Anti-Heartburn Effects of Sugar Cane Flour: A Double-Blind, Randomized, Placebo-Controlled Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
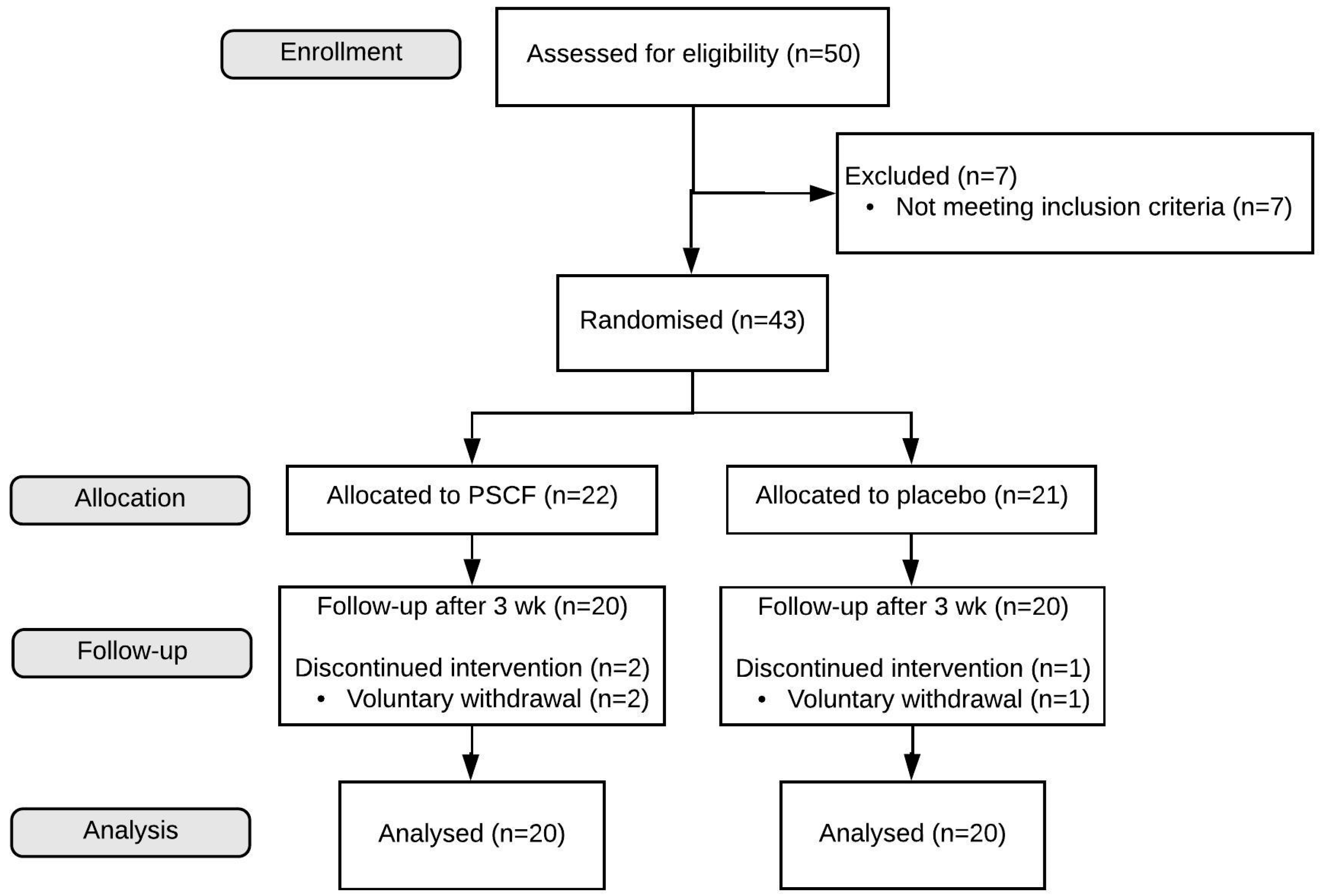
3. Results
3.1. Demographics and Baseline
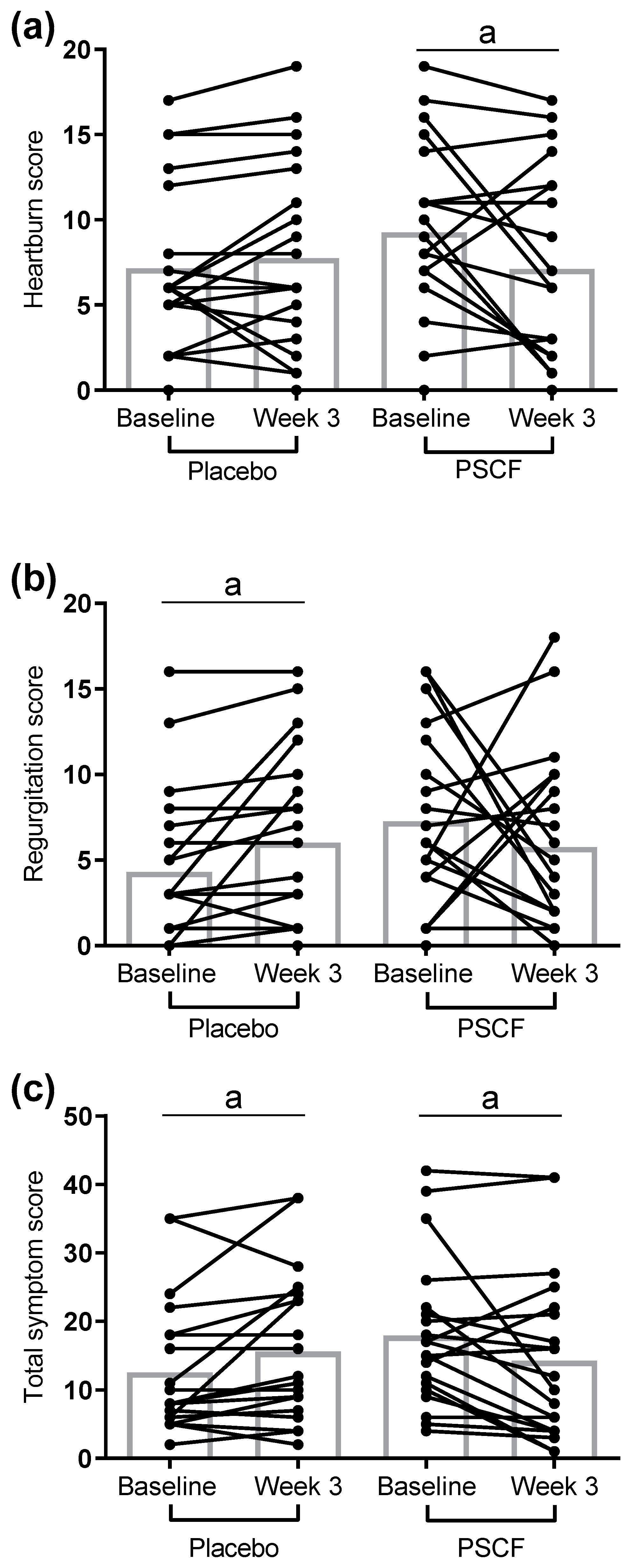
3.2. Changes after Three Weeks
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Sandhu, D.S.; Fass, R. Current trends in the management of gastroesophageal reflux disease. Gut Liver 2018, 12, 7–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morozov, S.; Isakov, V.; Konovalova, M. Fiber-enriched diet helps to control symptoms and improves esophageal motility in patients with non-erosive gastroesophageal reflux disease. World J. Gastroenterol. 2018, 24, 2291–2299. [Google Scholar] [CrossRef]
- Ronkainen, J.; Aro, P.; Storskrubb, T.; Lind, T.; Bolling-Sternevald, E.; Junghard, O.; Talley, N.J.; Agreus, L. Gastro-oesophageal reflux symptoms and health-related quality of life in the adult general population—The kalixanda study. Aliment. Pharmacol. Ther. 2006, 23, 1725–1733. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.; Wong, C.; Pollack, A. Gastro-oesophageal reflux disease (gord) in australian general practice patients. Aust. Fam. Physician 2015, 44, 701. [Google Scholar] [PubMed]
- Lagergren, J.; Bergström, R.; Lindgren, A.; Nyrén, O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N. Engl. J. Med. 1999, 340, 825–831. [Google Scholar] [CrossRef]
- Shaker, R.; Castell, D.O.; Schoenfeld, P.S.; Spechler, S.J. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: The results of a gallup survey conducted on behalf of the american gastroenterological association. Am. J. Gastroenterol. 2003, 98, 1487–1493. [Google Scholar] [CrossRef]
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 2013, 108, 308–328, quiz 329. [Google Scholar] [CrossRef]
- Wang, Y.-K.; Hsu, W.-H.; Wang, S.S.W.; Lu, C.-Y.; Kuo, F.-C.; Su, Y.-C.; Yang, S.-F.; Chen, C.-Y.; Wu, D.-C.; Kuo, C.-H. Current pharmacological management of gastroesophageal reflux disease. Gastroenterol. Res. Pract. 2013, 2013, 12. [Google Scholar] [CrossRef]
- Ang, D.; How, C.H.; Ang, T.L. Persistent gastro-oesophageal reflux symptoms despite proton pump inhibitor therapy. Singap. Med. J. 2016, 57, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, Y.; Ishimura, N.; Ishihara, S. Advantages and disadvantages of long-term proton pump inhibitor use. J. Neurogastroenterol. Motil. 2018, 24, 182–196. [Google Scholar] [CrossRef]
- Müller, M.; Canfora, E.E.; Blaak, E.E. Gastrointestinal transit time, glucose homeostasis and metabolic health: Modulation by dietary fibers. Nutrients 2018, 10, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emerenziani, S.; Sifrim, D. Gastroesophageal reflux and gastric emptying, revisited. Curr. Gastroenterol. Rep. 2005, 7, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Holloway, R.H.; Hongo, M.; Berger, K.; McCallum, R.W. Gastric distention: A mechanism for postprandial gastroesophageal reflux. Gastroenterology 1985, 89, 779–784. [Google Scholar] [CrossRef]
- Kahrilas, P.J.; Shi, G.; Manka, M.; Joehl, R.J. Increased frequency of transient lower esophageal sphincter relaxation induced by gastric distention in reflux patients with hiatal hernia. Gastroenterology 2000, 118, 688–695. [Google Scholar] [CrossRef]
- Harju, E. Guar gum benefits duodenal ulcer patients by decreasing gastric acidity and rate of emptying of gastric contents 60 to 120 min postprandially. Am. Surg. 1984, 50, 668–672. [Google Scholar]
- Edwards, G.; Ball, M. Dietary Supplement for the Treatment of Acid Reflux and Gastro-Oesophageal Reflux Disease (GORD/GERD). U.S. Patent US20190054136, 21 February 2019. [Google Scholar]
- Pluschke, A.M.; Feng, G.; Williams, B.A.; Gidley, M.J. Partial replacement of meat by sugar cane fibre: Cooking characteristics, sensory properties of beef burgers and in vitro fermentation of sugar cane fibre. Int. J. Food Sci. Technol. 2019, 54, 1760–1768. [Google Scholar] [CrossRef]
- Shinde, T.; Perera, A.P.; Vemuri, R.; Gondalia, S.V.; Karpe, A.V.; Beale, D.J.; Shastri, S.; Southam, B.; Eri, R.; Stanley, R. Synbiotic supplementation containing whole plant sugar cane fibre and probiotic spores potentiates protective synergistic effects in mouse model of ibd. Nutrients 2019, 11, 818. [Google Scholar] [CrossRef] [Green Version]
- Australian and New Zealand Clinical Trials Registry [Internet]: Sydney (NSW): NHMRC Clinical Trials Centre, University of Sydney (Australia); 2005—Identifier ACTRN12619001204134. Efficacy of Kfibre™ in Combating Gastroesophageal Reflux Disease Preliminary Human Clinical Study. Available online: www.anzctr.org.au/ACTRN12619001204134.aspx (accessed on 17 June 2020).
- Zavala-Gonzáles, M.A.; Azamar-Jacome, A.A.; Meixueiro-Daza, A.; De La Medina, A.R. Validation and diagnostic usefulness of gastroesophageal reflux disease questionnaire in a primary care level in mexico. J. Neurogastroenterol. Motil. 2014, 20, 475–482. [Google Scholar]
- El-Serag, H.; Satia, J.; Rabeneck, L. Dietary intake and the risk of gastro-oesophageal reflux disease: A cross sectional study in volunteers. Gut 2005, 54, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, M.; Johnsen, R.; Ye, W.; Hveem, K.; Lagergren, J. Lifestyle related risk factors in the aetiology of gastro-oesophageal reflux. Gut 2004, 53, 1730–1735. [Google Scholar] [CrossRef] [Green Version]
- Fass, R.; Shapiro, M.; Dekel, R.; Sewell, J. Systematic review: Proton-pump inhibitor failure in gastro-oesophageal reflux disease—Where next? Aliment. Pharmacol. Ther. 2005, 22, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Stefanidis, D.; Hope, W.W.; Kohn, G.P.; Reardon, P.R.; Richardson, W.S.; Fanelli, R.D.; Committee, S.G. Guidelines for surgical treatment of gastroesophageal reflux disease. Surg. Endosc. 2010, 24, 2647–2669. [Google Scholar] [CrossRef] [PubMed]
- Patrick, L. Gastroesophageal reflux disease (gerd): A review of conventional and alternative treatments. Altern. Med. Rev. 2011, 16, 116–133. [Google Scholar] [PubMed]
- DiSilvestro, R.A.; Verbruggen, M.A.; Offutt, E.J. Anti-heartburn effects of a fenugreek fiber product. Phytother. Res. 2011, 25, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.; Green, H. Dietary fibre and satiety. Nutr. Bull. 2007, 32, 32–42. [Google Scholar] [CrossRef]
- McIntyre, A.; Vincent, R.; Perkins, A.; Spiller, R. Effect of bran, ispaghula, and inert plastic particles on gastric emptying and small bowel transit in humans: The role of physical factors. Gut 1997, 40, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Vincent, R.; Roberts, A.; Frier, M.; Perkins, A.; MacDonald, I.; Spiller, R. Effect of bran particle size on gastric emptying and small bowel transit in humans: A scintigraphic study. Gut 1995, 37, 216–219. [Google Scholar] [CrossRef] [Green Version]
- Perera, C.O.; Hallett, I.C.; Nguyen, T.T.; Charles, J.C. Calcium oxalate crystals: The irritant factor in kiwifruit. J. Food Sci. 1990, 55, 1066–1069. [Google Scholar] [CrossRef]
- Ray, T.K.; Mansell, K.M.; Knight, L.; Malmud, L.; Owen, O.; Boden, G. Long-term effects of dietary fiber on glucose tolerance and gastric emptying in noninsulin-dependent diabetic patients. Am. J. Clin. Nutr. 1983, 37, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Karamanolis, G.; Tack, J. Nutrition and motility disorders. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 485–505. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Placebo (n = 20) | PSCF (n = 20) | p Value |
|---|---|---|---|
| Gender, n (%) | |||
| Male | 6 (30) | 8 (40) | |
| Female | 14 (70) | 12 (60) | |
| Age, years | 41.0 ± 12.9 | 51.1 ± 10.4 | 0.009 |
| Height, cm | 167 ± 7 | 169 ± 7 | 0.425 |
| Weight, kg | 91 ± 23 | 90 ± 24 | 0.880 |
| Body mass index, kg/m2 | 32 ± 9 | 33 ± 9 | 0.878 |
| Smoking, yes % | 35 | 40 | 1.000 |
| GERD-HRQL scores | |||
| Heartburn | 7.2 ± 4.8 | 9.3 ± 5.1 | 0.187 |
| Regurgitation | 4.3 ± 4.5 | 7.3 ± 5.1 | 0.039 |
| Total | 12.6 ± 10.0 | 17.9 ± 10.7 | 0.109 |
| Symptom | Placebo (n = 20) | PSCF (n = 20) | p Value |
|---|---|---|---|
| Heartburn, n (%) | |||
| Improved | 5 (25) | 13 (65) | 0.039 |
| Unchanged | 4 (20) | 2 (10) | |
| Worsened | 11 (55) | 5 (25) | |
| Regurgitation, n (%) | |||
| Improved | 1 (5) | 11 (55) | 0.001 |
| Unchanged | 9 (45) | 2 (10) | |
| Worsened | 10 (50) | 7 (35) | |
| Total score, n (%) | |||
| Improved | 4 (20) | 13 (65) | 0.015 |
| Unchanged | 3 (15) | 1 (5) | |
| Worsened | 13 (65) | 6 (30) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beckett, J.M.; Singh, N.K.; Phillips, J.; Kalpurath, K.; Taylor, K.; Stanley, R.A.; Eri, R.D. Anti-Heartburn Effects of Sugar Cane Flour: A Double-Blind, Randomized, Placebo-Controlled Study. Nutrients 2020, 12, 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061813
Beckett JM, Singh NK, Phillips J, Kalpurath K, Taylor K, Stanley RA, Eri RD. Anti-Heartburn Effects of Sugar Cane Flour: A Double-Blind, Randomized, Placebo-Controlled Study. Nutrients. 2020; 12(6):1813. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061813
Chicago/Turabian StyleBeckett, Jeffrey M., Neeraj K. Singh, Jehan Phillips, Krishnakumar Kalpurath, Kent Taylor, Roger A. Stanley, and Rajaraman D. Eri. 2020. "Anti-Heartburn Effects of Sugar Cane Flour: A Double-Blind, Randomized, Placebo-Controlled Study" Nutrients 12, no. 6: 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061813