Effects of Dietary Fibres on Acute Indomethacin-Induced Intestinal Hyperpermeability in the Elderly: A Randomised Placebo Controlled Parallel Clinical Trial

 ,
,  , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Participants and Ethics
2.2. Trial Design
2.3. Data Collection
2.3.1. Demographic Data
2.3.2. Medications
2.3.3. Primary Intervention Parameters
2.3.4. Secondary Parameters
2.4. Monitoring of Compliance and Adverse Events
2.5. Statistical Analysis
3. Results
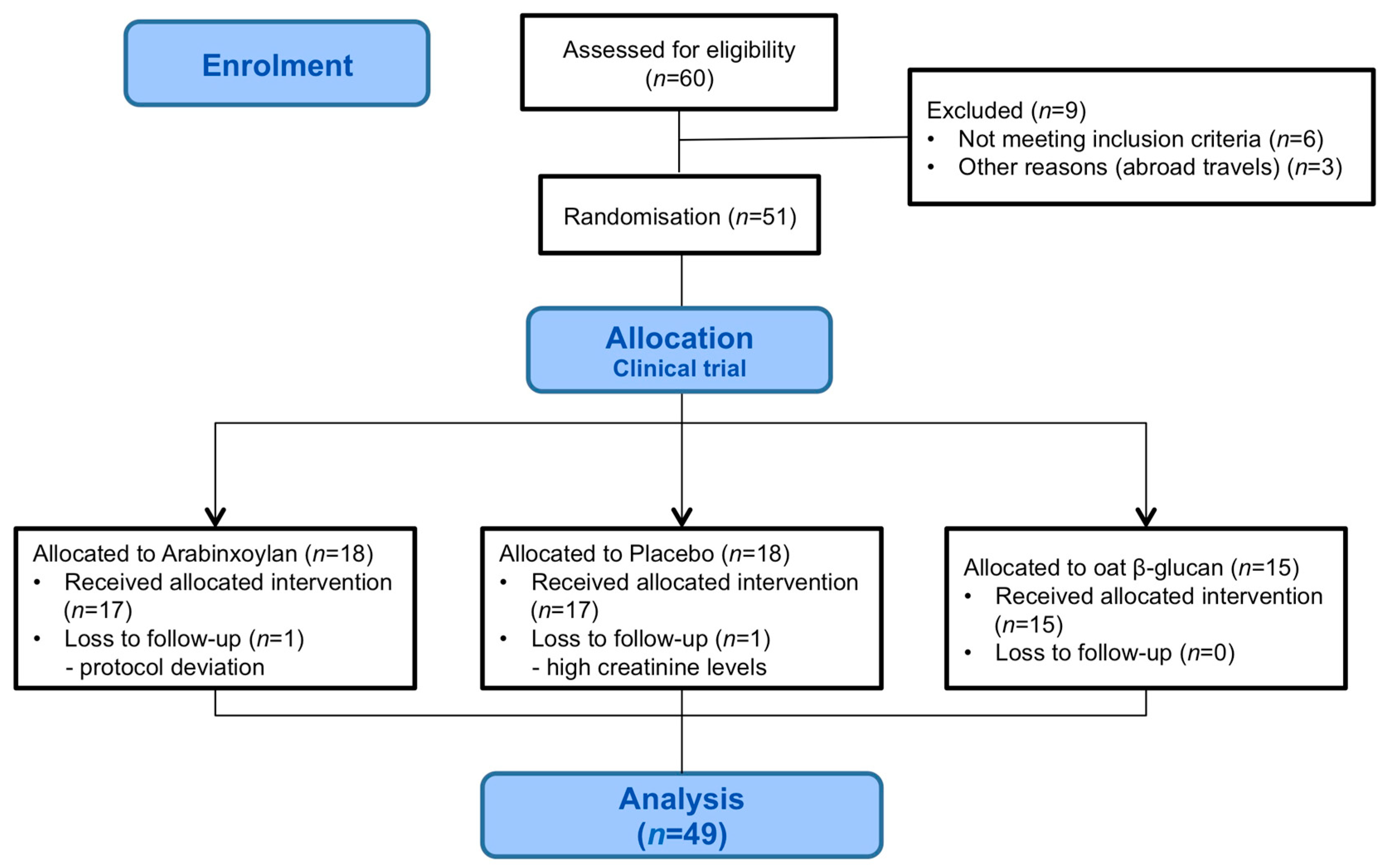
3.1. Participant Flow and Baseline Characteristics
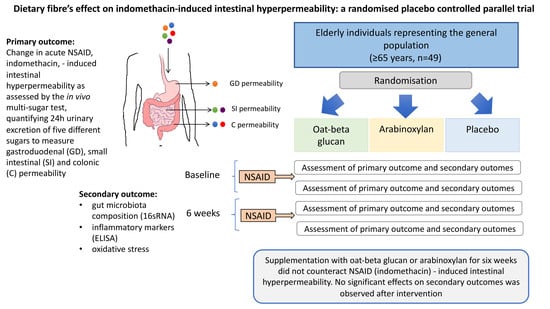
3.2. Primary Outcome
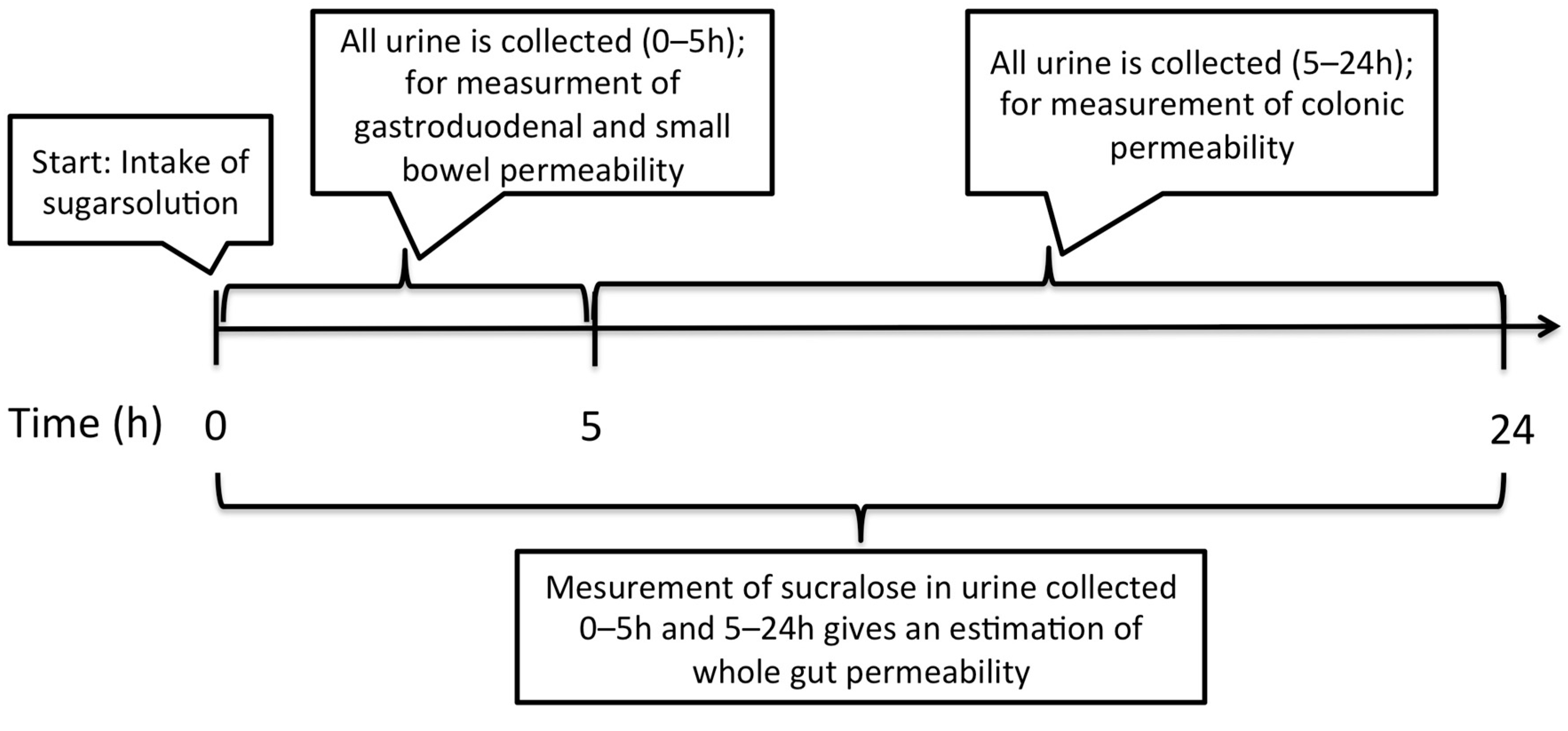
Assessment of Intestinal Permeability
3.3. Secondary Outcomes
3.3.1. Assessment of Gut Microbiota Composition
3.3.2. Evaluation of Gut Health, Wellbeing and Fibre Intake
3.3.3. Biomarkers of Inflammation and Oxidative Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
Appendix A.1. Measurement of Sugar Probes in Urine Samples
Appendix A.2. Measurement of Immune and Oxidative Markers in Blood
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bacterial Probe | Phylum | Class | References *,# |
|---|---|---|---|
| Roseburia intestinalis/hominis * | Firmicutes | Clostridia | Flint HJ et al. 2002 |
| Bacteroides vulgatus | Bacteroidetes | Bacteroidia | |
| Streptococcus agalactiae/Eubacterium rectale | Firmicutes | Bacilli/Clostridia | |
| Firmicutes/Tenericutes/Bacteroidetes species | Firmicutes/Tenericutes /Bacteroidetes species | ||
| Firmicutes (Bacilli) | Firmicutes | Bacilli | |
| Enterococcus, Listeria | Firmicutes | Bacilli | |
| Butyrivibrio crossotus * | Firmicutes | Clostridia | Marius Vita, André Karch & Dietmar H. Pieper. 2017 |
| Prevotella intermedia * | Bacterioidetes | Bacteroida | R. Krajmalnik-Brown et al. 2017 |
| Firmicutes (Negativicutes) | Firmicutes | Negativicutes | |
| Bacteroides sp 4 3 47FAA/vulgatus | Bacteroidetes | Bacteroidia | |
| Veillonella, Helicobacter, Clostridia | Firmicutes | Negativicutes/Epsilonproteobacteria/Clostridia | |
| Enterobacter | Proteobacteria | Gamma Proteobacteria | |
| Ruminococcus champanellensis | Firmicutes | Clostridia | |
| Proteobacteria | Proteobacteria | ||
| Bacteroides caccae | Bacteroidetes | Bacteroidia | |
| Clostridium leptum * | Firmicutes | Clostridia | Watada H. 2017 |
| Ruminococcus bromii | Firmicutes | Clostridia | |
| Subdoligranulum variabile * | Firmicutes | Clostridia | Suzuki et al. 2014 |
| Bacteroides pectinophilus | Bacteroidetes | Bacteroidia | |
| Coprococcus comes * | Firmicutes | Clostridia | De Vuyst et al. 2016 |
| Parabacteroides johnsonii | Bacteroidetes | Bacteroidia | |
| Firmicutes (Clostridia) * | Firmicutes | Clostridia | Marius Vita, André Karch & Dietmar H. Pieper. 2017 |
| Akkermansia municiphila # | Verrucomicrobia | Verrucomicrobiae | Cani & de Vos. 2017 |
| Bacterioides fragilis # | Bacteroidetes | Bacteroidia | Zhi et al. 2018 |
| Shigella/Echerichia | Proteobacteria | Gammaproteobacteria | |
| Prevotella nigrescens | Bacteroidetes | Bacteroidia | |
| Dorea longicatena | Firmicutes | Clostridia | |
| Bacteroides sp 2_2_4/ovatus/sp D1 # | Bacteroidetes | Bacteroidia | Chen W et al. 2019 |
| Eubacterium siraeum # | Firmicutes | Clostridia | Putigani et al. 2017 |
| Alistipes putredinis/onderdonki | Bacteroidetes | Bacteroidia | |
| Megasphaera micronuciformis/Dialister invisus | Firmicutes | Negativicutes | |
| Ruminococcus bicirculans | Firmicutes | Clostridia | |
| Eubacterium ventriosum * | Firmicutes | Clostridia | Kerckhof & Van de Wiele. 2012 |
| Actinobacteria | Actinobacteria | Actinobacteria | |
| Enterobacter/Aeromonas | Proteobacteria | Gamma Proteobacteria | |
| Faecalibacterium * | Firmicutes | Clostridia | Flint et al. 2002 |
| Providencia/Klebsiella/Pantoera | Proteobacteria | Gamma proteobacteria | |
| Lactobacillus # | Firmicutes | Bacilli | Rastall et al. 2019 |
| Collinsella aerofaciens | Actinobacteria | Actinobacteria | |
| Lachnospiraceae * | Firmicutes | Clostridia | Marius Vita, André Karch & Dietmar H. Pieper. 2017 |
| Prevotella bivia/amnii | Bacteroidetes | Bacterioa | |
| Bacterioides acidofaciens | Bacterioidetes | Bacterioidetes | |
| Desulfitobacterium/Blautia | Firmicutes | Clostridia | |
| Roseburia inulinivorans * | Firmicutes | Clostridia | Marius Vita, André Karch & Dietmar H. Pieper. 2017 |
| Streptococcus salivarius subsp.thermophilus # | Firmicutes | Bacilli | Gibson et al. 2003 |
| Bacteroides / Prevotella | Bacteroidetes | Bacteroidia | |
| Ruminococcus gnavus | Firmicutes | Clostridia | |
| Bacteroides dorei/sp. D4/sp. 9_1_42FAA | Bacteroidetes | Bacteroidia |
| Questionnaire | Variable | Scoring | Cut-off Values |
|---|---|---|---|
| Gastrointestinal Symptoms Rating Scale (GSRS) | Measure of gastrointestinal health, by five symptom domains: diarrhoea, indigestion, constipation, abdominal pain and reflux. | Fifteen questions rated on a 7-point scale using fixed respond alternatives. | 0-2, no symptoms >2-3, mild symptoms >3-4, moderate symptoms >5, severe symptoms |
| Hospital Anxiety and Depression Scale (HADS) | Measure of psychological distress divided into two subscales: depression and anxiety. | Fourteen questions (7 questions per subscale) rated on a 4-point scale using fixed respond alternatives. | >7, signs of depression and/or anxiety |
| Perceived Stress Scale (PSS) | Measure of perceived stress, providing a total score. | Ten questions rated on a 5-point scale using fixed respond alternatives. | None available, the total score was used to estimate the total stress level |
| EQ-5D-5L: EQ-Index | Health-related quality of life. Mobility, self-care, usual activities, pain/discomfort and anxiety/depression Visual analogue scale (VAS) | 5-point scale using fixed respond alternatives. | None available |
| EQ-VAS | recording subjective wellbeing | Respondents specify their subjective view on their wellbeing today on a scale from 0 (worst) to 100 (best). |
| AX (n = 16) | Placebo (n = 17) | OBG (n = 15) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End | p- Value | Baseline | End | p- Value | Baseline | End | p- Value | |
| IFN-y | 1.0 (0.0–4.7) | 0.0 (0.0–7.8) | 0.81 | 9.6 (0.0–44.3) | 4.7 (0.0–39.6) | 0.26 | 0.5 (0.0–13.0) | 0.0 (0.0–17.7) | 0.84 |
| IL-10 | 4.3 (3.4–6.2) | 4.5 (1.0–6.2) | 0.75 | 4.4 (0.0–5.9) | 5.0 (0.8–6.4) | 0.25 | 3.9 (1.1–5.6) | 4.9 (3.7–7.6) | 0.32 |
| IL-12p70 | 0.1 (0.0–0.5) | 0.5 (0.0–1.2) | 0.29 | 0.3 (0.0–0.5) | 0.2 (0.0–0.5) | 0.51 | 0.5 (0.1–0.8) | 0.5 (0.0–0.5) | 0.71 |
| IL-1b | 0.0 | 0.0 | >0.99 | 0.0 (0.0–0.6) | 0.0 (0.0–0.5) | 0.26 | 0.0 | 0.0 | 0.75 |
| IL-2 | 0.0 | 0.0 | - | 0.0 | 0.0 | - | 0.0 | 0.0 | - |
| IL-6 | 1.3 (0.1–3.3) | 1.4 (1.0–2.7) | 0.98 | 2.1 (1.0–4.0) | 1.4 (0.7–4.4) | 0.94 | 1.4 (0.9–3.3) | 1.5 (0.2–2.9) | 0.76 |
| IL-8 | 2.3 (1.4–3.7) | 4.0 (1.7–6.8) | 0.19 | 1.8 (1.3–3.6) | 2.8 (1.7–4.0) | 0.37 | 2.9 (1.6–5.9) | 2.0 (1.5–4.0) | 0.34 |
| TNF-a | 0.0 (0.0–1.9) | 0.0 (0.0–2.8) | 0.12 | 3.1 (0.0–10.9) | 0.0 (0.0–13.0) | 0.76 | 0.0 (0.0–1.9) | 0.0 | - |
| CRP | 0.7 (0.4–2.7) | 0.4 (0.2–2.3) | 0.26 | 0.6 (0.4–1.1) | 0.7 (0.3–1.2) | 0.78 | 0.8 (0.2–1.9) | 0.4 (0.2–2.4) | 0.12 |
| Intervention Group | Baseline | End | p-Value |
|---|---|---|---|
| AX (n = 13) | 2.01 (1.60–2.20) | 1.7 (1.52–2.14) | 0.106 |
| GSRS diarrhoea /constipation score >2 (n = 5) | 1.72 (1.52–2.20) | 1.7 (1.52–1.96) | 0.188 |
| GSRS diarrhoea/constipation score <2 (n = 8) | 2.07 (1.66–2.21) | 1.77 (1.39–2.29) | 0.383 |
| Placebo (n = 12) | 1.94 (1.84–2.19) | 1.89 (1.71–2.03) | 0.034 * |
| GSRS diarrhoea /constipation score >2 (n = 5) | 2.18 (1.89–2.22) | 2 (1.81–2.16) | 0.437 |
| GSRS diarrhoea /constipation score <2 (n = 7) | 1.9 (1.8–2.0) | 1.73 (1.54–2.0) | 0.03 * |
| OBG (n = 13) | 2.04 (1.87–2.15) | 1.76 (1.57–1.99) | 0.0005 *** |
| GSRS diarrhoea /constipation score >2 (n = 5) | 2.0 (1.87–2.34) | 1.8 (1.57–2.32) | 0.125 |
| GSRS diarrhoea /constipation score <2 (n = 8) | 2.08 (1.67–2.17) | 1.75 (1.41–1.93) | 0.008 ** |
References
- Cohen, J.E. Human population: The next half century. Science 2003, 302, 1172–1175. [Google Scholar] [CrossRef]
- Welfare, T.N.B.o.H.a. Läkemedelsorsakad Sjuklighet Hos Äldre (Drug-Induced Morbidity in Elderly). Available online: http://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2014-12-13.pdf (accessed on 25 May 2020).
- van Wijck, K.; Verlinden, T.J.; van Eijk, H.M.; Dekker, J.; Buurman, W.A.; Dejong, C.H.; Lenaerts, K. Novel multi-sugar assay for site-specific gastrointestinal permeability analysis: A randomized controlled crossover trial. Clin. Nutr. 2013, 32, 245–251. [Google Scholar] [CrossRef]
- Donini, L.M.; Savina, C.; Cannella, C. Nutrition in the elderly: Role of fiber. Arch. Gerontol. Geriatr. 2009, 49 (Suppl. 1), 61–69. [Google Scholar] [CrossRef]
- Neyrinck, A.M.; Possemiers, S.; Druart, C.; Van de Wiele, T.; De Backer, F.; Cani, P.D.; Larondelle, Y.; Delzenne, N.M. Prebiotic effects of wheat arabinoxylan related to the increase in bifidobacteria, roseburia and bacteroides/prevotella in diet-induced obese mice. PLoS ONE 2011, 6, e20944. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, T.S.; Laerke, H.N.; Theil, P.K.; Sorensen, J.F.; Saarinen, M.; Forssten, S.; Knudsen, K.E. Diets high in resistant starch and arabinoxylan modulate digestion processes and scfa pool size in the large intestine and faecal microbial composition in pigs. Br. J. Nutr. 2014, 112, 1837–1849. [Google Scholar] [CrossRef] [Green Version]
- Shen, R.L.; Dang, X.Y.; Dong, J.L.; Hu, X.Z. Effects of oat beta-glucan and barley beta-glucan on fecal characteristics, intestinal microflora, and intestinal bacterial metabolites in rats. J. Agric. Food Chem. 2012, 60, 11301–11308. [Google Scholar] [CrossRef]
- Lu, Z.X.; Walker, K.Z.; Muir, J.G.; Mascara, T.; O’Dea, K. Arabinoxylan fiber, a byproduct of wheat flour processing, reduces the postprandial glucose response in normoglycemic subjects. Am. J. Clin. Nutr. 2000, 71, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Hald, S.; Schioldan, A.G.; Moore, M.E.; Dige, A.; Laerke, H.N.; Agnholt, J.; Bach Knudsen, K.E.; Hermansen, K.; Marco, M.L.; Gregersen, S.; et al. Effects of arabinoxylan and resistant starch on intestinal microbiota and short-chain fatty acids in subjects with metabolic syndrome: A randomised crossover study. PLoS ONE 2016, 11, e0159223. [Google Scholar] [CrossRef] [PubMed]
- Metzler-Zebeli, B.U.; Zijlstra, R.T.; Mosenthin, R.; Ganzle, M.G. Dietary calcium phosphate content and oat beta-glucan influence gastrointestinal microbiota, butyrate-producing bacteria and butyrate fermentation in weaned pigs. FEMS Microbiol. Ecol. 2011, 75, 402–413. [Google Scholar] [CrossRef]
- Troost, F.J.; Saris, W.H.; Brummer, R.J. Recombinant human lactoferrin ingestion attenuates indomethacin-induced enteropathy in vivo in healthy volunteers. Eur. J. Clin. Nutr. 2003, 57, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Salden, B.N.; Troost, F.J.; Wilms, E.; Truchado, P.; Vilchez-Vargas, R.; Pieper, D.H.; Jauregui, R.; Marzorati, M.; van de Wiele, T.; Possemiers, S.; et al. Reinforcement of intestinal epithelial barrier by arabinoxylans in overweight and obese subjects: A randomized controlled trial: Arabinoxylans in gut barrier. Clin. Nutr. 2017, 37, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Johansson, I.; Hallmans, G.; Wikman, A.; Biessy, C.; Riboli, E.; Kaaks, R. Validation and calibration of food-frequency questionnaire measurements in the northern sweden health and disease cohort. Public Health Nutr. 2002, 5, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Casen, C.; Vebo, H.C.; Sekelja, M.; Hegge, F.T.; Karlsson, M.K.; Ciemniejewska, E.; Dzankovic, S.; Froyland, C.; Nestestog, R.; Engstrand, L.; et al. Deviations in human gut microbiota: A novel diagnostic test for determining dysbiosis in patients with ibs or ibd. Aliment Pharm. 2015, 42, 71–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedlund, J.; Sjodin, I.; Dotevall, G. Gsrs—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Ganda Mall, J.P.; Ostlund-Lagerstrom, L.; Lindqvist, C.M.; Algilani, S.; Rasoal, D.; Repsilber, D.; Brummer, R.J.; Åsa, V.K.; Schoultz, I. Are self-reported gastrointestinal symptoms among older adults associated with increased intestinal permeability and psychological distress? BMC Geriatr. 2018, 18, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; de Charro, F. Eq-5d: A measure of health status from the euroqol group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.H.; Fletcher, R.B.; Merrick, P.L. The validity and clinical utility of the hospital anxiety and depression scale (hads) with older adult new zealanders. Int. Psychogeriatr. 2014, 26, 325–333. [Google Scholar] [CrossRef]
- Ezzati, A.; Jiang, J.; Katz, M.J.; Sliwinski, M.J.; Zimmerman, M.E.; Lipton, R.B. Validation of the perceived stress scale in a community sample of older adults. Int. J. Geriatr. Psychiatry 2014, 29, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Smecuol, E.; Bai, J.C.; Sugai, E.; Vazquez, H.; Niveloni, S.; Pedreira, S.; Maurino, E.; Meddings, J. Acute gastrointestinal permeability responses to different non-steroidal anti-inflammatory drugs. Gut 2001, 49, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Wilms, E.; Jonkers, D.; Savelkoul, H.F.J.; Elizalde, M.; Tischmann, L.; de Vos, P.; Masclee, A.A.M.; Troost, F.J. The impact of pectin supplementation on intestinal barrier function in healthy young adults and healthy elderly. Nutrients 2019, 11, 1554. [Google Scholar] [CrossRef] [Green Version]
- Bjarnason, I.; Smethurst, P.; Fenn, C.G.; Lee, C.E.; Menzies, I.S.; Levi, A.J. Misoprostol reduces indomethacin-induced changes in human small intestinal permeability. Dig. Dis. Sci. 1989, 34, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Bours, M.J.; Troost, F.J.; Brummer, R.J.; Bast, A.; Dagnelie, P.C. Local effect of adenosine 5’-triphosphate on indomethacin-induced permeability changes in the human small intestine. Eur. J. Gastroenterol. Hepatol. 2007, 19, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Bours, M.J.; Bos, H.J.; Meddings, J.B.; Brummer, R.J.; van den Brandt, P.A.; Dagnelie, P.C. Effects of oral adenosine 5’-triphosphate and adenosine in enteric-coated capsules on indomethacin-induced permeability changes in the human small intestine: A randomized cross-over study. BMC Gastroenterol. 2007, 7, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walton, G.E.; Lu, C.; Trogh, I.; Arnaut, F.; Gibson, G.R. A randomised, double-blind, placebo controlled cross-over study to determine the gastrointestinal effects of consumption of arabinoxylan-oligosaccharides enriched bread in healthy volunteers. Nutr. J. 2012, 11, 36. [Google Scholar] [CrossRef] [Green Version]
- Fehlbaum, S.; Prudence, K.; Kieboom, J.; Heerikhuisen, M.; van den Broek, T.; Schuren, F.H.J.; Steinert, R.E.; Raederstorff, D. In vitro fermentation of selected prebiotics and their effects on the composition and activity of the adult gut microbiota. Int. J. Mol. Sci. 2018, 19, 3097. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Giacosa, A.; Faliva, M.A.; Perna, S.; Allieri, F.; Castellazzi, A.M. Review on microbiota and effectiveness of probiotics use in older. World J. Clin. Cases 2015, 3, 156–162. [Google Scholar] [CrossRef]
- Mueller, S.; Saunier, K.; Hanisch, C.; Norin, E.; Alm, L.; Midtvedt, T.; Cresci, A.; Silvi, S.; Orpianesi, C.; Verdenelli, M.C.; et al. Differences in fecal microbiota in different european study populations in relation to age, gender, and country: A cross-sectional study. Appl. Environ. Microbiol. 2006, 72, 1027–1033. [Google Scholar] [CrossRef] [Green Version]




| Inclusion criteria |
|
|
|
| Exclusion criteria |
|
|
|
|
| Arabinoxylan | Placebo | Oat β–Glucan | p–Value | |
|---|---|---|---|---|
| n = 17 | n = 17 | n = 15 | ||
| Male, n (%) | 9 (55%) | 9 (56%) | 9 (60%) | ns |
| Female, n (%) | 8 (47%) | 8 (44%) | 6 (40%) | ns |
| Age, years (median [IQR]) | 69.0 (66.0–71.5) | 70.5 (67.0–78.3) | 69.0 (66.0–72.0) | ns |
| BMI(median [IQR]) | 24.8 (23.0–29.1) | 24.7 (22.1–27.2) | 26.2 (22.4–28.0) | ns |
| Smokers | 0 | 0 | 0 | - |
| Baseline CRP levels (IQR) | 0.7 (0.4–2.7) | 0.6 (0.4–1.1) | 0.8 (0.2–1.9) | ns |
| Comorbidities | % | % | % | |
| Cardiovascular diseases | 41.2% | 50.0% | 33.3% | ns |
| Gut symptoms | 35.3% | 33.3% | 20.0% | ns |
| Psychological& neurodegenerative morbidities | 0% | 11.1% | 13.3% | ns |
| Others (lung, kidney, joints, eyes) | 17.6% | 50.0% | 13.3% | p = 0.05 |
| Medications | % | % | % | |
| Cardiovascular | 41.2% | 50.0% | 33.3% | ns |
| Anti-inflammation | 5.9% | 0% | 0% | ns |
| Gut regulating | 29.4% | 22.2% | 20.0% | ns |
| Antibiotics | 17.6% | 16.7% | 13.3% | ns |
| CNS-regulating drugs | 5.9% | 16.7% | 6.7% | ns |
| Others | 29.4% | 50.0% | 26.7% | ns |
| Multipharmacy (5 or more drugs) | 17.6% | 11.1% | 0% | ns |
| Other GI regulators (probiotics, fibres etc) | 17.6% | 16.7% | 0% | ns |
| Pre-Intervention | After Intervention | |||||
|---|---|---|---|---|---|---|
| Study Arm | Baseline | Indomethacin-Challenge | p–Value | Baseline | Indomethacin-Challenge | p–Value |
| AX (n = 17) | ||||||
| Gastroduodenal permeability [sucrose μg/mL] | 3.37 (1.35–6.08) | 3.86 (1.88–6.78) | ns | 3.09 (1.42–8.91) | 6.95 (2.67–13.04) | p < 0.05 |
| Small intestinal permeability [L/R ratio] | 0.038 (0.027–0.048) | 0.056 (0.034–0.099) | p < 0.05 | 0.031 (0.020–0.056) | 0.055 (0.045–0.125) | p < 0.05 |
| Colonic Permeability [S/E ratio] | 0.018 (0.009–0.027) | 0.033 (0.024–0.04) | p < 0.01 | 0.015 (0.011–0.022) | 0.029 (0.020–0.040) | p < 0.01 |
| Placebo (n = 17) | ||||||
| Gastroduodenal permeability [sucrose μg/mL] | 1.69 (1.04–2.96) | 2.26 (1.67–8.10) | ns | 1.96 (0.77–6.53) | 6.73 (2.03–11.99) | p < 0.05 |
| Small intestinal permeability [L/R ratio] | 0.029 (0.021–0.05) | 0.05 (0.025–0.074) | p < 0.01 | 0.034 (0.019–0.049) | 0.064 (0.028–0.098) | p < 0.01 |
| Colonic permeability [S/E ratio] | 0.023 (0.013–0.04) | 0.028 (0.020–0.048) | ns | 0.022 (0.017–0.030) | 0.029 (0.017–0.046) | ns |
| OBG (n = 15) | ||||||
| Gastroduodenal permeability [sucrose μg/mL] | 2.22 (1.21–3.86) | 2.79 (1.79–12.69) | ns | 3.28 (1.23–9.18) | 4.80 (1.35–13.05) | ns |
| Small intestinal permeability [L/R ratio] | 0.027 (0.021–0.035) | 0.056 (0.039–0.077) | p < 0.001 | 0.029 (0.018–0.040) | 0.057 (0.042–0.090) | p < 0.001 |
| Colonic permeability [S/E ratio] | 0.016 (0.010–0.034) | 0.029 (0.022–0.039) | ns | 0.016 (0.008–0.05) | 0.029 (0.014–0.038) | ns |
| AX (n = 17) * | Placebo (n = 17) | OBG (n = 15) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | p- value | Baseline | End of Study | p- Value | Baseline | End of Study | p- Value | |
| GSRS - Diarrha | 1.5 (1.0–2.8) | 1.3 (1.0–1.9) | 0.336 | 1.3 (1.0–2.7) | 1 (1.0–2.7) | 0.516 | 1.3 (1.0–2.0) | 1.3 (1.0–2.3) | 0.45 |
| GSRS - Constipation | 1.3 (1.0–2.6) | 1.2 (1.0–2.9) | 0.242 | 1.3 (1.2–3.2) | 1.3 (1.0–2.8) | 0.824 | 1.3 (1.0–1.7) | 1.0 (1.0–2.0) | >0.99 |
| HADS | 4 (2–5) | 3 ( 1–5.5) | 0.106 | 5.5 (3.3–9.5) | 5.5 (2.3–8) | 0.529 | 3 (2–5) | 5 (1–7) | 0.55 |
| PSS | 8 (4.3–12) | 6.5 (4.3–8.8) | 0.319 | 9.5 (6.3–14) | 10 (3–14) | 0.814 | 8 (4–12) | 6 (3–9) | 0.28 |
| EuroQol VAS | 85 (76–95) | 85 (80–90) | 0.621 | 83 (80–94) | 90 (76–95) | 0.762 | 90 (81–95) | 90 (80–95) | 0.36 |
| EuroQol Index | 0.86 (0.79–0.86) | 0.86 (0.79–0.86) | 0.875 | 0.86 (0.76–1) | 0.80 (0.76–1) | 0.594 | 0.93 (0.86–1) | 1 (0.86–1) | 0.83 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganda Mall, J.-P.; Fart, F.; Sabet, J.A.; Lindqvist, C.M.; Nestestog, R.; Hegge, F.T.; Keita, Å.V.; Brummer, R.J.; Schoultz, I. Effects of Dietary Fibres on Acute Indomethacin-Induced Intestinal Hyperpermeability in the Elderly: A Randomised Placebo Controlled Parallel Clinical Trial. Nutrients 2020, 12, 1954. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071954
Ganda Mall J-P, Fart F, Sabet JA, Lindqvist CM, Nestestog R, Hegge FT, Keita ÅV, Brummer RJ, Schoultz I. Effects of Dietary Fibres on Acute Indomethacin-Induced Intestinal Hyperpermeability in the Elderly: A Randomised Placebo Controlled Parallel Clinical Trial. Nutrients. 2020; 12(7):1954. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071954
Chicago/Turabian StyleGanda Mall, John-Peter, Frida Fart, Julia A. Sabet, Carl Mårten Lindqvist, Ragnhild Nestestog, Finn Terje Hegge, Åsa V. Keita, Robert J. Brummer, and Ida Schoultz. 2020. "Effects of Dietary Fibres on Acute Indomethacin-Induced Intestinal Hyperpermeability in the Elderly: A Randomised Placebo Controlled Parallel Clinical Trial" Nutrients 12, no. 7: 1954. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071954