Development of Criteria for a Positive Front-of-Package Food Labeling: The Israeli Case

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. The Rationale for Determining the Positive FOPL Criteria
2.1.1. Support of the Recommendations of the Mediterranean Diet
2.1.2. Adjustment to the Israeli Dietary Habits
2.1.3. Consideration of Food Processing Level
2.1.4. Consideration of the Natural Composition of the Foods
- Enable mixtures between categories that include only grains, legumes, fruits, vegetables, and nuts.
- Enable mixtures between all food groups while meeting each group’s criteria.
2.2. Assessment of the Expected Prevalence of Positive FOPL
3. Results
3.1. The Criteria for Positive FOPL
- Encourage the labeling of unpackaged foods, such as vegetables, fruits, whole grains, and legumes to enhance the visibility of the positive FOPL and promote their consumption by the public (Appendix C).
- Provide information about the criteria used for each food group (in addition to the prominent positive FOPL). If applicable, the recommended intake must be specified. Since the place on the food packages is limited, it has been suggested to publish the information on a dedicated Internet site.
- Launch the positive FOPL together with a comprehensive campaign and dissemination of information concerning the Mediterranean diet recommendations.
- Develop an evaluation plan for the public and industry acceptability of the positive FOPL. A measurement of changes in food purchasing and consumption behaviors (e.g., the degree of use of the positive FOPL by the retailers and the industry, the number of new products developed to meet the criteria, price changes, the public’s trust in the label, and health measures of the population).
- Update the criteria for positive FOPL as needed. It has been suggested that the committee continues to meet every six months to review applications received from the public and the industry and assess the need to expand the criteria to include additional food products.
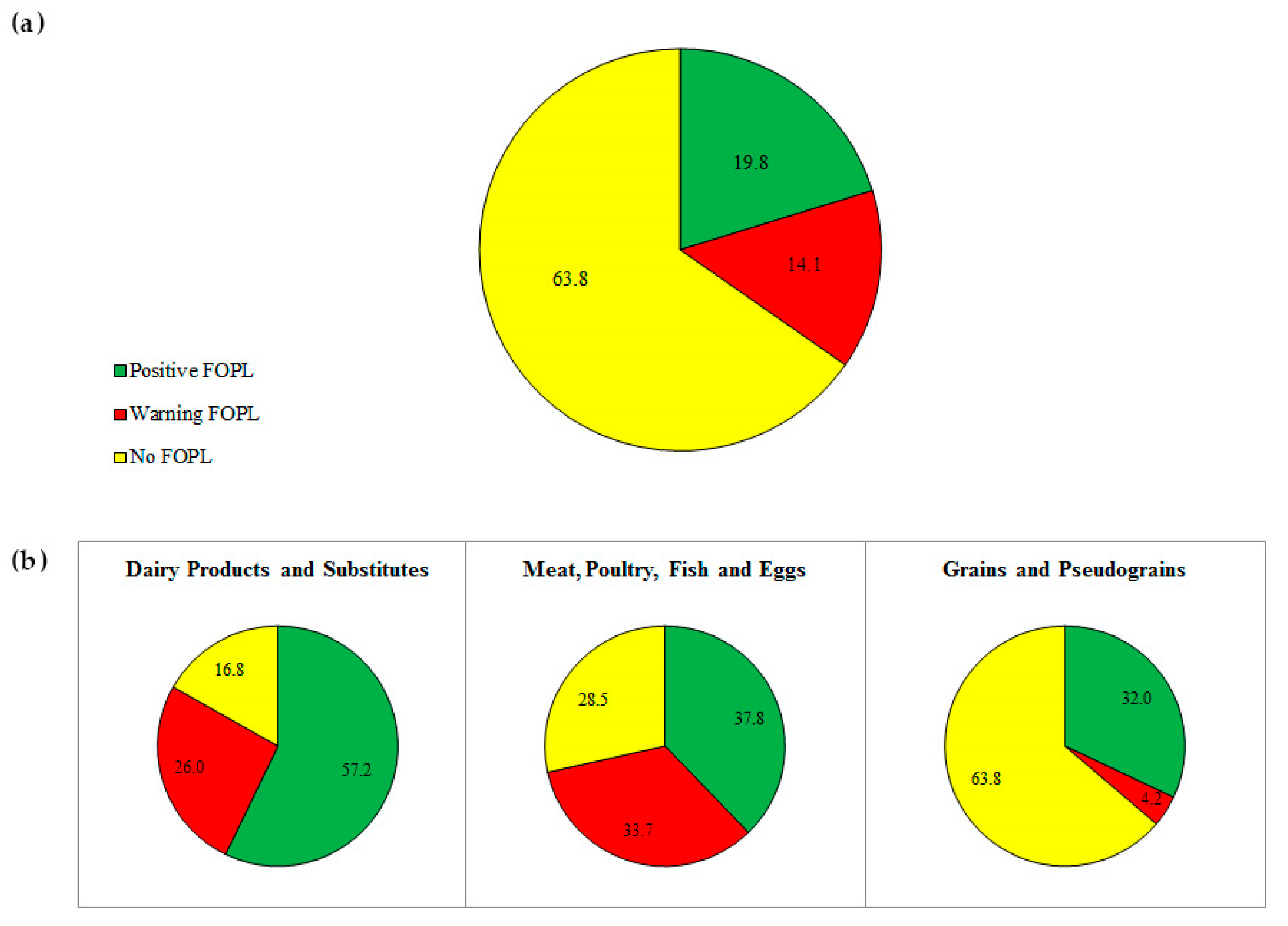
3.2. The Proportion of Foods Eligible for Positive FOPL
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutrient | Amount in 100 g Solid Food | Amount in 100 mL Liquid Food |
|---|---|---|
| First stage, January 2020 | ||
| Sodium (mg) | 500 | 400 |
| Total sugars (g) | 13.5 | 5 |
| Total saturated fatty acids (g) | 5 | 3 |
| Second stage, January 2021 | ||
| Sodium (mg) | 400 | 300 |
| Total sugars (g) | 10 | 5 |
| Total saturated fatty acids (g) | 4 | 3 |
Appendix C


References
- Ministry of Health/The Israel National Institute for Health Policy Research. National Program for Quality Indicators in Community Healthcare in Israel. Report 2016–2018. 2019. Available online: https://www.israelhealthindicators.org/publications (accessed on 6 April 2020).
- Ginsberg, G.M. Mortality, hospital days and treatment costs of current and reduced sugar consumption in Israel. Isr. J. Health Policy Res. 2017, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- OECD. The Heavy Burden of Obesity: The Economics of Prevention. 2019. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/social-issues-migration-health/the-heavy-burden-of-obesity_67450d67-en (accessed on 9 January 2020).
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Diet, Nutrition and Physical Activity: Energy Balance and Body Fatness. Available online: http://dietandcancerreport.org/ (accessed on 9 January 2020).
- Mendonça, R.D.D.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.S.; Bes-Rastrollo, M. Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.L.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System. Rome, FAO. 2019. Available online: http://www.fao.org/fsnforum/resources/fsn-resources/ultra-processed-foods-diet-quality-and-health-using-nova-classification (accessed on 10 January 2020).
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef] [Green Version]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rico-Campà, A.; Martínez-González, M.A.; Alvarez-Alvarez, I.; Mendonça, R.D.D.; de la Fuente-Arrillaga, C.; Gómez-Donoso, C.; Bes-Rastrollo, M. Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ 2019, 365, l1949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association Between Ultraprocessed Food Consumption and Risk of Mortality Among Middle-aged Adults in France. JAMA Intern. Med. 2019, 179, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Israel Center for Disease Control, Ministry of Health. Mabat Youth, Second National Health and Nutrition Survey of 7th–12th Grade Students 2015–2016. 2017. Available online: https://www.health.gov.il/publicationsfiles/mabat_kids2_11_2015-2016-eng.pdf (accessed on 22 June 2020).
- Israel Center for Disease Control, Ministry of Health. Rav Mabat Adult, Second National Health and Nutrition Survey Ages 18–64 2014–2016. 2019. Available online: https://www.health.gov.il/publicationsfiles/mabat_adults_2014_2016_383_en.pdf (accessed on 22 June 2020).
- Endevelt, R.; Grotto, I.; Sheffer, R.; Goldsmith, R.; Golan, M.; Mendlovic, J.; Bar-Siman-Tov, M.; World Health Organization. Regulatory measures to improve nutrition policy towards a better food environment for prevention of obesity and associated morbidity in Israel. Public Health Panor. 2017, 3, 566–574. [Google Scholar]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health: A Framework to Monitor and Evaluate Implementation. 2004. Available online: http://www.who.int/ncds/prevention/global-strategy-diet-physical-activity-2004-goals/en/ (accessed on 9 January 2020).
- World Cancer Research Fund International. Building Momentum: Lessons on Implementing a Robust Front-of-Pack Food Label. 2019. Available online: Wcrf.org/frontofpack. (accessed on 9 January 2020).
- Kelly, B.; Jewell, J. Front-of-pack nutrition labelling in the European region: Identifying what works for governments and consumers. Public Health Nutr. 2019, 22, 1125–1128. [Google Scholar] [CrossRef]
- World Health Organization. Guiding Principles and Framework Manual for Front-Of-Pack Labelling for Promoting Healthy Diets. 2019. Available online: http://www.who.int/nutrition/publications/policies/guidingprinciples-labelling-promoting-healthydiet/en/ (accessed on 6 April 2020).
- Hawley, K.L.; Roberto, C.A.; Bragg, M.A.; Liu, P.J.; Schwartz, M.B.; Brownell, K.D. The science on front-of-package food labels. Public Health Nutr. 2013, 16, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Van der Bend, D.; Lissner, L. Differences and Similarities between Front-of-Pack Nutrition Labels in Europe: A Comparison of Functional and Visual Aspects. Nutrients 2019, 11, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Food Agency’s Code of Statutes. Regulations Amending the National Food Agency’s Regulations (SLVFS 2005:9) on the Use of a Particular Symbol. 2015. Available online: https://www.livsmedelsverket.se/globalassets/om-oss/lagstiftning/livsmedelsinfo-till-konsum---markning/livsfs-2015-1-particular-symbol-eng.pdf. (accessed on 9 January 2020).
- Chantal, J.; Hercberg, S.; World Health Organization. Development of a new front-of-pack nutrition label in France: The five-colour Nutri-Score. Public Health Panor. 2017, 3, 712–725. [Google Scholar]
- UK Department of Health. Guide to Creating a Front of Pack (FoP) Nutrition Label for Pre-Packed Products Sold through Retail Outlets. 2016. Available online: https://www.gov.uk/government/publications/front-of-pack-nutrition-labelling-guidance (accessed on 16 January 2020).
- Reyes, M.; Garmendia, M.L.; Olivares, S.; Aqueveque, C.; Zacarías, I.; Corvalán, C. Development of the Chilean front-of-package food warning label. BMC Public Health 2019, 19, 906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownell, K.D.; Koplan, J.P. Front-of-package nutrition labeling--an abuse of trust by the food industry? N. Engl. J. Med. 2011, 364, 2373–2375. [Google Scholar] [CrossRef] [Green Version]
- Nestle, M.; Ludwig, D.S. Front-of-package food labels: Public health or propaganda? JAMA 2010, 303, 771–772. [Google Scholar] [CrossRef] [Green Version]
- Correa, T.; Fierro, C.; Reyes, M.; Dillman Carpentier, F.R.; Taillie, L.S.; Corvalan, C. Responses to the Chilean law of food labeling and advertising: Exploring knowledge, perceptions and behaviors of mothers of young children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 21. [Google Scholar] [CrossRef]
- Kanter, R.; Reyes, M.; Vandevijvere, S.; Swinburn, B.; Corvalán, C. Anticipatory effects of the implementation of the Chilean Law of Food Labeling and Advertising on food and beverage product reformulation. Obes. Rev. 2019, 20 (Suppl. 2), 129–140. [Google Scholar] [CrossRef]
- Drewnowski, A. Uses of nutrient profiling to address public health needs: From regulation to reformulation. Proc. Nutr. Soc. 2017, 76, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Vyth, E.L.; Steenhuis, I.H.; Roodenburg, A.J.; Brug, J.; Seidell, J.C. Front-of-pack nutrition label stimulates healthier product development: A quantitative analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkes, C.; Smith, T.G.; Jewell, J.; Wardle, J.; Hammond, R.A.; Friel, S.; Thow, A.M.; Kain, J. Smart food policies for obesity prevention. Lancet 2015, 385, 2410–2421. [Google Scholar] [CrossRef]
- Mhurchu, C.N.; Eyles, H.; Choi, Y.-H. Effects of a Voluntary Front-of-Pack Nutrition Labelling System on Packaged Food Reformulation: The Health Star Rating System in New Zealand. Nutrients 2017, 9, 918. [Google Scholar] [CrossRef]
- Thomson, R.K.; McLean, R.M.; Ning, S.X.; Mainvil, L.A. Tick front-of-pack label has a positive nutritional impact on foods sold in New Zealand. Public Health Nutr. 2016, 19, 2949–2958. [Google Scholar] [CrossRef] [PubMed]
- Ning, S.X.; Mainvil, L.A.; Thomson, R.K.; McLean, R.M. Dietary sodium reduction in New Zealand: Influence of the Tick label. Asia Pac. J. Clin. Nutr. 2017, 26, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; McMahon, A.; Boustead, R. A case study of sodium reduction in breakfast cereals and the impact of the Pick the Tick food information program in Australia. Health Promot. Int. 2003, 18, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Young, L.; Swinburn, B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Promot. Int. 2002, 17, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Thow, A.M.; Jones, A.; Schneider, C.H.; Labonté, R. Global Governance of Front-of-Pack Nutrition Labelling: A Qualitative Analysis. Nutrients 2019, 11, 268. [Google Scholar] [CrossRef] [Green Version]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S.; Lancet NCD Action Group. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Guide for Industry. Available online: www.healthstarrating.gov.au (accessed on 16 January 2020).
- Health Promotion Board Singapore. Healthier Choice Symbol Nutrient Guidelines. 2018. Available online: https://www.hpb.gov.sg/docs/default-source/default-document-library/hcs-guidelines-(january-2018)9ab599f6468366dea7adff00000d8c5a.pdf?sfvrsn=2d36ff72_0 (accessed on 16 January 2020).
- Choices International Foundation. Choices Programme International Product Criteria. 2016. Available online: https://www.choicesprogramme.org/ (accessed on 16 January 2020).
- Roodenburg, A.J.C.; Popkin, B.M.; Seidell, J.C. Development of international criteria for a front of package food labelling system: The International Choices Programme. Eur. J. Clin. Nutr. 2011, 65, 1190–1200. [Google Scholar] [CrossRef]
- Codex Alimentarius Commission. Joint FAO/WHO Food Standards Programme. Proposal for New Work Concerning a Global Standard for Front of Pack Interpretive Nutrition 2016. In Proceedings of the Codex Committee on Food Labelling, Forty-Third Session, Ottawa, ON, Canada, 9–13 May 2016. [Google Scholar]
- Nutrient Profiling: Report of a WHO/IASO Technical Meeting, London, United Kingdom 4–6 October 2010. Available online: http://www.who.int/nutrition/publications/profiling/WHO_IASO_report2010/en/ (accessed on 9 January 2020).
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Atherosclerosis 2016, 252, 207–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobstein, T.; Davies, S. Defining and labelling ‘healthy’ and ‘unhealthy’ food. PHN 2009, 12, 331–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tharrey, M.; Maillot, M.; Azaïs-Braesco, V.; Darmon, N. From the SAIN,LIM system to the SENS algorithm: A review of a French approach of nutrient profiling. Proc. Nutr. Soc. 2017, 76, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Rayner, M. Nutrient profiling for regulatory purposes. Proc. Nutr. Soc. 2017, 76, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feunekes, G.I.J.; Gortemaker, I.A.; Willems, A.A.; Lion, R.; van den Kommer, M. Front-of-pack nutrition labelling: Testing effectiveness of different nutrition labelling formats front-of-pack in four European countries. Appetite 2008, 50, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Foo, L.L.; Vijaya, K.; Sloan, R.A.; Ling, A. Obesity prevention and management: Singapore’s experience. Obes. Rev. 2013, 14, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Julia, C.; Méjean, C.; Péneau, S.; Buscail, C.; Alles, B.; Fézeu, L.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. The 5-CNL Front-of-Pack Nutrition Label Appears an Effective Tool to Achieve Food Substitutions towards Healthier Diets across Dietary Profiles. PLoS ONE 2016, 11, e0157545. [Google Scholar] [CrossRef]
- Julia, C.; Péneau, S.; Buscail, C.; Gonzalez, R.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. Perception of different formats of front-of-pack nutrition labels according to sociodemographic, lifestyle and dietary factors in a French population: Cross-sectional study among the NutriNet-Santé cohort participants. BMJ Open 2017, 7, e016108. [Google Scholar] [CrossRef]
- Mejean, C.; Macouillard, P.; Péneau, S.; Hercberg, S.; Castetbon, K. Consumer acceptability and understanding of front-of-pack nutrition labels. J. Hum. Nutr. Diet. 2013, 26, 494–503. [Google Scholar] [CrossRef]
- Kanter, R.; Vanderlee, L.; Vandevijvere, S. Front-of-package nutrition labelling policy: Global progress and future directions. Public Health Nutr. 2018, 21, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- Dernini, S.; Berry, E.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- The Israeli Ministry of Health. Nutritional Recommendations 2019. Available online: https://www.health.gov.il/PublicationsFiles/dietary%20guidelines%20EN.pdf (accessed on 6 April 2020).
- Galbete, C.; Schwingshackl, L.; Schwedhelm, C.; Boeing, H.; Schulze, M.B. Evaluating Mediterranean diet and risk of chronic disease in cohort studies: An umbrella review of meta-analyses. Eur. J. Epidemiol. 2018, 33, 909–931. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy traditional Mediterranean diet: An expression of culture, history, and lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Israel Center for Disease Control, Ministry of Health. Rav Mabat Kids, First National Health and Nutrition Survey Ages 2–11 Years 2015–2016; Ministry of Health: Tel Aviv, Israel, 2019. [Google Scholar]
- De Lorgeril, M.; Salen, P.; Rabaeus, M. New and traditional foods in a modernized Mediterranean diet model. Eur. J. Clin. Nutr. 2019, 72, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Laster, J.; Frame, L.A. Beyond the Calories-Is the Problem in the Processing? Curr. Treat. Options Gastroenterol. 2019, 17, 577–586. [Google Scholar] [CrossRef]
- Aguayo-Patrón, S.V.; Calderón de la Barca, A.M. Old Fashioned vs. Ultra-Processed-Based Current Diets: Possible Implication in the Increased Susceptibility to Type 1 Diabetes and Celiac Disease in Childhood. Foods 2017, 6, 100. [Google Scholar] [CrossRef] [Green Version]
- Marion-Letellier, R.; Amamou, A.; Savoye, G.; Ghosh, S. Inflammatory Bowel Diseases and Food Additives: To Add Fuel on the Flames! Nutrients 2019, 11, 1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poti, J.M.; Mendez, M.A.; Ng, S.W.; Popkin, B.M. Is the degree of food processing and convenience linked with the nutritional quality of foods purchased by US households? Am. J. Clin. Nutr. 2015, 101, 1251–1262. [Google Scholar] [CrossRef] [Green Version]
- Neltner, T.G.; Kulkarni, N.R.; Alger, H.M.; Maffini, M.V.; Bongard, E.D.; Fortin, N.D.; Olson, E.D. Navigating the U.S. Food Additive Regulatory Program. Compr. Rev. Food Sci. Food Saf. 2011, 10, 342–368. [Google Scholar] [CrossRef]
- Costa, C.S.; Del-Ponte, B.; Assunção, M.C.F.; Santos, I.S. Consumption of ultra-processed foods and body fat during childhood and adolescence: A systematic review. Public Health Nutr. 2018, 21, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Trasande, L.; Shaffer, R.M.; Sathyanarayana, S.; Council on Environmental Health. Food Additives and Child Health. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [Green Version]
- Moubarac, J.-C.; Parra, D.C.; Cannon, G.; Monteiro, C.A. Food Classification Systems Based on Food Processing: Significance and Implications for Policies and Actions: A Systematic Literature Review and Assessment. Curr. Obes. Rep. 2014, 3, 256–272. [Google Scholar] [CrossRef]
- Talati, Z.; Pettigrew, S.; Dixon, H.; Neal, B.; Ball, K.; Hughes, C. Do Health Claims and Front-of-Pack Labels Lead to a Positivity Bias in Unhealthy Foods? Nutrients 2016, 8, 787. [Google Scholar] [CrossRef] [Green Version]
- Ikonen, I.; Sotgiu, F.; Aydinli, A.; Verlegh, P.W.J. Consumer effects of front-of-package nutrition labeling: An interdisciplinary meta-analysis. J. Acad. Mark. Sci. 2019, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Curtain, F.; Grafenauer, S. Health Star Rating in Grain Foods-Does It Adequately Differentiate Refined and Whole Grain Foods? Nutrients 2019, 11, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleef, E.V.; Dagevos, H. The growing role of front-of-pack nutrition profile labeling: A consumer perspective on key issues and controversies. Crit. Rev. Food Sci. Nutr. 2015, 55, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Bix, L.; Sundar, R.P.; Bello, N.M.; Peltier, C.; Weatherspoon, L.J.; Becker, M.W. To See or Not to See: Do Front of Pack Nutrition Labels Affect Attention to Overall Nutrition Information? PLoS ONE 2015, 10, e0139732. [Google Scholar] [CrossRef] [PubMed]
- Talati, Z.; Norman, R.; Pettigrew, S.; Neal, B.; Kelly, B.; Dixon, H.; Ball, K.; Miller, C.; Shilton, T. The impact of interpretive and reductive front-of-pack labels on food choice and willingness to pay. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 171. [Google Scholar] [CrossRef] [Green Version]
- Newman, C.L.; Howlett, E.; Burton, S. Shopper Response to Front-of-Package Nutrition Labeling Programs: Potential Consumer and Retail Store Benefits. J. Retail. 2014, 90, 13–26. [Google Scholar] [CrossRef]
- Tempels, T.; Verweij, M.; Blok, V. Big Food’s Ambivalence: Seeking Profit and Responsibility for Health. Am. J. Public Health 2017, 107, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Ministry for Primary Industries, New Zealand Government. The Health Star Rating System in New Zealand 2014–2018: System Uptake and Nutrient Content of Foods by HSR Status. New Zealand Food Safety Technical Report No: 2018/09. Wellington, New Zealand. 2018. Available online: https://www.mpi.govt.nz/dmsdocument/31635/direct (accessed on 16 January 2020).
- Jones, A.; Shahid, M.; Neal, B. Uptake of Australia’s Health Star Rating System. Nutrients 2018, 10, 997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, M.; Charlton, K.; Probst, Y.; Li, N.; Crino, M.; Wu, J.H.Y. Nutrient profiling and food prices: What is the cost of choosing healthier products? J. Hum. Nutr. Diet. 2019, 32, 432–442. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fiscal Policies for Diet and Prevention of Noncommunicable Diseases: Technical Meeting Report, 5–6 May 2015, Geneva, Switzerland. Available online: http://www.who.int/dietphysicalactivity/publications/fiscal-policies-diet-prevention/en/ (accessed on 9 January 2020).
- Moore, M.; Jones, A.; Pollard, C.M.; Yeatman, H. Development of Australia’s front-of-pack interpretative nutrition labelling Health Star Rating system: Lessons for public health advocates. Aust. N. Z. J. Public Health 2019, 43, 352–354. [Google Scholar] [CrossRef]

| Category | Subcategory | Allowed Additives 1 | Maximum Levels per 100 g |
|---|---|---|---|
| Dairy products | Liquid milk | According to food standards | |
| Fermented milk products | No additives except raw materials | Total fat ≤5% | |
| Cheeses | No additives except salt and spices 2 | Total fat ≤5 g Sodium ≤200 mg | |
| Soy products | Tofu | No additives except salt, spices and gelling agents, as allowed by food standards | Sodium ≤200 mg |
| Soy Drink | Soybeans, water, salt | Sodium ≤50 mg | |
| Vegetable oils | Avocado oil | No additives except tocopherols and ascorbic acid | |
| Almond oil | |||
| Olive oil | |||
| Safflower oil | |||
| Sunflower oil | |||
| Seeds, Nuts, Almonds | Raw or roasted/flour/spreads | No additives | |
| Grains and pseudo-grains | Whole grains 3 in any kind of preparation and packaging (e.g., roasted, cooked, baked, cut, steamed, frozen, vacuum-packed, tinned), not fried | No additives except salt and spices 2 | Sodium ≤200 mg |
| Flour from whole grains ground from the entire kernel | |||
| Puffed rice/crackers 100% whole grains | No additives except salt and spices | Sodium ≤200 mg | |
| Whole pasta according to food standards | No additives | ||
| Legumes | Legumes whole kernel, in any kind of preparation and packaging (e.g., roasted, cooked, baked, cut, steamed, frozen, sprouted, vacuum-packed tinned), not fried | No additives except salt and spices | Sodium ≤200 mg |
| Legume flour (100%) | No additives | ||
| Legume spreads (100%) | No additives except salt, spices, tahini, olive oil, lemon | Sodium ≤200 mg Total fat <7% | |
| Tahini from whole sesame | Raw (not diluted) | No additives | |
| Salad | No additives except salt, spices | Sodium ≤200 mg | |
| Eggs | Fresh, unpeeled | ||
| Fish | Fresh, chilled or frozen (raw), whole or parts | No additives | |
| Baked, roasted or spiced | No additives except spices, salt | Sodium ≤200 mg | |
| Canned | No additives except spices, oils from the list above, salt, water | Sodium ≤200 mg | |
| Poultry | Fresh, chilled or frozen (raw), whole or parts | No additives | Sodium ≤300 mg |
| Baked, roasted or spiced | No additives except spices, salt | Sodium ≤200 mg | |
| Fruits | All kinds of preparation and packaging (e.g., fresh, frozen, cooked, pureed, pickled, roasted, baked, vacuum-packed, tinned). Not jams, confitures, not fried, no juice, not powder, not dried/dry except reconstituted from freeze-drying | No additives | |
| Vegetables | All kind of preparation and packaging (e.g., fresh, frozen, cooked, pureed, pickled, roasted, baked, vacuum-packed, tinned), not fried | No additives except spices, salt | Sodium ≤ 200 mg |
| Tea | Tea and herbal infusion according to food standards | No additives |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gillon-Keren, M.; Kaufman-Shriqui, V.; Goldsmith, R.; Safra, C.; Shai, I.; Fayman, G.; Berry, E.; Tirosh, A.; Dicker, D.; Froy, O.; et al. Development of Criteria for a Positive Front-of-Package Food Labeling: The Israeli Case. Nutrients 2020, 12, 1875. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061875
Gillon-Keren M, Kaufman-Shriqui V, Goldsmith R, Safra C, Shai I, Fayman G, Berry E, Tirosh A, Dicker D, Froy O, et al. Development of Criteria for a Positive Front-of-Package Food Labeling: The Israeli Case. Nutrients. 2020; 12(6):1875. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061875
Chicago/Turabian StyleGillon-Keren, Michal, Vered Kaufman-Shriqui, Rebecca Goldsmith, Carmit Safra, Iris Shai, Gila Fayman, Elliot Berry, Amir Tirosh, Dror Dicker, Oren Froy, and et al. 2020. "Development of Criteria for a Positive Front-of-Package Food Labeling: The Israeli Case" Nutrients 12, no. 6: 1875. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12061875