The Effectiveness of Synbiotic Preparation Containing Lactobacillus and Bifidobacterium Probiotic Strains and Short Chain Fructooligosaccharides in Patients with Diarrhea Predominant Irritable Bowel Syndrome—A Randomized Double-Blind, Placebo-Controlled Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Study Design
2.2. Patients
2.3. The Synbiotic Preparation
2.4. Scheme of the Study
2.5. Endpoint Definitions
2.6. Statistical Analyses
3. Results
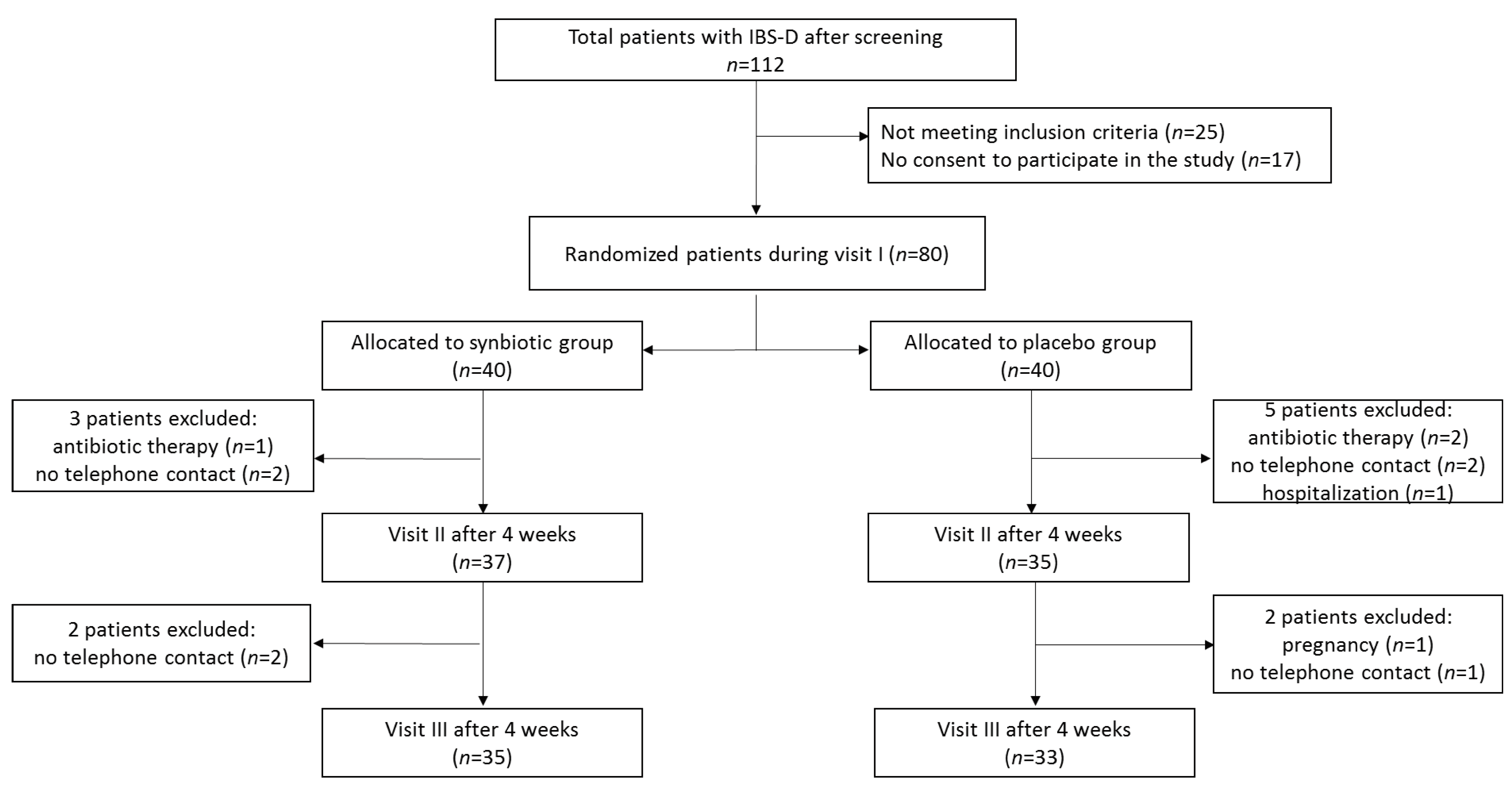
3.1. Subjects
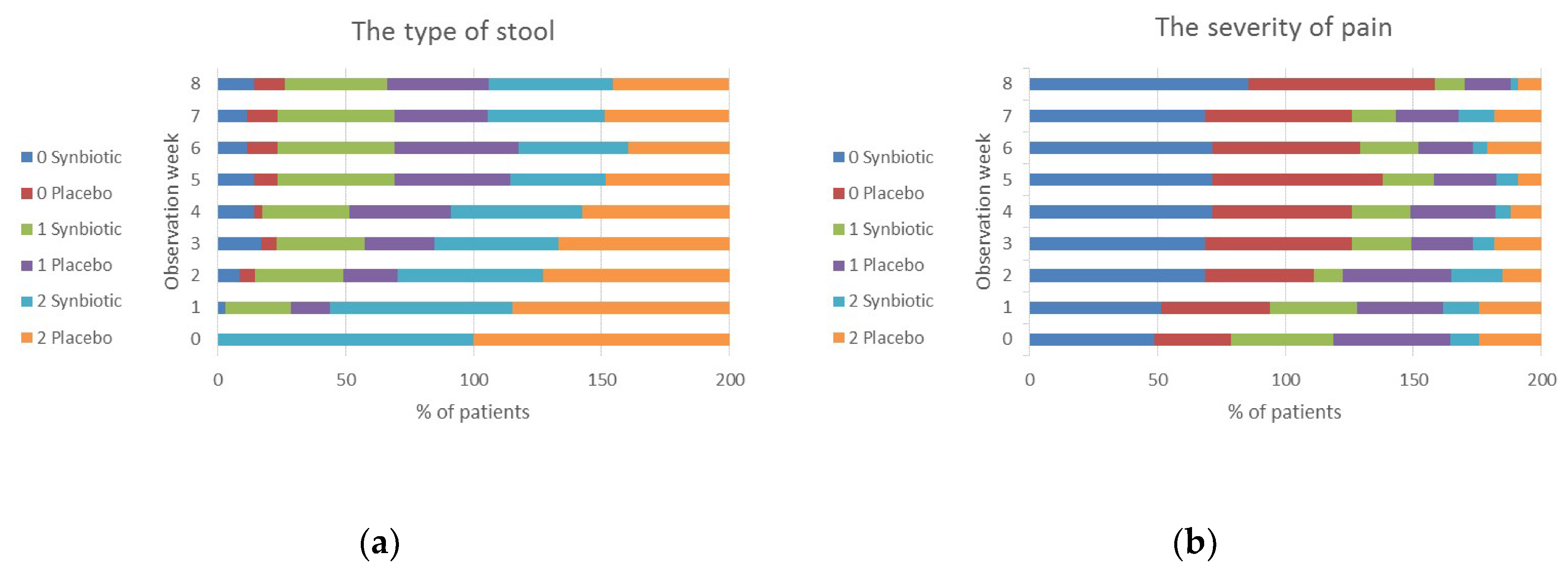
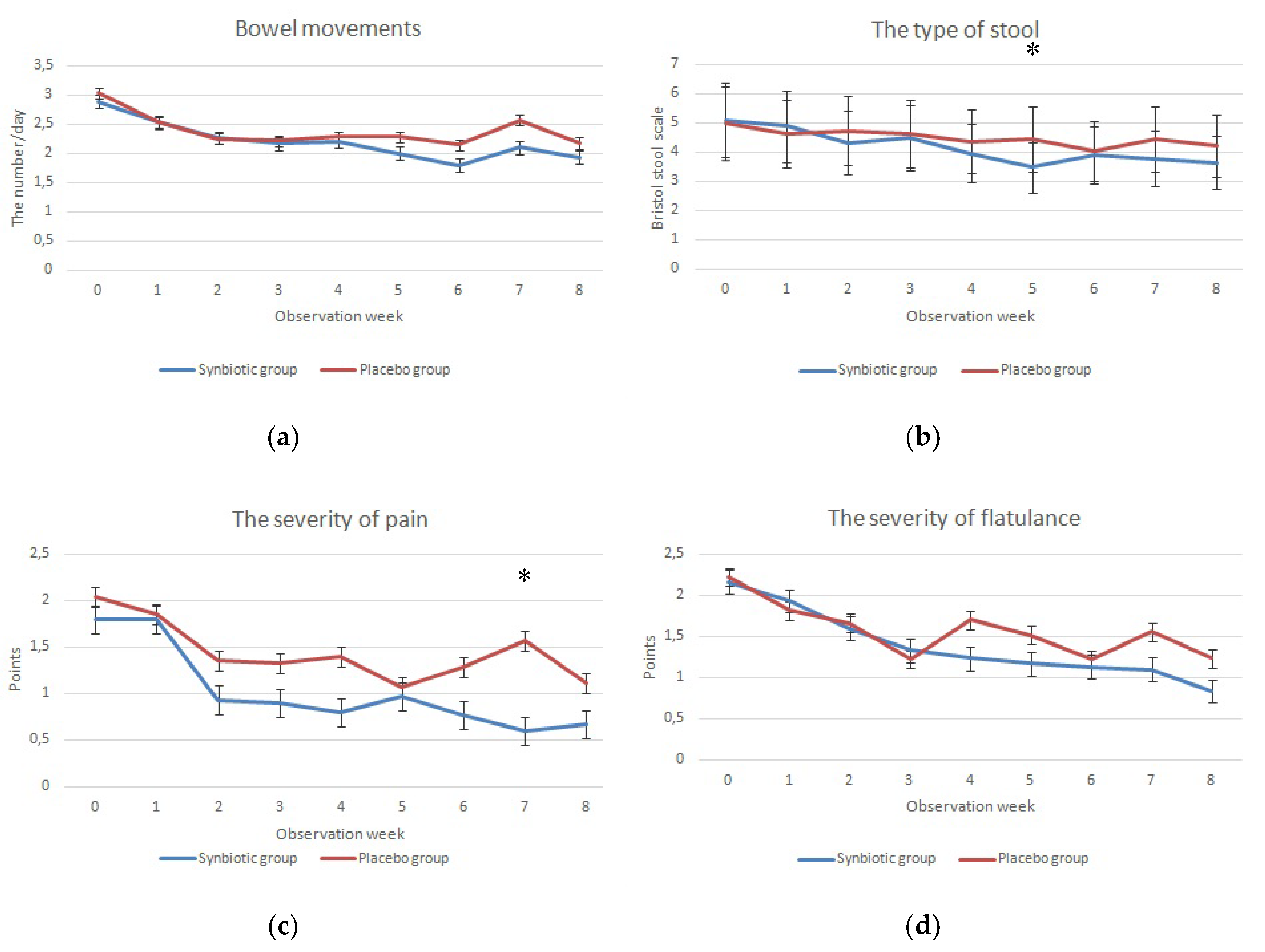
3.2. Study Primary Endpoints
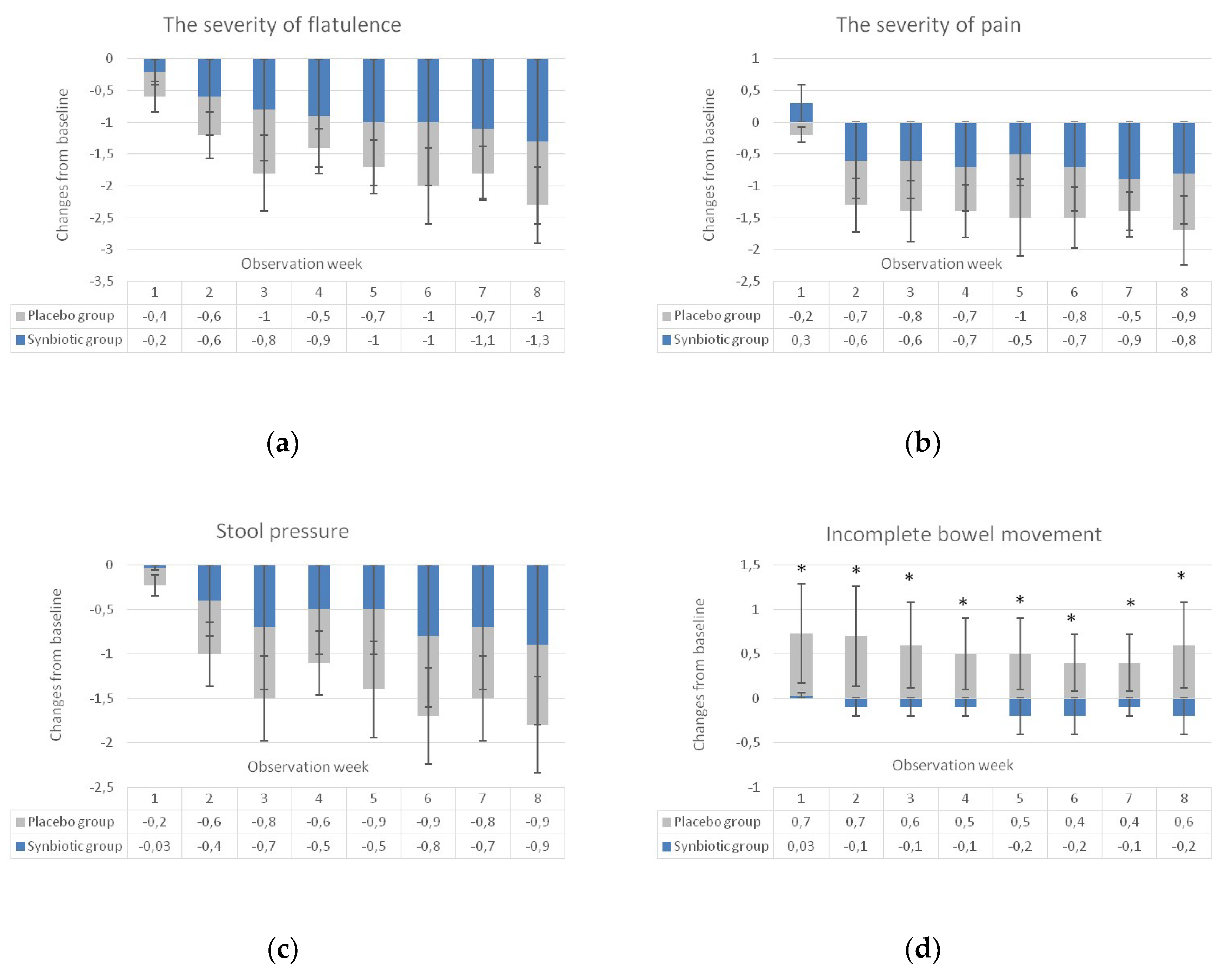
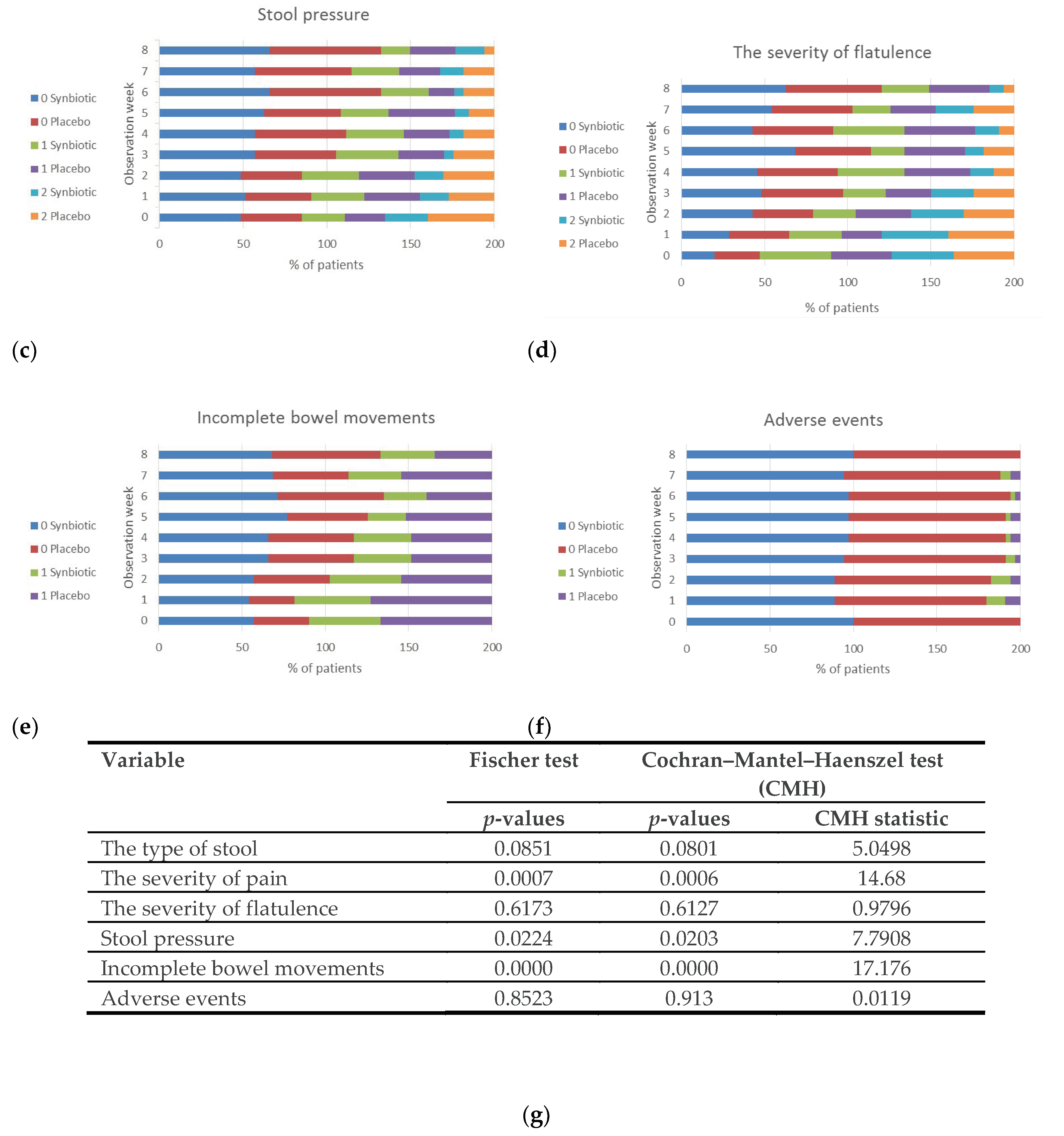
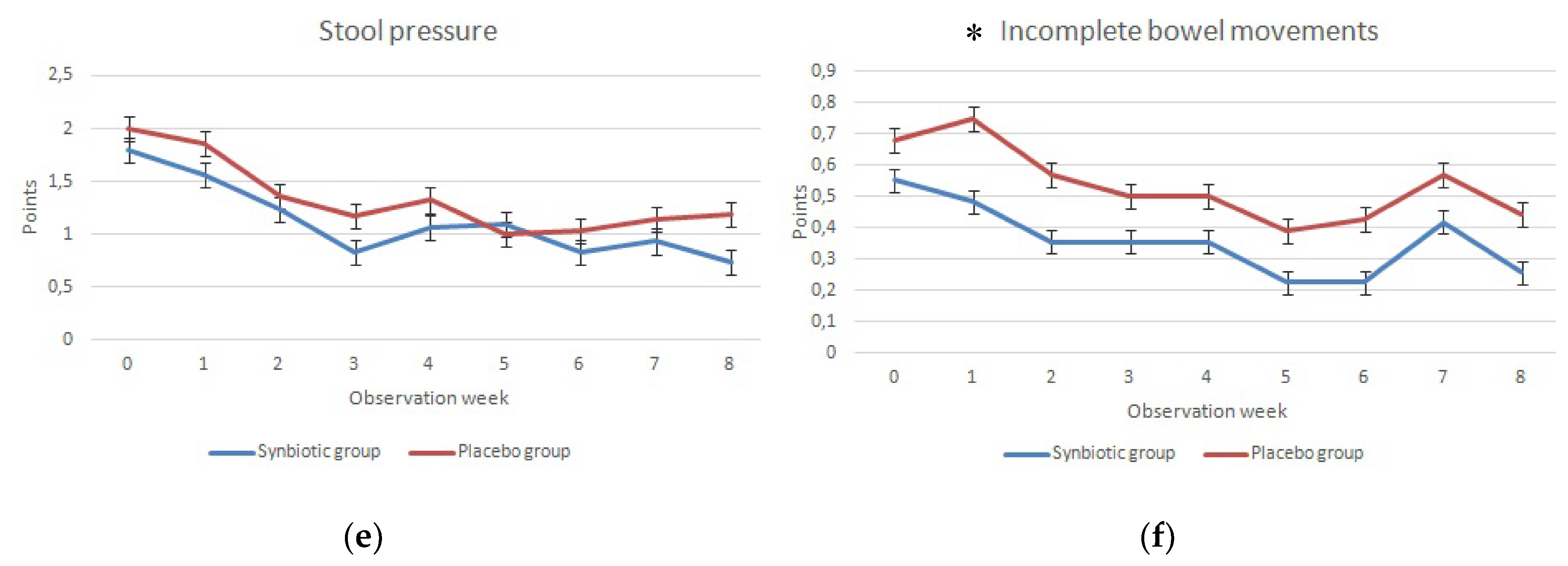
3.3. Study Secondary Endpoints
3.4. Safety and Adverse Events
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Synbiotic Group (n = 35) | Placebo Group (n = 33) | p-Value | OR | |||
|---|---|---|---|---|---|---|
| Improvement | No Improvement | Improvement | No Improvement | |||
| IBS-SSS 1 (the severity of pain) | ||||||
| Visit II | 6 (17.1) | 29 (82.9) | 9 (27.3) | 24 (72.7) | 0.387 | 1.797 |
| Visit III | 13 (37.1) | 22 (62.9) | 10 (30.3) | 23 (69.7) | 0.614 | 0.739 |
| IBS-SSS 2 (the frequency of pain) | ||||||
| Visit II | 6 (17.1) | 29 (82.9) | 5 (15.1) | 28 (84.9) | 1.000 | 0.865 |
| Visit III | 6 (17.1) | 29 (82.9) | 6 (18.2) | 27 (81.8) | 0.749 | 1.328 |
| IBS-SSS 3 (the severity of flatulence) | ||||||
| Visit II | 12 (34.3) | 23 (65.7) | 8 (24.2) | 25 (75.8) | 0.431 | 0.618 |
| Visit III | 18 (51.4) | 17 (48.6) | 12 (36.4) | 21 (63.6) | 0.232 | 0.545 |
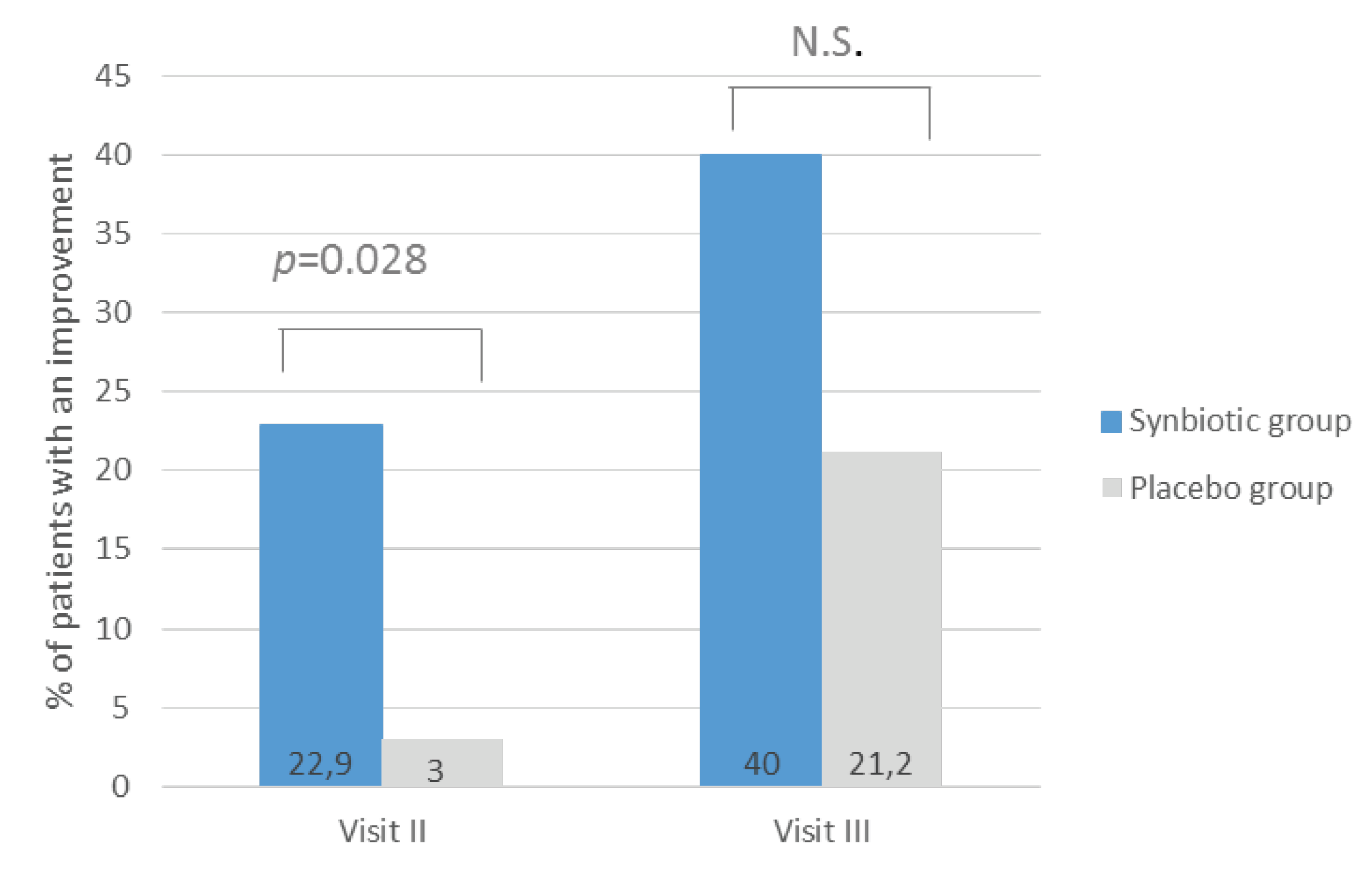
| IBS-SSS 4 (dissatisfaction with bowel habit) | ||||||
| Visit II | 8 (22.9) | 27(77.1) | 1 (3.0) | 32 (97.0) | 0.028 | 0.108 |
| Visit III | 14 (40.0) | 21 (60.0) | 7 (21.2) | 26(78.8) | 0.119 | 0.409 |
| IBS-SSS 5 (quality of life) | ||||||
| Visit II | 5 (14.3) | 30 (85.7) | 14 (40.0) | 21 (60.0) | 0.710 | 0.604 |
| Visit III | 3 (9.1) | 30 (90.9) | 10 (30.3) | 23 (69.7) | 0.454 | 0.656 |


References
- Ford, A.C.; Lacy, B.E.; Talley, N.J. Irritable bowel syndrome. N. Engl. J. Med. 2017, 376, 2566–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canavan, C.; West, J.; Card, T. The epidemiology of irritable bowel syndrome. Clin. Epidemiol. 2014, 6, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, B.M.; Farid, M.; Esrailian, E.; Talley, J.; Chang, L. Is Irritable bowel syndrome a diagnosis of exclusion? A survey of primary care providers, gastroenterologists, and IBS experts. Am. J. Gastroenterol. 2010, 105, 848–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattarai, Y.; Pedrogo, D.A.M.; Kashyap, P.C. Irritable bowel syndrome: A gut microbiota-related disorder? Am. J. Physiol.-Gastrointest. Liver Physiol. 2016, 312, G52–G62. [Google Scholar] [CrossRef]
- Distrutti, E.; Monaldi, L.; Ricci, P.; Fiorucci, S. Gut microbiota role in irritable bowel syndrome: New therapeutic strategies. World J. Gastroenterol. 2016, 22, 2219–2241. [Google Scholar] [CrossRef]
- Mari, A.; Baker, F.A.; Mahamid, M.; Sbeit, W.; Khoury, T. The Evolving role of gut microbiota in the management of irritable bowel syndrome: An overview of the current knowledge. J. Clin. Med. 2020, 9, 685. [Google Scholar] [CrossRef] [Green Version]
- Vivinus-Nébot, M.; Frin-Mathy, G.; Bzioueche, H.; Dainese, R.; Bernard, G.; Anty, R.; Filippi, J.; Saint-Paul, M.C.; Tulic, M.K.; Verhasselt, V.; et al. Functional bowel symptoms in quiescent inflammatory bowel diseases: Role of epithelial barrier disruption and low-grade inflammation. Gut 2013, 63, 744–752. [Google Scholar] [CrossRef]
- Pusceddu, M.M.; Gareau, M.G. Visceral pain: Gut microbiota, a new hope? J. Biomed. Sci. 2018, 25, 73. [Google Scholar] [CrossRef]
- Zhou, S.; Gillilland, M.G.; Wu, X.; Leelasinjaroen, P.; Zhang, G.; Zhou, H.; Ye, B.; Lu, Y.; Owyang, C. FODMAP diet modulates visceral nociception by lipopolysaccharide-mediated intestinal inflammation and barrier dysfunction. J. Clin. Investig. 2017, 128, 267–280. [Google Scholar] [CrossRef]
- Lee, H.R.; Pimentel, M. Bacteria and irritable bowel syndrome: The evidence for small intestinal bacterial overgrowth. Curr. Gastroenterol. Rep. 2006, 8, 305–311. [Google Scholar] [CrossRef]
- Carroll, I.M.; Ringel-Kulka, T.; Siddle, J.P.; Ringel, Y. Alterations in composition and diversity of the intestinal microbiota in patients with diarrhea-predominant irritable bowel syndrome. Neurogastroenterol. Motil. 2012, 24, 521–530.e248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, I.M.; Ringel-Kulka, T.; Keku, T.O.; Chang, Y.-H.; Packey, C.D.; Sartor, R.B.; Ringel, Y. Molecular analysis of the luminal- and mucosal-associated intestinal microbiota in diarrhea-predominant irritable bowel syndrome. Am. J. Physiol.-Gastrointest. Liver Physiol. 2011, 301, G799–G807. [Google Scholar] [CrossRef] [PubMed]
- Kerckhoffs, A.P.M.; Samsom, M.; van der Rest, M.E.; de Vogel, J.; Knol, J.; Ben-Amor, K.; Akkermans, L.M. Lower Bifidobacteria counts in both duodenal mucosa-associated and fecal microbiota in irritable bowel syndrome patients. World J. Gastroenterol. 2009, 15, 2887–2892. [Google Scholar] [CrossRef] [PubMed]
- Pozuelo, M.; Panda, S.; Santiago, A.; Mendez, S.; Accarino, A.; Santos, J.; Guarner, F.; Azpiroz, F.; Manichanh, C. Reduction of butyrate- and methane-producing microorganisms in patients with Irritable Bowel Syndrome. Sci. Rep. 2015, 5, 12693. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Liang, L.; Deng, H.; Guo, J.; Shu, H.; Zhang, L. Efficacy and Safety of Probiotics in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 332. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Harris, L.A.; Lacy, B.E.; Quigley, E.; Moayyedi, P. Systematic review with meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2018, 48, 1044–1060. [Google Scholar] [CrossRef] [Green Version]
- Asha, M.Z.; Khalil, S.F.H. Efficacy and safety of probiotics, prebiotics and synbiotics in the treatment of irritable bowel syndrome: A systematic review and meta-analysis. Sultan Qaboos Univ. Med. J. 2020, 20, e13–e24. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, L.; Guo, C.; Mu, D.; Feng, B.; Zuo, X.; Li, Y. Effects of probiotic type, dose and treatment duration on irritable bowel syndrome diagnosed by Rome III criteria: A meta-analysis. BMC Gastroenterol. 2016, 16, 62. [Google Scholar] [CrossRef] [Green Version]
- Tsuchiya, J.; Barreto, R.; Okura, R.; Kawakita, S.; Fesce, E.; Marotta, F. Single-blind follow-up study on the effectiveness of a symbiotic preparation in irritable bowel syndrome. Chin. J. Dig. Dis. 2004, 5, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.W.; Park, S.U.; Jang, Y.S.; Kim, Y.-H.; Rhee, P.-L.; Ko, S.H.; Joo, N.; Kim, S.I.; Kim, C.-H.; Chang, D.K. Effect of composite yogurt enriched with acacia fiber and Bifidobacterium lactis. World J. Gastroenterol. 2012, 18, 4563–4569. [Google Scholar] [CrossRef] [PubMed]
- A Drossman, U.; Dumitrascu, D.L. Rome III: New standard for functional gastrointestinal disorders. J. Gastrointest. Liver Dis. 2006, 15, 237–241. [Google Scholar]
- Riegler, G.; Esposito, I. Bristol scale stool form. A still valid help in medical practice and clinical research. Tech. Coloproctology 2001, 5, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagala, R.; Routray, C. Clinical case study—Multispecies probiotic supplement minimizes symptoms of irritable bowel syndrome. US Gastroenterol. Hepatol. Rev. 2011, 7, 36–37. [Google Scholar]
- Gerasimov, S.; Gantzel, J.; Dementieva, N.; Schevchenko, O.; Tsitsura, O.; Guta, N.; Bobyk, V.; Kaprus, V. Role of Lactobacillus rhamnosus (FloraActive™) 19070-2 and Lactobacillus reuteri (FloraActive™) 12246 in Infant Colic: A Randomized Dietary Study. Nutrients 2018, 10, 1975. [Google Scholar] [CrossRef] [Green Version]
- Liang, D.; Longgui, N.; Guoqiang, X. Efficacy of different probiotic protocols in irritable bowel syndrome: A network meta-analysis. Medicine 2019, 98, e16068. [Google Scholar] [CrossRef]
- Gordon, S.; Ameen, V.; Bagby, B.; Shahan, B.; Jhingran, P.; Carter, E. Validation of irritable bowel syndrome Global Improvement Scale: An integrated symptom end point for assessing treatment efficacy. Dig. Dis. Sci. 2003, 48, 1317–1323. [Google Scholar] [CrossRef]
- Gracie, D.J.; Ford, A.C. Symbiotics in irritable bowel syndrome—Better than probiotics alone? Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 485–489. [Google Scholar] [CrossRef]
- Shavakhi, A.; Minakari, M.; Farzamnia, S.; Peykar, M.S.; Taghipour, G.; Tayebi, A.; Hashemi, H.; Shavakhi, S. The effects of multi-strain probiotic compound on symptoms and quality-of-life in patients with irritable bowel syndrome: A randomized placebo-controlled trial. Adv. Biomed. Res. 2014, 3, 139. [Google Scholar] [CrossRef] [PubMed]
- Cappello, C.; Tremolaterra, F.; Pascariello, A.; Ciacci, C.; Iovino, P. A randomised clinical trial (RCT) of a symbiotic mixture in patients with irritable bowel syndrome (IBS): Effects on symptoms, colonic transit and quality of life. Int. J. Colorectal Dis. 2012, 28, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogha, M.; Esfahani, M.Z.; Zargarzadeh, A.H. The efficacy of a synbiotic containing Bacillus Coagulans in treatment of irritable bowel syndrome: A randomized placebo-controlled trial. Gastroenterol. Hepatol. Bed Bench 2014, 7, 156–163. [Google Scholar]
- Guarino, M.P.L.; Altomare, A.; Emerenziani, S.; Di Rosa, C.; Ribolsi, M.; Balestrieri, P.; Iovino, P.; Rocchi, G.; Cicala, M. Mechanisms of action of prebiotics and their effects on gastro-intestinal disorders in adults. Nutrients 2020, 12, 1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlop, S.P.; Hebden, J.; Campbell, E.; Naesdal, J.; Olbe, L.; Perkins, A.C.; Spiller, R.C. Abnormal intestinal permeability in subgroups of diarrhea-predominant irritable bowel syndromes. Am. J. Gastroenterol. 2006, 101, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Bouhnik, Y.; Raskine, L.; Simoneau, G.; Paineau, D.; Bornet, F. The capacity of short-chain fructo-oligosaccharides to stimulate faecal bifidobacteria: A dose-response relationship study in healthy humans. Nutr. J. 2006, 5, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukahara, T.; Iwasaki, Y.; Nakayama, K.; Ushida, K. Stimulation of butyrate production in the large intestine of weaning piglets by dietary fructooligosaccharides and its influence on the histological variables of the large intestinal mucosa. J. Nutr. Sci. Vitaminol. 2003, 49, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Paineau, D.; Payen, F.; Panserieu, S.; Coulombier, G.; Sobaszek, A.; Lartigau, I.; Brabet, M.; Galmiche, J.-P.; Tripodi, D.; Sacher-Huvelin, S.; et al. The effects of regular consumption of short-chain fructo-oligosaccharides on digestive comfort of subjects with minor functional bowel disorders. Br. J. Nutr. 2008, 99, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Azpiroz, F.; DuBray, C.; Bernalier-Donadille, A.; Cardot, J.M.; Accarino, A.; Serra, J.; Wagner, A.; Respondek, F.; Dapoigny, M. Effects of scFOS on the composition of fecal microbiota and anxiety in patients with irritable bowel syndrome: A randomized, double blind, placebo controlled study. Neurogastroenterol. Motil. 2016, 29, e12911. [Google Scholar] [CrossRef] [Green Version]
- Basturk, A.; Artan, R.; Yılmaz, A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk. J. Gastroenterol. 2020, 27, 439–443. [Google Scholar] [CrossRef]
- Bahrudin, M.F.; Rani, R.A.; Tamil, A.M.; Mokhtar, N.M.; Ali, R.A.R. Effectiveness of sterilized symbiotic drink containing Lactobacillus helveticus comparable to probiotic alone in patients with constipation-predominant irritable bowel syndrome. Dig. Dis. Sci. 2019, 65, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]






| Strain | Colony-Forming Units (CFU) Per Sachet | CFU Per Daily Dose (2 Sachets) | Strain Number |
|---|---|---|---|
| Bifidobacterium lactis | 2.94 × 109 | 5.88 × 109 | DSMZ 32269 |
| Bifidobacterium longum | 2.94 × 108 | 5.88 × 108 | DSMZ 32946 |
| Bifidobacterium bifidum | 2.94 × 108 | 5.88 × 108 | DSMZ 32403 |
| Lactobacillus rhamnosus | 9.80 × 108 | 1.96 × 109 | FloraActive 19070-2 |
| Lactobacillus acidophilus | 4.90 × 108 | 9.80 × 108 | DSMZ 32418 |
| Total CFU | 5.00 × 109 | 1.00 × 1010 |
| Variable | Primary Score | Transformed Score |
|---|---|---|
| The type of stool | Bristol stool scale (points 1–7) | 0—constipation if primary scale = 1 or 2 1—normal stool if primary scale = 3 or 4 2—diarrhea if primary scale = 5 or 6 or 7 |
| The severity of pain, flatulence, stool pressure | 5-point Likert scale | 0—no or weak if primary scale = 0 or 1 1—intermediate if primary scale = 2 2—strong or very strong if primary scale = 3 or 4 |
| Synbiotic Group (n = 35) n (%) or Mean ± SD | Placebo Group (n = 33) n (%) or Mean ± SD | |
|---|---|---|
| Gender | ||
| Female | 25 (71.4%) | 24 (72.7%) |
| Male | 10 (28.6%) | 9 (27.3%) |
| Age in years | 43.2 ± 14.0 | 36.7 ± 12.7 |
| Weight in kg | 74.9 ± 14.6 | 69.0 ± 14.2 |
| Height in m | 1.69 ± 0.08 | 1.7 ± 0.09 |
| BMI | 26.21 ± 5.43 | 23.86 4.65 |
| IBS severity * | ||
| Moderate | 14 (40.0%) | 10 (30.3%) |
| Severe | 21 (60.0%) | 23 (69.7%) |
| Total IBS-SSS score | 318.1 ± 63.6 | 325.5 ± 49.9 |
| Groups | Baseline (Visit I) | Week 4 (Visit II) | Week 8 (Visit III) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Change from Baseline | p-Values within-Group | p-Values Comparison with Placebo | Mean ± SD | Change form Baseline | p-Values within-Group | p-Values Comparison with Placebo | ||
| Total IBS-SSS | ||||||||||
| Synbiotic | 318.1 ± 63.6 | 213.8 ± 58.7 | −104.3 ± 88.2 | <0.01 | 0.248 | 148.5 ± 51.2 | −169.6 ± 88.7 | <0.01 | 0.042 | |
| Placebo | 325.5 ± 49.9 | 233.8 ± 81.7 | −91.7 ± 82.0 | <0.01 | NA | 183.7 ± 85.7 | −141.8 ± 95.4 | <0.01 | NA | |
| IBS-SSS 1 (the severity of pain) | ||||||||||
| Synbiotic | 55.7 ± 23.4 | 37.1 ± 21.3 | −18.7 ± 28.8 | <0.01 | 0.878 | 24.9 ± 12.2 | −30.9 ± 24.7 | <0.01 | 0.118 | |
| Placebo | 60.6 ± 20.8 | 37.9 ± 17.8 | −22.7 ± 29.5 | <0.01 | NA | 31.8 ± 22.8 | −28.8 ± 32.5 | <0.01 | NA | |
| IBS-SSS 2 (the frequency of pain) | ||||||||||
| Synbiotic | 32.1 ± 18.5 | 20.3 ± 17.0 | −13.0 ± 28.1 | <0.01 | 0.509 | 12.5 ± 16.3 | −19.6 ± 20.4 | <0.01 | 0.151 | |
| Placebo | 34.8 ± 21.6 | 23.5 ± 21.6 | −11.4 ± 26.6 | <0.01 | NA | 19.7 ± 24.0 | −15.2 ± 29.9 | <0.01 | NA | |
| IBS-SSS 3 (the severity of flatulence) | ||||||||||
| Synbiotic | 63.2 ± 30.2 | 42.4 ± 25.0 | −20.8 ± 32.8 | <0.01 | 0.039 | 23.6 ± 19.1 | −40.1 ± 35.4 | <0.01 | 0.028 | |
| Placebo | 68.2 ± 18.0 | 55.3 ± 25.6 | −12.9 ± 26.6 | <0.01 | NA | 34.1 ± 19.6 | −33.9 ± 29.9 | <0.01 | NA | |
| IBS-SSS 4 (dissatisfaction with bowel habit) | ||||||||||
| Synbiotic | 83.5 ± 19.0 | 58.5 ± 16.3 | −25.0 ± 29.7 | <0.01 | 0.590 | 44.1 ± 21.3 | −39.4 ± 30.0 | <0.01 | 0.135 | |
| Placebo | 80.2 ± 17.1 | 61.1 ± 22.6 | −19.4 ± 22.0 | <0.01 | NA | 52.1 ± 22.0 | −28.4 ± 25.2 | <0.01 | NA | |
| IBS-SSS 5 (quality of life) | ||||||||||
| Synbiotic | 83.5 ± 19.0 | 56.6 ± 17.2 | −26.9 ± 22.7 | <0.01 | 0.913 | 43.4 ± 21.0 | −40.1 ± 25.4 | <0.01 | 0.618 | |
| Placebo | 81.5 ± 17.2 | 56.1 ± 21.2 | −25.4 ± 22.3 | <0.01 | NA | 46.0 ± 21.8 | −35.4 ± 25.0 | <0.01 | NA | |
| Probiotic Group (n = 35) | Placebo Group (n = 33) | p-Value | OR | |||
|---|---|---|---|---|---|---|
| Improvement | No Improvement | Improvement | No Improvement | |||
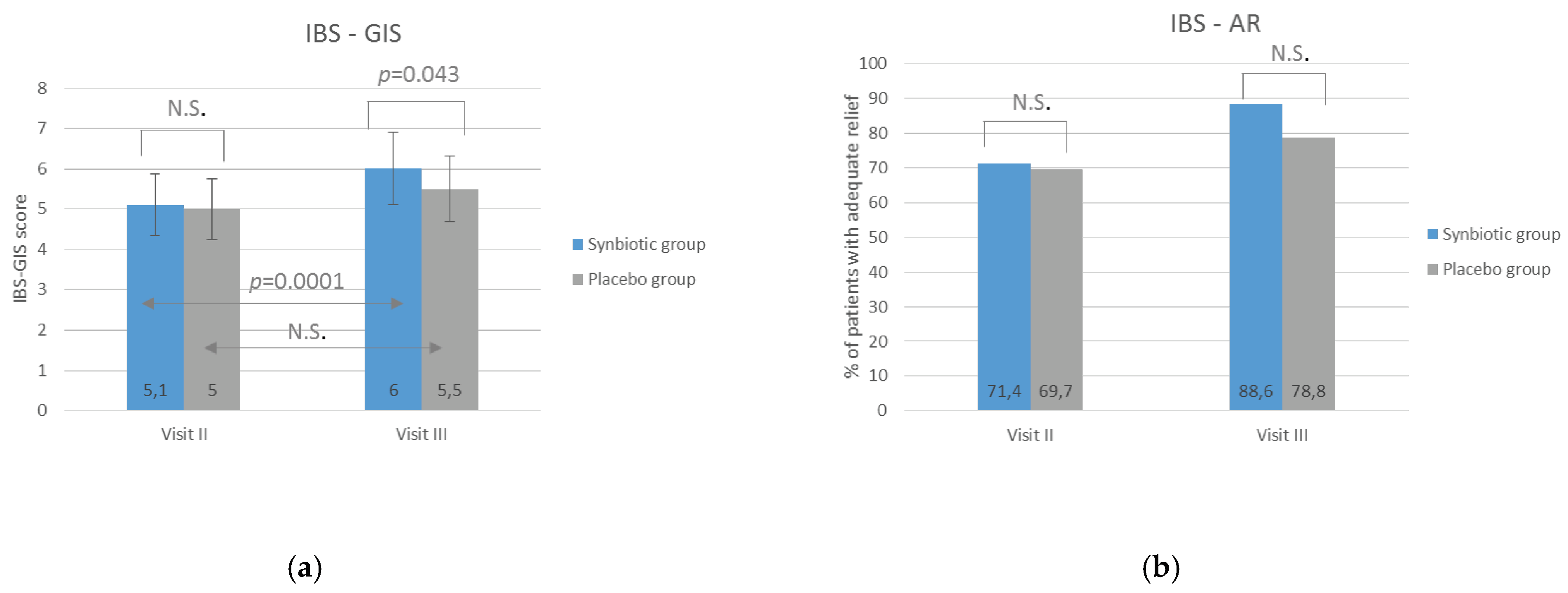
| Visit II | 27 (77.1) | 8 (22.9) | 24 (72.7) | 9 (27.3) | 0.7819 | 0.7929 |
| Visit III | 33 (94.3) | 2 (5.7) | 26 (78.8) | 7 (21.2) | 0.0794 | 0.2299 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skrzydło-Radomańska, B.; Prozorow-Król, B.; Cichoż-Lach, H.; Majsiak, E.; Bierła, J.B.; Kosikowski, W.; Szczerbiński, M.; Gantzel, J.; Cukrowska, B. The Effectiveness of Synbiotic Preparation Containing Lactobacillus and Bifidobacterium Probiotic Strains and Short Chain Fructooligosaccharides in Patients with Diarrhea Predominant Irritable Bowel Syndrome—A Randomized Double-Blind, Placebo-Controlled Study. Nutrients 2020, 12, 1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071999
Skrzydło-Radomańska B, Prozorow-Król B, Cichoż-Lach H, Majsiak E, Bierła JB, Kosikowski W, Szczerbiński M, Gantzel J, Cukrowska B. The Effectiveness of Synbiotic Preparation Containing Lactobacillus and Bifidobacterium Probiotic Strains and Short Chain Fructooligosaccharides in Patients with Diarrhea Predominant Irritable Bowel Syndrome—A Randomized Double-Blind, Placebo-Controlled Study. Nutrients. 2020; 12(7):1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071999
Chicago/Turabian StyleSkrzydło-Radomańska, Barbara, Beata Prozorow-Król, Halina Cichoż-Lach, Emilia Majsiak, Joanna B. Bierła, Wojciech Kosikowski, Mariusz Szczerbiński, Jesper Gantzel, and Bożena Cukrowska. 2020. "The Effectiveness of Synbiotic Preparation Containing Lactobacillus and Bifidobacterium Probiotic Strains and Short Chain Fructooligosaccharides in Patients with Diarrhea Predominant Irritable Bowel Syndrome—A Randomized Double-Blind, Placebo-Controlled Study" Nutrients 12, no. 7: 1999. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12071999