Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Dysphagia Assessment
2.4. Clinical Assessment of Patients with Dementia
2.5. Management of OD During Admission
2.6. Adaptation of Fluid Viscosity
2.7. Texture Modified Diets
2.8. Recommendations on Discharge
2.9. Follow-Up Period
2.10. Statistical Analysis
3. Results
3.1. Hospitalization Period
3.1.1. Demographic and Clinical Characteristics of Study Population
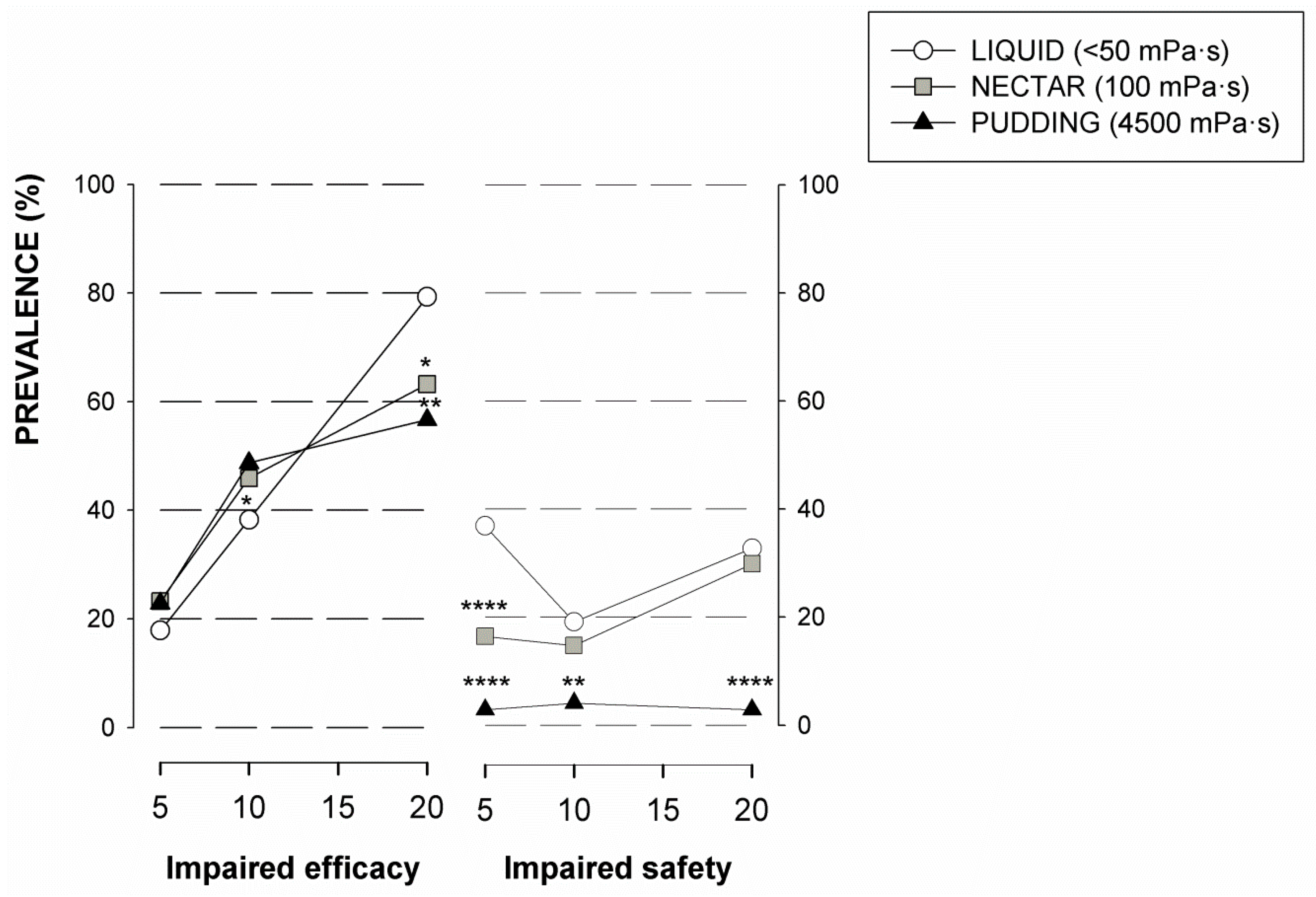
3.1.2. Oropharyngeal Dysphagia
3.1.3. Nutritional Status
3.1.4. Oral health and Hygiene Status
3.1.5. Clinical Outcomes during Hospitalization
3.2. Follow-Up Period—18 months after Discharge
3.2.1. Treatment Compliance
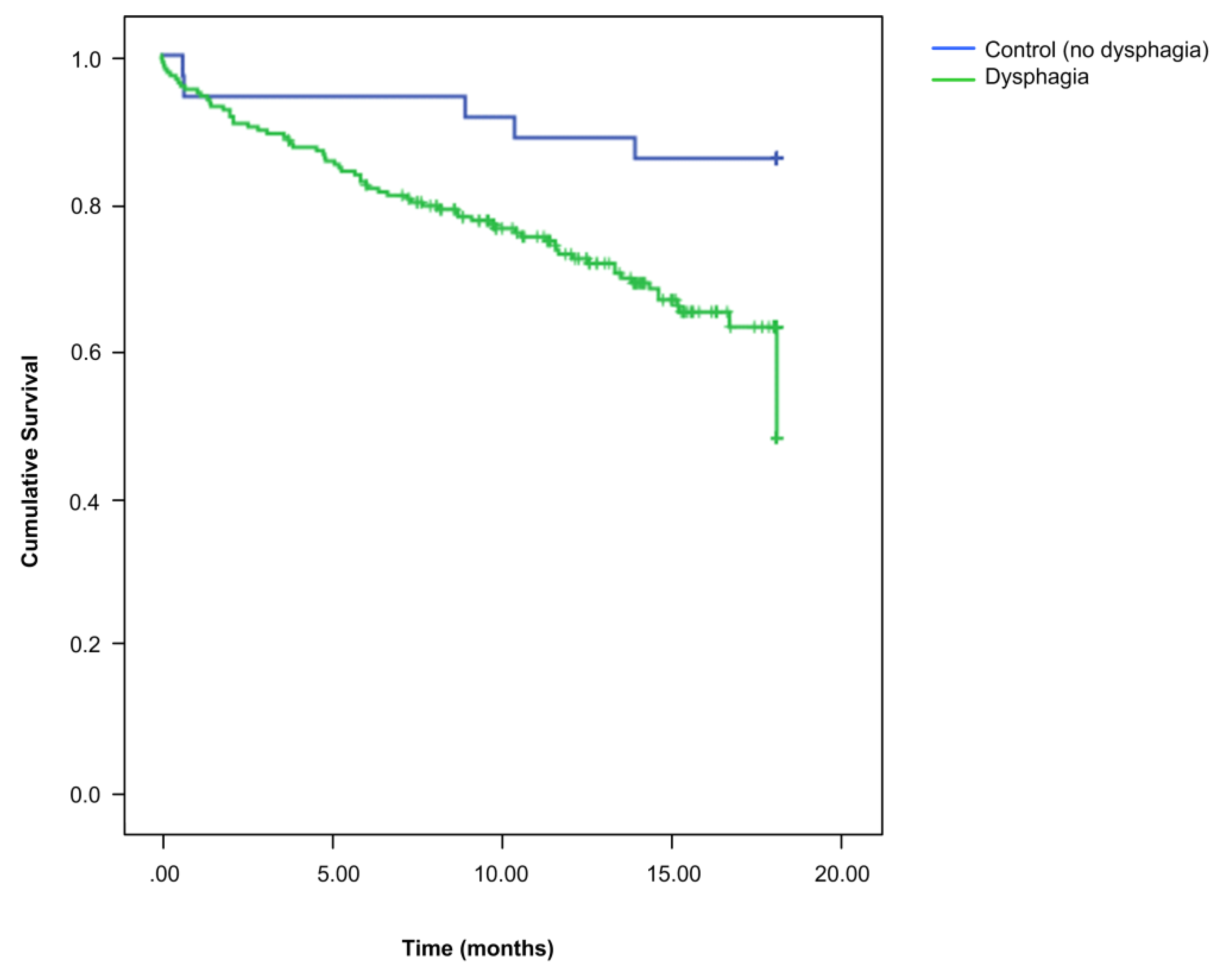
3.2.2. Long Term Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Affoo, R.H.; Foley, N.; Rosenbek, J.; Kevin Shoemaker, J.; Martin, R.E. Swallowing dysfunction and autonomic nervous system dysfunction in Alzheimer’s disease: A scoping review of the evidence. J. Am. Geriatr. Soc. 2013, 61, 2203–2213. [Google Scholar] [CrossRef] [PubMed]
- Paranji, S.; Paranji, N.; Wright, S.; Chandra, S. A Nationwide Study of the Impact of Dysphagia on Hospital Outcomes among Patients with Dementia. Am. J. Alzheimers Dis. Dement. 2016, 32, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 28 February 2020).
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Brunnström, H.; Englund, E. Cause of death in patients with dementia disorders. Eur. J. Neurol. 2009, 16, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.L.; Teno, J.M.; Kiely, D.K.; Shaffer, M.L.; Jones, R.N.; Prigerson, H.G.; Volicer, L.; Givens, J.L.; Hamel, M.B. The clinical course of advanced dementia. N. Engl. J. Med. 2009, 361, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Busto, F.; Andia, V.; De Alegria, L.R.; Francés, I. Abordaje de la disfagia en la demencia avanzada. Revista Española de Geriatría y Gerontología 2009, 44 (Suppl. 2), 29–36. [Google Scholar]
- Chouinard, J. Dysphagia in Alzheimer disease: A review. J. Nutr. Heal. Aging 2000, 4, 214–217. [Google Scholar]
- Humbert, I.A.; McLaren, D.G.; Kosmatka, K.; Fitzgerald, M.; Johnson, S.; Porcaro, E.; Kays, S.; Umoh, E.-O.; Robbins, J.; Fitzgerald, M. Early Deficits in Cortical Control of Swallowing in Alzheimer’s Disease. J. Alzheimers Dis. 2010, 19, 1185–1197. [Google Scholar] [CrossRef] [Green Version]
- Miarons, M.; Clavé, P.; Wijngaard, R.; Ortega, O.; Arreola, V.; Nascimento, W.; Rofes, L. Pathophysiology of Oropharyngeal Dysphagia Assessed by Videofluoroscopy in Patients with Dementia Taking Antipsychotics. J. Am. Med. Dir. Assoc. 2018, 19, 812.e1–812.e10. [Google Scholar] [CrossRef]
- Groher, M.E. Determination of the risks and benefits of oral feeding. Dysphagia 1994, 9, 233–235. [Google Scholar] [CrossRef]
- Clavé, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Michel, A.; Vérin, E.; Gbaguidi, X.; Druesne, L.; Roca, F.; Chassagne, P. Oropharyngeal Dysphagia in Community-Dwelling Older Patients with Dementia: Prevalence and Relationship with Geriatric Parameters. J. Am. Med. Dir. Assoc. 2018, 19, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.; Ortega, O.; Roca, M.; Arús, M.; Clavé Civit, P. Effect of a Minimal-Massive Intervention in Hospitalized Older Patients with Oropharyngeal Dysphagia: A Proof of Concept Study. J. Nutr. Heal. Aging 2018, 22, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [Green Version]
- Rofes, L.; Arreola, V.; Clavé, P. The Volume-Viscosity Swallow Test for Clinical Screening of Dysphagia and Aspiration. Nestlé Nutr. Workshop Ser. 2012, 72, 33–42. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Reisberg, B.; Ferris, S.H.; De Leon, M.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar]
- Reisberg, B. Functional assessment staging (FAST). Psychopharmacol. Bull. 1988, 24, 653–659. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Greene, J.G.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Formiga, F.; Fort, I.; Robles, M.J.; Barranco, E.; Espinosa, M.C.; Riu, S. Medical comorbidity in elderly patients with dementia. Differences according age and gender. Revista Clínica Española 2007, 207, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Rösler, A.; Pfeil, S.; Lessmann, H.; Höder, J.; Befahr, A.; Von Renteln-Kruse, W. Dysphagia in Dementia: Influence of Dementia Severity and Food Texture on the Prevalence of Aspiration and Latency to Swallow in Hospitalized Geriatric Patients. J. Am. Med. Dir. Assoc. 2015, 16, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Jodra, A.F.; Ordóñez, M.C.; Lidón, E.G.; Monforte, C.A. Evaluación de la actividad de una unidad de media estancia de psicogeriatria. Revista Española de Geriatría y Gerontología 2002, 37, 190–197. [Google Scholar] [CrossRef]
- Cabré, M.; Serra-Prat, M.; Force, L.; Mir, P.; Palomera, E.; Clavé, P. Oropharyngeal Dysphagia is a Risk Factor for Readmission for Pneumonia in the Very Elderly Persons: Observational Prospective Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2013, 69, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Cabré, M.; Serra-Prat, M.; Palomera, E.; Mir, P.; Pallares, R.; Clavé, P. Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age Ageing 2009, 39, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Horner, J.; Alberts, M.J.; Dawson, D.V.; Cook, G.M. Swallowing in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 1994, 8, 177–189. [Google Scholar]
- Langmore, S.; Olney, R.K.; Lomen-Hoerth, C.; Miller, B.L. Dysphagia in Patients with Frontotemporal Lobar Dementia. Arch. Neurol. 2007, 64, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Suh, M.K.; Kim, H.; Na, D.L. Dysphagia in Patients with Dementia. Alzheimer Dis. Assoc. Disord. 2009, 23, 178–184. [Google Scholar] [CrossRef]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders–European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [Green Version]
- Ortega, O.; Clavé, P. Oral Hygiene, Aspiration, and Aspiration Pneumonia: From Pathophysiology to Therapeutic Strategies. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 292–295. [Google Scholar] [CrossRef] [Green Version]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Mir, P.; Cabre, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851–858, e230. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rofes, L.; Arreola, V.; Mukherjee, R.; Swanson, J.; Clavé, P. The effects of a xanthan gum-based thickener on the swallowing function of patients with dysphagia. Aliment. Pharmacol. Ther. 2014, 39, 1169–1179. [Google Scholar] [CrossRef]
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. 2015, 34, 436–442. [Google Scholar] [CrossRef]
- Li, S.-C. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar] [CrossRef] [Green Version]
- Crawford, H.; Leslie, P.; Drinnan, M. Compliance with Dysphagia Recommendations by Carers of Adults with Intellectual Impairment. Dysphagia 2007, 22, 326–334. [Google Scholar] [CrossRef]
- Cichero, J. Thickening agents used for dysphagia management: Effect on bioavailability of water, medication and feelings of satiety. Nutr. J. 2013, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Matta, Z.; Iv, E.C.; Garcia, J.M.; Helverson, J.M. Sensory Characteristics of Beverages Prepared with Commercial Thickeners Used for Dysphagia Diets. J. Am. Diet. Assoc. 2006, 106, 1049–1054. [Google Scholar] [CrossRef]
- National Patient Safety Agency (NPSA). Dysphagia Diet Food Texture Descriptors; National Patient Safety Agency: London, UK, 2011.
- Costa, A.; Carrión, S.; Puig-Pey, M.; Juárez, F.; Clavé, P. Triple Adaptation of the Mediterranean Diet: Design of A Meal Plan for Older People with Oropharyngeal Dysphagia Based on Home Cooking. Nutrients 2019, 11, 425. [Google Scholar] [CrossRef] [Green Version]
- O’keeffe, S.T. Use of modified diets to prevent aspiration in oropharyngeal dysphagia: Is current practice justified? BMC Geriatr. 2018, 18, 167. [Google Scholar]
- Kossioni, A. Is Europe prepared to meet the oral health needs of older people? Gerodontology 2011, 29, e1230–e1240. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Soga, Y.; Maekawa, K.; Kanda, Y.; Kobayashi, E.; Inoue, H.; Kanao, A.; Himuro, Y.; Fujiwara, Y. Prevalence of oral health-related conditions that could trigger accidents for patients with moderate-to-severe dementia. Gerodontology 2016, 34, 129–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, O.; Parra, C.; Zarcero, S.; Nart, J.; Sakwinska, O.; Clavé, P.; Ortega, O. Oral health in older patients with oropharyngeal dysphagia. Age Ageing 2014, 43, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, O.; Sakwinska, O.; Combremont, S.; Berger, B.; Sauser, J.; Parra, C.; Zarcero, S.; Nart, J.; Carrión, S.; Clavé, P. High prevalence of colonization of oral cavity by respiratory pathogens in frail older patients with oropharyngeal dysphagia. Neurogastroenterol. Motil. 2015, 27, 1804–1816. [Google Scholar] [CrossRef]
- Hoppitt, T.; Sackley, C.M.; Wright, C. Finding the right outcome measures for care home research. Age Ageing 2009, 39, 119–122. [Google Scholar] [CrossRef] [Green Version]
- Serra-Prat, M.; Palomera, M.; Gomez, C.; Sar-Shalom, D.; Saiz, A.; Montoya, J.G.; Navajas, M.; Clavé, P. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: A population-based prospective study. Age Ageing 2012, 41, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and Management of Oropharyngeal Dysphagia among Older Persons, State of the Art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| TOTAL (n = 255) | OD (n = 219) | ND (n = 36) | p-Value | |
|---|---|---|---|---|
| Age (years) | 83.5 ± 8 | 84.06 ± 7.8 | 80.16 ± 8.5 | 0.007 |
| Sex (♀) | 61.6% (157) | 61.2% (134) | 63.9% (23) | 0.757 |
| Charlson | 2.01 ± 1.4 | 2.1 ± 1.4 | 1.8 ± 1.1 | 0.432 |
| Barthel Admission Discharge | 30.8 ± 24.7 39.6 ± 26.5 | 28.65 ± 24.4 37.46 ± 26.6 | 44.03 ± 23.1 52.64 ± 21.7 | < 0.0001 0.002 |
| Dementia severity GDS (% (n)) 2–3 4 5 6 7 FAST (% (n)) 2–3 4 5 6 7 Cognitive assessment MMSE MMSE (% (n)) < 11 11–19 > 19 | n = 233 1.6 (4) 9.0 (23) 20.8 (53) 42.7 (109) 17.3 (44) n = 228 0.4 (1) 8.3 (19) 14.9 (34) 50.4 (115) 25.9 (59) n = 191 11.9 ± 7.0 38.2 (73) 49.2 (94) 12.6 (24) | n =2 01 0.5 (1) 9.5 (19) 21.9 (44) 46.3 (93) 21.9 (44) n = 200 0 (0) 8 (16) 15.5 (31) 48.0 (96) 28.5 (57) n = 161 11.7 ± 7.1 38.5 (62) 49.7 (80) 11.8 (19) | n = 32 9.4 (3) 12.5 (4) 28.1 (9) 50.0 (16) 0.0 (0) n = 28 3.6 (1) 10.7 (3) 10.7 (3) 67.9 (19) 7.1 (2) n = 30 12.1 ± 6.8 36.7 (11) 46.7 (14) 16.7 (5) | < 0.001 0.007 0.759 0.761 |
| MNA-sf | 7.17 ± 2.67 | 7 ± 2.68 | 8.2 ± 2.45 | 0.014 |
MNA-sf (% (n)) Well-nourished (12–14) At risk (8–11) Malnourished (0–7) | n = 255 3.7 (9) 44.7 (110) 51.6 (127) | n = 211 3.3 (7) 43.1 (91) 53.6 (113) | n = 35 5.7 (2) 54.3 (19) 40.0 (14) | 0.305 |
| OHI-S DI-S CI-S | 2.7 ± 1.2 1.4 ± 0.8 1.3 ± 1.0 | 2.7 ± 1.2 1.4 ± 0.9 1.4 ± 1.0 | 2.5 ± 1.1 1.4 ± 0.5 1.1 ± 0.7 | 0.540 0.790 0.410 |
| 18 MONTHS FOLLOW-UP | ||||
|---|---|---|---|---|
| TOTAL (n = 255) | OD (n = 219) | ND (n = 36) | p-Value | |
| Resp. Infections (episodes/patient) Resp. Infections (% (n)) LTRI (% (n)) Pneumonia (% (n)) Fever without focus (% (n)) | 0.9 ± 1.5 48.1 (112) 43.0 (99) 12.6 (28) 6.4 (14) | 1.0 ± 1.5 51.8 (102) 45.9 (89) 14.0 (26) 7.7 (14) | 0.6 ± 1.2 27.8 (10) 27.8 (10) 5.6 (2) 0.0 (0) | 0.040 0.011 0.046 0.270 0.134 |
| Re-admissions (episodes/patient) Re-admissions (% (n)) Respiratory infections (% (n)) Other diseases (% (n)) | 0.6 ± 1.0 44.3 (104) 21.2 (49) 30.9 (69) | 0.6 ± 0.9 41.7 (83) 21.0 (41) 28.3 (53) | 0.9 ± 1.0 58.3 (21) 22.2 (8) 44.4 (16) | 0.015 0.071 0.828 0.075 |
| Institutionalization rate (% (n)) | 45.9 (117) | 47.5 (104) | 36.1 (13) | 0.118 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Mortality during follow-up | ||
| Oropharyngeal dysphagia | 2.81 (0.972–8.106) | 0.056 |
| Age | 1.04 (1.012–1.075) | 0.012 |
| Barthel score | 0.98 (0.971–0.994) | 0.004 |
| Dementia severity | 1.09 (0.552–2.160) | 0.801 |
| Respiratory Infection during follow-up | ||
| Oropharyngeal dysphagia | 2.36 (0.958–5.793) | 0.062 |
| Age | 1.05 (1.004–1.088) | 0.029 |
| Barthel score | 1.00 (0.984–1.013) | 0.823 |
| Dementia severity | 0.93 (0.438–1.965) | 0.846 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients 2020, 12, 863. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030863
Espinosa-Val MC, Martín-Martínez A, Graupera M, Arias O, Elvira A, Cabré M, Palomera E, Bolívar-Prados M, Clavé P, Ortega O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients. 2020; 12(3):863. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030863
Chicago/Turabian StyleEspinosa-Val, Mᵃ Carmen, Alberto Martín-Martínez, Mercè Graupera, Olivia Arias, Amparo Elvira, Mateu Cabré, Elisabet Palomera, Mireia Bolívar-Prados, Pere Clavé, and Omar Ortega. 2020. "Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia" Nutrients 12, no. 3: 863. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12030863