Dietary Diversity among Chinese Residents during the COVID-19 Outbreak and Its Associated Factors

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Ethics
2.4. Statistics
2.5. Heat Map
3. Results
3.1. Household Dietary Diversity Score (HDDS) Status of Participants
3.2. HDDS among Participants with Different Socio-Demographic Characteristics
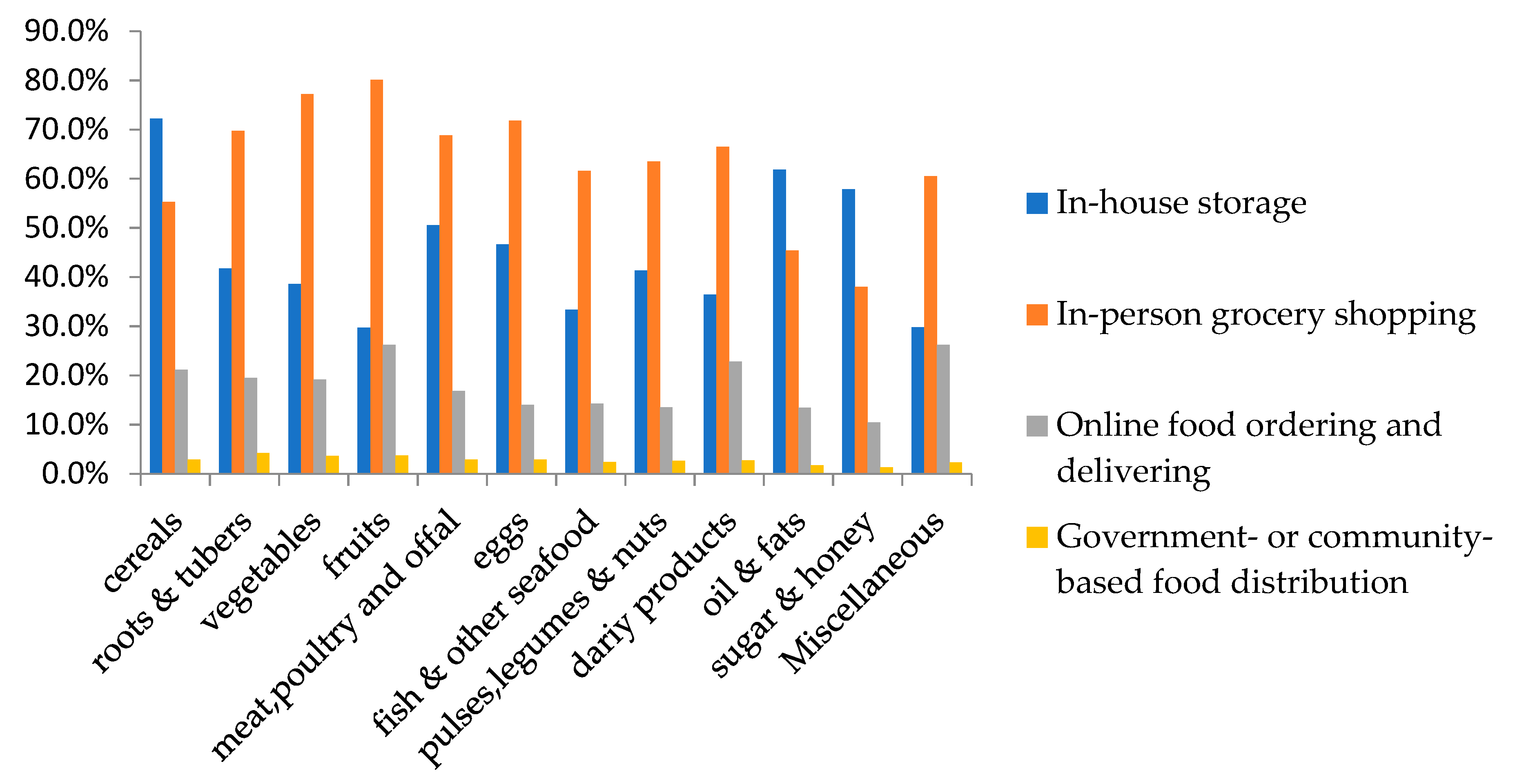
3.3. Sources for Obtaining and Purchasing Foods during Isolation Period
3.4. Dietary Behaviors Coped with COVID-19
3.5. Factors Associated with HDDS
4. Discussion
4.1. Dietary Diversity in Participants
4.2. Factors Associated with Dietary Diversity
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chin. J. Epidemiol. 2020, 41, 145–151. [Google Scholar]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Boil. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 16 April 2020).
- United Nations. Shared Responsibility, Global Solidarity: Responding to the Socio-Economic Impacts of COVID-19. Available online: https://www.un.org/en/un-coronavirus-communications-team/launch-report-socio-economic-impacts-covid-19 (accessed on 1 April 2020).
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemilä, H. Vitamin C and Infections. Nutrients 2017, 9, 339. [Google Scholar] [CrossRef] [Green Version]
- Markowiak, P.; Śliżewska, K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients 2017, 9, 1021. [Google Scholar] [CrossRef]
- Swindale, A.; Bilinsky, P. Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide VERSION 2. Academy for Educational Development; FANTA: Washington, DC, USA, 2006. [Google Scholar]
- Chandra, S.; Chandra, R.K. Nutrition, immune response, and outcome. Prog. Food Nutr. Sci. 1986, 10, 1–65. [Google Scholar]
- Center for Disease Control and Prevention, Outbreaks Can Be Stressful. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fprepare%2Fmanaging-stress-anxiety.html (accessed on 1 April 2020).
- EnfoDesk. Chinese Restaurant Super Digital Time Insight 2020. Available online: https://www.analysys.cn/article/analysis/detail/20019629 (accessed on 1 April 2020).
- Beijing Youth Daily. The Vast Majority of Express Delivery Companies across China Resumed Normal Work. Available online: http://www.xinhuanet.com/info/2020-02/11/c_138772679.htm (accessed on 1 April 2020).
- Chinese Center for Disease Control and Prevention. The Distribution of COVID-19. Available online: http://2019ncov.chinacdc.cn/2019-nCoV/Discussion (accessed on 1 April 2020).
- The R Project for Statistical Computing. Available online: https://www.r-project.org/. (accessed on 5 April 2020).
- World Health Organization. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---6-april-2020 (accessed on 6 April 2020).
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. Social Capital and Sleep Quality in Individuals Who Self-Isolated for 14 Days During the Coronavirus Disease 2019 (COVID-19) Outbreak in January 2020 in China. Med Sci. Monit. 2020, 26, e923921. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- National Health Commission of China, Dietary Guidelines for the Prevention and Treatment of Novel Coronavirus. Available online: http://www.nhc.gov.cn/xcs/fkdt/202002/a69fd36d54514c5a9a3f456188cbc428.shtml (accessed on 1 April 2020).
- World Health Organization. Coping with Stress during the 2019-nCov Outbreak. Available online: https://www.who.int/docs/default-source/coronaviruse/coping-with-stress.pdf?sfvrsn=9845bc3a_8 (accessed on 1 April 2020).
- Mahmudiono, T.; Sumarmi, S.; Rosenkranz, R.R. Household dietary diversity and child stunting in East Java, Indonesia. Asia Pac. J. Clin. Nutr. 2017, 26, 317–325. [Google Scholar]
- Chakona, G.; Shackleton, C.M. Household Food Insecurity along an Agro-Ecological Gradient Influences Children’s Nutritional Status in South Africa. Front. Nutr. 2018, 4, 72. [Google Scholar] [CrossRef] [Green Version]
- Habte, T.-Y.; Krawinkel, M. Dietary Diversity Score: A Measure of Nutritional Adequacy or an Indicator of Healthy Diet? J. Nutr. Heal. Sci. 2016, 3, 303. [Google Scholar]
- Decker, D.; Flynn, M. Food Insecurity and Chronic Disease: Addressing Food Access as a Healthcare Issue. Rhode Isl. Med. J. 2018, 101, 28–30. [Google Scholar]
- Darapheak, C.; Takano, T.; Kizuki, M.; Nakamura, K.; Ishii, H. Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. Int. Arch. Med. 2013, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Anthony, F. Characterization of the Degree of Food Processing in Relation with Its Health Potential and Effects, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volume 3, pp. 79–129. [Google Scholar]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Hongyi, C.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020. online ahead of print. [Google Scholar] [CrossRef]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Du, W.W.; Jia, X.F.; Jiang, H.R.; Wang, Y.; Li, L.; Zhang, B. Consumption of dried legume and legume products among adults aged 18–59 years old in 15 provinces of China in 2015. Acta Nutr. Sinca 2018, 40, 17–22. [Google Scholar]
- Su, C.; Wang, Z.H.; Jia, X.F.; Zhang, B.; Ding, G.Q. Consumption of marine food consumption among adults aged 18–59 years old in 15 provinces of China in 2015. Acta Nutr. Sinca 2018, 1, 23–26. [Google Scholar]
- Ma, G. Food, eating behavior, and culture in Chinese society. J. Ethn. Foods 2015, 2, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Guangming Daily. Wuhan: Ensure Household Has Fresh Fish. Available online: http://special.chinadevelopment.com.cn/2020zt/xgfyjjz/yqzj/2020/03/1629097.shtml (accessed on 1 April 2020).
- Rochfort, S.; Panozzo, J. Phytochemicals for Health, the Role of Pulses. J. Agric. Food Chem. 2007, 55, 7981–7994. [Google Scholar] [CrossRef] [PubMed]
- Mudryj, A.N.; Yu, N.; Aukema, H.M. Nutritional and health benefits of pulses. Appl. Physiol. Nutr. Metab. 2014, 39, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Anon. Ebola in Liberia: Impact on Food Security and Livelihoods. Action against Hunger UK. 2015. Available online: https://www.actionagainsthunger.org.uk (accessed on 1 April 2020).
- Anon. Ebola to Worsen Food Security Conditions in Liberia, Sierra Leone and Guinea. Available online: https://ec.europa.eu/jrc/en/news/ebola-worsen-food-security-conditions-liberia-sierra-leone-and-guinea (accessed on 14 April 2020).
- Chinese State Administration for Market Regulation. Notice of Market Regulation on Further Strengthening Food Safety Supervision during the Prevention and Control of the COVID-19. Available online: http://www.samr.gov.cn/spjys/tzgg/202002/t20200211_311452.html (accessed on 1 April 2020).
- Lau, J.T.; Yang, X.; Tsui, H.; Kim, J. Impacts of SARS on health-seeking behaviors in general population in Hong Kong. Prev. Med. 2005, 41, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Sohu News. Smoking, Alcohol Drinking Cannot Help for Preventing the Corona Virus. Available online: https://www.sohu.com/a/368530580_162522 (accessed on 1 April 2020).
- Malekian, S. Iran Confronts Deadly Alcohol Crisis in Midst of Dealing with Coronavirus. Available online: https://abcnews.go.com/Health/iran-confronts-deadly-alcohol-crisis-midst-dealing-coronavirus/story?id=69842613 (accessed on 14 April 2020).
- Huang, G.B.; Zhang, Y.L.; Wang, F.R. Help-seeking pattern of college students during the time of severe acute respiratory syndrome. Chin. J. Clin. Rehabil. 2004, 8, 5966–5968. [Google Scholar]
- Vellema, W.; Desiere, S.; Dhaese, M. Verifying Validity of the Household Dietary Diversity Score: An Application of Rasch Modeling. Food Nutr. Bull. 2016, 37, 27–41. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Food Groups | Consumed | Not-Consumed |
|---|---|---|
| Cereals | 1896 (97.8) | 42 (2.2) |
| Tubers and roots | 1549 (79.9) | 389 (20.1) |
| Vegetables | 1913 (98.7) | 225 (1.3) |
| Fruits | 1823 (94.1) | 115 (5.9) |
| Meat, poultry and offal | 1547 (79.8) | 391 (20.2) |
| Fish and other seafood | 1110 (57.2) | 828 (42.7) |
| Eggs | 1801 (92.9) | 137 (7.1) |
| Pulses, legumes, and nuts | 1360 (70.1) | 578 (29.8) |
| Dairy products | 1545 (79.7) | 393 (20.3) |
| Oils and fats | 1817 (93.7) | 121 (6.2) |
| Sugar and honey | 1345 (69.4) | 593 (30.6) |
| Miscellaneous a | 1103 (56.9) | 835 (43.1) |
| n (%) | HDDS (Mean ± SD) b | p | ||
|---|---|---|---|---|
| Gender | Male | 665 (34.3) | 9.68 ± 2.61 | 0.275 |
| Female | 1273 (65.7) | 9.72 ± 2.04 | ||
| Age group(y) | 18–45 | 1620 (83.6) | 9.65 ± 2.10 | <0.001 |
| >45 | 318 (16.4) | 9.97 ± 1.89 | ||
| Education level | Senior high school or under | 219 (11.3) | 9.60 ± 2.23 | 0.121 |
| Bachelor degree | 1464 (75.5) | 9.76 ± 2.03 | ||
| Master degree or above | 255 (13.2) | 9.49 ± 2.08 | ||
| Family annual income (Chinese yuan) | <30 thousands | 206 (10.6) | 8.98 ± 2.43 | <0.001 a |
| 30–100 thousands | 690 (35.6) | 9.69 ± 2.02 | ||
| 100–300 thousands | 750 (38.7) | 9.80 ± 1.97 | ||
| >300 thousands | 292 (15.1) | 10.02 ± 2.06 | ||
| Family size (people living in the same household during isolation) | <3 | 979 (50.5) | 9.73 ± 1.97 | 0.887 |
| 3–5 | 760 (39.2) | 9.68 ± 2.09 | ||
| >5 | 197 (10.2) | 9.68 ± 2.41 | ||
| Geographic Region | Urban | 414(21.4) | 9.78 ± 2.04 | 0.003 |
| Rural | 1524(78.6) | 9.44 ± 2.15 | ||
| Pregnant or lactating women in the household | Yes | 44 (2.3) | 9.80 ± 2.37 | 0.770 |
| No | 1894 (97.7) | 9.70 ± 2.06 | ||
| <5 y children in the household | Yes | 325 (16.8) | 9.86 ± 2.12 | 0.143 |
| No | 1613 (83.2) | 9.67 ± 2.05 | ||
| >65 y elders in the household | Yes | 805 (41.5) | 9.70 ± 2.06 | 0.262 |
| No | 1133 (58.5) | 9.66 ± 2.03 |
| n (%) | OR (95% CI) | ORadjust1 (95% CI) a | ||
|---|---|---|---|---|
| Participants characteristics | ||||
| Geographic regions by case number | <500case/province b | 987 (50.9) | 1 | 1 |
| >500case/province b | 862 (44.5) | 0.84 (0.70, 1.01) | 0.79 (0.65, 0.96) | |
| Hubei | 89 (4.6) | 0.58 (0.38, 0.90) | 0.60 (0.39, 0.93) | |
| Status during isolation | Self-isolation | 1254 (64.7) | 1 | |
| Working outside | 684 (35.3) | 1.04 (0.86, 1.25) | 0.95 (0.78, 1.15) | |
| Total of going out times | 0–2×/week | 401 (20.7) | 1 | 1 |
| 3–4×/week | 916 (47.3) | 1.13 (0.89, 1.43) | 1.06 (0.84, 1.35) | |
| ≥5×/week | 621 (32.0) | 1.01 (0.78, 1.30) | 0.91 (0.70, 1.78) | |
| Frequencies of going out for food purchase | 0–2×/week | 417 (21.5) | 1 | 1 |
| 3–4×/week | 1125 (58.0) | 1.20 (0.96, 1.51) | 1.15 (0.92, 1.45) | |
| ≥5×/week | 396 (20.4) | 1.06 (0.80, 1.40) | 0.97 (0.74, 1.29) | |
| Food purchasing behaviors c | ||||
| Cluster1 | 320 (16.5) | 1 | 1 | |
| Cluster2 | 752 (38.8) | 1.03 (0.79, 1.34) | 1.03(0.79, 1.35) | |
| Cluster3 | 866 (44.7) | 1.12 (0.87, 1.45) | 1.11(0.86, 1.44) | |
| Dietary behaviors in COVID-19 d | ||||
| Reported dietary behaviors to cope with COVID-19 | No | 126 (62.7) | 1 | 1 |
| Yes | 722 (37.2) | 1.27 (1.05, 1.53) | 1.23 (1.02, 1.45) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, A.; Li, Z.; Ke, Y.; Huo, S.; Ma, Y.; Zhang, Y.; Zhang, J.; Ren, Z. Dietary Diversity among Chinese Residents during the COVID-19 Outbreak and Its Associated Factors. Nutrients 2020, 12, 1699. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061699
Zhao A, Li Z, Ke Y, Huo S, Ma Y, Zhang Y, Zhang J, Ren Z. Dietary Diversity among Chinese Residents during the COVID-19 Outbreak and Its Associated Factors. Nutrients. 2020; 12(6):1699. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061699
Chicago/Turabian StyleZhao, Ai, Zhongyu Li, Yalei Ke, Shanshan Huo, Yidi Ma, Yumei Zhang, Jian Zhang, and Zhongxia Ren. 2020. "Dietary Diversity among Chinese Residents during the COVID-19 Outbreak and Its Associated Factors" Nutrients 12, no. 6: 1699. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061699