Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
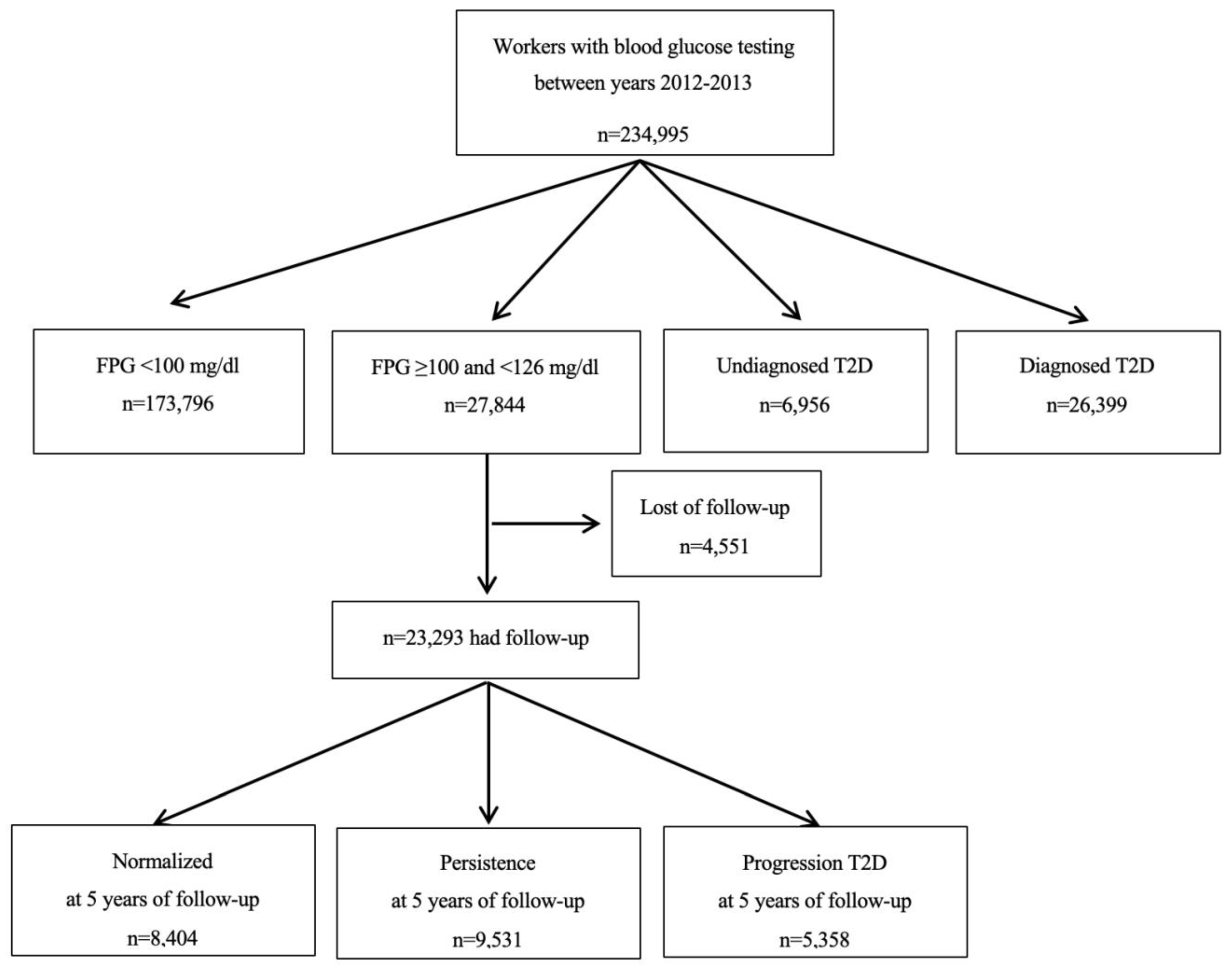
2.1. Data Collection and Definition of Variables
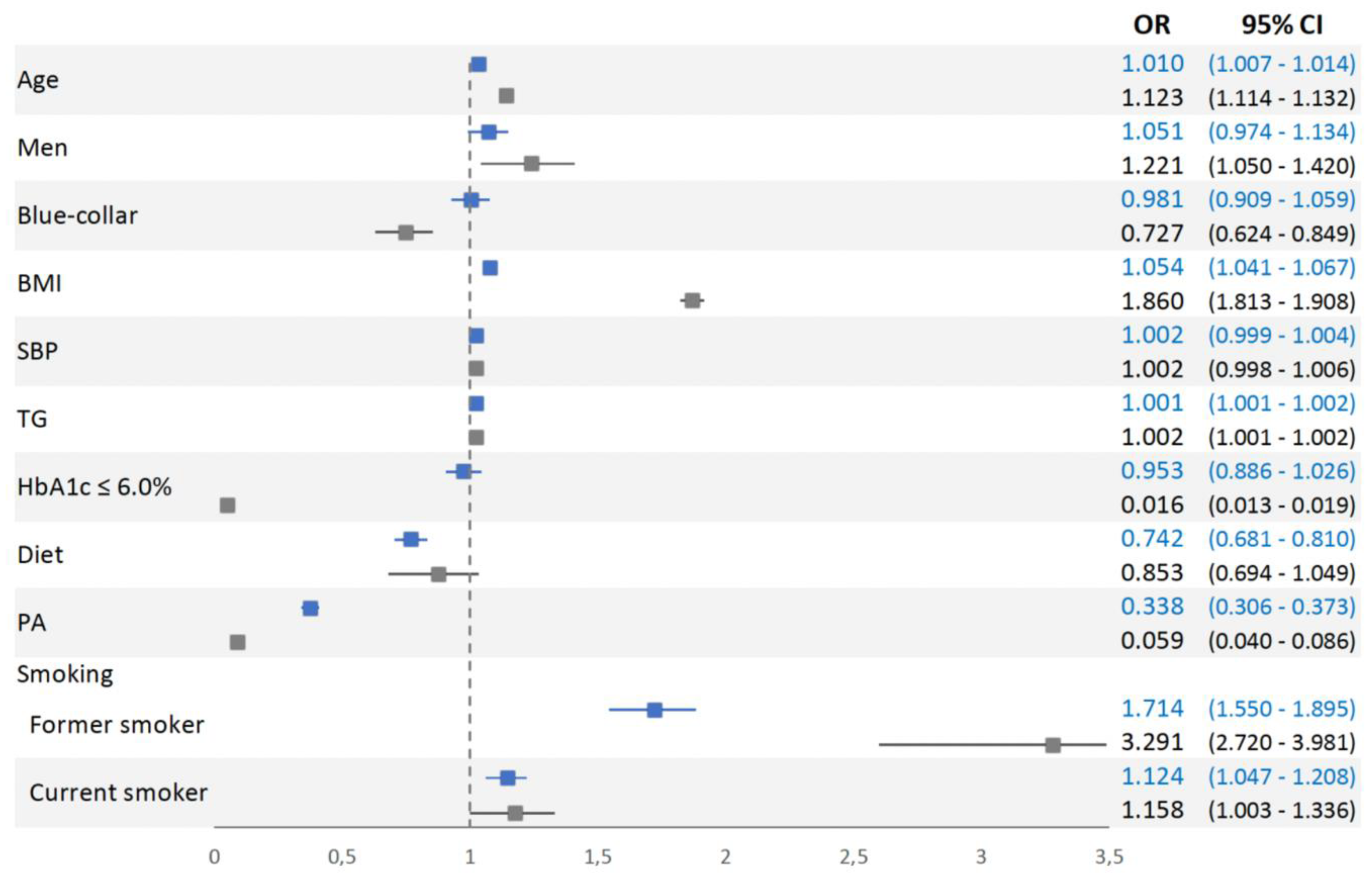
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4·4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [Green Version]
- Chamnan, P.; Simmons, R.K.; Forouhi, N.G.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Griffin, S.J. Incidence of type 2 diabetes using proposed HbA1c diagnostic criteria in the european prospective investigation of cancer-norfolk cohort: Implications for preventive strategies. Diabetes Care 2011, 34, 950–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standl, E.; Khunti, K.; Hansen, T.B.; Schnell, O. The global epidemics of diabetes in the 21st century: Current situation and perspectives. Eur. J. Prev. Cardiol. 2019, 26, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dall, T.M.; Narayan, K.M.; Gillespie, K.B.; Gallo, P.D.; Blanchard, T.D.; Solcan, M.; O’Grady, M.; Quick, W.W. Detecting type 2 diabetes and prediabetes among asymptomatic adults in the United States: Modeling American Diabetes Association versus US Preventive Services Task Force diabetes screening guidelines. Popul. Health Metr. 2014, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Vistisen, D.; Witte, D.R.; Brunner, E.J.; Kivimaki, M.; Tabak, A.; Jorgensen, M.E.; Faerch, K. Risk of Cardiovascular Disease and Death in Individuals with Prediabetes Defined by Different Criteria: The Whitehall II Study. Diabetes Care 2018, 41, 899–906. [Google Scholar] [CrossRef] [Green Version]
- Stevens, J.W.; Khunti, K.; Harvey, R.; Johnson, M.; Preston, L.; Woods, H.B.; Davies, M.; Goyder, E. Preventing the progression to type 2 diabetes mellitus in adults at high risk: A systematic review and network meta-analysis of lifestyle, pharmacological and surgical interventions. Diabetes Res. Clin. Pract. 2015, 107, 320–331. [Google Scholar] [CrossRef]
- Tabak, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimaki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2012, 35 (Suppl. 1), S64–S71. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Saver, J.L.; Hong, K.S.; Song, S.; Chang, K.H.; Ovbiagele, B. Effect of pre-diabetes on future risk of stroke: Meta-analysis. BMJ 2012, 344, e3564. [Google Scholar] [CrossRef] [Green Version]
- Vilanova, M.B.; Falguera, M.; Marsal, J.R.; Rubinat, E.; Alcubierre, N.; Castelblanco, E.; Granado-Casas, M.; Miro, N.; Mollo, A.; Mata-Cases, M.; et al. Prevalence, clinical features and risk assessment of pre-diabetes in Spain: The prospective Mollerussa cohort study. BMJ Open 2017, 7, e015158. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Canada Clinical Practice Guidelines Expert Committee; Punthakee, Z.; Goldenberg, R.; Katz, P. Definition, Classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Can. J. Diabetes 2018, 42 (Suppl. 1), S10–S15. [Google Scholar] [CrossRef] [Green Version]
- Mann, D.M.; Carson, A.P.; Shimbo, D.; Fonseca, V.; Fox, C.S.; Muntner, P. Impact of A1C screening criterion on the diagnosis of pre-diabetes among U.S. adults. Diabetes Care 2010, 33, 2190–2195. [Google Scholar] [CrossRef] [Green Version]
- Rosella, L.C.; Lebenbaum, M.; Fitzpatrick, T.; Zuk, A.; Booth, G.L. Prevalence of Prediabetes and Undiagnosed Diabetes in Canada (2007–2011) According to Fasting Plasma Glucose and HbA1c Screening Criteria. Diabetes Care 2015, 38, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- NICE. Preventing Type 2 Diabetes: Risk Identification and Interventions for Individuals at High Risk; NICE Public Health Guidance: London, UK, 2012. [Google Scholar]
- Kim, C.H.; Kim, H.K.; Kim, E.H.; Bae, S.J.; Choe, J.; Park, J.Y. Risk of progression to diabetes from prediabetes defined by HbA1c or fasting plasma glucose criteria in Koreans. Diabetes Res. Clin. Pract. 2016, 118, 105–111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus. Abbreviated Report of a WHO Consultation; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Warren, B.; Pankow, J.S.; Matsushita, K.; Punjabi, N.M.; Daya, N.R.; Grams, M.; Woodward, M.; Selvin, E. Comparative prognostic performance of definitions of prediabetes: A prospective cohort analysis of the Atherosclerosis Risk in Communities (ARIC) study. Lancet Diabetes Endocrinol. 2017, 5, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Yudkin, J.S.; Montori, V.M. The epidemic of pre-diabetes: The medicine and the politics. BMJ 2014, 349, g4485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, E.; Roberts, S.; Oke, J.; Vijayaraghavan, S.; Normansell, R.; Greenhalgh, T. Efficacy and effectiveness of screen and treat policies in prevention of type 2 diabetes: Systematic review and meta-analysis of screening tests and interventions. BMJ 2017, 356, i6538. [Google Scholar] [CrossRef] [Green Version]
- Sacks, D.B. A1C versus glucose testing: A comparison. Diabetes Care 2011, 34, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezquerra-Lazaro, I.; Cea-Soriano, L.; Giraldez-Garcia, C.; Ruiz, A.; Franch-Nadal, J.; Diez-Espino, J.; Nogales, P.; Carraminana, F.; Javier Sangros, F.; Regidor, E.; et al. Lifestyle factors do not explain the difference on diabetes progression according to type of prediabetes: Results from a Spanish prospective cohort of prediabetic patients. Diabetes Res. Clin. Pract. 2019, 153, 66–75. [Google Scholar] [CrossRef]
- Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, D.M.; Davidson, M.B.; DeFronzo, R.A.; Heine, R.J.; Henry, R.R.; Pratley, R.; Zinman, B.; American Diabetes, A. Impaired fasting glucose and impaired glucose tolerance: Implications for care. Diabetes Care 2007, 30, 753–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, B.; Hemmingsen, B.; Metzendorf, M.I.; Takwoingi, Y. Development of type 2 diabetes mellitus in people with intermediate hyperglycaemia. Cochrane Database Syst. Rev. 2018, 10, CD012661. [Google Scholar] [CrossRef] [PubMed]
- Heianza, Y.; Hara, S.; Arase, Y.; Saito, K.; Fujiwara, K.; Tsuji, H.; Kodama, S.; Hsieh, S.D.; Mori, Y.; Shimano, H.; et al. HbA1c 5.7–6.4% and impaired fasting plasma glucose for diagnosis of prediabetes and risk of progression to diabetes in Japan (TOPICS 3): A longitudinal cohort study. Lancet 2011, 378, 147–155. [Google Scholar] [CrossRef]
- Perreault, L.; Pan, Q.; Mather, K.J.; Watson, K.E.; Hamman, R.F.; Kahn, S.E.; Diabetes Prevention Program Research Group. Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: Results from the Diabetes Prevention Program Outcomes Study. Lancet 2012, 379, 2243–2251. [Google Scholar] [CrossRef] [Green Version]
- Vistisen, D.; Kivimaki, M.; Perreault, L.; Hulman, A.; Witte, D.R.; Brunner, E.J.; Tabak, A.; Jorgensen, M.E.; Faerch, K. Reversion from prediabetes to normoglycaemia and risk of cardiovascular disease and mortality: The Whitehall II cohort study. Diabetologia 2019, 62, 1385–1390. [Google Scholar] [CrossRef] [Green Version]
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C.; del Grupo de Determinantes Sociales de Sociedad Espanola de Epidemiología. Proposals for social class classification based on the Spanish National Classification of Occupations 2011 using neo-Weberian and neo-Marxist approaches. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; De Ridder, J. International Standards for Anthropometric Assessment; International Standards for Anthropometric Assessment (ISAK): Wellington, New Zeland, 2011. [Google Scholar]
- Carolina Giráldez-García, M.d.C.G.; Suárez, D.; Sánchez, L.G.; Mur, T.; Pujol, R.; Igual, D.; Malo, F.; Ibáñez, M.; Marín, M.T.; Buil, P.; et al. Evolución de pacientes con prediabetes en Atención Primaria de Salud (PREDAPS): Resultados del quinto año de seguimiento. Diabetes Práctica 2018, 9, 37–80. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Santaguida, P.; Raina, P.; Morrison, K.M.; Balion, C.; Hunt, D.; Yazdi, H.; Booker, L. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: A systematic overview and meta-analysis of prospective studies. Diabetes Res. Clin. Pract. 2007, 78, 305–312. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Bracco, P.A.; Yudkin, J.S.; Bensenor, I.M.; Griep, R.H.; Barreto, S.M.; Castilhos, C.D.; Duncan, B.B. Intermediate hyperglycaemia to predict progression to type 2 diabetes (ELSA-Brasil): An occupational cohort study in Brazil. Lancet Diabetes Endocrinol. 2019, 7, 267–277. [Google Scholar] [CrossRef]
- Vazquez, L.A.; Calvo-Bonacho, E.; Reviriego, J.; Garcia-Margallo, T.; Caveda, E.; Goday, A. Incidence of Diabetes in the Working Population in Spain: Results from the ICARIA Cohort. Diabetes Ther. 2019, 10, 57–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.M.Y.; Colagiuri, S.; Woodward, M.; Gregg, E.W.; Adams, R.; Azizi, F.; Gabriel, R.; Gill, T.K.; Gonzalez, C.; Hodge, A.; et al. Comparing different definitions of prediabetes with subsequent risk of diabetes: An individual participant data meta-analysis involving 76 513 individuals and 8208 cases of incident diabetes. BMJ Open Diabetes Res. Care 2019, 7, e000794. [Google Scholar] [CrossRef] [Green Version]
- Paulweber, B.; Valensi, P.; Lindstrom, J.; Lalic, N.M.; Greaves, C.J.; McKee, M.; Kissimova-Skarbek, K.; Liatis, S.; Cosson, E.; Szendroedi, J.; et al. A European evidence-based guideline for the prevention of type 2 diabetes. Horm. Metab. Res. 2010, 42 (Suppl. 1), S3–S36. [Google Scholar] [CrossRef] [Green Version]
- Selvin, E.; Steffes, M.W.; Gregg, E.; Brancati, F.L.; Coresh, J. Performance of A1C for the classification and prediction of diabetes. Diabetes Care 2011, 34, 84–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregg, E.W.; Li, Y.; Wang, J.; Burrows, N.R.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in diabetes-related complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Hemmingsen, B.; Sonne, D.P.; Metzendorf, M.I.; Richter, B. Dipeptidyl-peptidase (DPP)-4 inhibitors and glucagon-like peptide (GLP)-1 analogues for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk for the development of type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2017, 5, CD012204. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J.; Peltonen, M.; Eriksson, J.G.; Ilanne-Parikka, P.; Aunola, S.; Keinanen-Kiukaanniemi, S.; Uusitupa, M.; Tuomilehto, J.; Finnish Diabetes Prevention Study. Improved lifestyle and decreased diabetes risk over 13 years: Long-term follow-up of the randomised Finnish Diabetes Prevention Study (DPS). Diabetologia 2013, 56, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Jadhav, R.A.; Hazari, A.; Monterio, A.; Kumar, S.; Maiya, A.G. Effect of Physical Activity Intervention in Prediabetes: A Systematic Review with Meta-analysis. J. Phys. Act. Health 2017, 14, 745–755. [Google Scholar] [CrossRef]
- Boniol, M.; Dragomir, M.; Autier, P.; Boyle, P. Physical activity and change in fasting glucose and HbA1c: A quantitative meta-analysis of randomized trials. Acta Diabetol. 2017, 54, 983–991. [Google Scholar] [CrossRef] [Green Version]
- Zand, A.; Ibrahim, K.; Patham, B. Prediabetes: Why Should We Care? Methodist DeBakey Cardiovasc. J. 2018, 14, 289–297. [Google Scholar]
- Karve, A.; Hayward, R.A. Prevalence, diagnosis, and treatment of impaired fasting glucose and impaired glucose tolerance in nondiabetic U.S. adults. Diabetes Care 2010, 33, 2355–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chomistek, A.K.; Chiuve, S.E.; Eliassen, A.H.; Mukamal, K.J.; Willett, W.C.; Rimm, E.B. Healthy lifestyle in the primordial prevention of cardiovascular disease among young women. J. Am. Coll. Cardiol. 2015, 65, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Li, Y.; Hu, Y.; Zong, G.; Li, S.; Rimm, E.B.; Hu, F.B.; Manson, J.E.; Rexrode, K.M.; Shin, H.J.; et al. Influence of Lifestyle on Incident Cardiovascular Disease and Mortality in Patients with Diabetes Mellitus. J. Am. Coll. Cardiol. 2018, 71, 2867–2876. [Google Scholar] [CrossRef] [PubMed]
- Ayensa-Vazquez, J.A.; Leiva, A.; Tauler, P.; Lopez-Gonzalez, A.A.; Aguilo, A.; Tomas-Salva, M.; Bennasar-Veny, M. Agreement between Type 2 Diabetes Risk Scales in a Caucasian Population: A Systematic Review and Report. J Clin Med. 2020, 9, 1546. [Google Scholar] [CrossRef]
- Hernan, M.A.; Hernandez-Diaz, S.; Robins, J.M. A structural approach to selection bias. Epidemiology 2004, 15, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Lajous, M.; Bijon, A.; Fagherazzi, G.; Boutron-Ruault, M.C.; Balkau, B.; Clavel-Chapelon, F.; Hernan, M.A. Body mass index, diabetes, and mortality in French women: Explaining away a “paradox”. Epidemiology 2014, 25, 10–14. [Google Scholar] [CrossRef]
- Unwin, N.; Shaw, J.; Zimmet, P.; Alberti, K.G. Impaired glucose tolerance and impaired fasting glycaemia: The current status on definition and intervention. Diabet. Med. 2002, 19, 708–723. [Google Scholar] [CrossRef]
- Perry, R.C.; Shankar, R.R.; Fineberg, N.; McGill, J.; Baron, A.D.; Early Diabetes Intervention Program. HbA1c measurement improves the detection of type 2 diabetes in high-risk individuals with nondiagnostic levels of fasting plasma glucose: The Early Diabetes Intervention Program (EDIP). Diabetes Care 2001, 24, 465–471. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Normoglycemia FPG < 100 mg/dL (n = 173,796) | Prediabetes FPG 100–125 mg/dL (n = 27,844) | Diabetes FPG ≥ 126 mg/dL (n = 33,355) | p Value |
|---|---|---|---|---|
| Sex (male) | 95,414 (54.9%) | 20,131 (72.3%) | 21,781 (65.3%) | <0.001 |
| Age (years) | 38.07 ± 10.19 | 44.62 ± 10.04 | 47.38 ± 9.23 | <0.001 |
| Social status Blue-collar | 122,700 (70.6%) | 21,329 (76.6%) | 25,016 (75.0%) | <0.001 |
| BMI (kg/m2) | 25.20 ± 4.26 | 27.79 ± 4.82 | 29.69 ± 5.02 | <0.001 |
| BMI categories | ||||
| Overweight | 57,874 (33.3%) | 11,973 (43.0%) | 15,710 (47.1%) | <0.001 |
| Obesity | 21,725 (12.5%) | 7713 (27.7%) | 13,642 (40.9%) | |
| WC (cm) | 82.10 ± 10.47 | 87.01 ± 10.48 | 87.67 ± 10.58 | <0.001 |
| SBP (mmHg) | 120.19 ± 15.32 | 127.65 ± 17.09 | 130.92 ± 17.94 | <0.001 |
| DBP (mmHg) | 73.04 ± 10.45 | 78.17 ± 11.18 | 80.14 ± 11.46 | <0.001 |
| Hypertension | 25,374 (14.6%) | 8214 (29.5%) | 12,541 (37.6%) | <0.001 |
| FPG (mg/dL) | 84.62 ± 9.39 | 106.24 ± 5.86 | 109.25 ± 41.63 | <0.001 |
| TG (mg/dL) | 102.40 ± 62.92 | 136.64 ± 104.10 | 147.81 ± 101.04 | <0.001 |
| High TG | 9733 (5.6%) | 3954 (14.2%) | 5537 (16.6%) | <0.001 |
| Total Cholesterol (mg/dL) | 188.51 ± 36.19 | 203.63 ± 38.60 | 202.78 ± 36.26 | <0.001 |
| High Cholesterol | 14,773 (8.5%) | 3487 (16.5%) | 4670 (14.0%) | <0.001 |
| Smoking status | ||||
| Former smoker | 15,642 (9.0%) | 4260 (15.3%) | 7772 (23.3%) | <0.001 |
| Current smoker | 59,438 (34.2%) | 9189 (33.0%) | 9306 (27.9%) |
| Variables | Normalized (n = 8404) | Persisted (n = 9531) | Progressed (n = 5358) | p Value |
|---|---|---|---|---|
| Age (years) | 42.14 ± 10.14 | 44.41 ± 9.47 | 48.65 ± 8.78 | <0.001*,‡,† |
| Male (%) | 5925 (70.5%) | 7154 (75.1%) | 3913 (73.0%) | <0.001* |
| Blue-collar | 7942 (94.5%) | 9050 (95.0%) | 5146 (96.0%) | 0.130 |
| Smoking status | ||||
| Former smoker | 910 (10.8%) | 1606 (16.9%) | 1041 (19.4%) | <0.001*,‡,† |
| Current smoker | 3034 (36.1%) | 3294 (34.6%) | 1407 (26.3%) | |
| PA (≥150 min/week) | 5777 (68.7%) | 2958 (31.0%) | 61 (1.1%) | <0.001*,‡,† |
| Diet (daily fruits and vegetables) | 5170 (61.5%) | 2968 (31.1%) | 403 (7.5%) | <0.001*,‡,† |
| BMI (kg/m2) | 25.09 ± 3.24 | 26.98 ± 3.58 | 33.42 ± 4.09 | <0.001*,‡,† |
| FPG (mg/dL) | 104.65 ± 4.73 | 106.37 ± 5.79 | 108.50 ± 6.73 | <0.001*,‡,† |
| HbA1c (%) | 5.892 ± 0.19 | 5.89 ± 0.17 | 6.20 ± 0.16 | <0.001*,‡,† |
| SBP (mmHg) | 123.76 ± 16.21 | 127.25 ± 16.25 | 134.72 ± 17.5 | <0.001*,‡,† |
| DBP (mmHg) | 75.39 ± 10.69 | 78.13 ± 10.78 | 82.75 ± 11.1 | <0.001*,‡,† |
| TG (mg/dL) | 108.56 ± 72.55 | 145.32 ± 116.72 | 166.84 ± 112.79 | <0.001*,‡,† |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennasar-Veny, M.; Fresneda, S.; López-González, A.; Busquets-Cortés, C.; Aguiló, A.; Yañez, A.M. Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes. Nutrients 2020, 12, 1538. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051538
Bennasar-Veny M, Fresneda S, López-González A, Busquets-Cortés C, Aguiló A, Yañez AM. Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes. Nutrients. 2020; 12(5):1538. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051538
Chicago/Turabian StyleBennasar-Veny, Miquel, Sergio Fresneda, Arturo López-González, Carla Busquets-Cortés, Antoni Aguiló, and Aina M. Yañez. 2020. "Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes" Nutrients 12, no. 5: 1538. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12051538