Oral Supplementation with Sucrosomial Ferric Pyrophosphate Plus L-Ascorbic Acid to Ameliorate the Martial Status: A Randomized Controlled Trial

 ,
,  ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
Martial Status in Orthopedic Surgery
2. Materials and Methods
2.1. Study Design and Participants
2.2. Intervention and Biochemical Analyses
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Dietary Supplement

Appendix B

{kind=link}
{kind=link}
| Marker | Description | Ref. val. | Significance |
|---|---|---|---|
 Hb | Assembly of four globular polypeptide chain, with each one being associated with a prosthetic heme group that contains an atom of iron either in the ferrous or in the ferric state. The four oxidized ion atoms in Hb carry four oxygen molecules. | ♂ [13.7–17.5 g/dL] ♀ [11.2–15.7 g/dL] | Hb concentration in blood is a measure for anemia. Low serum values reflect low functional iron when there are no concurrent infective/inflammatory disorders or other micronutrient deficits, such as vitamin A or B group. |
 RBCs | Anucleated biconcave disks with an aphospholipid bilayer. They lack most organelles and appear with a central pallor and surrounding warp filled with Hb. The deformable shape allows the traversing of the smallest capillaries. | ♂ [4.63–6.08 106/μL] ♀ [3.93–5.22 106/μL] | They reflect the intensity of erythropoiesis when there are no concurrent B vitamin deficiencies, or diseases of kidneys, liver, and thyroid. Low RBCs can mirror an iron depletion. |
 MCV | Average size/volume of a red blood cell. Calculated as the ratio of hematocrit, which measures the volume percentage of RBCs, to RBCs concentration. The higher the MCV the greater the average size/volume of erythrocytes. | ♂ [79.0–92.2 fL/cell] ♀ [79.4–94.8 fL/cell] | Indicative of a correct erythropoiesis. When bone marrow lacks a proper iron supply, MCV is low and RBCs are microcytic. A deficiency of cobalamin or folate results in higher MCV, which is a condition named macrocytic anemia. |
 MCH | Indirect index calculated as the ratio of Hb to RBCs. Haemoglobin molecules in erythrocytes are located in the periphery and surround a central pallor. The more extensive the central pallor the lesser Hb is contained (left erythrocyte). | ♂ [25.7–32.2 pg/cell] ♀ [25.6–32.2 pg/cell] | MCH value closely parallels the value of MCV. Defects in nuclear maturation, such as in megaloblastic anemia, result in high values of MCH. |
 MCHC | Indirect index calculated as the ratio of Hb to the volume percentage of RBCs. The value of MCHC is increased in spherocytosis as erythrocyte assume a spherical shape because of the loss of membrane (erythrocyte on the right). | ♂ [32.3–36.5 g/dL] ♀ [32.2–35.5 g/dL] | It correlates Hb with RBCs volume. Low values can reflect micronutrient deficiencies. When no genetic disease or hemolysis is present, high values are mostly artefact (lipemia), because RBCs cannot contain more Hb than normal. |
 Iron | The amount of the metal that is circulating in blood, primarily bound to proteins, such as Tf and ferritin. A slightest part is non-transferrin bound iron (NTBI) and has capacity to generate highly reactive free radicals. | ♂ [31–144 μg/dL] ♀ [25–156 μg/dL] | The highest serum levels can result from intravenous iron or genetic diseases, whereas lowest concentrations can be found in anemias for inflammation or chronic diseases. |
 Tf | A single polypeptide chain and two carbohydrate chains forms Tf. When no iron is bound, the protein is called apotransferrin. Tf binds a maximum of two atoms of ferric iron for its solubilisation and reactiveness reduction. | ♂ [163–344 mg/dL] ♀ [180–382 mg/dL] | It transports iron and reflects, similarly to its receptors on RBCS, the demand of iron. If there are no other reasons for abnormal erythropoiesis, its serum levels increase when iron stores are exhausting. It is a negative acute-phase protein. |
| Tf saturation | The binding sites on all Tf molecules occupied with iron. It is calculated as the ratio of serum iron to Tf or serum iron to total iron binding capacity (TIBC), the latter being the total amount of blood iron that can be bound by proteins. | ♂ [20–50%] ♀ [15–50%] | It provides information, similarly to Tf, about the adequacy of iron supply to meet cellular requirements. High degrees of saturation identify patients at risk of iron overload. |
 Ferritin | A 24-units globular protein with both light and the heavy chains that takes up to 4300 iron atoms to be deposited in its core of few nm. The form of iron deposit consists of crystals of ferric hydroxides and phosphates. | ♂ [22–275 ng/mL] ♀ [5–204 ng/mL] | Its serum levels represent a small fraction of the body’s ferritin pool. Low serum values reflect a depletion of iron stores when there are no concurrent infections or vitamin C deficits. It is a positive acute-phase protein. |
References
- World Health Organisation (WHO). Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Pfeiffer, C.M.; Looker, A.C. Laboratory methodologies for indicators of iron status: Strengths, limitations, and analytical challenges. Am. J. Clin. Nutr. 2017, 106, 1606S–1614S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jans, Ø.; Nielsen, C.S.; Khan, N.; Gromov, K.; Troelsen, A.; Husted, H. Iron deficiency and preoperative anaemia in patients scheduled for elective hip- and knee arthroplasty - an observational study. Vox Sang. 2018, 113, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, M.; Gómez-Ramírez, S.; Campos, A.; Ruiz, J.; Liumbruno, G.M. Pre-operative anaemia: Prevalence, consequences and approaches to management. High Speed Blood Transfus. Equip. 2015, 13, 370–379. [Google Scholar]
- Kapadia, B.H.; Banerjee, S.; Issa, K.; McElroy, M.J.; Harwin, S.F.; Mont, M.A. Preoperative Blood Management Strategies for Total Knee Arthroplasty. J. Knee Surg. 2013, 26, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Pitter, F.T.; Jorgensen, C.C.; Lindberg-Larsen, M.; Kehlet, H. Postoperative Morbidity and Discharge Destinations After Fast-Track Hip and Knee Arthroplasty in Patients Older Than 85 Years. Anesth. Analg. 2016, 122, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Yombi, J.C.; Putineanu, D.C.; Cornu, O.; Lavand’Homme, P.; Cornette, P.; Castanares-Zapatero, D. Low haemoglobin at admission is associated with mortality after hip fractures in elderly patients. Bone Jt. J. 2019, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Gherini, S.; Vaughn, B.K.; Lombardi, A.V.; Mallory, T.H. Delayed Wound Healing and Nutritional Deficiencies After Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 1993, 293, 188. [Google Scholar] [CrossRef]
- Briguglio, M.; Gianola, S.; Aguirre, M.-F.I.; Sirtori, P.; Perazzo, P.; Pennestri, F.; Brayda-Bruno, M.; Sansone, V.; Banfi, G. Nutritional support for enhanced recovery programs in orthopedics: Future perspectives for implementing clinical practice. Nutr. Clin. Métabolisme 2019, 33, 190–198. [Google Scholar] [CrossRef]
- A Hallquist, N.; McNeil, L.K.; Lockwood, J.F.; Sherman, A.R. Maternal-iron-deficiency effects on peritoneal macrophage and peritoneal natural-killer-cell cytotoxicity in rat pups. Am. J. Clin. Nutr. 1992, 55, 741–746. [Google Scholar] [CrossRef]
- Britigan, B.E.; Ratcliffe, H.R.; Buettner, G.R.; Rosen, G.M. Binding of myeloperoxidase to bacteria: Effect on hydroxyl radical formation and susceptibility to oxidant-mediated killing. Biochim. et Biophys. Acta (BBA) Gen. Subj. 1996, 1290, 231–240. [Google Scholar] [CrossRef]
- Kuvibidila, S.R.; Kitchens, D.; Baliga, B.S. In vivo and in vitro iron deficiency reduces protein kinase C activity and translocation in murine splenic and purified T cells. J. Cell. Biochem. 1999, 74, 74. [Google Scholar] [CrossRef]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–580S. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhabyeyev, P.; Wang, S.; Oudit, G.Y. Role of iron metabolism in heart failure: From iron deficiency to iron overload. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2019, 1865, 1925–1937. [Google Scholar] [CrossRef] [PubMed]
- Biccard, B.M.; Rodseth, R.N. The pathophysiology of peri-operative myocardial infarction. Anaesthesia 2010, 65, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Karcz, M.; Papadakos, P.J. Respiratory complications in the postanesthesia care unit: A review of pathophysiological mechanisms. Can. J. Respir. Ther. 2013, 49, 21–29. [Google Scholar] [PubMed]
- Kansagra, A.; Krushell, R.; Lehman, A.; Greenbaum, J.; Visintainer, P.; McGirr, J.; Mahoney, K.; Cloutier, D.; Ehresman, A.; Andrzejewski, C.; et al. Blood Management Strategies to Reduce Transfusions After Elective Lower-Extremity Joint Arthroplasty Surgeries: One Tertiary Care Hospital’s Early Experience with an Alternative Payment Model-a Total Joint “Bundle”. Am. J. Med Qual. 2017, 32, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, M.; Gómez-Ramírez, S.; Kozek-Langeneker, S.; Shander, A.; Richards, T.; Pavía, J.; Kehlet, H.; Acheson, A.G.; Evans, C.; Raobaikady, R.; et al. ‘Fit to fly’: Overcoming barriers to preoperative haemoglobin optimization in surgical patients. Br. J. Anaesth. 2015, 115, 15–24. [Google Scholar]
- Baldini, G.; Fawcett, W.J. Anesthesia for Colorectal Surgery. Anesthesiol. Clin. 2015, 33, 93–123. [Google Scholar] [CrossRef]
- Goodnough, L.T.; Maniatis, A.; Earnshaw, P.; Benoni, G.; Beris, P.; Bisbe, E.; Fergusson, D.A.; Gombotz, H.; Habler, O.; Monk, T.G.; et al. Detection, evaluation, and management of preoperative anaemia in the elective orthopaedic surgical patient: NATA guidelines. Br. J. Anaesth. 2011, 106, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Munoz, M.; Acheson, A.G.; Auerbach, M.; Besser, M.; Habler, O.; Kehlet, H.; Liumbruno, G.M.; Lasocki, S.; Meybohm, P.; Rao Baikady, R.; et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017, 72, 233–247. [Google Scholar] [CrossRef] [Green Version]
- Kopanidis, P.; Hardidge, A.; McNicol, L.; Tay, S.; McCall, P.; Weinberg, L. Perioperative blood management programme reduces the use of allogenic blood transfusion in patients undergoing total hip and knee arthroplasty. J. Orthop. Surg. Res. 2016, 11, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Iorio, R. The 5 Clinical Pillars of Value for Total Joint Arthroplasty in a Bundled Payment Paradigm. J. Arthroplast. 2017, 32, 1712–1716. [Google Scholar] [CrossRef] [PubMed]
- Andrews, C.M.; Lane, D.W.; Bradley, J.G. Iron pre-load for major joint replacement. Transfus. Med. 1997, 7, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Scardino, M.; Di Matteo, B.; Martorelli, F.; Tanzi, D.; Kon, E.; D’Amato, T. Improved patient blood management and cost saving in hip replacement surgery through the implementation of pre-operative Sucrosomial(R) iron supplementation: A quality improvement assessment study. Anaesthesia 2018, 73, 1418–1431. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, R.; Toblli, J.E.; Romero, J.D.; Monterrosa, B.; Frer, C.; Macagno, E.; Breymann, C. Efficacy and safety of oral iron(III) polymaltose complex versus ferrous sulfate in pregnant women with iron-deficiency anemia: A multicenter, randomized, controlled study. J. Matern. Neonatal Med. 2011, 24, 1347–1352. [Google Scholar] [CrossRef]
- Asperti, M.; Gryzik, M.; Brilli, E.; Castagna, A.; Corbella, M.; Gottardo, R.; Girelli, D.; Tarantino, G.; Arosio., P. Sucrosomial((R)) Iron Supplementation in Mice: Effects on Blood Parameters, Hepcidin, and Inflammation. Nutrients 2018, 10, 1349. [Google Scholar] [CrossRef] [Green Version]
- Tobias, J.D. Preoperative anesthesia evaluation. Semin. Pediatr. Surg. 2018, 27, 67–74. [Google Scholar] [CrossRef]
- Briguglio, M.; Gianturco, L.; Stella, D.; Colombo, C.; Bonadies, M.; Sala, O.; Anselmi, M.; Banfi, G.; Turiel, M. Correction of hypovitaminosis D improved global longitudinal strain earlier than left ventricular ejection fraction in cardiovascular older adults after orthopaedic surgery. J. Geriatr. Cardiol. 2018, 15, 519–522. [Google Scholar]
- Lasocki, S.; Krauspe, R.; von Heymann, C.; Mezzacasa, A.; Chainey, S.; Spahn, D.R. PREPARE: The prevalence of perioperative anaemia and need for patient blood management in elective orthopaedic surgery: A multicentre, observational study. Eur. J. Anaesthesiol. 2015, 32, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Minnella, E.M.; Awasthi, R.; Gillis, C.; Fiore, J.F.; Liberman, A.S.; Charlebois, P.; Stein, B.; Bousquet-Dion, G.; Feldman, L.S.; Carli, F. Patients with poor baseline walking capacity are most likely to improve their functional status with multimodal prehabilitation. Surgery 2016, 160, 1070–1079. [Google Scholar] [CrossRef]
- Handelman, G.J.; Levin, N.W. Iron and anemia in human biology: A review of mechanisms. Hear. Fail. Rev. 2008, 13, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. Methods to assess iron and iodine status. Br. J. Nutr. 2008, 99, S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Nordin, T.; Jecmenica, M.; Lalosevic, M.S.; Milosavljevic, T.; Milovanovic, T. Gastrointestinal Tract Disorders in Older Age. Can. J. Gastroenterol. Hepatol. 2019, 2019, 6757524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chasteen, N.; Harrison, P.M. Mineralization in Ferritin: An Efficient Means of Iron Storage. J. Struct. Boil. 1999, 126, 182–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lönnerdal, B. Calcium and Iron Absorption - Mechanisms and Public Health Relevance. Int. J. Vitam. Nutr. Res. 2010, 80, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Da Silveira, V.C.; De Oliveira, A.P.; Sperotto, R.A.; Espindola, L.S.; Dias, J.F.; Da Cunha, J.B.; Amaral, L.; Fett, J.P.; Iv, I. Influence of iron on mineral status of two rice (Oryza sativa L.) cultivars. Braz. J. Plant Physiol. 2007, 19, 127–139. [Google Scholar] [CrossRef]
- Moretti, D.; Zimmermann, M.B.; Wegmüller, R.; Walczyk, T.; Zeder, C.; Hurrell, R.F. Iron status and food matrix strongly affect the relative bioavailability of ferric pyrophosphate in humans. Am. J. Clin. Nutr. 2006, 83, 632–638. [Google Scholar] [CrossRef] [Green Version]
- WHO; FAO. Vitamin and Mineral Requirements in Human Nutrition; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Nutrition ISoH. LARN—Livelli di Assunzione di Riferimento di Nutrienti ed Energia per la Popolazione Italiana, 4th ed.; SICS Editore Srl: Rome, Italy, 2014; pp. 482–502. [Google Scholar]
- Teucher, B.; Olivares, M.; Cori, H. Enhancers of Iron Absorption: Ascorbic Acid and other Organic Acids. Int. J. Vitam. Nutr. Res. 2004, 74, 403–419. [Google Scholar] [CrossRef]
- Conrad, M.E.; Umbreit, J.N. A concise review: Iron absorption—The mucin-mobilferrin-integrin pathway. A competitive pathway for metal absorption. Am. J. Hematol. 1993, 42, 67–73. [Google Scholar] [CrossRef]
- Wang, S.; Geraci, G.; Kuhlmann, M.K.; Levin, N.W.; Handelman, G.J. Chemical reactions of vitamin C with intravenous-iron formulations. Nephrol. Dial. Transplant. 2008, 23, 120–125. [Google Scholar]
- Jain, R.; Venkatasubramanian, P. Sugarcane Molasses—A Potential Dietary Supplement in the Management of Iron Deficiency Anemia. J. Diet. Suppl. 2017, 14, 589–598. [Google Scholar] [CrossRef] [PubMed]
- García-Casal, M.N.; Layrisse, M.; Solano, L.; A Barón, M.; Arguello, F.; Llovera, D.; Ramírez, J.; Leets, I.; Tropper, E. Vitamin A and beta-carotene can improve nonheme iron absorption from rice, wheat and corn by humans. J. Nutr. 1998, 128, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briguglio, M.; Dell’Osso, B.; Panzica, G.; Malgaroli, A.; Banfi, G.; Dina, C.Z.; Galentino, R.; Porta, M. Dietary Neurotransmitters: A Narrative Review on Current Knowledge. Nutrients 2018, 10, 591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briguglio, M.; Dell’Osso, B.; Galentino, R.; Dina, C.Z.; Banfi, G.; Porta, M. Tics and obsessive-compulsive disorder in relation to diet: Two case reports. L’Encéphale 2018, 44, 479–481. [Google Scholar] [CrossRef] [PubMed]
- Camaschella, C. Iron-Deficiency Anemia. N. Engl. J. Med. 2015, 373, 485–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz, M.; Gomez-Ramirez, S.; Bhandari, S. The safety of available treatment options for iron-deficiency anemia. Expert. Opin. Drug Saf. 2018, 17, 149–159. [Google Scholar]
- Briguglio, M.; Hrelia, S.; Malaguti, M.; Serpe, L.; Canaparo, R.; Dell’Osso, B.; Galentino, R.; De Michele, S.; Dina, C.Z.; Porta, M.; et al. Food Bioactive Compounds and Their Interference in Drug Pharmacokinetic/Pharmacodynamic Profiles. Pharmaceutics 2018, 10, 277. [Google Scholar] [CrossRef] [Green Version]
- Tolkien, Z.; Stecher, L.; Mander, A.P.; Pereira, D.I.A.; Powell, J.J. Ferrous Sulfate Supplementation Causes Significant Gastrointestinal Side-Effects in Adults: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0117383. [Google Scholar] [CrossRef] [Green Version]
- Cancelo-Hidalgo, M.J.; Castelo-Branco, C.; Palacios, S.; Haya-Palazuelos, J.; Ciria-Recasens, M.; Manasanch, J.; Pérez-Edo, L. Tolerability of different oral iron supplements: A systematic review. Curr. Med Res. Opin. 2013, 29, 291–303. [Google Scholar] [CrossRef]
- Briguglio, M.; Dell’Osso, B.; Galentino, R.; Banfi, G.; Porta, M. Higher adherence to the Mediterranean diet is associated with reduced tics and obsessive-compulsive symptoms: A series of nine boys with Obsessive-Compulsive Tic Disorder. Nutrition Clinique et Métabolisme 2019, 33, 227–230. [Google Scholar] [CrossRef]
- Cinnella, G.; Pavesi, M.; De Gasperi, A.; Ranucci, M.; Mirabella, L. Clinical standards for patient blood management and perioperative hemostasis and coagulation management. Position Paper of the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care (SIAARTI). Minerva Anestesiol. 2019, 85, 635–664. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, M.; Deloughery, T. Single-dose intravenous iron for iron deficiency: A new paradigm. Hematol. Am. Soc. Hematol. Educ. Program. 2016, 2016, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assessing the IRON Status of Populations: Including Literature Reviews; Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level; 6–8 April 2004; WHO: Geneva, Switzerland, 2007.
- Graves, A.; Yates, P.; O Hofmann, A.; Farmer, S.; Ferrari, P. Predictors of perioperative blood transfusions in patients with chronic kidney disease undergoing elective knee and hip arthroplasty. Nephrology 2014, 19, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, N.U.; I Cercamondi, C.; Brittenham, G.; Zeder, C.; Geurts-Moespot, A.J.; Swinkels, D.W.; Moretti, D.; Zimmermann, M.B. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: Two open-label, randomised controlled trials. Lancet Haematol. 2017, 4, e524–e533. [Google Scholar] [CrossRef]
- Rimon, E.; Kagansky, N.; Kagansky, M.; Mechnick, L.; Mashiah, T.; Namir, M.; Levy, S. Are we giving too much iron? Low-dose iron therapy is effective in octogenarians. Am. J. Med. 2005, 118, 1142–1147. [Google Scholar] [CrossRef]
- The National Heart L, and Blood Institute (NHLBI). Iron-Deficiency Anemia. Available online: https://www.nhlbi.nih.gov/health-topics/iron-deficiency-anemia (accessed on 24 December 2019).
- Briguglio, M.; Vitale, J.A.; Galentino, R.; Banfi, G.; Dina, C.Z.; Bona, A.; Panzica, G.; Porta, M.; Dell’Osso, B.; Glick, I.D. Healthy Eating, Physical Activity, and Sleep Hygiene (HEPAS) as the Winning Triad for Sustaining Physical and Mental Health in Patients at Risk for or with Neuropsychiatric Disorders: Considerations for Clinical Practice. Neuropsychiatr. Dis. Treat. 2020, 16, 55–70. [Google Scholar] [CrossRef] [Green Version]
- Melcrová, A.; Pokorna, S.; Pullanchery, S.; Kohagen, M.; Jurkiewicz, P.; Hof, M.; Jungwirth, P.; Cremer, P.S.; Cwiklik, L. The complex nature of calcium cation interactions with phospholipid bilayers. Sci. Rep. 2016, 6, 38035. [Google Scholar] [CrossRef]
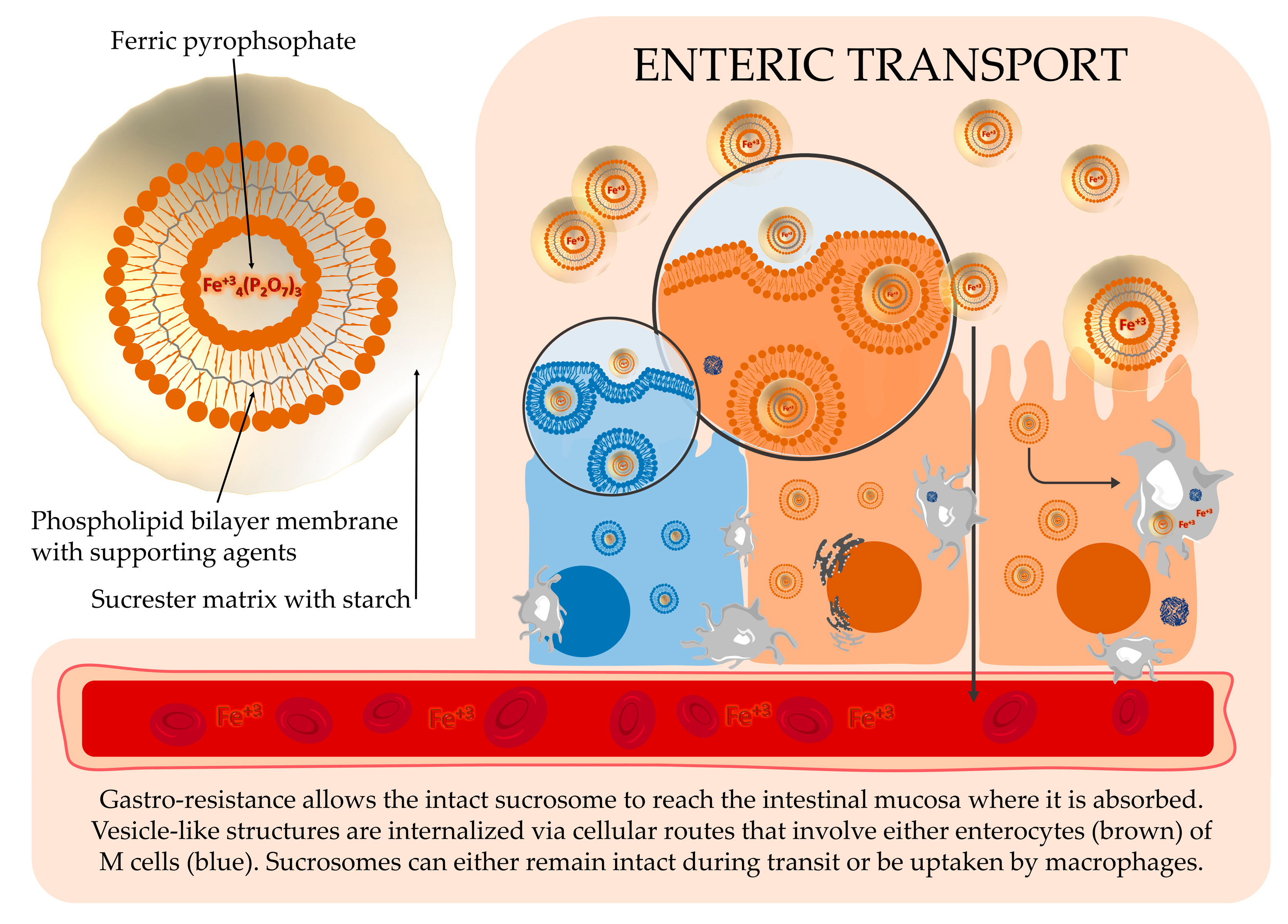
- Gómez-Ramírez, S.; Brilli, E.; Tarantino, G.; Muñoz, M. Sucrosomial® Iron: A New Generation Iron for Improving Oral Supplementation. Pharm. 2018, 11, 97. [Google Scholar] [CrossRef] [Green Version]
- Kiss, L.; Hellinger, É.; Pilbat, A.-M.; Kittel, Á.; Török, Z.; Füredi, A.; Szakacs, G.; Veszelka, S.; Sipos, P.; Ózsvári, B.; et al. Sucrose Esters Increase Drug Penetration, But Do Not Inhibit P-Glycoprotein in Caco-2 Intestinal Epithelial Cells. J. Pharm. Sci. 2014, 103, 3107–3119. [Google Scholar] [CrossRef]
- Fabiano, A.; Brilli, E.; Mattii, L.; Testai, L.; Moscato, S.; Citi, V.; Tarantino, G.; Zambito, Y. Ex Vivo and in Vivo Study of Sucrosomial((R)) Iron Intestinal Absorption and Bioavailability. Int. J. Mol. Sci. 2018, 19, 2722. [Google Scholar] [CrossRef] [Green Version]
- Noel, G.; Baetz, N.W.; Staab, J.F.; Donowitz, M.; Kovbasnjuk, O.; Pasetti, M.F.; Zachos, N.C. A primary human macrophage-enteroid co-culture model to investigate mucosal gut physiology and host-pathogen interactions. Sci. Rep. 2017, 7, 45270. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Randomization Step (Baseline, T0) (n = 73) | Prevalence out of Ref. Val. n (%) | |||
|---|---|---|---|---|
| ♂ (n = 30) | ♀ (n = 43) | ♂ | ♀ | |
| Hb (g/dL) | 15.0 ± 1.3 (11.7–17.0) | 13.5 ± 1.3 (9.6–16.1) | 2 (6.7) | 3 (6.9) |
| [ref. val.] | [13.7–17.5] | [11.2–15.7] | ||
| RBCs (106/μL) | 4.9 ± 0.4 (3.8–5.5) | 4.8 ± 0.5 (3.8–6.1) | 7 (23.4) | 8 (18.6) |
| [ref. val.] | [4.63–6.08] | [3.93–5.22] | ||
| MCV (fL/cell) | 89.8 (88.2; 92.5) | 88.4 (85.5; 90.8) | 8 (26.7) | 7 (16.3) |
| [ref. val.] | [79.0–92.2] | [79.4–94.8] | ||
| MCH (pg/cell) | 30.5 (29.7; 31.0) | 29.0 (27.5; 30.2) | 2 (6.7) | 7 (16.3) |
| [ref. val.] | [25.7–32.2] | [25.6–32.2] | ||
| MCHC (g/dL) | 33.9 ± 0.9 (32.6–35.6) | 32.7 ± 1.0 (30.7–34.8) | 0 (0.0) | 12 (27.9) |
| [ref. val.] | [32.3–36.5] | [32.2–35.5] | ||
| Iron (μg/dL) | 76.5 (65.5; 89.0) | 67.0 (57.0; 83.5) | 2 (6.7) | 2 (4.6) |
| [ref. val.] | [31–144] | [25–156] | ||
| Tf (mg/dL) | 247.0 (227.3; 256.3) | 268.0 (239.0; 296.0) | 2 (6.7) | 1 (2.3) |
| [ref. val.] | [163–344] | [180–382] | ||
| Tf sat (%) | 21.5 (18.3; 25.8) | 17.0 (13.0; 23.0) | 11 (36.7) | 14 (32.6) |
| [ref. val.] | [20–50] | [15–50] | ||
| Ferritin (ng/mL) | 190.5 (125.5; 313.3) | 75.0 (39.5; 125.0) | 12 (40.0) | 4 (9.3) |
| [ref. val.] | [22–275] | [5–204] | ||
| Randomization Step (baseline, T0) | Preoperative Step (after 30 days, T1) | T0 p-Values * | T1 p-Values * | ||
|---|---|---|---|---|---|
| Hb (g/dL) | C | 14.3 ± 1.3 (11.7–16.4) | 14.1 ± 1.2 (11.2–15.9) | p = 0.403 | p = 0.259 |
| I | 14.0 ± 1.7 (9.6–17.0) | 13.8 ± 1.5 (10.7–16.6) | |||
| RBCs (106/μL) | C | 4.9 ± 0.4 (3.8–5.7) | 4.8 ± 0.4 (3.7–5.4) | p = 0.483 | p = 0.584 |
| I | 4.8 ± 0.6 (3.8–6.1) | 4.7 ± 0.5 (3.6–6.0) | |||
| MCV (fL/cell) | C | 89.5 (86.3; 91.5) | 88.1 (86.1; 92.3) | p = 0.608 | p = 0.825 |
| I | 89.0 (86.1; 92.0) | 89.5 (85.3; 91.2) | |||
| MCH (pg/cell) | C | 30.0 (28.5; 30.6) | 30.0 (28.5; 30.9) | p = 0.800 | p = 0.627 |
| I | 29.7 (28.5; 30.7) | 29.7 (28.5; 30.9) | |||
| MCHC (g/dL) | C | 33.2 ± 1.0 (30.8–35.5) | 33.5 ± 1.0 (31.9–35.6) | p = 0.904 | p = 0.906 |
| I | 33.2 ± 1.2 (30.7–35.6) | 33.5 ± 1.4 (30.5–37.0) | |||
| Iron (μg/dL) | C | 74.0 (64.0; 85.0) | 87.0 (66.0; 107.0) | p = 0.476 | p = 0.830 |
| I | 69.0 (61.0; 83.0) | 94.0 (66.0; 110.0) | |||
| Tf (mg/dL) | C | 258.0 (234.8; 287.0) | 256.5 (229.8; 291.8) | p = 0.402 | p = 0.559 |
| I | 253.0 (228.0; 285.0) | 248.0 (229.0; 274.0) | |||
| Tf sat (%) | C | 20.0 (15.0; 23.0) | 22.0 (16.8; 30.3) | p = 0.774 | p = 0.515 |
| I | 20.0 (16.0; 23.0) | 24.0 (17.0; 32.0) | |||
| Ferritin (ng/mL) | C | 129.0 (75.0; 218.0) | 151.5 (68.8; 229.0) | p = 0.318 | p = 0.256 |
| I | 100.0 (51.0; 181.0) | 94.0 (51.0; 161.0) |
| 30-Days Changes (T1-T0)% | p-Values * | ||
|---|---|---|---|
| C | I | ||
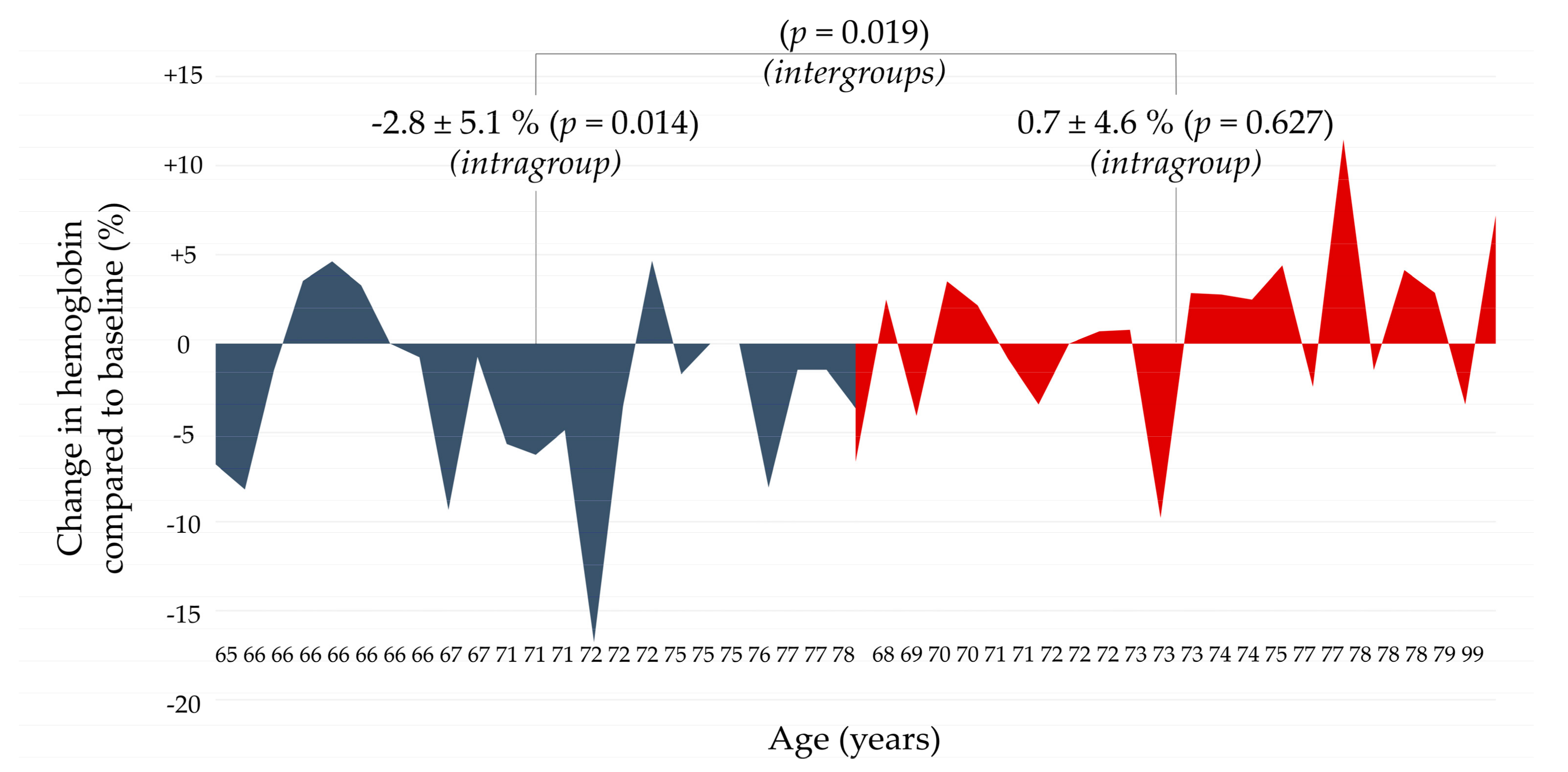
| Δ *Hb | −2.8 ± 5.1 | 0.7 ± 4.6 | p = 0.019 |
| ΔRBCs | −3.3 ± 5.7 | 0.0 ± 4.8 | p = 0.041 |
| ΔMCV | −0.2 | −0.1 | p = 0.923 |
| ΔMCH | 0.3 | 0.0 | p = 0.708 |
| ΔMCHC | 0.8 ± 2.0 | 1.1 ± 4.5 | p = 0.806 |
| ΔIron | 24.2 | 40.8 | p = 0.709 |
| ΔTf | −0.2 | 0.9 | p = 0.904 |
| ΔTIBC | 20.0 | 42.6 | p = 0.754 |
| ΔFerritin | 7.3 | 1.7 | p = 0.952 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briguglio, M.; Hrelia, S.; Malaguti, M.; De Vecchi, E.; Lombardi, G.; Banfi, G.; Riso, P.; Porrini, M.; Romagnoli, S.; Pino, F.; et al. Oral Supplementation with Sucrosomial Ferric Pyrophosphate Plus L-Ascorbic Acid to Ameliorate the Martial Status: A Randomized Controlled Trial. Nutrients 2020, 12, 386. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020386
Briguglio M, Hrelia S, Malaguti M, De Vecchi E, Lombardi G, Banfi G, Riso P, Porrini M, Romagnoli S, Pino F, et al. Oral Supplementation with Sucrosomial Ferric Pyrophosphate Plus L-Ascorbic Acid to Ameliorate the Martial Status: A Randomized Controlled Trial. Nutrients. 2020; 12(2):386. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020386
Chicago/Turabian StyleBriguglio, Matteo, Silvana Hrelia, Marco Malaguti, Elena De Vecchi, Giovanni Lombardi, Giuseppe Banfi, Patrizia Riso, Marisa Porrini, Sergio Romagnoli, Fabio Pino, and et al. 2020. "Oral Supplementation with Sucrosomial Ferric Pyrophosphate Plus L-Ascorbic Acid to Ameliorate the Martial Status: A Randomized Controlled Trial" Nutrients 12, no. 2: 386. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12020386