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123788
Chicago/Turabian StyleHawrysz, Iwona, Lidia Wadolowska, Malgorzata Anna Slowinska, Anna Czerwinska, and Janusz Jacek Golota. 2020. "Adherence to Prudent and Mediterranean Dietary Patterns Is Inversely Associated with Lung Cancer in Moderate But Not Heavy Male Polish Smokers: A Case-Control Study" Nutrients 12, no. 12: 3788. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123788