Complementary Feeding in Preterm Infants: A Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
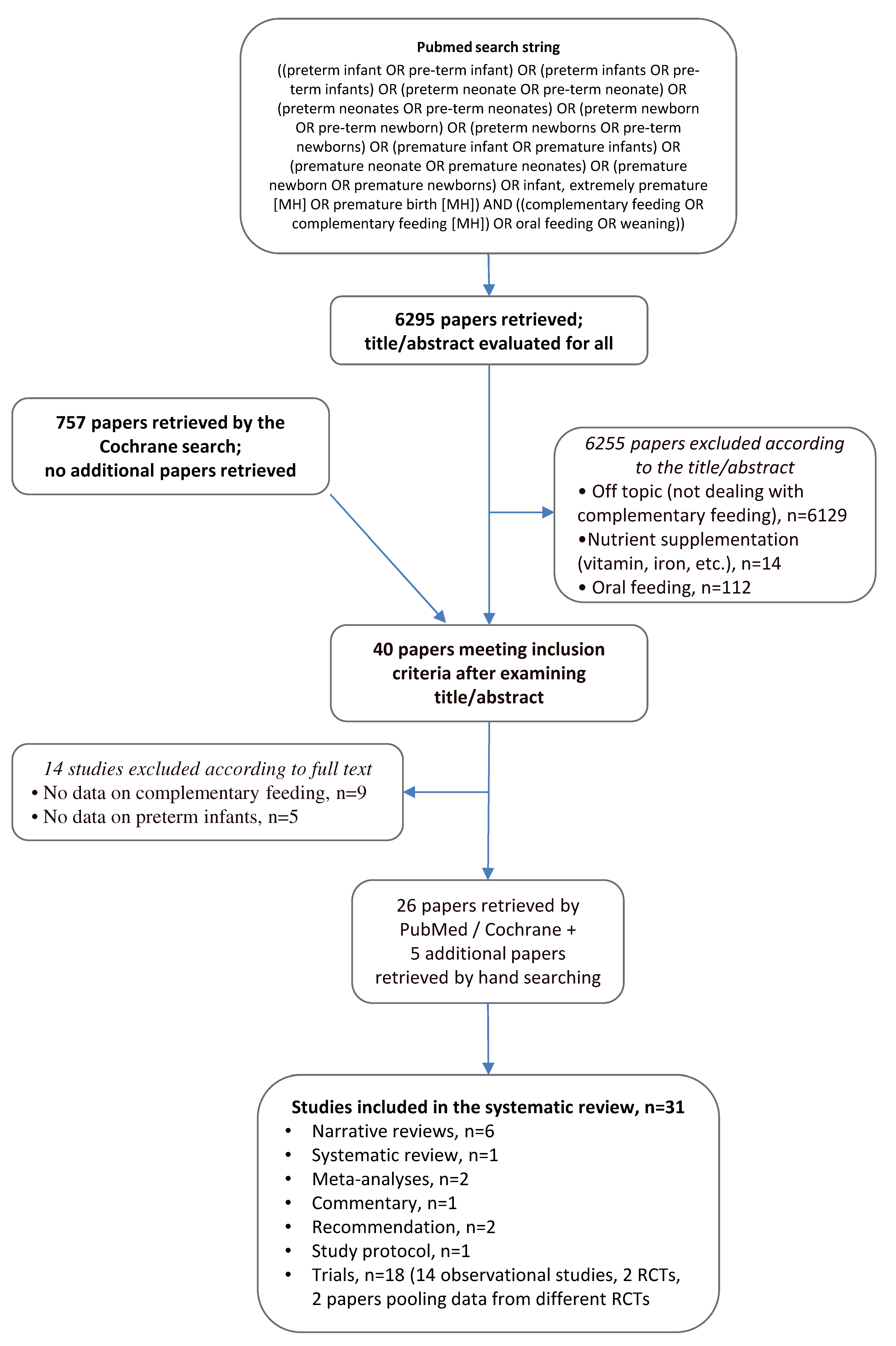
Literature Search
3. Results
Literature Search
4. Discussion
4.1. Timing and Quality of Complementary Feeding
4.2. Complementary Feeding and Clinical Outcome
4.3. Currently Available Recommendations on CF
4.4. Complementary Feeding Strategies for Infants with Oral Dysfunctions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schwarzenberg, S.J.; Georgieff, M.K. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO) Complementary Feeding: Report of the Global Consultation, and Summary of Guiding Principles for Complementary Feeding of the Breastfed Child. Available online: http://www.who.int/iris/handle/10665/42739 (accessed on 19 May 2019).
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A position paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Alvisi, P.; Brusa, S.; Alboresi, S.; Amarri, S.; Bottau, P.; Cavagni, G.; Corradini, B.; Landi, L.; Loroni, L.; Marani, M.; et al. Recommendations on complementary feeding for healthy, full-term infants. Ital. J. Pediatr. 2015, 41, 36. [Google Scholar] [CrossRef] [Green Version]
- Palmer, D.J.; Makrides, M. Introducing solid foods to preterm infants in developed countries. Ann. Nutr. Metab. 2012, 60, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, M.E.; Di Mauro, A.; Pedico, A.; Rizzo, V.; Capozza, M.; Meneghin, F.; Lista, G.; Laforgia, N. Weaning time in preterm infants: An audit of italian primary care paediatricians. Nutrients 2018, 10, 616. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef] [Green Version]
- Zielinska, M.A.; Rust, P.; Masztalerz-Kozubek, D.; Bichler, J.; Hamułka, J. Factors influencing the age of complementary feeding—A cross-sectional study from two European countries. Int. J. Environ. Res. Public Health 2019, 16, 3799. [Google Scholar] [CrossRef] [Green Version]
- Cleary, J.; Dalton, S.M.C.; Harman, A.; Wright, I.M. Current practice in the introduction of solid foods for preterm infants. Public Health Nutr. 2020, 23, 94–101. [Google Scholar] [CrossRef]
- Elfzzani, Z.; Kwok, T.C.; Ojha, S.; Dorling, J. Education of family members to support weaning to solids and nutrition in infants born preterm. Cochrane Database Syst. Rev. 2019, 2, CD012240. [Google Scholar] [CrossRef]
- Yrjänä, J.M.S.; Koski, T.; Törölä, H.; Valkama, M.; Kulmala, P. Very early introduction of semisolid foods in preterm infants does not increase food allergies or atopic dermatitis. Ann. Allergy Asthma Immunol. 2018, 121, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, K.M.; Feskens, E.J.M.; Van Goudoever, J.B.; Janse, A.J. The Timing of Initiating Complementary Feeding in Preterm Infants and Its Effect on Overweight: A Systematic Review. Ann. Nutr. Metab. 2018, 72, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Peters, T.; Pompeii-Wolfe, C. Nutrition considerations after NICU discharge. Pediatr Ann. 2018, 47, e154–e158. [Google Scholar] [CrossRef] [PubMed]
- Barachetti, R.; Villa, E.; Barbarini, M. Weaning and complementary feeding in preterm infants: Management, timing and health outcome. Pediatr. Med. Chir. 2017, 39, 115–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Agarwal, R.; Aggarwal, K.C.; Chellani, H.; Duggal, A.; Arya, S.; Bhatia, S.; Sankar, M.J.; Sreenivas, V.; Jain, V.; et al. Investigators of the CF Trial Complementary feeding at 4 versus 6 months of age for preterm infants born at less than 34 weeks of gestation: A randomised, open-label, multicentre trial. Lancet Glob. Heal. 2017, 5, E501–E511. [Google Scholar] [CrossRef] [Green Version]
- Embleton, N.D.; Fewtrell, M. Complementary feeding in preterm infants. Lancet Glob. Health 2017, 5, e470–e471. [Google Scholar] [CrossRef]
- Longfier, L.; Soussignan, R.; Reissland, N.; Leconte, M.; Marret, S.; Schaal, B.; Mellier, D. Emotional expressiveness of 5 e 6 month-old infants born very premature versus full-term at initial exposure to weaning foods. Appetite 2016, 107, 494–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegler, J.; Eisemann, N.; Ehlers, S.; Orlikowsky, T.; Kannt, O.; Herting, E.; Göpel, W. Length and weight of very low birth weight infants in Germany at 2 years of age: Does it matter at what age they start complementary food ? Eur. J. Clin. Nutr. 2015, 69, 662–667. [Google Scholar] [CrossRef]
- Braid, S.; Harvey, E.M.; Bernstein, J.; Matoba, N. Early introduction of complementary foods in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 811–818. [Google Scholar] [CrossRef]
- Fanaro, S.; Borsari, G.; Vigi, V. Complementary Feeding Practices in Preterm Infants: An Observational Study in a Cohort of Italian Infants. J. Pediatr. Gastroenterol. Nutr. 2007, 45, S210–S214. [Google Scholar] [CrossRef]
- Fanaro, S.; Vigi, V. Weaning Preterm Infants: An Open Issue. J. Pediatr. Gastroenterol. Nutr. 2007, 45, S204–S209. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.B.; Lucas, A.; Fewtrell, M.S. Does weaning influence growth and health up to 18 months? Arch. Dis. Child. 2004, 89, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.; Williams, P.; Norris, F.; Williams, C.M.; Larkin, M.; Hampton, S. Eczema and early solid feeding in preterm infants. Arch. Dis. Child. 2004, 89, 309–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marriott, L.D.; Foote, K.D.; Bishop, J.A.; Kimber, A.C.; Morgan, J.B.; Article, O. Weaning preterm infants: A randomised controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F302–F307. [Google Scholar] [CrossRef] [Green Version]
- Fewtrell, M.S.; Lucas, A.; Morgan, J.B. Factors associated with weaning in full term and preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F296–F301. [Google Scholar] [CrossRef] [PubMed]
- Foote, K.D.; Marriott, L.D. Weaning of infants. Arch. Dis. Child. 2003, 488–492. [Google Scholar] [CrossRef] [Green Version]
- Norris, F.J.; Larkin, M.S.; Williams, C.M.; Hampton, S.M.; Morgan, J.B. Factors affecting the introduction of complementary foods in the preterm infant. Eur. J. Clin. Nutr. 2002, 56, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Giannì, M.L.; Bezze, E.; Colombo, L.; Rossetti, C.; Pesenti, N.; Roggero, P.; Sannino, P.; Muscolo, S.; Plevani, L.; Mosca, F. Complementary feeding practices in a cohort of Italian late preterm infants. Nutrients 2018, 10, 1861. [Google Scholar] [CrossRef] [Green Version]
- Menezes, L.V.P.; Steinberg, C.; Nobrega, A.C. Complementary feeding in infants born prematurely. CODAS 2018, 30, e20170157. [Google Scholar] [CrossRef]
- Vissers, K.M.; Feskens, E.J.; van Goudoever, J.B.; Janse, A.J. The timing of complementary feeding in preterm infants and the effect on overweight: Study protocol for a systematic review. Syst. Rev. 2016, 5, 149. [Google Scholar] [CrossRef] [Green Version]
- Fanaro, S.; Ballardini, E.; Vigi, V. Weaning in Pre-Term Infants. Minerva Pediatr. 2009, 61, 859–863. [Google Scholar] [PubMed]
- Gupta, S.; Sankar, M.J.; Agarwal, R.; Natarajan, C.K. Initiation of complementary feeding before four months of age for prevention of postnatal growth restriction in preterm infants. Cochrane Database Syst. Rev. 2016, 2016, CD012153. [Google Scholar] [CrossRef]
- Rodriguez, J.; Affuso, O.; Azuero, A.; Downs, C.A.; Turner-Henson, A.; Rice, M. Infant Feeding Practices and Weight Gain in Toddlers Born Very Preterm: A Pilot Study. J. Pediatr. Nurs. 2018, 43, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.B.; Williams, P.; Foote, K.D.; Marriott, L.D. Do mothers understand healthy eating principles for low-birth-weight infants? Public Health Nutr. 2016, 9, 700–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, C. An evidence based guide to weaning preterm infants. Paediatr. Child. Health 2009, 19, 405–414. [Google Scholar] [CrossRef]
- Weaning and the weaning diet. Report of the Working Group on the Weaning Diet of the Committee on Medical Aspects of Food Policy. Rep. Health Soc. Subj. 1994, 45, 1–113. [Google Scholar]
- Chawla, D. Oral Feeding in Neonates With Bronchopulmonary Dysplasia. Indian J. Pediatr. 2019, 86, 319–320. [Google Scholar] [CrossRef]
- Hübl, N.; da Costa, S.; Kaufmann, N.; Oh, J.; Willmes, K. Sucking Patterns Are Not Predictive of Further Feeding Development in Healthy Preterm Infants. Infant Behav. Dev. 2020, 58, 101412. [Google Scholar] [CrossRef]
- Sanchez, K.; Spittle, A.; Slattery, J.; Morgan, A. Oromotor Feeding in Children Born Before 30 Weeks’ Gestation and Term-Born Peers at 12 Months’ Corrected Age. J. Pediatr. 2016, 178, 113–118. [Google Scholar] [CrossRef]
- Dusick, A. Investigation and management of dysphagia. Semin. Pediatr. Neurol. 2003, 10, 255–264. [Google Scholar] [CrossRef]
- Gingras, V.; Aris, I.M.; Rifas-Shiman, S.L.; Switkowski, K.M.; Oken, E.; Hivert, M.-F.F. Timing of complementary feeding introduction and adiposity throughout childhood. Pediatrics 2019, 144, e20191320. [Google Scholar] [CrossRef]
- Papoutsou, S.; Savva, S.C.; Hunsberger, M.; Jilani, H.; Michels, N.; Ahrens, W.; Tornaritis, M.; Veidebaum, T.; Molnár, D.; Siani, A.; et al. Timing of solid food introduction and association with later childhood overweight and obesity: The IDEFICS study. Matern. Child. Nutr. 2018, 14, e12471. [Google Scholar] [CrossRef] [Green Version]
- Pahsini, K.; Marinschek, S.; Khan, Z.; Urlesberger, B.; Scheer, P.J.P.; Dunitz-Scheer, M. Tube Dependency as a Result of Prematurity. J. Neonatal Perinat. Med. 2018, 11, 311–316. [Google Scholar] [CrossRef]
- Lau, C. Development of infant oral feeding skills: What do we know? Am. J. Clin. Nutr. 2016, 103, 616S–621S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamitsuka, M.D.; Nervik, P.A.; Nielsen, S.L.; Clark, R.H. Incidence of Nasogastric and Gastrostomy Tube at Discharge Is Reduced after Implementing an Oral Feeding Protocol in Premature. Am. J. Perinatol. 2017, 34, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, N.; Vishwambaran, L.; Sundaram, K.; Narayanan, I. A Controlled Trial of Alternative Methods of Oral Feeding in Neonates. Early Hum. Dev. 1999, 54, 29–38. [Google Scholar] [CrossRef]
- Lipner, H.S.; Huron, R.F. Developmental and Interprofessional Care of the Preterm Infant: Neonatal Intensive Care Unit Through High-Risk Infant Follow-up. Pediatr. Clin. N. Am. 2018, 65, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Biniwale, M.A.; Ehrenkranz, R.A. The Role of Nutrition in the Prevention and Management of Bronchopulmonary Dysplasia. Semin. Perinatol. 2006, 30, 200–208. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Study Design | Main Findings |
|---|---|---|
| Recommendations | ||
| COMA report, 1994 [37] | Recommendation | Report of the Working Group on the Weaning Diet of the Committee on Medical Aspects of Food Policy. Recommendations for CF in term infants. Brief specific advice for preterm infants. |
| King, 2009 [36] | Recommendations | Proposed evidence-based guide for CF tailored to preterm infants. |
| Reviews | ||
| Barachetti, 2018 [15] | Narrative review | Review of management, timing and health outcomes of CF in preterm infants. |
| Embleton, 2017 [17] | Commentary on Gupta, 2017 | Commentary on the trial by Gupta et al. examining the effect of two different timings of PCF on preterm infants’ growth and clinical outcome |
| Fanaro, 2007 [22] | Narrative review | Review of growth and feeding issues in preterm infants after hospital discharge, with specific focus on age, type and frequency of complementary foods |
| Fanaro, 2009 [32] | Narrative review | Review of CF introduction in preterm infants |
| Foote, 2003 [27] | Narrative review | Overview of CF with a focus on low birth weight and preterm infants |
| Palmer, 2012 [5] | Narrative review | Available guidelines and current practices regarding PCF; evaluation of possible harms of early introduction of solid foods |
| Peters, 2018 [14] | Narrative review | Review on nutrition after discharge of preterm infants from the Neonatal Intensive Care Unit, with a focus on CF and allergenic foods |
| Elfzzani, 2019 [11] | Meta-analysis | Role of nutritional education of family members in supporting CF practices in preterm infants. No eligible trials looking at the impact of nutrition education of family members on PCF fulfilled the inclusion criteria of this systematic review. |
| Gupta, 2016 [33] | Study protocol for a meta-analysis | To evaluate the effect and safety of early (at or before four months) vs. late (after four months) initiation of PCF. Both corrected and postnatal age will be examined. |
| Vissers, 2016 [31] | Study protocol for Vissers, 2018 [13] | Protocol for a systematic review on the effect of PCF timing on overweight. |
| Vissers, 2018 [13] | Systematic review | Effect of the timing of CF introduction (early vs. late) on the risk of overweight in preterm infants The five included papers (thee RCTs, two cohort studies) showed conflicting results: two RCTs → no significant difference in BMI Z-score between the intervention groups at 12 months of age; one RCT → higher rate of length growth until 12 months in the preterm weaning strategy-group compared with the current best practices; one observational study → inverse relationship between timing of CF and length and weight Z-scores. |
| Chawla, 2019 [38] | Editorial commentary | An overview regarding the CF strategies for preterm infants with bronchopulmonary dysplasia |
| Dusick, 2003 [41] | Narrative review | A review regarding the nutritional management of infants with dysphagia. |
| Trials | ||
| Baldassarre, 2018 [6] | Observational trial | Survey of PCF among Italian primary care pediatricians. Heterogeneity in PCF timing (based on infants age, and/or neurodevelopment and/or body weight), quality, and prescription of vitamin D and iron supplements. |
| Braid, 2015 [20] | Observational trial | Analysis of factors associated with early CF in preterm infants from the Early Childhood Longitudinal Study, Birth Cohort (2001–2002). Higher odds of early CF in preterm vs. term infants. The lower the GA, the higher the odds. Predictors of early CF different in preterm compared to term infants. |
| Cleary, 2020 [10] | Observational trial | Structured interviews on infant feeding practices, growth and medical status in term and preterm infants. Preterm infants received CF earlier than term infants; lower maternal education and male gender were associated with early CF among preterm infants. |
| Fanaro, 2007 [21] | Observational trial | Survey of CF practices in an Italian region. Wide variation in timing (corrected vs. chronological age) and quality of CF (low energy and low protein often offered as first solid food, with negligible iron and zinc content). |
| Fewtrell, 2003 [26] | Pooled RCTs results | Data from >2000 infants from seven prospective UK RCTs, comparing the age at CF in term appropriate size for gestational age (AGA), small for gestational age, and preterm infants. Preterm infants were significantly more likely to receive solids at both six and twelve weeks after term than term AGA infants. Factors associated with earlier CF were formula feeding and maternal smoking. |
| Giannì, 2018 [29] | Observational trial | Evaluation of practices related to CF in a cohort of Italian late preterm infants. Late preterm infants were weaned at almost six months of age and received low energy and/or low protein-dense foods as first solid foods. |
| Gupta, 2017 [16] | RCT | RCT comparing the initiation of CF at four vs. six months CA in preterm infants in India. No difference was documented in the primary aim (weight-for-age z score at 12 months CA) between groups, but a higher rate of hospital admission was recorded in the four-month group. |
| Hüb, 2020 [39] | Observational trial | Evaluation of the association between sucking patterns, assisted spoon feeding, and chewing skills in preterm infants. Sucking patterns were evaluated at 34, 37, and 44 weeks CA, assisted spoon feeding was evaluated at six, nine, and 12 months PMA, and chewing was evaluated at 9, 12, and 24 months PMA. |
| Longfier, 2016 [18] | Observational trial | Analysis of facial expression and infant’s temperament in response to the introduction of CF in preterm vs. term infants. Infants born preterm expressed fewer negative emotions in response to first CF than infants born full-term and showed a familiarization effect with the frequency of negative expressions decreasing after tasting the second spoon, regardless of infant age, type of food and order of presentation. |
| Marriott, 2004 [25] | RCT | RCT aimed at comparing a “preterm weaning strategy (PWS)” vs. conventional CF management in preterm infants. Infants receiving CF according to PWS showed higher standard deviation length scores and length growth velocity, and higher intake of energy, protein, and carbohydrate, and iron during follow up. |
| Menezes, 2018 [30] | Observational trial | Structured interviews administered to parents of preterm infants to highlight feeding difficulties during CF. Most infants had at least one defensive behavior at mealtime, including refusal to open their mouth, food selectivity, and feeding refusal. |
| Morgan, 2004 [23] | Pooled RCTs results | Data from >1600 term and preterm infants from five prospective UK RCTs, comparing early (<12 weeks) vs. late (>12 weeks) introduction of CF. As for preterm infants, those weaned before 12 weeks showed slower gain in weight, length, and head circumference between 12 weeks and 18 months than those weaned after 12 weeks; by 18 months, there were no significant differences in size between the two groups. No effect of CF on other clinical outcomes was observed |
| Morgan, 2004 [24] | Observational trial | Evaluation of CF-related risk factors for eczema at 12 months post-term in preterm infants. Identified risk factors were the introduction of ≥4 solid foods by or before 17 weeks post-term, male gender, having atopic parents who introduced solid foods before 10 weeks post-term or having at least one atopic parent. |
| Morgan, 2016 [35] | Observational trial | Cohort study performed by means of postal questionnaires aimed at describing feeding patterns and mothers’ perceptions of desirable feeding practices in preterm infants in England. CF was introduced at a median age of 17 postnatal weeks. Mothers perceived a high-fiber, low-fat diet as important for their infants. A high calorie intake was not given the correct importance by 25% of mothers. |
| Norris, 2002 [28] | Observational trial | Structured interviews conducted in the UK to evaluate factors associated with PCF. Almost half of the infants received early CF, both considering corrected and chronological age. Differences between human milk- and formula-fed infants in the timing of CF were documented. |
| Rodriguez, 2018 [34] | Observational trial | Cross-sectional study aimed at examining the relationship between feeding practices and weight gain. Almost half infants received CF before four months CA. A greater weight gain was documented in infants receiving early CF, but the results were considered of little clinical relevance. |
| Sanchez, 2016 [40] | Observational trial | Evaluation of oro-motor feeding at 12 months’ CA in children born before 30 weeks’ GA compared with term-born peers by observational assessment. Infants born before 30 weeks presented with higher odds of oro-motor feeding problems at 12 months’ CA than their term-born peers (OR 2.21; 95% CI 1.55–3.16). Neonatal surgery was associated with increased odds of feeding difficulties in children born before 30 weeks (OR 11.66; 95% CI 1.56–87.23). |
| Spiegler, 2015 [19] | Observational trial | Longitudinal analysis of timing of CF introduction in German VLBW infants, risk factors for early introduction of CF, and relationship between PCF timing and growth at 2 years of age. Average age at introduction of CF: 3.5 months post-term. Low GA at birth = early PCF introduction. Age at introduction of CF influenced by intrauterine growth restriction, GA at birth, maternal education and a developmental delay perceived by the parents. No negative effect of early introduction of CF on length and weight at two years of age. |
| Yrjänä, 2018 [12] | Observational trial | Evaluation of the association between very early introduction of semi-solid foods on food allergies or atopic dermatitis. Preterm infants were introduced safely to semi-solid foods earlier than term infants but did not show an increased risk for food allergies or atopic dermatitis. |
| Zielinska, 2019 [9] | Observational trial | Cross-sectional study investigating factors for early CF in Poland and Austria. Preterm birth was identified among significant risk factors for early CF, together with lower maternal age and educational level, absence of breastfeeding and formula feeding after hospital discharge. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liotto, N.; Cresi, F.; Beghetti, I.; Roggero, P.; Menis, C.; Corvaglia, L.; Mosca, F.; Aceti, A.; on behalf of the Study Group on Neonatal Nutrition and Gastroenterology—Italian Society of Neonatology. Complementary Feeding in Preterm Infants: A Systematic Review. Nutrients 2020, 12, 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061843
Liotto N, Cresi F, Beghetti I, Roggero P, Menis C, Corvaglia L, Mosca F, Aceti A, on behalf of the Study Group on Neonatal Nutrition and Gastroenterology—Italian Society of Neonatology. Complementary Feeding in Preterm Infants: A Systematic Review. Nutrients. 2020; 12(6):1843. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061843
Chicago/Turabian StyleLiotto, Nadia, Francesco Cresi, Isadora Beghetti, Paola Roggero, Camilla Menis, Luigi Corvaglia, Fabio Mosca, Arianna Aceti, and on behalf of the Study Group on Neonatal Nutrition and Gastroenterology—Italian Society of Neonatology. 2020. "Complementary Feeding in Preterm Infants: A Systematic Review" Nutrients 12, no. 6: 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061843