Randomised Controlled Trial: Partial Hydrolysation of Casein Protein in Milk Decreases Gastrointestinal Symptoms in Subjects with Functional Gastrointestinal Disorders

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
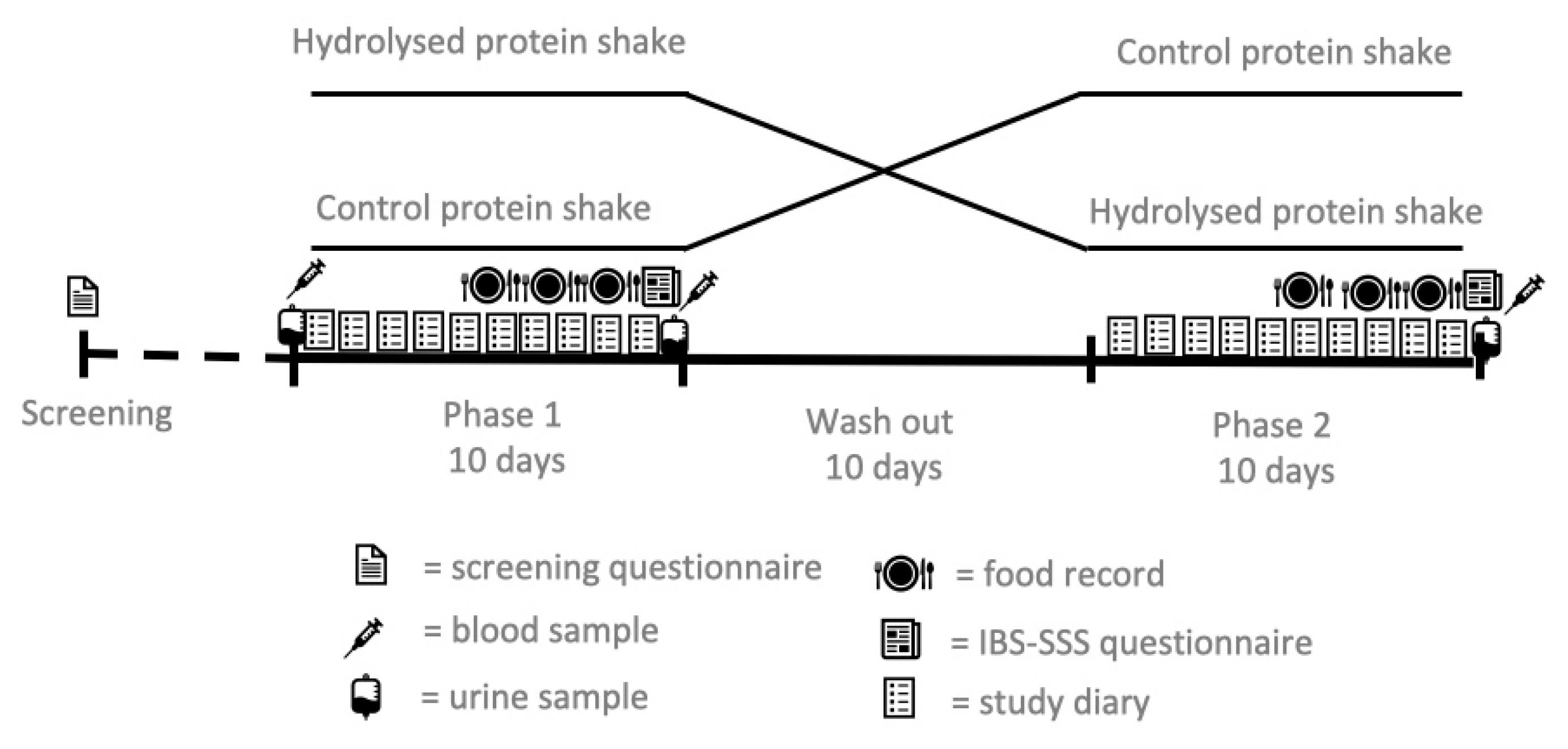
2.1. Subjects and Study Design
2.2. Study Products and Diet
2.3. Gastrointestinal Symptoms
2.4. Urine Samples
2.5. Blood Samples
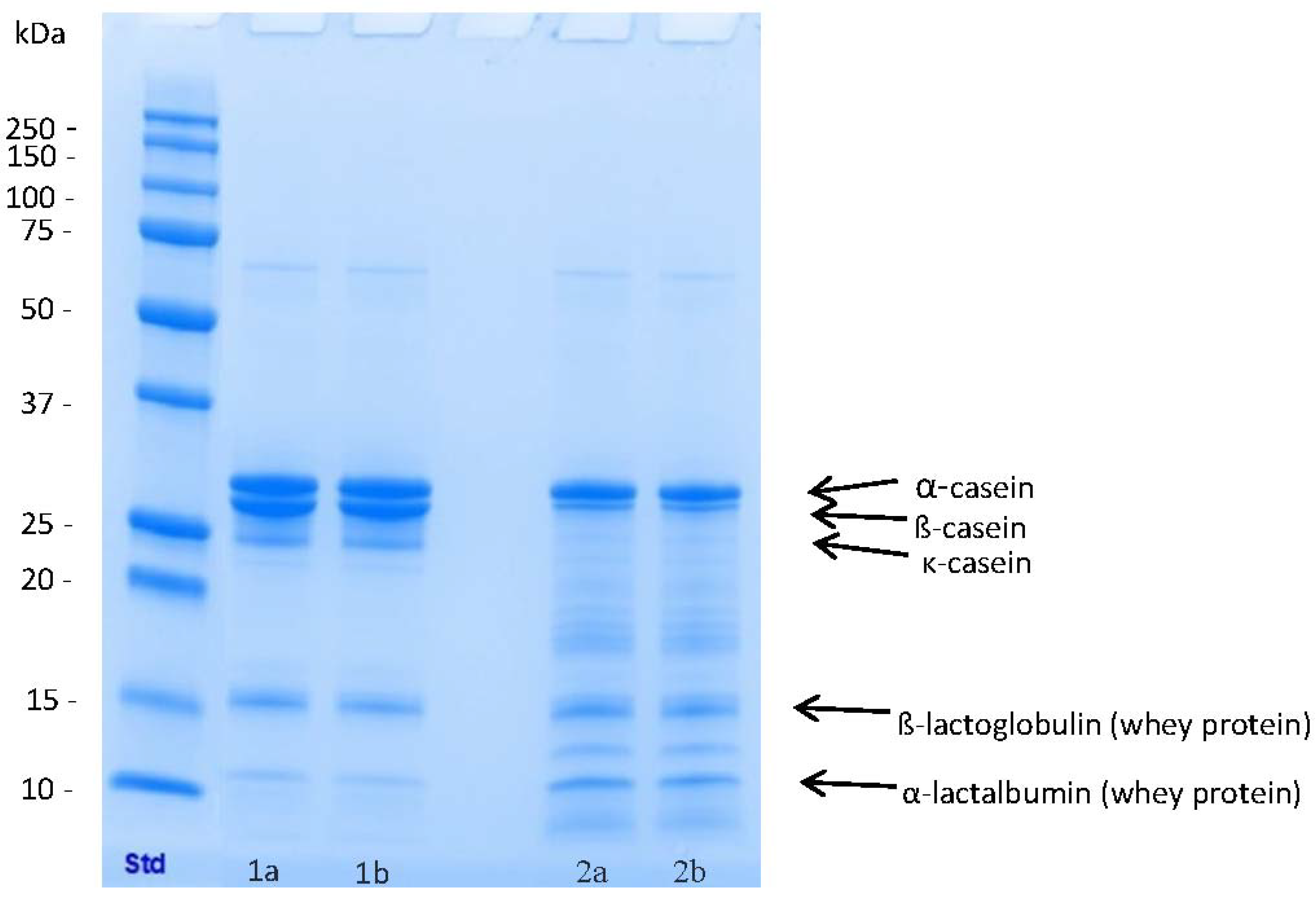
2.6. Laboratory Methods
2.7. Statistical Analyses
3. Results
3.1. Compliance
3.2. Gastrointestinal Symptoms
3.3. Inflammatory Markers, Intestinal Permeability and Immune Activation
3.4. Dietary Intakes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Simrén, M.; Tack, J. New treatments and therapeutic targets for IBS and other functional bowel disorders. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 589–605. [Google Scholar] [CrossRef] [PubMed]
- Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A.; Chang, L.; Chey, W.; Crowell, M.D.; Keefer, L.; Lembo, A.J.; Parkman, H.P.; Rao, S.S.; et al. Development and validation of the Rome IV diagnostic questionnaire for adults. Gastroenterology 2016, 150, 1481–1491. [Google Scholar] [CrossRef]
- Simren, M.; Månsson, A.; Langkilde, A.M.; Svedlund, J.; Abrahamsson, H.; Bengtsson, U.; Björnsson, E.S. Food-related gastrointestinal symptoms in the irritable bowel syndrome. Digestion 2001, 63, 108–115. [Google Scholar] [CrossRef]
- Böhn, L.; Störsrud, S.; Törnblom, H.; Bengtsson, U.; Simren, M. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am. J. Gastroenterol. 2013, 108, 634–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staudacher, H.M.; Whelan, K. The low FODMAP diet: Recent advances in understanding its mechanisms and efficacy in IBS. Gut 2017, 66, 1517–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthoni, S. Cow’s Milk Related Gastrointestinal Symptoms in Adults. Ph.D. Thesis, University of Helsinki, Helsinki, Finland, 2009. [Google Scholar]
- Sahi, T.; Launiala, K.; Laitinen, H. Hypolactasia in a fixed cohort of young Finnish adults. A follow-up study. Scand. J. Gastroenterol. 1983, 18, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Kristjánsson, G.; Venge, P.; Hällgren, R. Mucosal reactivity to cow’s milk protein in coeliac disease. Clin. Exp. Immunol. 2007, 147, 449–455. [Google Scholar] [CrossRef]
- Pelto, L.; Salminen, S.; Lilius, E.M.; Nuutila, J.; Isolauri, E. Milk hypersensitivity—Key to poorly defined gastrointestinal symptoms in adults. Allergy 1998, 53, 307–310. [Google Scholar] [CrossRef]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D’Alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: Exploring a new clinical entity. Am. J. Gastroenterol. 2012, 107, 1898–1906. [Google Scholar] [CrossRef] [Green Version]
- Turpeinen, A.; Kautiainen, H.; Tikkanen, M.L.; Sibakov, T.; Tossavainen, O.; Myllyluoma, E. Mild protein hydrolysation of lactose-free milk further reduces milk-related gastrointestinal symptoms. J. Dairy Res. 2016, 83, 256–260. [Google Scholar] [CrossRef]
- Sibakov, T.; Tossavainen, O. Milk Product and Preparation Method. Finland EP Patent 2632277B1, 4 September 2013. [Google Scholar]
- Matsubara, H.; Hagihara, B.; Nakai, M.; Komaki, T.; Yonetani, T.; Okunuki, K. Crystalline bacterial proteinase II. General properties of crystalline proteinase of Bacillus subtilis N. J. Biochem. 1958, 45, 251–258. [Google Scholar] [CrossRef]
- Bonfatti, V.; Grigoletto, L.; Cecchinato, A.; Gallo, L.; Carnier, P. Validation of a new reversed phase high-performance liquid chromatography method for separation and quantification of bovine milk protein genetic variants. J. Chromatogr. A 2008, 1195, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Laemmli, U.K. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature 1970, 227, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Drossman, D.A.; Chang, L.; Bellamy, N.; Gallo-Torres, H.E.; Lembo, A.; Mearin, F.; Norton, N.J.; Whorwell, P. Severity in irritable bowel syndrome: A Rome Foundation Working Team report. Am. J. Gastroenterol. 2011, 106, 1749–1759. [Google Scholar] [CrossRef]
- Nuora, A.; Tupasela, T.; Jokioja, R.; Tahvonen, R.; Kallio, H.; Yang, B.; Viitanen, M.; Linderborg, K.M. The effect of heat treatments and homogenisation of cows’ milk on gastrointestinal symptoms, inflammation markers and postprandial lipid metabolism. Int. Dairy J. 2018, 85, 184–190. [Google Scholar] [CrossRef]
- Mummah, S.; Oelrich, J.; Hope, Q.; Vu, C.D. Effect of raw milk on lactose intolerance: A randomized controlled pilot study. Ann. Fam. Med. 2014, 12, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Korpela, R.; Paajanen, L.; Tuure, T. Homogenization of milk has no effect on the gastrointestinal symptoms of lactose intolerant subjects. Milchwissenschaft 2005, 6, 3–6. [Google Scholar]
- Paajanen, L.; Tuure, T.; Poussa, T.; Korpela, R. No difference in symptoms during challenges with homogenized and unhomogenized cow’s milk in subjects with subjective hypersensitivity to homogenized milk. J. Dairy Res. 2003, 70, 175–179. [Google Scholar] [CrossRef]
- Pelto, L.; Rantakokko, H.-K.; Lilius, E.-M.; Nuutila, J.; Salminen, S. No difference in symptoms and receptor expression in lactose-intolerant and in milk-hypersensitive subjects following intake of homogenized and unhomogenized milk. Int. Dairy J. 2000, 10, 799–803. [Google Scholar] [CrossRef]
- Brooke-Taylor, S.; Dwyer, K.; Woodford, K.; Kost, N. Systematic review of the gastrointestinal effects of a1 compared with a2 β-casein. Adv. Nutr. 2017, 8, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.; Woodford, K.; Kukuljan, S.; Pal, S. Comparative effects of A1 versus A2 beta-casein on gastrointestinal measures: A blinded randomised cross-over pilot study. Eur. J. Clin. Nutr. 2014, 68, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Krammer, L.; Sowa, A.S.; Lorentz, A. Mast cells in irritable bowel syndrome: A systematic review. J. Gastrointest. Liver Dis. 2019, 28, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Robles, A.; Perez Ingles, D.; Myneedu, K.; Deoker, A.; Sarosiek, I.; Zuckerman, M.J.; Schmulson, M.J.; Bashashati, M. Mast cells are increased in the small intestinal mucosa of patients with irritable bowel syndrome: A systematic review and metaanalysis. Neurogastroenterol. Motil. 2019, 31, e13718. [Google Scholar] [CrossRef] [Green Version]
- McIntosh, K.; Reed, D.E.; Schneider, T.; Dang, F.; Keshteli, A.H.; De Palma, G.; Madsen, K.; Bercik, P.; Vanner, S. FODMAPs alter symptoms and the metabolome of patients with IBS: A randomised controlled trial. Gut 2019, 66, 1241–1251, Erratum in Gut 2019, 68, 1342. [Google Scholar] [CrossRef]
- Wouters, M.M.; Balemans, D.; Van Wanrooy, S.; Dooley, J.; Cibert-Goton, V.; Alpizar, Y.A.; Valdez-Morales, E.E.; Nasser, Y.; Van Veldhoven, P.P.; Vanbrabant, W.; et al. Histamine receptor H1-mediated sensitization of TRPV1 mediates visceral hypersensitivity and symptoms in patients with irritable bowel syndrome. Gastroenterology 2016, 150, 875–887. [Google Scholar] [CrossRef] [Green Version]
- Staudacher, H.M.; Irving, P.M.; Lomer, M.C.E.; Whelan, K. The challenges of control groups, placebos and blinding in clinical trials of dietary interventions. Proc. Nutr. Soc. 2017, 76, 203–212. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All n = 41 | Women n = 33 | Men n = 8 | |
|---|---|---|---|
| Age, years | 44.0 ± 10.8 | 44.9 ± 10.9 | 40.6 ± 10.2 |
| Height, cm | 170.0 ± 10.8 | 166.8 ± 5.8 | 182.3 ± 8.3 |
| Weight, kg | 75.8 ± 16.2 | 72.2 ± 15.2 | 90.2 ± 11.8 |
| BMI, kg/m2 | 26.2 ± 4.9 | 26.0 ± 5.3 | 27.1 ± 2.9 |
| Diagnosis | |||
| IBS | 23 | 17 | 6 |
| Functional dyspepsia | 3 | 3 | 0 |
| Functional diarrhoea | 6 | 5 | 1 |
| Functional bloating | 9 | 8 | 1 |
| Control | Hydrolysed | |
|---|---|---|
| Energy, kJ/kcal | 335/80 | 322/77 |
| Protein, g | 10.6 | 10.3 |
| Fat, g | 1.6 | 1.5 |
| Carbohydrates, g | 5.7 | 5.5 |
| Lactose, g | <0.01 | <0.01 |
| Baseline | Hydrolysed | Control | p-Value Hydrolysed versus Control † | |
|---|---|---|---|---|
| IBS-SSS | 199 ± 71 | 163 ± 74 * | 205 ± 75 | 0.001 |
| Symptom score | 14.7 ± 3.9 | 12.5 ± 2.4 * | 14.0 ± 3.4 | 0.002 |
| Abdominal pain | 1.89 ± 0.74 | 1.61 ± 0.56 | 1.85 ± 0.67 | 0.09 |
| Bloating | 2.46 ± 1.00 | 2.05 ± 0.70 * | 2.17± 0.88 * | 0.72 |
| Flatulence | 2.49 ± 0.77 | 2.12 ± 0.61 * | 2.32 ± 0.63 | 0.16 |
| Rumbling | 1.68 ± 0.81 | 1.39 ± 0.48 | 1.51 ± 0.59 | 0.25 |
| Diarrhoea | 1.85 ± 0.82 | 1.55 ± 0.64 | 1.62 ± 0.68 | 0.89 |
| Constipation | 1.45 ± 0.70 | 1.42 ± 0.54 | 1.54 ± 0.74 | 0.74 |
| Heartburn | 1.31 ± 0.56 | 1.09 ± 0.20 * | 1.25 ± 0.40 | 0.01 |
| Rapid feeling of fullness | 1.55 ± 0.97 | 1.40 ± 0.59 | 1.38 ± 0.70 | 0.37 |
| Baseline | Hydrolysed | Control | p-Value † | |
|---|---|---|---|---|
| Plasma IL-6, pg/mL | 1.16 ± 0.94 | 1.60 ± 1.34 * | 1.28 ± 1.23 | 0.20 |
| Plasma TNF-α, pg/mL | 0.82 ± 0.35 | 0.84 ± 0.37 | 0.84 ± 0.38 | 0.48 |
| Plasma FABP2, ng/mL | 1.29 ± 0.47 | 1.42 ± 0.68 | 1.26 ± 0.52 | 0.13 |
| Histamine ‡ | 131 ± 41 | 111 ± 37 * | 117 ± 44 | 0.43 |
| Hydrolysed | Control | p-Value † | |
|---|---|---|---|
| Energy, KJ/day | 8404 ± 1753 | 8786 ± 2352 | 0.139 |
| Energy, Kcal/day | 2008 ± 419 | 2100 ± 562 | 0.139 |
| Protein, g/day | 121 ± 28 | 117 ± 30 | 0.562 |
| Fat, g/day | 76 ± 23 | 79 ± 33 | 0.442 |
| Carbohydrates, g/day | 185 ± 50 | 198 ± 65 | 0.111 |
| Fibre, g/day | 27 ± 9 | 27 ± 9 | 0.872 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laatikainen, R.; Salmenkari, H.; Sibakov, T.; Vapaatalo, H.; Turpeinen, A. Randomised Controlled Trial: Partial Hydrolysation of Casein Protein in Milk Decreases Gastrointestinal Symptoms in Subjects with Functional Gastrointestinal Disorders. Nutrients 2020, 12, 2140. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072140
Laatikainen R, Salmenkari H, Sibakov T, Vapaatalo H, Turpeinen A. Randomised Controlled Trial: Partial Hydrolysation of Casein Protein in Milk Decreases Gastrointestinal Symptoms in Subjects with Functional Gastrointestinal Disorders. Nutrients. 2020; 12(7):2140. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072140
Chicago/Turabian StyleLaatikainen, Reijo, Hanne Salmenkari, Timo Sibakov, Heikki Vapaatalo, and Anu Turpeinen. 2020. "Randomised Controlled Trial: Partial Hydrolysation of Casein Protein in Milk Decreases Gastrointestinal Symptoms in Subjects with Functional Gastrointestinal Disorders" Nutrients 12, no. 7: 2140. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12072140