Appetite Control Might not Be Improved after Weight Loss in Adolescents with Obesity, Despite Non-Persistent Metabolic Syndrome

 , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Population and Methods
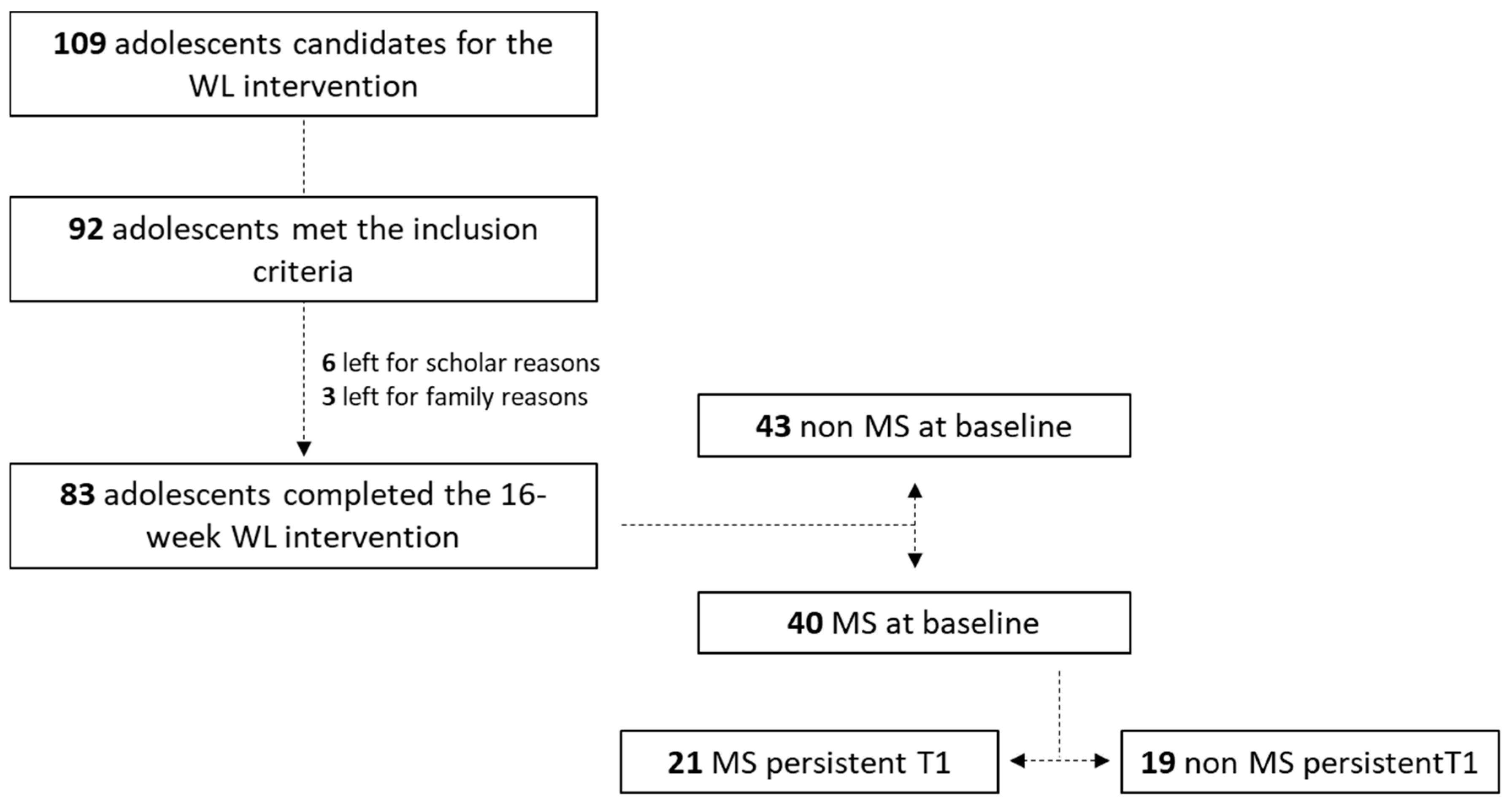
2.1. Population
2.2. Study Design
2.3. Measurements
2.3.1. Blood Pressure
2.3.2. Blood Samples
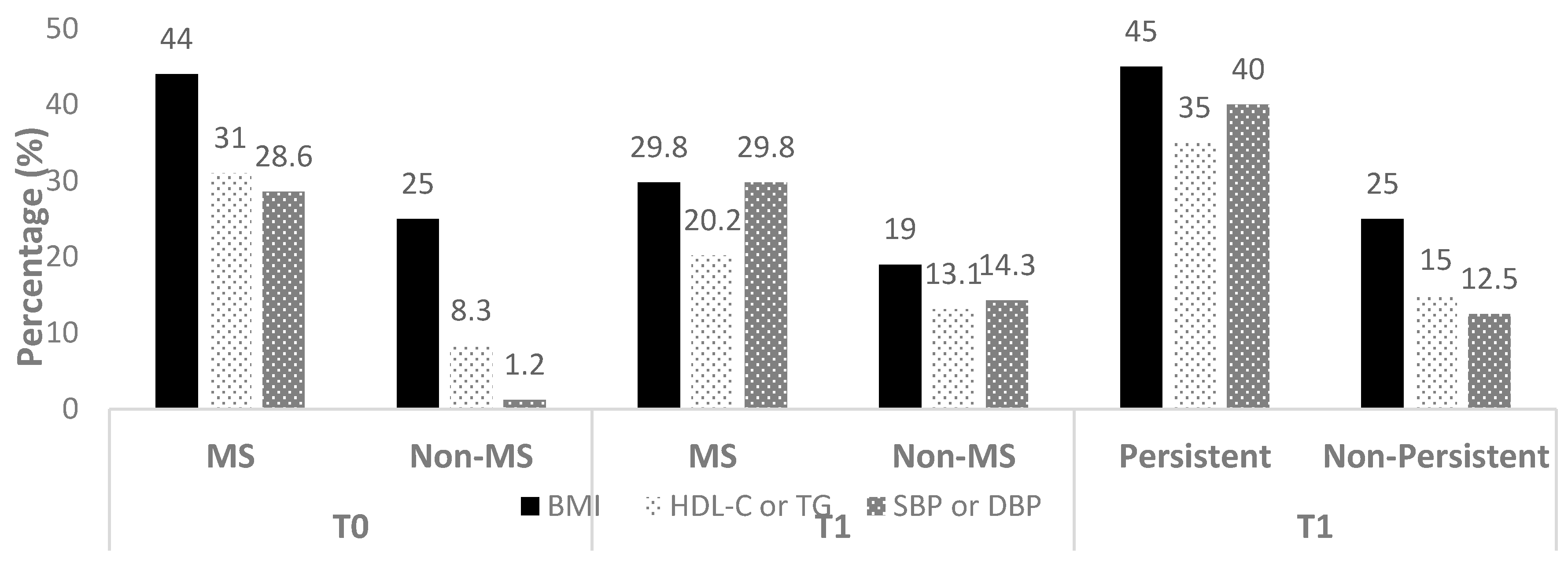
2.3.3. Detection of the Metabolic Syndrome
2.3.4. Ad libitum Energy Intake
2.3.5. Subjective Appetite Sensations
2.3.6. Multidisciplinary Weight Loss Program
2.4. Statistical Analysis
3. Results
3.1. Anthropometric Variables and Body Composition
3.2. Food Consumption and Macronutrient Intake
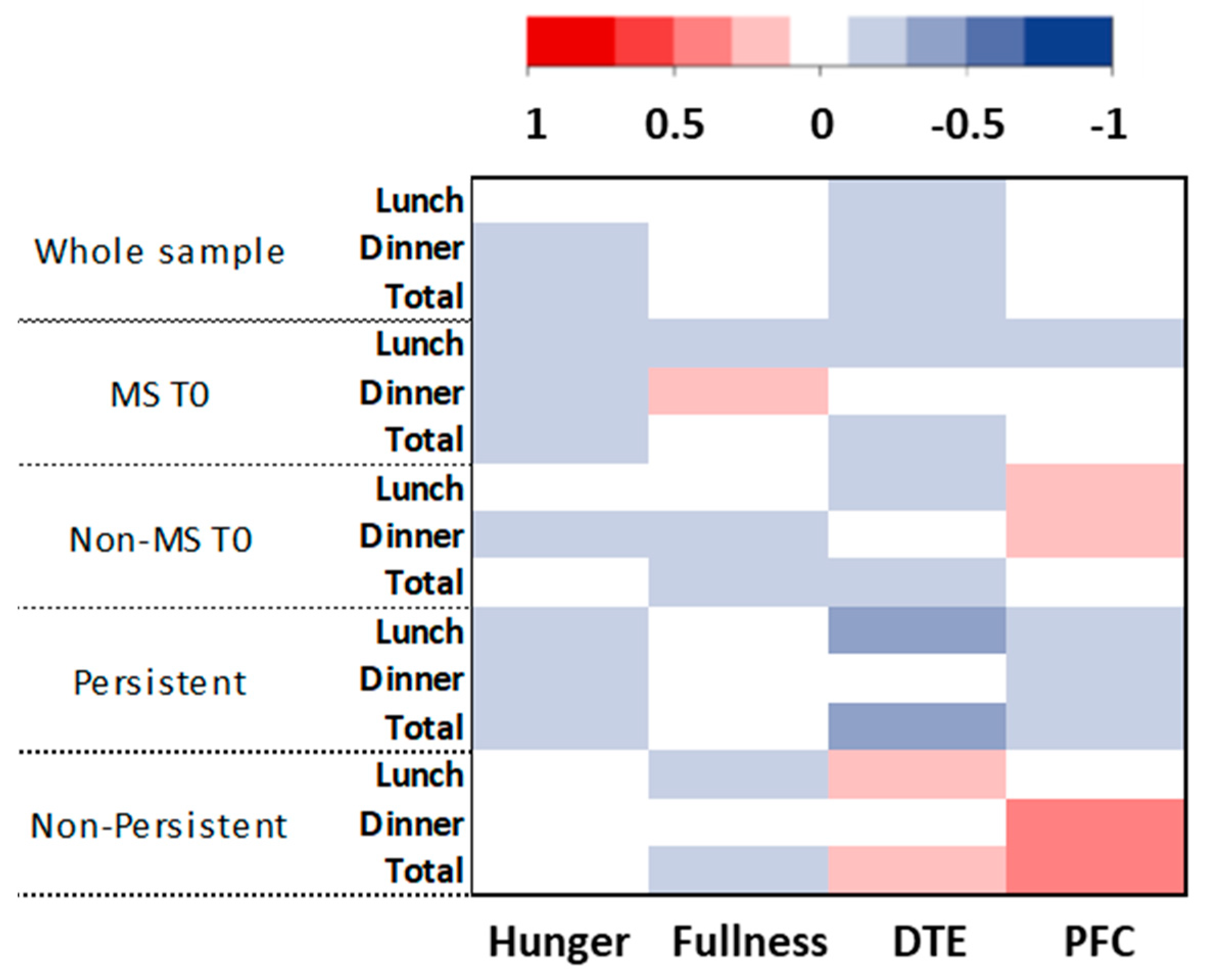
3.3. Appetite Sensations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. World Health Organization Surveillance Initiative. In Proceedings of the 9th Meeting of the WHO European Childhood Obesity Surveillance Initiative (COSI), Saint Petersburg, Russia, 10 June 2016. [Google Scholar]
- Guo, S.S.; Chumlea, W.C. Tracking of body mass index in children in relation to overweight in adulthood. Am. J. Clin. Nutr. 1999, 70, 145S–148S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lifshitz, F. Obesity in Children. J. Clin. Res. Pediatr. Endocrinol. 2011, 1, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Boff, R.D.M.; Liboni, R.P.A.; Batista, I.P.D.A.; De Souza, L.H.; Oliveira, M.D.S. Weight loss interventions for overweight and obese adolescents: A systematic review. Eat. Weight. Disord. Stud. Anorexia, Bulim. Obes. 2017, 22, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Knöpfli, B.H.; Radtke, T.; Lehmann, M.; Schätzle, B.; Eisenblätter, J.; Gachnang, A.; Wiederkehr, P.; Hammer, J.; Brooks-Wildhaber, J. Effects of a multidisciplinary inpatient intervention on body composition, aerobic fitness, and quality of life in severely obese girls and boys. J Adolesc. Health 2008, 42, 119–127. [Google Scholar] [CrossRef]
- Bianchini, J.A.A.; Da Silva, D.F.; Nardo, C.C.S.; Carolino, I.D.R.; Hernandes, F.; Junior, N.N. Multidisciplinary therapy reduces risk factors for metabolic syndrome in obese adolescents. Eur. J. Nucl. Med. Mol. Imaging 2012, 172, 215–221. [Google Scholar] [CrossRef]
- Fonvig, C.E.; Hamann, S.A.; Nielsen, T.R.H.; Johansen, M.Ø.; Grønbæk, H.N.; Mollerup, P.M.; Holm, J.-C. Subjective evaluation of psychosocial well-being in children and youths with overweight or obesity: The impact of multidisciplinary obesity treatment. Qual. Life Res. 2017, 26, 3279–3288. [Google Scholar] [CrossRef]
- Miguet, M.; Masurier, J.; Chaput, J.-P.; Pereira, B.; Lambert, C.; Dâmaso, A.R.; Courteix, D.; Duclos, M.; Boirie, Y.; Thivel, D. Cognitive restriction accentuates the increased energy intake response to a 10-month multidisciplinary weight loss program in adolescents with obesity. Appetite 2019, 134, 125–134. [Google Scholar] [CrossRef]
- Miguet, M.; Fearnbach, N.S.; Metz, L.; Khammassi, M.; Julian, V.; Cardenoux, C.; Pereira, B.; Boirie, Y.; Duclos, M.; Thivel, D. Effect of HIIT versus MICT on body composition and energy intake in dietary restrained and unrestrained adolescents with obesity. Appl. Physiol. Nutr. Metab. 2020, 45, 437–445. [Google Scholar] [CrossRef]
- Thivel, D.; Julian, V.; Miguet, M.; Pereira, B.; Beaulieu, K.; Finlayson, G.; Richard, R.; Duclos, M. Introducing eccentric cycling during a multidisciplinary weight loss intervention might prevent adolescents with obesity from increasing their food intake: The TEXTOO study. Physiol. Behav. 2020, 214, 112744. [Google Scholar] [CrossRef]
- Taetzsch, A.; Roberts, S.B.; Gilhooly, C.H.; Lichtenstein, A.H.; Krauss, A.; Bukhari, A.S.; Martin, E.; Hatch-McChesney, A.; Das, S.K. Food cravings: Associations with dietary intake and metabolic health. Appetite 2020, 152, 104711. [Google Scholar] [CrossRef]
- Mirmiran, P.; Ziadlou, M.; Karimi, S.; Hosseini-Esfahani, F.; Azizi, F. The association of dietary patterns and adherence to WHO healthy diet with metabolic syndrome in children and adolescents: Tehran lipid and glucose study. BMC Public Health 2019, 19, 1457. [Google Scholar] [CrossRef] [PubMed]
- Farr, O.M.; Mantzoros, C.S. Obese individuals with more components of the metabolic syndrome and/or prediabetes demonstrate decreased activation of reward-related brain centers in response to food cues in both the fed and fasting states: A preliminary fMRI study. Int. J. Obes. 2016, 41, 471–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthony, K.; Reed, L.J.; Dunn, J.T.; Bingham, E.; Hopkins, D.; Marsden, P.K.; Amiel, S.A. Attenuation of Insulin-Evoked Responses in Brain Networks Controlling Appetite and Reward in Insulin Resistance: The Cerebral Basis for Impaired Control of Food Intake in Metabolic Syndrome? Diabetes 2006, 55, 2986–2992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwirska-Korczala, K.; Konturek, S.J.; Sodowski, M.; Wylezol, M.S.; Kuka, D.; Sowa, P.; Adamczyk-Sowa, M.; Kukla, M.; Berdowska, A.; Rehfeld, J.F.; et al. Basal and postprandial plasma levels of PYY, ghrelin, cholecystokinin, gastrin and insulin in women with moderate and morbid obesity and metabolic syndrome. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2007, 58, 13–35. [Google Scholar]
- Mesgari-Abbasi, M. Serum Concentrations of Cholecystokinin, Peptide YY, Ghrelin and High Sensitive C-Reactive Protein in Association with Metabolic Syndrome Ingredients in Obese Individuals. Acta Endocrinol. Buchar. 2020, 16, 37–42. [Google Scholar] [CrossRef]
- Chen, M.-Y.; Wang, E.K.; Jeng, Y.-J. Adequate sleep among adolescents is positively associated with health status and health-related behaviors. BMC Public Health 2006, 6, 59. [Google Scholar] [CrossRef]
- Isacco, L.; Roche, J.; Quinart, S.; Thivel, D.; Gillet, V.; Nègre, V.; Mougin, F. Cardiometabolic risk is associated with the severity of sleep-disordered breathing in children with obesity. Physiol. Behav. 2017, 170, 62–67. [Google Scholar] [CrossRef]
- Thivel, D.; Malina, R.M.; Isacco, L.; Aucouturier, J.; Meyer, M.; Duché, P. Metabolic Syndrome in Obese Children and Adolescents: Dichotomous or Continuous? Metab. Syndr. Relat. Disord. 2009, 7, 549–556. [Google Scholar] [CrossRef]
- Pradalie, L. Alimentation et santé des lycéens et des collégiens. L’obésité chez l’enfant et l’adolescent, Comité des Yvelines d’Éducation pour la Santé 2003, 2, 2158–2168. [Google Scholar]
- Thivel, D.; Genin, P.M.; Mathieu, M.-E.; Pereira, B.; Metz, L.; David, T.; Manon, G.P.; Marie-Eve, M.; Bruno, P.; Lore, M. Reproducibility of an in-laboratory test meal to assess ad libitum energy intake in adolescents with obesity. Appetite 2016, 105, 129–133. [Google Scholar] [CrossRef]
- Flint, A.; Raben, A.; Blundell, J.E.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelalian, E.; Hart, C.N.; Mehlenbeck, R.S.; Lloyd-Richardson, E.E.; Kaplan, J.D.; Flynn-O’Brien, K.T.; Wing, R.R. Predictors of Attrition and Weight Loss in an Adolescent Weight Control Program. Obesity 2008, 16, 1318–1323. [Google Scholar] [CrossRef] [PubMed]
- Dâmaso, A.R.; De Piano, A.; Campos, R.M.D.S.; Corgosinho, F.C.; Siegfried, W.; Caranti, D.A.; Masquio, D.C.L.; Carnier, J.; Sanches, P.D.L.; Da Silva, P.L.; et al. Multidisciplinary Approach to the Treatment of Obese Adolescents: Effects on Cardiovascular Risk Factors, Inflammatory Profile, and Neuroendocrine Regulation of Energy Balance. Int. J. Endocrinol. 2013, 2013, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Masquio, D.C.L.; De Piano, A.; Sanches, P.L.; Corgosinho, F.C.; Campos, R.M.D.S.; Carnier, J.; Da Silva, P.L.; Caranti, D.A.; Tock, L.; Oyama, L.M.; et al. The effect of weight loss magnitude on pro-/anti-inflammatory adipokines and carotid intima-media thickness in obese adolescents engaged in interdisciplinary weight loss therapy. Clin. Endocrinol. 2012, 79, 55–64. [Google Scholar] [CrossRef]
- Khammassi, M.; Isacco, L.; Pereira, B.; Damaso, A.R.; Matlosz, P.; Maruszczak, K.; Weghuber, D.; Dutheil, F.; Duclos, M.; Boirie, Y.; et al. The cardiometabolic efficacy of multidisciplinary weight loss interventions is not altered in adolescents with obesity initially diagnosed or with a persistent metabolic syndrome. Nutr. Res. 2020. [Google Scholar] [CrossRef]
- Martín-García, M.; Alegre, L.M.; García-Cuartero, B.; Bryant, E.J.; Gutin, B.; Ara, I. Effects of a 3-month vigorous physical activity intervention on eating behaviors and body composition in overweight and obese boys and girls. J. Sport Health Sci. 2019, 8, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Gueugnon, C.; Mougin, F.; Nguyen, N.U.; Bouhaddi, M.; Nicolet-Guénat, M.; Dumoulin, G. Ghrelin and PYY levels in adolescents with severe obesity: Effects of weight loss induced by long-term exercise training and modified food habits. Eur. J. Appl. Physiol. 2012, 112, 1797–1805. [Google Scholar] [CrossRef]
- Roche, J.; Isacco, L.; Perret, F.; Dumoulin, G.; Gillet, V.; Mougin, F. Beneficial effects of a lifestyle intervention program on C-reactive protein: Impact of cardiorespiratory fitness in obese adolescents with sleep disturbances. Am. J. Physiol. Integr. Comp. Physiol. 2019, 316, R376–R386. [Google Scholar] [CrossRef]
- Miguet, M.; Beaulieu, K.; Fillon, A.; Khammassi, M.; Masurier, J.; Lambert, C.; Duclos, M.; Boirie, Y.; Finlayson, G.; Thivel, D. Effect of a 10-month residential multidisciplinary weight loss intervention on food reward in adolescents with obesity. Physiol. Behav. 2020, 223, 112996. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Whole Sample | MS | Non-MS | Group | Time | Interaction | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p | T0 | T1 | T0 | T1 | ||||
| Body weight (kg) | 87.1 ± 14.9 | 81.2 ± 13.0 | <0.001 | 93.3 ± 12.6 | 86.0 ± 10.6 *** | 81.4 ± 14.6 c | 76.8 ± 13.6 ***,b | <0.000 | <0.000 | 0.005 |
| BMI (kg.m−2) | 32.9 ± 4.7 | 30.4 ± 4.2 | <0.001 | 34.7 ± 3.8 | 31.8 ± 3.5 *** | 31.2 ± 4.9 c | 29.1 ± 4.5 ***,a | <0.000 | <0.000 | 0.026 |
| z-BMI | 1.9 ± 0.4 | 1.7 ± 0.5 | <0.001 | 2.2 ± 0.3 | 1.9 ± 0.3 *** | 1.7 ± 0.4 c | 1.5 ± 0.5 ***,c | <0.000 | <0.000 | 0.871 |
| BMI percentile | 96.2 ± 4.2 | 93.8 ± 8.4 | <0.001 | 98.1 ± 2.1 | 96.7 ± 3.2 *** | 94.6 ± 5.0 | 91.1 ± 10.6 c | <0.000 | <0.000 | 0.031 |
| FM% | 38.1 ± 3.8 | 33.8 ± 4.7 | <0.001 | 38.3 ± 3.7 | 33.3 ± 4.4 *** | 38.0 ± 3.9 | 34.3 ± 5.1 *** | 0.658 | <0.000 | 0.021 |
| FFM (kg) | 51.8 ± 8.0 | 52.1 ± 7.8 | 0.16 | 55.5 ± 7.3 | 55.6 ± 7.1 | 48.5 ± 7.2 c | 48.9 ± 7.2 c | <0.000 | 0.165 | 0.528 |
| Persistent T1 | Non-Persistent T1 | p | Non-MS T0 | Non-Persistent T1 | p | |
|---|---|---|---|---|---|---|
| Body weight (kg) | 88.5 ± 10.3 | 83.2 ± 10.5 | 0.116 | 81.4 ± 14.6 | 83.2 ± 10.5 | 0.628 |
| BMI (kg.m−2) | 33.1 ± 3.5 | 30.3 ± 3.3 | 0.011 | 31.2 ± 4.8 | 30.3 ± 3.3 | 0.454 |
| z-BMI | 2.0 ± 1.8 | 1.8 ± 0.3 | 0.024 | 1.7 ± 0.4 | 1.8 ± 0.3 | 0.720 |
| BMI percentile | 97.6 ± 1.4 | 95.7 ± 4.3 | 0.076 | 94.6 ± 5.0 | 95.7 ± 4.3 | 0.430 |
| FM% | 34.0 ± 4.4 | 32.5 ± 4.2 | 0.273 | 38.0 ± 3.9 | 32.5 ± 4.2 | 0.000 |
| FFM (kg) | 56.5 ± 6.8 | 54.6 ± 7.4 | 0.386 | 48.5 ± 7.2 | 54.6 ± 7.4 | 0.003 |
| Whole Sample | MS | Non-MS | Group | Time | Interaction | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p | T0 | T1 | T0 | T1 | ||||
| Lunch (kcal) | 1000 ± 349 | 1085 ± 415 | 0.03 | 1125 ± 335 | 1222 ± 397 | 885 ± 325 | 964 ± 396 b | <0.000 | 0.027 | 0.473 |
| Diner (kcal) | 892 ± 286 | 891 ± 229 | 0.9 | 938 ± 312 | 893 ± 207 | 850 ± 256 | 890 ± 249 | 0.403 | 0.95 | 0.19 |
| Total ad libitum (kcal) | 1893 ± 548 | 1977 ± 523 | 0.07 | 2063 ± 557 | 2116 ± 502 | 1735 ± 496 | 1854 ± 516 | 0.005 | 0.081 | 0.842 |
| Protein Lunch (g) | 49 ± 18 | 54 ± 22 | 0.004 | 57 ± 17 | 63 ± 18 b | 42 ± 16 b | 47 ± 21 | <0.000 | 0.004 | 0.724 |
| Fat lunch (g) | 27 ± 17 | 29 ± 19 | 0.04 | 35 ± 16 | 37 ± 17 | 19 ± 13 c | 22 ± 18 c | <0.000 | 0.042 | 0.934 |
| CHO lunch (g) | 137 ± 55 | 147 ± 73 | 0.18 | 143 ± 54 | 154 ± 78 | 131 ± 56 | 141 ± 68 | 0.242 | 0.174 | 0.52 |
| Protein dinner (g) | 54 ± 24 | 54 ± 24 | 0.71 | 55 ± 25 | 52 ± 19 | 53 ± 24 | 57 ± 27 | 0.848 | 0.758 | 0.097 |
| Fat dinner (g) | 28 ± 15 | 27 ± 12 | 0.78 | 32 ± 17 | 30 ± 13 | 26 ± 13 | 25 ± 11 | 0.074 | 0.768 | 0.742 |
| CHO dinner (g) | 105 ± 34 | 105 ± 29 | 0.87 | 107 ± 37 | 103 ± 25 | 104 ± 30 | 107 ± 32 | 0.979 | 0.835 | 0.329 |
| Total Protein (g) | 104 ± 32 | 109 ± 33 | 0.03 | 113 ± 33 | 115 ± 30 | 95 ± 28 | 104 ± 34 | 0.030 | 0.032 | 0.393 |
| Total Fat (g) | 56 ± 27 | 57 ± 25 | 0.26 | 67 ± 28 | 67 ± 23 | 45 ± 21 | 47 ± 22 | <0.000 | 0.271 | 0.773 |
| Total CHO (g) | 242 ± 76 | 253 ± 87 | 0.29 | 250 ± 75 | 258 ± 89 | 235 ± 76 | 248 ± 86 | 0.376 | 0.292 | 0.934 |
| Protein Lunch (%) | 19.6 ± 3.8 | 20.3 ± 4.2 | 0.06 | 20.5 ± 3.4 | 20.8 ± 3.0 | 18.8 ± 3.9 | 19.8 ± 5.0 | 0.102 | 0.060 | 0.28 |
| Fat lunch (%) | 23.1 ± 11.4 | 23.4 ± 11.2 | 0.55 | 27.8 ± 10.8 | 27.6 ± 9.8 | 18.7 ± 10.3 b | 19.6 ± 11.1 b | <0.000 | 0.561 | 0.377 |
| CHO lunch (%) | 55.5 ± 14.4 | 55.2 ± 14.3 | 0.54 | 51.6 ± 12.7 | 50.5 ± 12.2 | 59.3 ± 14.7 | 59.5 ± 14.8 a | 0.008 | 0.600 | 0.527 |
| Protein dinner (%) | 24.6 ± 9.5 | 24.2 ± 7.3 | 0.51 | 23.7 ± 7.8 | 23.5 ± 7.1 | 25.6 ± 10.7 | 24.8 ± 7.5 | 0.394 | 0.583 | 0.678 |
| Fat dinner (%) | 30.7 ± 23.1 | 28.2 ± 10.6 | 0.36 | 30.4 ± 10.7 | 30.0 ± 9.6 | 31.5 ± 30.7 | 26.6 ± 11.2 | 0.781 | 0.428 | 0.393 |
| CHO dinner (%) | 49.6 ± 24.3 | 47.6 ± 8.2 | 0.31 | 46.1 ± 10.0 | 46.6 ± 6.7 | 53.4 ± 32.0 | 48.4 ± 9.2 | 0.201 | 0.376 | 0.388 |
| Total Protein (%) | 22.1 ± 3.6 | 22.2 ± 3.3 | 0.68 | 22.0 ± 3.3 | 21.8 ± 2.7 | 22.1 ± 4.0 | 22.5 ± 3.7 | 0.516 | 0.714 | 0.355 |
| Total Fat (%) | 26.2 ± 8.8 | 26.1 ± 8.8 | 0.63 | 29.1 ± 8.4 | 29.1 ± 7.8 *** | 23.5 ± 8.2 | 23.4 ± 8.8 ***,c | 0.003 | 0.636 | 0.973 |
| Total CHO (%) | 51.9 ± 9.4 | 51.1 ± 9.2 | 0.18 | 48.9 ± 8.4 | 48.5 ± 8.1 *** | 54.6 ± 9.5 | 53.4 ± 9.5 *** | 0.626 | <0.000 | 0.274 |
| Persistent T1 | Non-Persistent T1 | p | Non-MS T0 | Non-Persistent T1 | p | |
|---|---|---|---|---|---|---|
| Lunch (kcal) | 1229 ± 84 | 1214 ± 98 | 0.907 | 885 ± 325 | 1214 ± 98 | 0.0061 |
| Diner (kcal) | 891 ± 49 | 895 ± 45 | 0.952 | 850 ± 256 | 895 ± 45 | 0.4535 |
| Total ad libitum (kcal) | 2121 ± 111 | 2110 ± 119 | 0.946 | 1735 ± 496 | 2110 ± 119 | 0.0122 |
| Protein Lunch (g) | 62 ± 3 | 63 ± 5 | 0.895 | 42 ± 16 | 63 ± 5 | 0.0014 |
| Fat lunch (g) | 37 ± 3 | 37 ± 5 | 0.921 | 19 ± 13 | 37 ± 5 | 0.0025 |
| CHO lunch (g) | 157 ± 17 | 151 ± 18 | 0.821 | 131 ± 56 | 151 ± 18 | 0.3163 |
| Protein dinner (g) | 50 ± 4 | 54 ± 5 | 0.508 | 53 ± 24 | 54 ± 5 | 0.7597 |
| Fat dinner (g) | 30 ± 3 | 30 ± 2 | 0.961 | 26 ± 13 | 30 ± 2 | 0.2442 |
| CHO dinner (g) | 104 ± 5 | 101 ± 6 | 0.692 | 104 ± 30 | 101 ± 6 | 0.7315 |
| Total Protein (g) | 113 ± 28 | 118 ± 33 | 0.612 | 95 ± 28 | 118 ± 33 | 0.0163 |
| Total Fat (g) | 67 ± 21 | 67 ± 25 | 0.96 | 45 ± 21 | 67 ± 25 | 0.0028 |
| Total CHO (g) | 262 ± 19 | 253 ± 21 | 0.756 | 235 ± 76 | 253 ± 21 | 0.4697 |
| Protein Lunch (%) | 20.8 ± 0.5 | 21.0 ± 0.8 | 0.826 | 18.8 ± 3.9 | 21.0 ± 0.8 | 0.0458 |
| Fat lunch (%) | 27.7 ± 1.7 | 27.5 ± 2.8 | 0.953 | 18.7 ± 10.3 | 27.5 ± 2.8 | 0.011 |
| CHO lunch (%) | 50.5 ± 2.1 | 50.5 ± 3.5 | 0.997 | 59.3 ± 14.7 | 50.5 ± 3.5 | 0.0441 |
| Protein dinner (%) | 22.7 ± 1.4 | 24.6 ± 1.8 | 0.43 | 25.6 ± 10.7 | 24.6 ± 1.8 | 0.6694 |
| Fat dinner (%) | 29.8 ± 2.0 | 30.2 ± 2.4 | 0.886 | 31.5 ± 30.7 | 30.2 ± 2.4 | 0.8134 |
| CHO dinner (%) | 47.8 ± 1.5 | 45.3 ± 1.6 | 0.252 | 53.4 ± 32.0 | 45.3 ± 1.6 | 0.1221 |
| Total Protein (%) | 21.4 ± 0.5 | 22.3 ± 0.7 | 0.306 | 22.1 ± 4.0 | 22.3 ± 0.7 | 0.8523 |
| Total Fat (%) | 28.9 ± 1.4 | 29.3 ± 2.2 | 0.865 | 23.5 ± 8.2 | 29.3 ± 2.2 | 0.0281 |
| Total CHO (%) | 49.2 ± 1.5 | 47.8 ± 2.2 | 0.604 | 54.6 ± 9.5 | 47.8 ± 2.2 | 0.0149 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Julian, V.; Isacco, L.; Khammassi, M.; Fillon, A.; Miguet, M.; Dutheil, F.; Courteix, D.; Zak, M.; Bicki, J.; Głuszek, S.; et al. Appetite Control Might not Be Improved after Weight Loss in Adolescents with Obesity, Despite Non-Persistent Metabolic Syndrome. Nutrients 2020, 12, 3885. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123885
Julian V, Isacco L, Khammassi M, Fillon A, Miguet M, Dutheil F, Courteix D, Zak M, Bicki J, Głuszek S, et al. Appetite Control Might not Be Improved after Weight Loss in Adolescents with Obesity, Despite Non-Persistent Metabolic Syndrome. Nutrients. 2020; 12(12):3885. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123885
Chicago/Turabian StyleJulian, Valérie, Laurie Isacco, Marwa Khammassi, Alicia Fillon, Maud Miguet, Frederic Dutheil, Daniel Courteix, Marek Zak, Jacek Bicki, Stanisław Głuszek, and et al. 2020. "Appetite Control Might not Be Improved after Weight Loss in Adolescents with Obesity, Despite Non-Persistent Metabolic Syndrome" Nutrients 12, no. 12: 3885. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12123885