Increasing Food Expenditure in Long Day-Care by an Extra $0.50 Per Child/Day Would Improve Core Food Group Provision



Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Data Analysis
2.3. Exclusion Criteria
3. Results
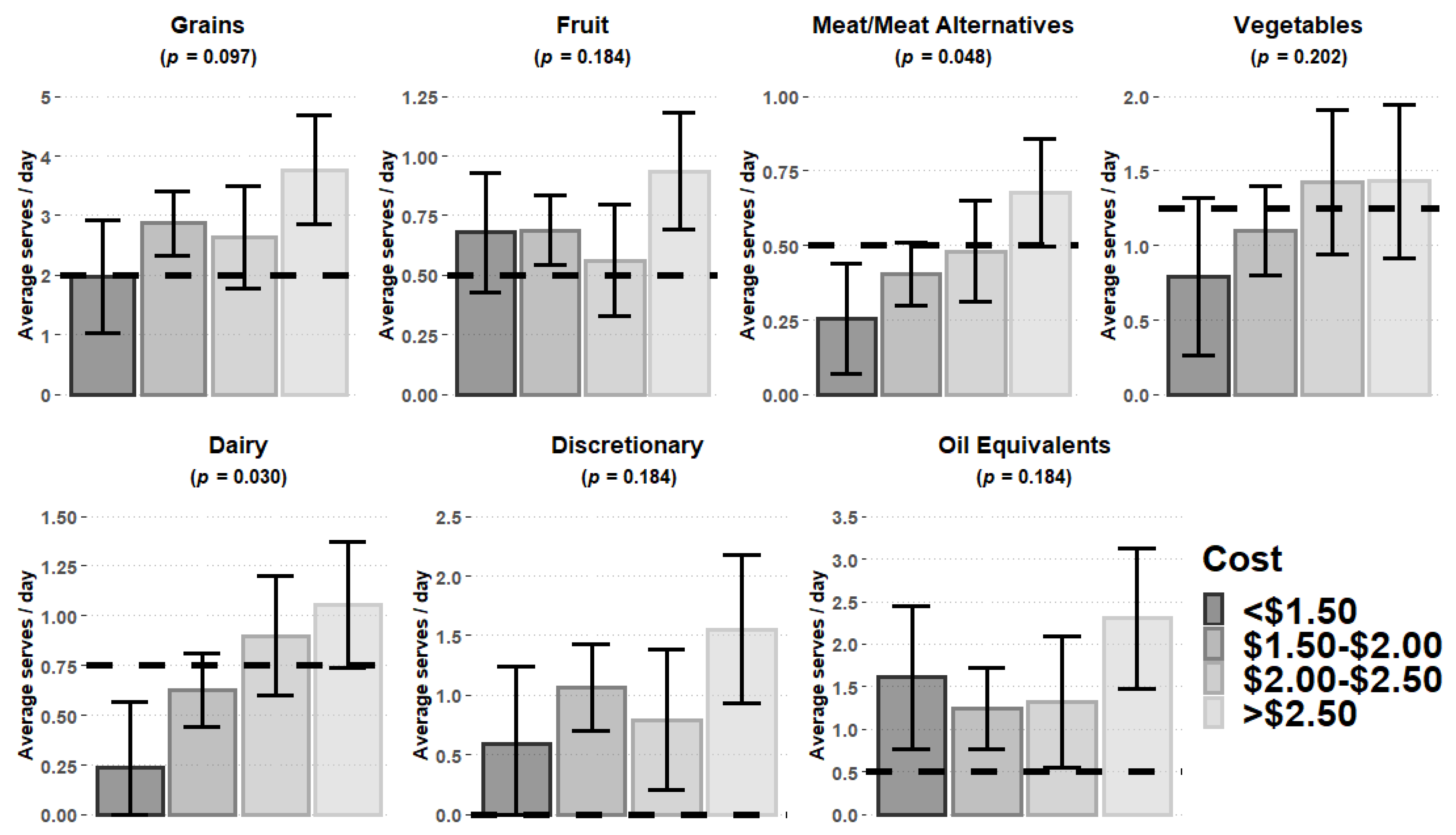
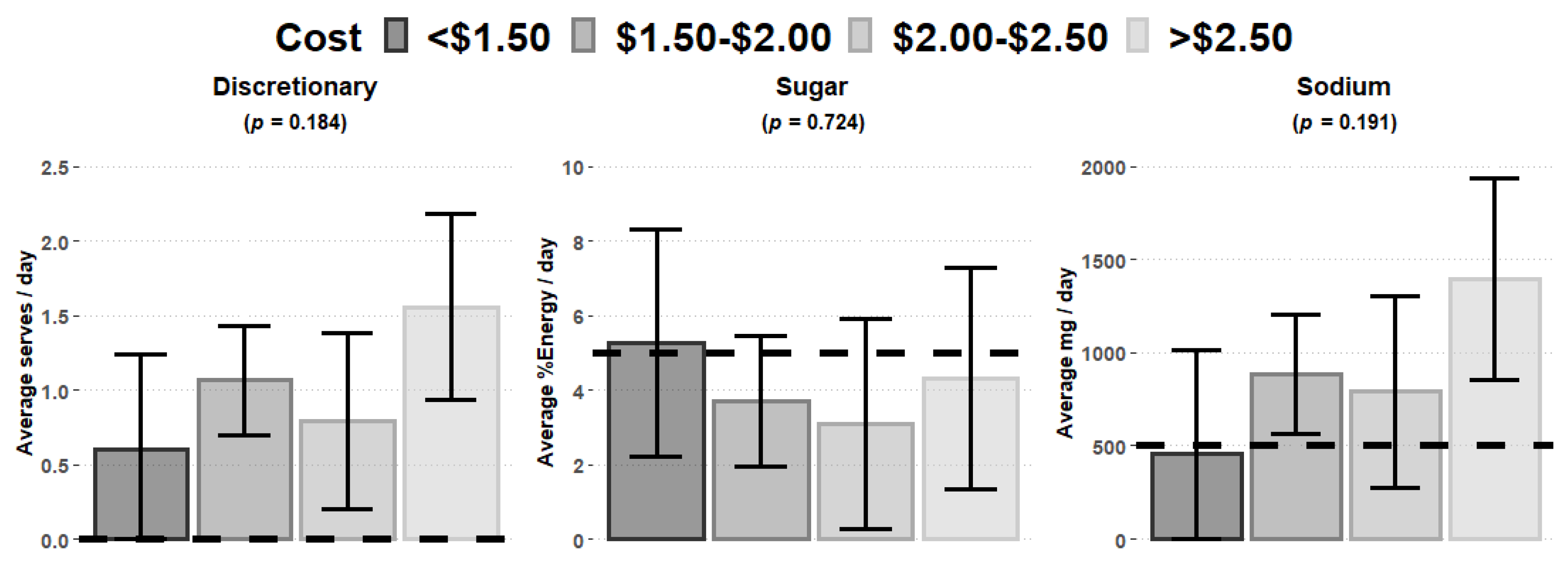
Food Expenditure vs. Food Group Provision
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Spence, A.C.; Campbell, K.J.; Lioret, S.; McNaughton, S.A. Early childhood vegetable, fruit, and discretionary food intakes do not meet dietary guidelines, but do show socioeconomic differences and tracking over time. J. Acad. Nutr. Diet. 2018, 118, 1634–1643.e1. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Li, J.; Foster, J.; Hickling, S.; Jacques, A.; O’Sullivan, T.A.; Oddy, W.H. Good-quality diet in the early years may have a positive effect on academic achievement. Acta Paediatr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Foster, J.K.; Hickling, S.; Li, J.; Ambrosini, G.L.; Jacques, A.; Oddy, W.H. Prospective associations between dietary patterns and cognitive performance during adolescence. J. Child Psychol. Psychiatry 2014, 55, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health and Welfare. Nutrition Across the Life Stages; Australian Institute of Health and Welfare [AIHW]: Canberra, Australia, 2018.
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition—Barriers to and opportunities for healthier eating. BMJ 2018, 361, k2426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Education and Training. Early Childhood and Child Care in Summary: Sept Quarter 2019; Department of Education and Training, Ed.; Department of Education and Training: Canberra, Australia, 2019.
- Department of Education and Training. Early Childhood and Child Care in Summary: June Quarter 2018; Department of Education and Training, Ed.; Department of Education and Training: Canberra, Australia, 2018.
- Queensland Government. Long Day Care, Queensland, Australia: Early Childhood Information Service. 2019. Available online: https://www.qld.gov.au/families/babies/childcare/types/long (accessed on 6 March 2020).
- ABS. ABoS. Child Care. 2010. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4102.0Main+Features50Jun+2010 (accessed on 6 March 2020).
- ABS. ABoS. Child Care. 2017. Available online: https://www.abs.gov.au/ausstats/[email protected]/Latestproducts/4402.0Media%20Release1June%202017?opendocument&tabname=Summary&prodno=4402.0&issue=June%202017&num=&view= (accessed on 6 March 2020).
- Briley, M.; McAllaster, M. Nutrition and the child-care setting. J. Am. Diet. Assoc. 2011, 111, 1298–1300. [Google Scholar] [CrossRef]
- Australian Institute of Health Welfare. Overweight and Obesity: An Interactive Insight; AIHW: Canberra, Australia, 2019.
- Brown, V.; Moodie, M.; Baur, L.; Wen, L.; Hayes, A. The high cost of obesity in Australian pre-schoolers. Aust. N. Z. J. Public Health 2017. [Google Scholar] [CrossRef] [Green Version]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Population-Based Approaches to Childhood Obesity Prevention; Switzerland WHO Document Production Services: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organisation. Report of the Commission on Ending Childhood Obesity; Production, W.D., Ed.; WHO Document Production: Genva, Switzerland, 2016. [Google Scholar]
- National Health and Medical Research Council. Australian Dietary Guidelines; NHMRC: Canberra, Australia, 2013.
- Bell, L.; Hendrie, G.; Hartley, J.; Golley, R. Impact of a nutrition award scheme on the food and nutrient intakes of 2- to 4-year-olds attending long day care. Public Health Nutr. 2015. [Google Scholar] [CrossRef] [Green Version]
- O’Halloran, S.A.; Lacy, K.E.; Grimes, C.A.; Campbell, K.J.; Nowson, C.A. Sodium content of lunches and snacks provided in australian long day care centres: A cross-sectional study. Nutrients 2018, 10, 284. [Google Scholar] [CrossRef] [Green Version]
- Finch, M.; Wolfenden, L.; Falkiner, M.; Edenden, D.; Pond, N.; Hardy, L.L.; Milat, A.J.; Wiggers, J. Impact of a population based intervention to increase the adoption of multiple physical activity practices in centre based childcare services: A quasi experimental, effectiveness study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambell, R.; Devine, A.; Lo, J. Does the food group provision in early years’ education and care settings in metropolitan Perth, Western Australia, meet national dietary requirements; and how can home economics support this? J. Home Econ. Inst. Aust. 2014, 21, 20–27. [Google Scholar]
- Wallace, R.; Costello, L.; Devine, A. Over-provision of discretionary foods at childcare dilutes the nutritional quality of diets for children. Aust. N. Z. J. Public Health 2017, 41, 447. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, T.; Lim, C.; Otten, J. What’s for lunch? A socio-ecological approach to childcare nutrition. In Proceedings of the DIS ‘16: Proceedings of the 2016 ACM Conference on Designing Interactive Systems, Brisbane, Australia, 4–8 June 2016. [Google Scholar]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Drewnowski, A. Nutrition economics: How to eat better for less. J. Nutr. Sci. Vitaminol. 2015, 61 (Suppl. S69–S71). [Google Scholar] [CrossRef] [Green Version]
- Australian Children’s Education & Care Quality Authority [ACECQA]. Guide to National Quality Framework. 2018. Available online: https://www.acecqa.gov.au/sites/default/files/2018-03/Guide-to-the-NQF_0.pdf (accessed on 10 December 2018).
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analyses for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Sambell, R.; Wallace, R.; Costello, L.; Lo, J.; Devine, A. Measuring food provision in Western Australian long day care (LDC) services: A weighed food record method/protocol at a service level. Nutr. J. 2019, 18, 38. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics [ABS]. Socio-Economic Indexes for Areas: ABS. 2016. Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 10 August 2019).
- Xyris Software. FoodWorks 9 Professional; High Gate Hill: Brisbane, Australia, 2018. [Google Scholar]
- World Health Organisation. Healthy Diet. Fact Sheet No 394; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; NHMRC: Canberra, Australia, 2017.
- Eat for Health. Discretionary Food and Drink Choices, Australian Government—National Health and Medical Research Council. 2017. Available online: https://www.eatforhealth.gov.au/food-essentials/discretionary-food-and-drink-choices (accessed on 16 May 2019).
- IBM Corp. IBM SPSS Statistics for Windows; Version 250; IBM Corp.: Armonk, NY, USA, 2018. [Google Scholar]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Hodder, R.K.; Stacey, F.G.; O’Brien, K.M.; Wyse, R.J.; Clinton-McHarg, T.; Tzelepis, F.; Nathan, N.K.; James, E.L.; Bartlem, K.M.; Sutherland, R.; et al. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane database Syst. Rev. 2018, 1, CD008552. [Google Scholar]
- Mennella, J.A.; Reiter, A.R.; Daniels, L.M. Vegetable and fruit acceptance during infancy: Impact of ontogeny, genetics, and early experiences. Adv. Nutr. 2016, 7, 211S–219S. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.J.; Kane, S.; Ramsey, R.; Good, E.; Dick, M. Testing the price and affordability of healthy and current (unhealthy) diets and the potential impacts of policy change in Australia. BMC Public Health 2016, 16, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, M.; Li, A.; Hill, A.J.; Cunich, M.; Skilton, M.R.; Madigan, C.D.; Caterson, I.D. Modelling the association between core and discretionary energy intake in adults with and without obesity. Nutrients 2019, 11, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Expect A Star. Cook Qualification Requirements. 2018. Available online: https://expectastar.com.au/cook-qualifications-and-requirements (accessed on 15 February 2020).
- Australian Academy of Science. Rethinking food and nutrition science: The food environment. In 2017 Theo Murphy High Flyers Think Tank Discussion Paper; Australian Academy of Science: Canberra, Australia, 2017. [Google Scholar]
- Wallace, R. Supporting Nutrition for Australian Childcare (SNAC): The Development, Implementation and Evaluation of an Online Nutrition Education Intervention. Ph.D. Thesis, Edith Cowan University, Perth, Australia, 2016. [Google Scholar]
- Yoong, L.; Skelton, E.; Jones, J.; Wolfenden, L. Do childcare services provide foods in line with the 2013 Australian dietary guidelines? A cross-sectional study. Aust. N. Z. J. Public Health 2014, 38, 595–596. [Google Scholar] [CrossRef] [Green Version]
- Lynch, M.; Batal, M. Factors influencing childcare providers’ food and mealtime decisions: An ecological approach. Child Care Pract. 2011, 17, 185–203. [Google Scholar] [CrossRef]
- Myszkowska-Ryciak, J.; Harton, A. Eating healthy, growing healthy: Outcome evaluation of the nutrition education program optimizing the nutritional value of preschool menus, Poland. Nutrients 2019, 11, 2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otten, J.J.; Hirsch, T.; Lim, C. Factors influencing the food purchases of early care and education providers. J. Acad. Nutr. Diet. 2017, 117, 725–734. [Google Scholar] [CrossRef]
- Driessen, C.E.; Cameron, A.J.; Thornton, L.E.; Lai, S.K.; Barnett, L.M. Effect of changes to the school food environment on eating behaviours and/or body weight in children: A systematic review. Obes. Rev. 2014, 15, 968–982. [Google Scholar] [CrossRef]
- Birch, L.L.; Doub, A.E. Learning to eat: Birth to age 2 y. Am. J. Clin. Nutr. 2014, 99, 723S–728S. [Google Scholar] [CrossRef] [Green Version]
- Cruwys, T.; Bevelander, K.E.; Hermans, R.C.J. Social modeling of eating: A review of when and why social influence affects food intake and choice. Appetite 2015, 86, 3–18. [Google Scholar] [CrossRef]
- French, S.A.; Epstein, L.H.; Jeffery, R.W.; Blundell, J.E.; Wardle, J. Eating behavior dimensions. Associations with energy intake and body weight. A review. Appetite 2012, 59, 541–549. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Food Group [18] | ADG Recommendation [18] | >50% Serves |
|---|---|---|
| Vegetables, legumes, beans | 2.5 | 1.25 |
| Fruit | 1 | 0.5 |
| Grains (cereals) | 4 | 2 |
| Meat and meat alternatives | 1 | 0.5 |
| Dairy and dairy alternatives | 1.5 | 0.75 |
| Additional comparisons | ||
| Unsaturated fats/oil equivalents | 6.5 g (as a midpoint between ADG recommendations for 2–3 and 3–12 years old) | 3.25 g |
| Added sugars | 10% of total energy | 50% of 10% of total energy |
| Sodium | 1000 mg/day | 500 mg/day |
| Discretionary foods | 0 serves | 0 serves |
| Variable | Response | n (%) | Univariable | Multivariable | ||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||
| Year | Overall | 0.602 | 0.407 | |||
| 2015 | 10 (33.3%) | 1.00 (Ref) | 1.00 (Ref) | |||
| 2016 | 11 (36.7%) | 3.4 (0.3, 40.9) | 0.330 | 0.63 (0.04, 9.00) | 0.737 | |
| 2017 | 9 (30%) | 3.0 (0.3, 35.3) | 0.383 | 0.05 (0.001, 4.353) | 0.190 | |
| Service | Private | 20 (66.7%) | 1.00 (Ref) | 1.00 (Ref) | ||
| Community-based | 10 (33.3%) | 1.7 (0.3, 9.8) | 0.544 | 2.3 (0.2, 25.5) | 0.505 | |
| SEIFA | Range 1–10 | 1.2 (0.4, 3.5) | 0.794 | 1.1 (0.7, 1.8) | 0.658 | |
| Cost per child (per 50¢ increment) | Range $1.17–$4.03 | 2.00 ± 0.59 | 2.6 (1, 6.7) | 0.050 * | 4.0 (1.1, 13.9) | 0.030 * |
| Meat and Meat Alternatives Food Group | Cost | Serve Size | Dairy Food Group | Cost | Serve Size |
|---|---|---|---|---|---|
| Lean beef mince—raw ($1.30/100 g) | $0.50/39 g | 0.5 | Milk—reduced fat ($0.10/100 ml) | $0.50/500 mL | 2.0 |
| Lean chicken—raw ($0.90/100 g) | $0.45/50 g | 0.5 | Hard cheese ($1.20/100 g) | $0.50/42 g | 1.0 |
| Canned legumes—cooked ($0.19/100 g) | $0.46/240 g | 2.0 | Yoghurt ($0.35/100 g) | $0.50/142 g | 0.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sambell, R.; Wallace, R.; Lo, J.; Costello, L.; Devine, A. Increasing Food Expenditure in Long Day-Care by an Extra $0.50 Per Child/Day Would Improve Core Food Group Provision. Nutrients 2020, 12, 968. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040968
Sambell R, Wallace R, Lo J, Costello L, Devine A. Increasing Food Expenditure in Long Day-Care by an Extra $0.50 Per Child/Day Would Improve Core Food Group Provision. Nutrients. 2020; 12(4):968. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040968
Chicago/Turabian StyleSambell, Ros, Ruth Wallace, Johnny Lo, Leesa Costello, and Amanda Devine. 2020. "Increasing Food Expenditure in Long Day-Care by an Extra $0.50 Per Child/Day Would Improve Core Food Group Provision" Nutrients 12, no. 4: 968. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12040968